
Abstract
Background
Accurate preoperative staging of peritoneal carcinomatosis (PC) is crucial for planning cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). However, conventional imaging often underestimates disease burden. This study evaluated whether three-dimensional (3D) reconstruction based on multimodality imaging improves estimation of the peritoneal cancer index (PCI) compared with CT.
Methods
We conducted a retrospective analysis of patients with PC undergoing CRS–HIPEC between February 2022 and February 2025. Preoperative imaging included contrast-enhanced CT and multimodality-based 3D reconstruction (CT, MRI, PET). Imaging-derived PCI (CT-PCI and 3D-PCI) was compared with surgical PCI (reference standard). The primary endpoint was the signed difference (PCI_ref − PCI_index). Agreement was assessed using Bland–Altman analysis. Region-level diagnostic performance (sensitivity, specificity, PPV, NPV) was evaluated.
Results
Among 62 patients undergoing 3D reconstruction, 42 were included in the final analysis. The median signed difference between imaging and surgical PCI was lower for 3D than for CT (2.0 vs 3.0), although not statistically significant (P = 0.101). Bland–Altman analysis showed a slightly lower mean bias for 3D compared with CT (+5.3 vs +6.2), indicating a tendency toward underestimation by both modalities. Region-level analysis demonstrated high specificity (>90%) but limited sensitivity, particularly in anatomically challenging areas such as the mesenteric root and small-bowel serosa.
Conclusions
Multimodality-based 3D reconstruction may improve PCI estimation compared with CT alone, although differences were not statistically significant. Both approaches showed limited sensitivity in critical regions. These findings are exploratory and highlight the need for prospective validation.
Introduction
Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) play an increasingly important role in the treatment of peritoneal carcinomatosis (PC), marking a paradigm shift in the management of this disease. However, despite recent advancements in radiological imaging, an accurate preoperative assessment of peritoneal disease-related burden remains a significant clinical challenge. 1
Conventional imaging modalities—including computed tomography (CT) scan, magnetic resonance imaging (MRI), and positron emission tomography (PET)—often have a limited sensitivity in detecting small peritoneal metastases or differentiating them from postoperative changes, fibrosis, or benign lesions. Further, the evaluation of disease extent based on these techniques is subject to considerable interobserver variability, particularly when estimating the peritoneal cancer index (PCI). 2 As a result, diagnostic laparoscopy remains essential in most cases for definitive preoperative staging. 3
In relation to this, three-dimensional (3D) imaging has emerged as a potential tool that can allow precise anatomical visualization and enhanced surgical planning. However, its application in peritoneal surface malignancies remains limited.4,5
The present study evaluates a multimodality 3D reconstruction workflow as a complementary tool to conventional CT imaging and it aims to explore the potential role of 3D reconstruction in PCI estimation by comparing the PCI obtained via 3D modeling with that derived from conventional CT scan and intraoperative assessment, the feasibility, reliability, and potential added value of this approach in optimizing surgical strategy were assessed.
Material and Methods
Selection of Patients
This retrospective study was conducted at Sanchinarro University Hospital from February 2022 to February 2025. Patients with PC who underwent CRS and HIPEC during the study period were retrospectively analyzed. Each patient underwent standard preoperative imaging and 3D reconstruction. The Ethics Committee of Sanchinarro Hospital approved this study. All experiments were performed in accordance with the relevant guidelines and regulations (such as the Declaration of Helsinki). Informed consent was obtained from all participants of this study.
Preoperative Study
All clinical cases described in this study were discussed by a multidisciplinary committee. The results of the comprehensive blood chemistry, including tumor markers (carcinoembryonic antigen, cancer antigen [CA] 19.9, CA 125, CA 15.3, alpha fetoprotein, chromogranin A, and neuron-specific enolase), were used in the patient evaluations. All patients were then subjected to a general evaluation that included cardiological tests (cardiology visit, baseline electrocardiogram, and second-level tests on request), respiratory function assessment (blood gas analysis, respiratory function tests if requested), and kidney function tests. The anesthetic risk was assessed according to the American Society of Anesthesiologists scoring system (the cardiac risk index by Goldman).
Each preoperative imaging study was conducted with conventional CT scan, entero-MRI, and PET-CT scan or entero-PET-MRI). 3D imaging reconstruction with the 3D Cella Medical Solutions (3D-MSP®) models performed for each patient.
This study was designed and reported in accordance with the STARD (Standards for Reporting Diagnostic Accuracy Studies) guidelines.
