
Abstract
Background and Study Aims
Tibial plateau fractures with articular depression are difficult to treat. The purpose of this paper is to present a novel technique for the effective and efficient use of crushed cancellous allograft for management of depressed tibial plateau fractures.
Patients and Methods
A retrospective, single-surgeon study of sixteen cases of depressed tibial plateau fractures augmented with cancellous allograft via the following technique was conducted. The technique involved utilization of multiple 3 mL syringes for introduction of allograft into the identified tibial metaphyseal defects followed by bone tamping to create a packed bed of structural allograft. Patients were included only if presenting with traumatic, closed tibial plateau fractures who underwent indicated open reduction and internal fixation with the noted technique with at least 12 months of radiographic follow-up.
Results
All sixteen cases went on to union as determined by radiographic evaluation with minimal subsidence of the articular surface.
Conclusion
The described technique provides an effective, efficient, and novel method of filling the metaphyseal defect created after restoring articular depression in tibial plateau fractures.
Introduction
Tibial plateau fractures are relatively common, accounting for approximately 1% of all fractures.1,2 Articular depression of the tibial plateau is commonly seen with such fractures, with restoration and postoperative maintenance of articular congruity critical for prevention of postoperative complications.3-7 In tibial plateau fractures with significant depression of the articular surface, bone graft use has been well-described in augmenting fixation with reduction in the incidence of subsidence postoperatively.3,4,8 Historically, iliac crest autograft has been considered the gold standard throughout literature for bone defect supplementation across a variety of orthopaedic procedures, including open reduction and internal fixation of tibial plateau fractures.9-11 However, iliac crest autografting has been associated with significant donor site morbidity along with increased risk of infection, increased surgical time, and greater blood loss.9-12
While other methods of autografting are being explored,13-15 alternatives to autograft in the management of tibial plateau fractures include both cancellous bone allograft and bone graft substitutes.11,16-21 Although bone graft substitutes have demonstrated promising early results in augmentation of tibial plateau fixation constructs, significant limitations including expense and concerns for higher complication rates including heterotopic ossification encourage further study before routine implementation.11,16-18,20,22 Alternatively, allograft possesses several consistent advantages including general ease of use, decreased operative time, versatility in morphology of graft, and lack of the donor-site morbidity seen in autograft. 11 However, in the setting of tibial plateau fractures, application of the graft into the defect can be both challenging and time consuming.23,24 This paper presents a novel technique for the effective and efficient use of crushed, cancellous allograft for management of depressed tibial plateau fractures in sixteen cases across fourteen patients.
Methods
Patient Population
Patients from a single institution above the age of eighteen who presented with traumatic, non-elective, indications for operative management of closed tibial plateau fractures retrospectively identified by Current Procedural Terminology (CPT) codes 27535 and 27536, designating unicondylar and bicondylar fixations respectively, between September 2016 and November 2019 were included in the present study. Patients were included if they underwent the tibial allograft technique as described below in the Surgical Technique and Perioperative Protocol subsection. Further inclusion criteria included at least 12 months of radiographic follow-up. All surgeries were performed by the senior author (M.P.S.). This study was exempt from requiring Institutional Review Board approval due its nature as a retrospective chart review in addition to maintained anonymity of included patients.