Acquisition and Processing of 3D-MSP® Imaging
A preoperative 3D reconstruction was generated for each patient using the 3D-MSP® platform developed by Cella Medical Solutions. Figure 1 shows the reconstruction workflow. Three-dimensional model of peritoneal carcinomatosis with PCI calculated before (A) and after (B) neoadjuvant treatment. Detail of three-dimensional model of the same patient with before (C) and after neoadjuvant treatment (D)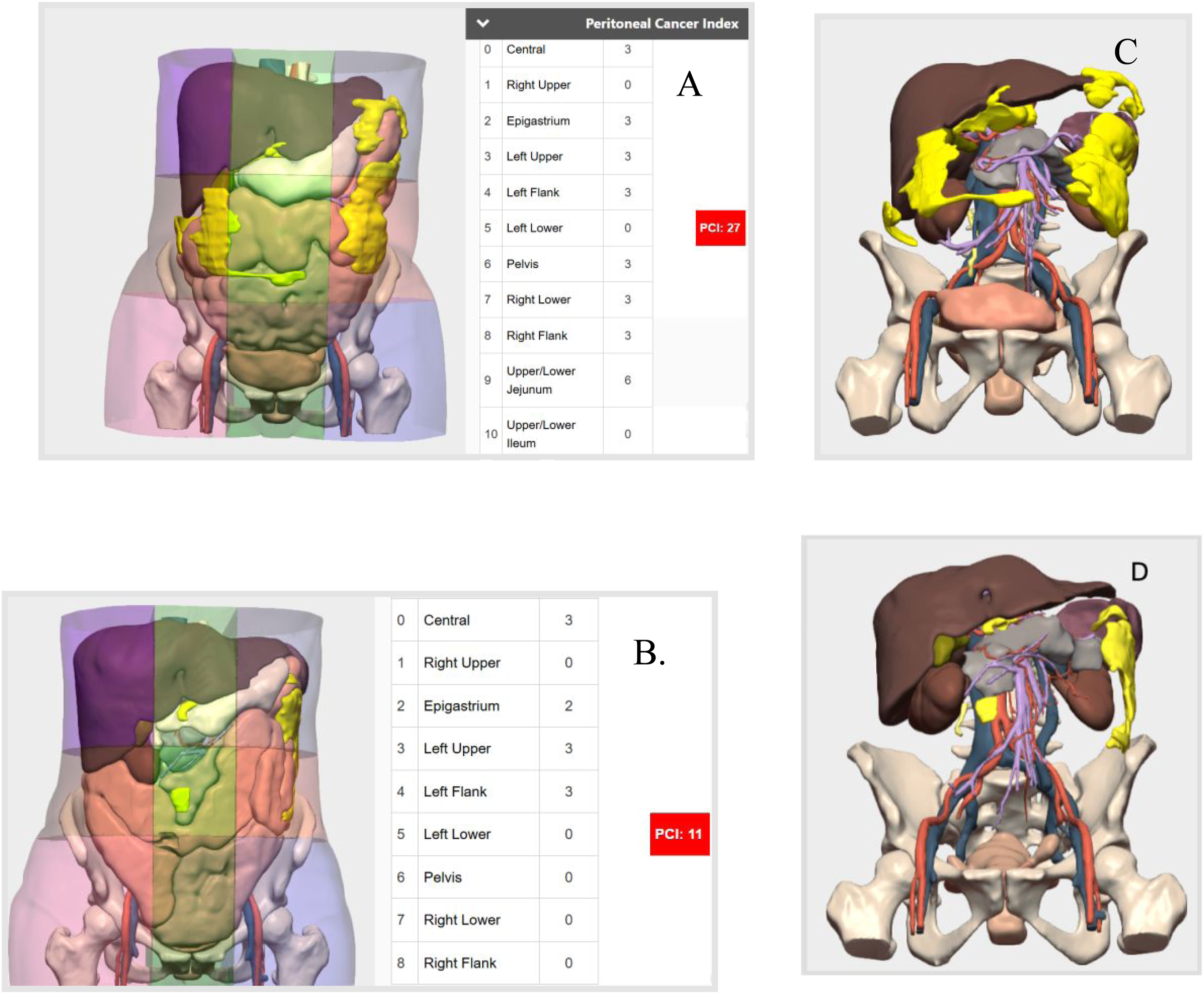
Three-Dimensional Imaging Acquisition Methods
Data Acquisition
To create 3D models, CT scan, MRI, PET-CT, or PET-MRI was analyzed and used for data acquisition. The data were exported in the Digital Imaging and Communication in Medicine format, anonymized, and later distributed via the Picture Archiving and Communication System.
Image Fusion
The image coregistration techniques enable the merging of different functional and anatomical modalities (eg, PET.RM and TAC), attributing a different amount of information in proportion. Register algorithms are used with linear or rigid transformation on the global nature of the lesion and elastic or nonrigid transformations for the local deformations of the image elements.