Surgical Technique and Perioperative Protocol
All patients were brought to the operating room and positioned supine on a radiolucent table. After induction of anesthesia, the extremity was prepped and draped, and the limb was exsanguinated using an esmarch wrap and tourniquet. A one- or two-incision approach to the proximal tibia was performed depending on fracture pattern and planned fixation. Submeniscal arthrotomy was performed to visualize the joint surface. For this technique, an anterolateral corticotomy was performed on the proximal tibia if a cortical window was not already present through the fracture fragments. The joint surface was reduced using bone tamps and provisionally fixed with K-wires. While the approach and reduction were being performed, an assistant prepared the syringes for the bone grafting technique. Multiple 3 mL syringes, typically 10 total, were utilized. The tips of each syringe were cut off. Each syringe was loaded with freeze-dried, crushed, cancellous allograft and set aside (Figure 1). Multiple 3 mL syringes are opened in a sterile fashion, the tips are cut off, and each syringe is loaded with crushed cancellous allograft and set aside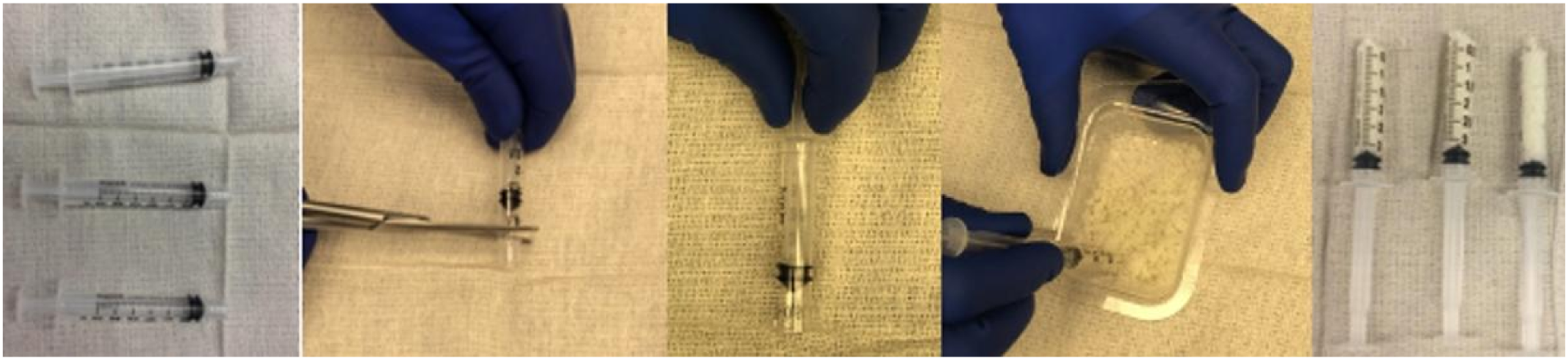
When the reduction and provisional fixation was completed, the graft-filled syringes were placed through the cortical window into the metaphyseal region. The plungers were pushed down so that the stopper pushes the allograft into the defect. Bone tamps were utilized intermittently to create a densely packed bed of structural allograft. Fluoroscopic images can be used to visualize graft placement and adequate filling of the defect. Figure 2 demonstrates intraoperative insertion of the allograft using this technique as well as intraoperative fluoroscopic images of the defect being filled. Care should be utilized while filling the defect to not inadvertently leave behind the rubber stopper of the syringe. After making the standard cortical window in the proximal tibia and reducing the articular surface, the syringes are placed into the defect and the bone graft is inserted. Caution should be taken during this step to avoid accidentally inserting the rubber portion of the plunger into the defect. Multiple syringes are used until the defect is completely filled. Fluoroscopy can be utilized to visualize the defect being filled
Once the defect was adequately filled, the cortical window was replaced and definitive fixation was placed. In this case series, precontoured periarticular locking plates with 3.5 mm screws were used. Final fluoroscopic images were obtained to confirm appropriate reduction and fixation (Figure 3). Wounds were irrigated, closed in multiple layers, and dressed with soft, sterile dressings. The patients were kept non-weight bearing to the operative extremity for 12 weeks with full, unrestricted active and passive knee range of motion. Final fluoroscopic images of filled defect and definitive internal fixation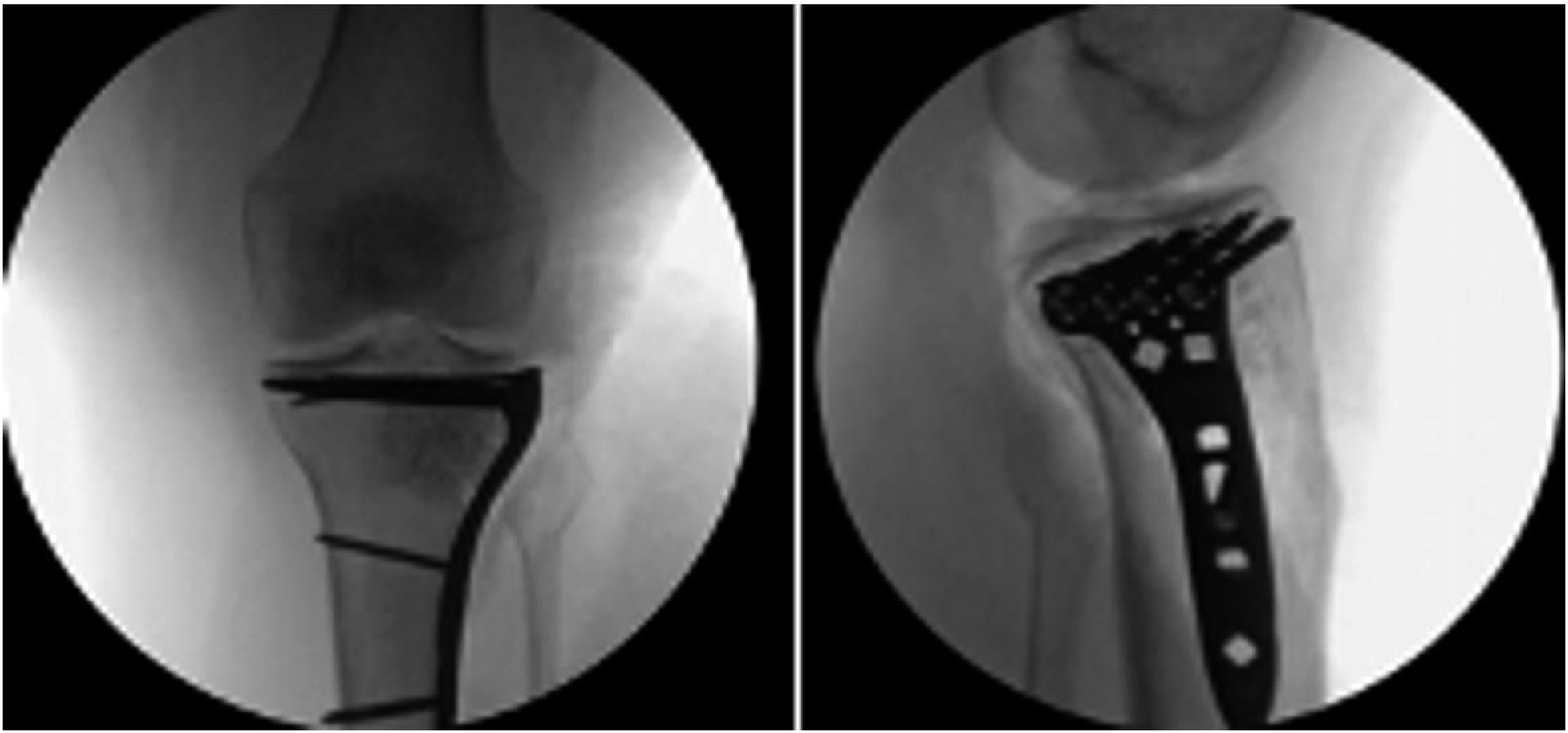
Data Collection
Data collected included demographic variables and risk factors of age, sex, obesity (body mass index ≥30), active smoking, and diabetes. Preoperative radiographic data collected included Arbeitsgemeinschaft für Osteosynthesefragen (AO) and Schatzker classifications, determined by authors S.M.C. and J.A.R. with any disputes in classification finalized by senior author M.P.S. Anteroposterior and lateral radiographs were obtained of the operative knee immediately postoperatively and at 6-week (initial), 12-week, 6-month, and 1-year (final) follow-up.