Image Pre-Processing and Segmentation
In the first phase of image processing, noise and artifacts are reduced by using anisotropic diffusion filters and normalizing the intensity through the N3 algorithm (nonparametric nonuniform intensity normalization) with the aim of delimiting the edges of the structures with ease. In the standard protocol, segmentation of the tumor or tumors, vascular structures, and neighboring organs is performed if required for interventional planning. The segmentation algorithms include active contour techniques and adaptive region growth.
Processing of Modeling
To reduce segmentation due to the different cuts of the imaging techniques, Laplacian filters were used. Finally, the models were processed to add interactive features, such as the distribution of the tumor implant in the abdominal quadrants according to the Sugar Baker classification, and the PCI was calculated.
Representative images were included to show the utility of 3D reconstruction (Figures 1 and 2 and video 1 and 2). Preoperative imaging of a patient with local and peritoneal recurrence of rectal adenocarcinoma three years after primary surgery. (A) Estimated peritoneal carcinomatosis index (PCI). (B) Relationship of recurrent disease with retroperitoneal vascular structures. (C) Relationship of recurrent disease with small and large bowel loops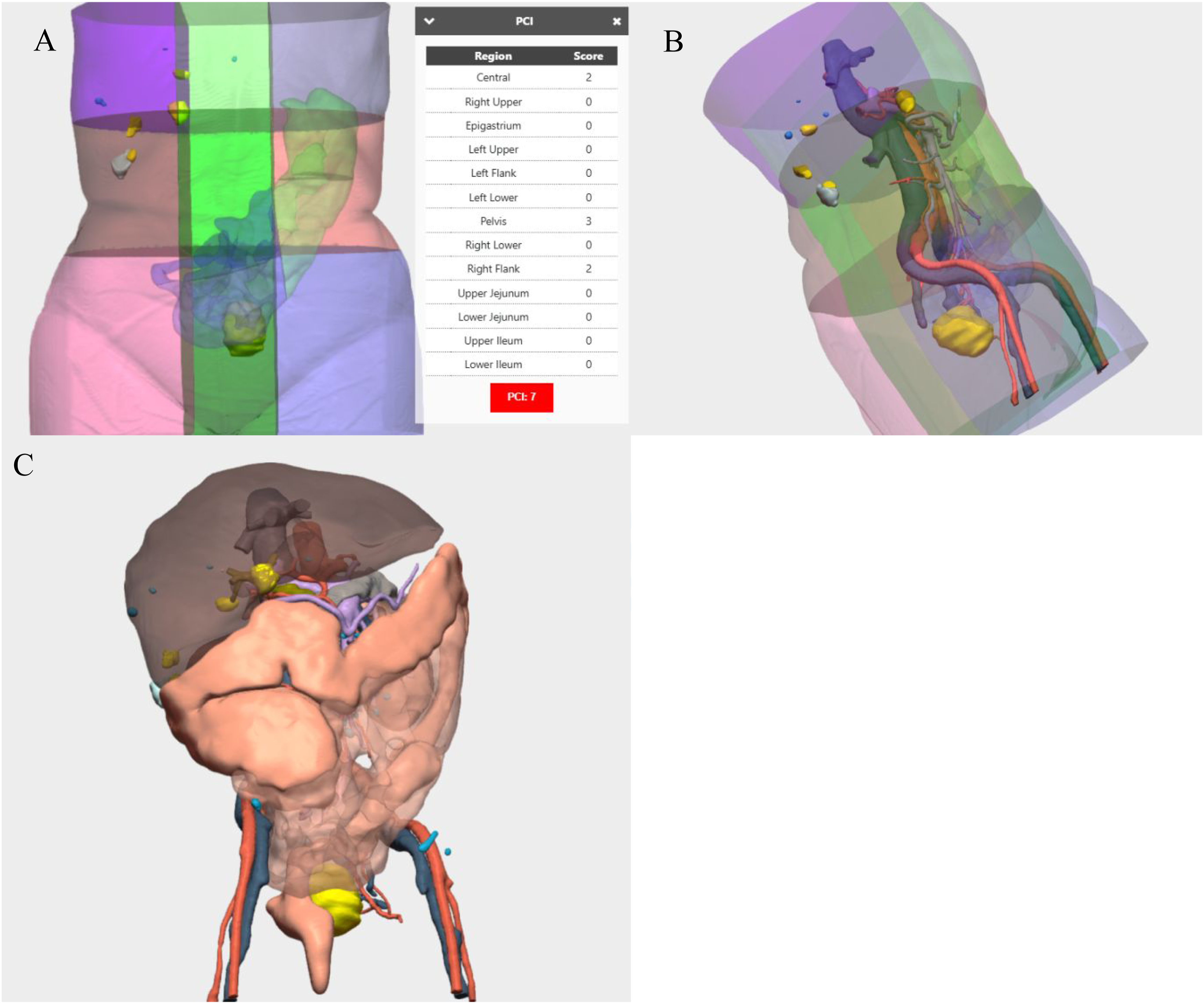
The median time required to complete the full reconstruction is approximately 7-10 days. However, in urgent cases, the turnaround time can be reduced to within 24 h.
Standard CT Interpretation
Imaging interpretation and PCI assessment of CT was performed by board-certified radiologists with specific expertise in peritoneal surface malignancies, with more than 20 years of experience and having evaluated more than 300 cases of peritoneal carcinomatosis.
Primary Endpoint
In this study, the primary end point was the accuracy of the preoperative 3D reconstruction in estimating the PCI, using the intraoperative surgical PCI as the reference standard and to compare it with the accuracy of standard CT scan imaging.
Secondary Endpoint
The secondary end points were sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the accuracy of CT scan and 3D reconstruction in detecting peritoneal metastases.
Statistical Analysis
Considering the non-normal distribution of the data, as determined using the Shapiro–Wilk test, the results were expressed as median values with corresponding ranges. Categorical data were presented as percentages.
For paired data, the non-parametric Wilcoxon signed-rank test was used to calculate and compare signed difference between PCI (CT) and PCI (Ref) (PCI (Ref) - PCI(CT)) and between PCI (3D) and PCI (Ref) (PCI (Ref) - PCI (3D)). Positive values indicate underestimation of PCI by imaging, whereas negative values indicate overestimation.
The frequency of underestimation—defined as an imaging-derived PCI lower than the surgical PCI, was calculated for each modality and expressed as a proportion of the total cohort. An agreement analysis between imaging and surgical PCI was further conducted using the Bland–Altman method. Bland–Altman plots were constructed to visualize systematic bias and the limits of agreement for each imaging technique.
The sensitivity, specificity, PPV, NPV, and accuracy for each imaging set and for each reader were calculated in a binary fashion (presence or absence of peritoneal metastases).
All statistical tests were two-tailed, and a P value of < 0⋅050 indicated statistically significant differences.
Results
Characteristics of the Patients
From January 2022 to February 2025, 62 3D imaging studies were carried out to evaluate for PC (Figure 3). Of all the patients, eight underwent two separate 3D reconstructions, one before and one after neoadjuvant therapy. This allowed for a direct comparison of disease burden and treatment response. In addition, 12 patients did not undergo surgery based on clinical judgment. Patient flow and eligibility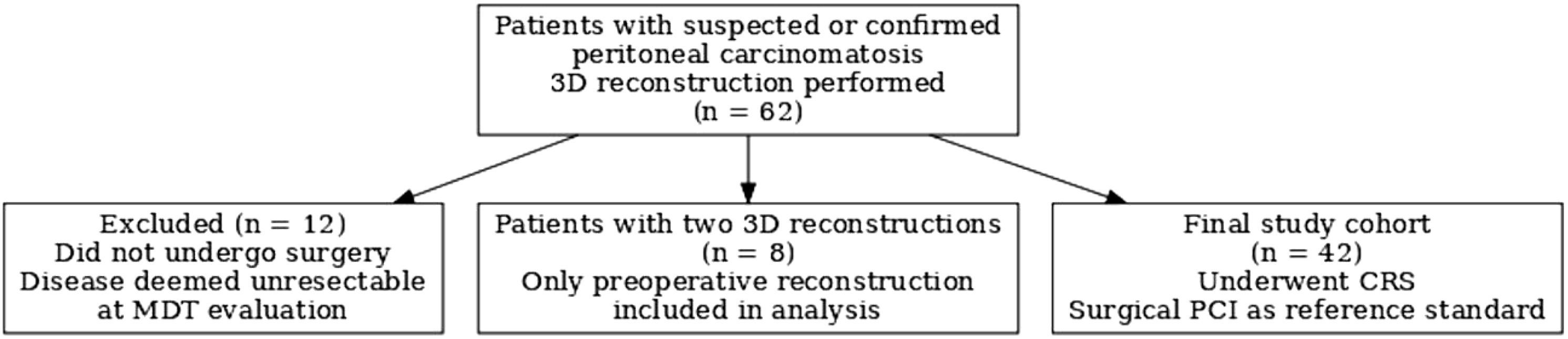
Finally, 42 patients, including 16 men and 26 women, with a median age of 62 years, were prospectively included and analyzed in this study.
The primary tumors were ovarian serous carcinoma (30.9%), non-mucinous adenocarcinoma of the colon (40.4%), pseudomyxoma peritonei (11.9%), gastric non-mucinous adenocarcinoma (7.1%), mesotelioma (2.3%), and pathology with no conventional indication (7.1%).