The primary outcome of this present case series was subsidence at the time of 12-month follow-up. Subsidence was determined as a ratio through two measurements obtained, A and B (Figure 4). Measurement A represented the vertical distance between the cranial junction of the axilla screw at the plate interface to the level of the most proximal subchondral rafting screw. Measurement B represented the vertical distance between the cranial junction of the axilla screw at the plate interface to the proximal extension of the plate. Thus, measurement B could be considered a fixed distance from which measurement A could be compared as a ratio, measurement A divided by measurement B, to assess for subsidence while avoiding variations in magnification or obliquity in radiographs that could lead to inaccuracies with raw measurement alone. Measurements A and B for all patients were independently collected by authors S.M.C., J.A.R., and M.P.S. from initial postoperative (6-week) and final postoperative follow-up (12-month) radiographs. Example of measurement technique. (A) represents the measurement from the cranial junction of the axilla screw and the plate to the level of the most proximal subchondral rafting screw in line with the articular surface at the site of initial depression. (B) represents the measurement along the same line starting at the cranial junction of the axilla screw and the plate extending proximally to the articular surface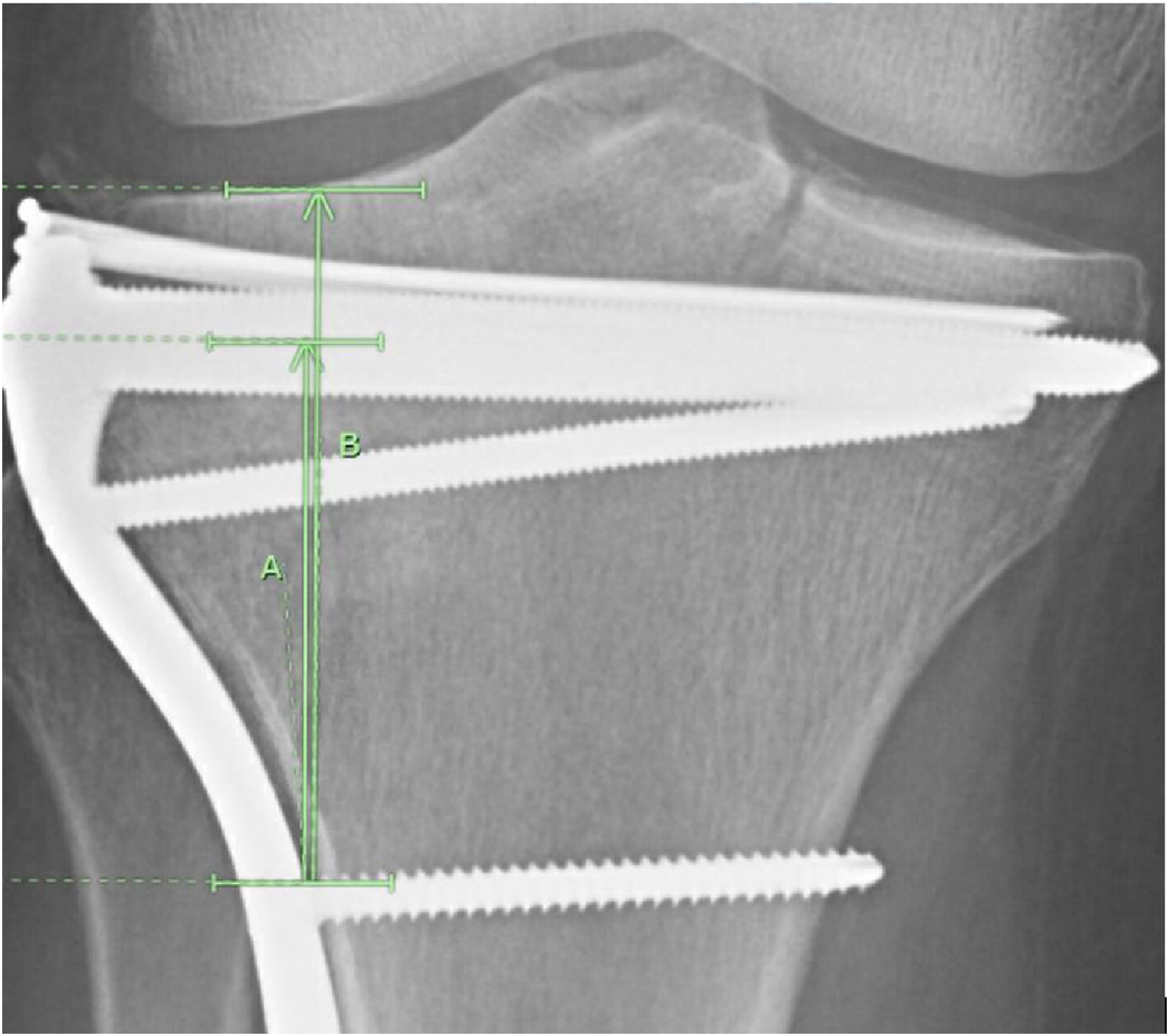