Estimation of the PCI
A descriptive analysis showed that the median absolute difference between 3D reconstruction and the surgical PCI was slightly lower than that of CT scan (Figure 4). In fact, the absolute difference (PCI (Ref) - PCI (3D)) was smaller than the absolute difference (PCI (Ref) - PCI(CT)) (median [range]: 2.0 [–7 to 28] vs 3.0 [–7 to 30]; (P = 0.101). Box plot showing the differences between the PCI calculated with 3D models and the surgical reference, compared to the differences between the PCI calculated with standard CT and the surgical reference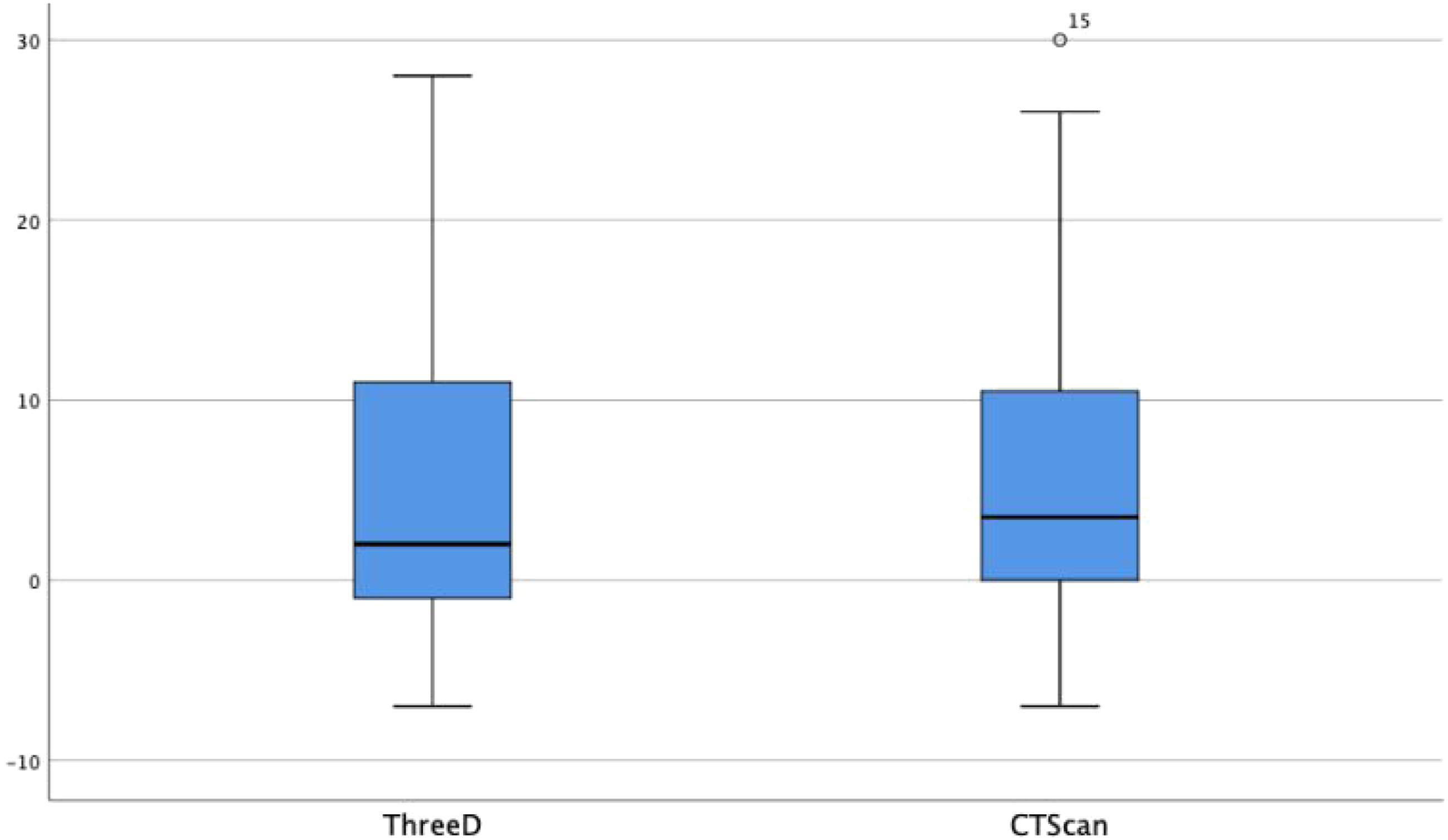
The Wilcoxon signed-rank test revealed a trend toward statistical significance in favor of 3D reconstruction (P = 0.101), indicating a potential improvement in accuracy.
Based on these findings, 3D reconstruction may provide a closer estimation of the surgical PCI than CT scan alone, particularly in reducing significant deviations in cases of extensive peritoneal disease.
Bland-Altman Analysis
A Bland-Altman analysis was performed to assess the agreement between imaging-based PCI and the surgical PCI. CT scan alone was more likely to underestimate the PCI, with a median difference of 6.2 (range: −11 to +23) (Figure 5). Meanwhile, 3D reconstruction also showed a tendency toward overestimation but to a lesser extent, with a median difference of 5.3 (range: −11,2 to +24) (Figure 6). Bland- Altman plot illustrating the agreement between CT scan-based reconstruction and surgical PCI Bland-Altman plot illustrating the agreement between 3D scan reconstruction and surgical PCI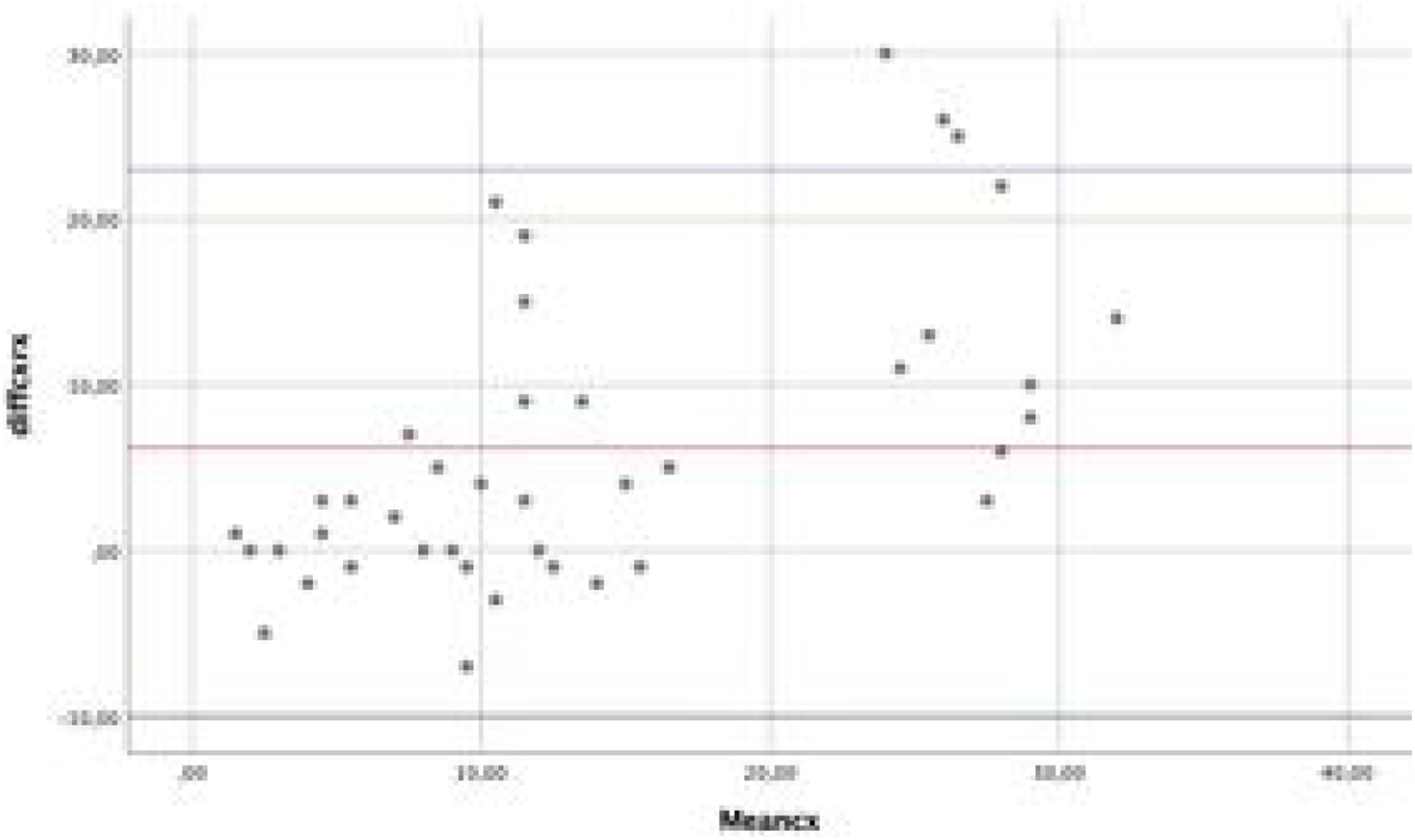
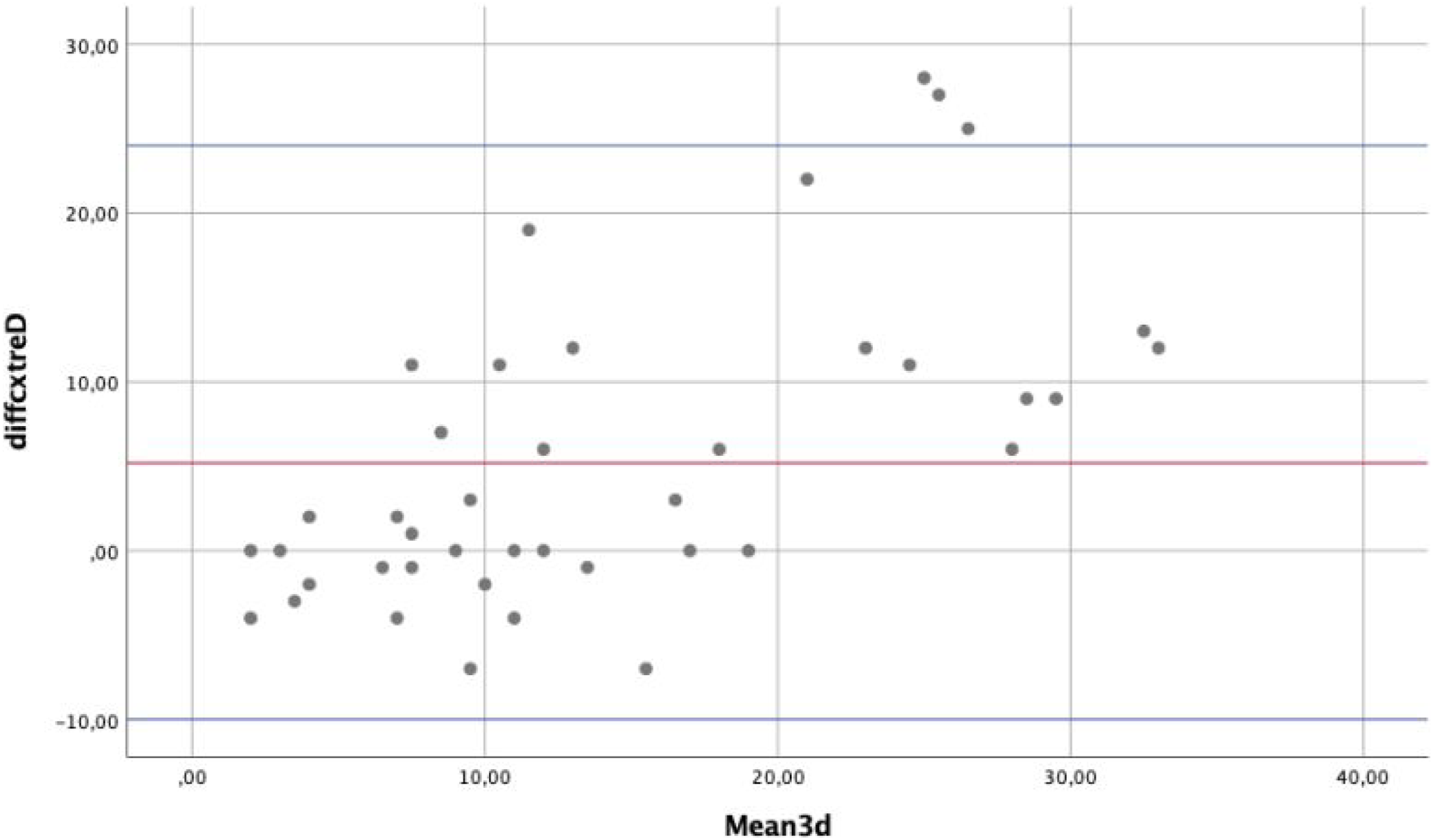
According to these findings, both modalities systematically underestimate the extent of peritoneal disease. However, 3D reconstruction may offer a slightly closer estimation to the surgical reference.