Statistical Analysis
All statistical analyses were performed using Microsoft Excel Version 16.83 (Microsoft Corporation, Redmond, WA). For each individual patient, the mean of measurement A was calculated as the average between all three authors both for immediate postoperative and final follow-up measurements. Similarly, the mean of measurement B was calculated as the average between all three authors both for initial postoperative and final follow-up measurements. These mean values were used to calculate the ratio of measurement A to measurement B (A/B) for both initial and final postoperative follow-up. The final follow-up ratio was then arithmetically subtracted from the initial follow-up ratio to determine the percentage of subsidence with positive values indicating relative loss of articular height. Any obtained negative values were determined to represent lack of measurable subsidence with the positive height variation indicating expected random error in measurement or resultant of variation in interobserver measurement. Average subsidence across the case series was determined via arithmetic mean while using values of 0.00 for patients with a positive height variation for lack of measurable subsidence.
Results
Descriptive Analysis
Demographics
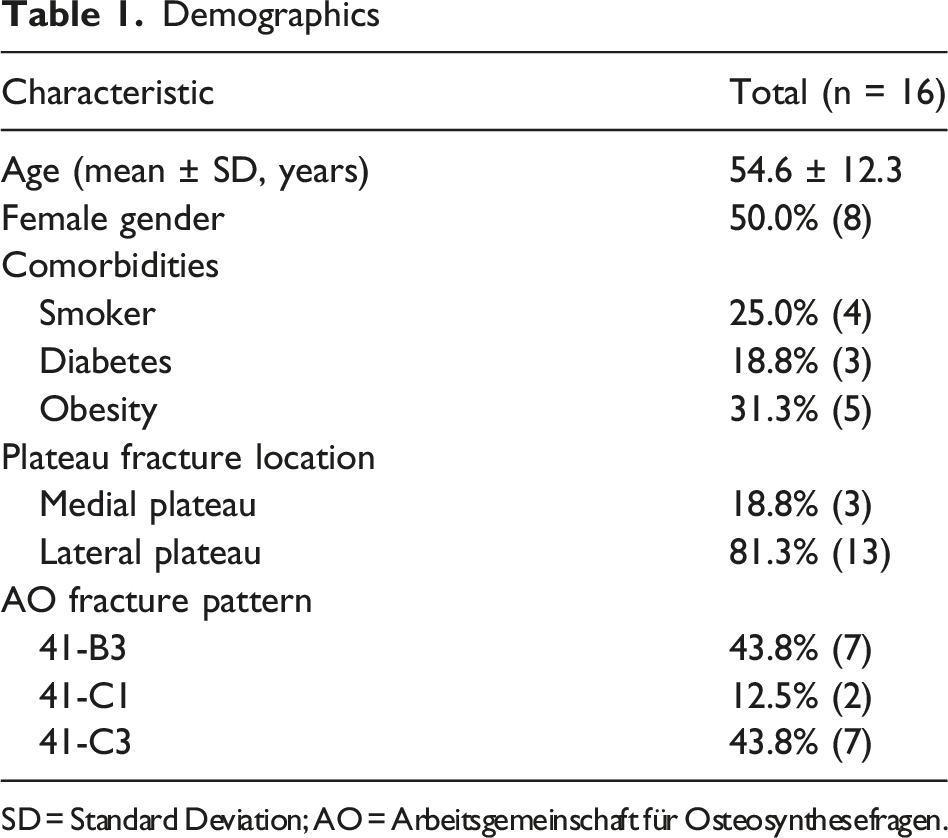
SD = Standard Deviation; AO = Arbeitsgemeinschaft für Osteosynthesefragen.
Primary Outcome Measures
Percentage of Articular Subsidence by Patient
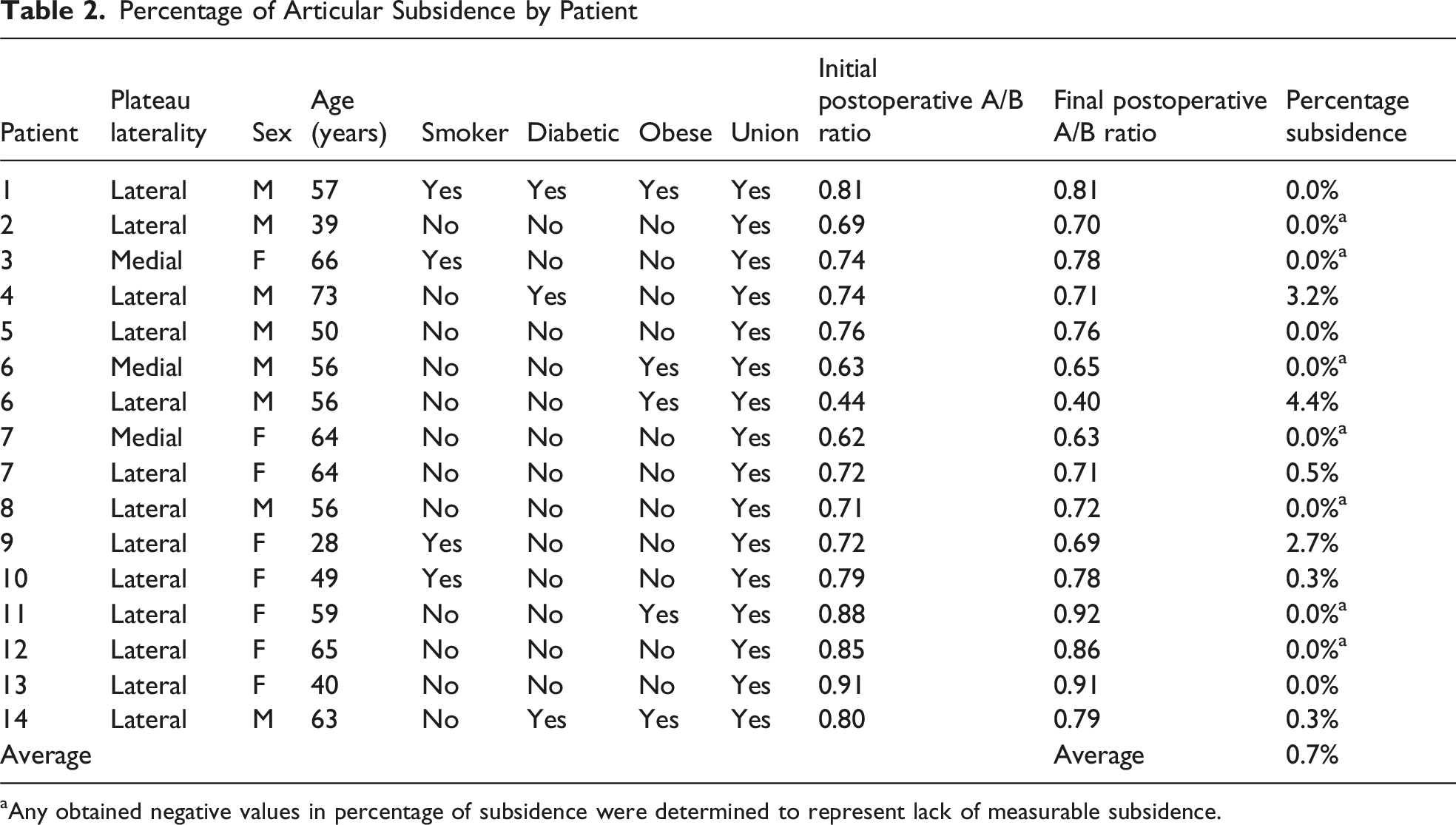
aAny obtained negative values in percentage of subsidence were determined to represent lack of measurable subsidence.
Discussion
Despite maintaining several advantages compared to autograft, application of allograft augmentation in the operative management of depressed tibial plateau fractures may still be limited by inefficient technique resulting in increased operative time and surgeon frustration.23,24 This present study sought to describe a feasibly applicable technique for allograft administration in the setting of depressed tibial plateau fracture management. While other bone substitutes such as demineralized bone matrix products may offer a variety of tools to assist with delivery of these products, this study focused solely on cancellous allograft delivery strategies with the goal of maintaining the benefits of this supplement inclusive of the osteoconductive and mechanically supportive benefits of crushed cancellous autograft while keeping costs to a minimum. 11 In this case series, patients underwent allograft implantation via modified syringes that may be readily available and cost effective in the operative setting. Throughout the follow-up period, all cases demonstrated radiographic evidence of graft incorporation. Further, there was a very low degree of average subsidence at 0.7% with the greatest percentage of subsidence in this series measuring 4.4% indicating minimal-to-no joint subsidence by one year follow-up. These findings highlight the ability of the cancellous autograft to provide structural support in the short term and while providing osteoconductive properties to facilitate bone ingrowth in the long term.
Our method of using a ratio between two screw positions and the articular surface allows for evaluation of joint depression while minimizing the effect of confounding variables such as X-ray beam angulation differences and magnification changes. This measurement assumes that the distance between the two screws remains unchanged throughout the study and any failure of the implants would result in skewed measurements. In our case series, the surgical implants remained well-aligned throughout all time points without evidence of failure or loosening. As a result, we feel that our method of measurement offers the best objective evaluation of joint subsidence without using computed tomography scans.
Limitations of the present study include the small sample size, which may be exacerbated in applying these findings to medial plateau fractures, and use of single-surgeon data which may limit the generalizability of these results. However, our population was fairly representative of general tibial plateau fractures as reported in the literature. Elsoe et al (2015) reported an average age of patients suffering tibial plateau fractures of 52.6 years, while this study reported an average age of 54.6 years. 2 Further, Elsoe et al (2015) noted AO type 41-B3 and 41-C3 to represent the most common variations of tibial plateau fractures reported, similar to the present population in this study. 2 Additional limitations present may include confounding factors in this patient population that are not able to be elucidated, such as variations in screw joint distance as reported by Ye et al (2019) that may lead to altered experiences across surgeons. 25 Yet, this limitation may be positively influenced by the nature of this case series being a single-surgeon study. Finally, while the required duration of radiographic follow-up of this study may add strength to these findings, a large proportion of patients were not able to be included due to loss to follow-up which may introduce inherent bias.
In areas of future study, functional outcomes of patients undergoing this or similar grafting techniques may be beneficial in bolstering clinical meaning to the radiographic findings noted in this initial study. Additionally, future studies may also benefit from collecting “grafting time” intraoperatively as this would help verify the efficiency of this technique. While our study did not routinely collect computed tomography (CT) scans at 12-month follow-up, in future studies, if feasible, comparison of CT scans could be beneficial for further validation of the findings noted in this present study.
Conclusion
Allograft utilization in the management of depressed tibial plateau fractures is known to improve postoperative outcomes, especially with respect to rates of subsidence. However, implantation of the crushed, cancellous allograft into the metaphyseal defect can be cumbersome. In this case series, we have described an effective, efficient, and novel method of filling the metaphyseal defect created after restoring articular depression in tibial plateau fractures.
Footnotes
Author Contributions
Hartman T, Cavallaro S, Reiser J: Design of the work. Hartman T, Cavallaro S, Reiser J: Acquisition of the data. Hartman T, Cavallaro S, Reiser J, Mumtaz S: Analysis and interpretation of the data. Hartman T, Cavallaro S, Reiser J, Mumtaz S: Drafting. Hartman T, Cavallaro S, Reiser J, Sullivan M: Important intellectual content. All the authors have approved the final version of the manuscript to be published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
This study was exempt from requiring Institutional Review Board approval due its nature as a retrospective chart review in addition to maintained anonymity of included patients.