Estimation of the PCI
Detection Rate of Peritoneal Metastases Across the Different Anatomical Regions for CT Scan and 3D Comparing With Surgical Examination
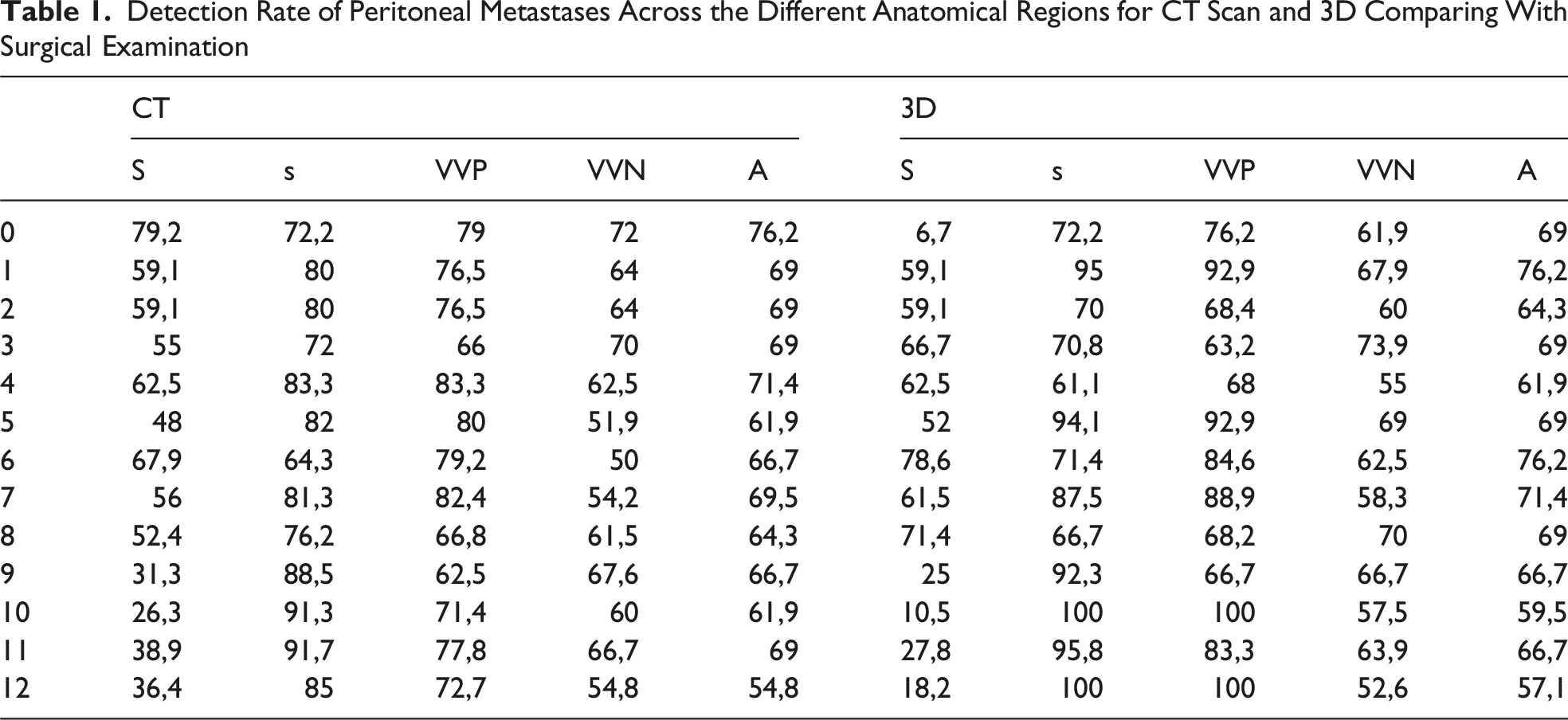
For regions 10 (mesenteric root) and 12 (small bowel serosa), the sensitivity remained significantly low even with 3D, even if the specificity reached 100%.
Discussion
Accurate preoperative staging of peritoneal carcinomatosis (PC) remains challenging due to the significant diagnostic limitations of current imaging modalities, especially in detecting small-volume disease. 6 Multidetector CT is still the first-line tool because of its accessibility, but its sensitivity for subcentimeter peritoneal metastases—particularly on the intestinal serosa, mesentery, and subphrenic spaces—remains low. 7 MRI, especially diffusion-weighted sequences, offers higher sensitivity for lesions ≥3-5 mm in selected cohorts, yet still falls short in reliably characterizing the full extent of disease. 8 PET-CT provides complementary metabolic information and may detect occult nodal or peritoneal metastases, though its diagnostic accuracy is hampered by false positives (inflammation) and false negatives in non-FDG-avid or microscopic disease.9,10 More recently, hybrid PET-MRI has shown improved sensitivity and better correlation with surgical PCI, with high accuracy in identifying patients with heavy tumor burden (PCI >21). 11
Despite these advances, no modality can consistently and accurately stage PC preoperatively, underscoring the persistent difficulty of estimating true disease extent before surgery.
The integration of 3D imaging technologies—such as the 3D-MSP® platform evaluated in our study—represents a natural evolution toward improving diagnostic accuracy and surgical planning. These tools generate interactive, anatomically precise models from CT scan or MRI via the segmentation of key structures such as the organs, vessels, and tumors. Their clinical utility is well established in the field of digestive tract oncology. In colorectal cancer, they enhance the understanding of complex anatomy. 12 In pancreatic tumors, they help assess vascular involvement and resectability. 13 In liver surgery, they support accurate resections and risk assessment.14,15 Notably, Vicente et al have shown that combining liver modeling with functional evaluation can predict postoperative liver failure and guide major hepatectomy procedures. 16 Three-dimensional reconstruction based on multimodality imaging may improve PCI estimation compared with CT alone.
However, its application to PC remains extremely limited. To date, only one clinical case report has shown the use of 3D modeling in this setting. Gomes da Costa et al described the use of a 3D-MSP® model in recurrent ovarian cancer, which allowed an accurate localization of peritoneal metastases and facilitated complete cytoreduction. 17 This emphasizes the potential of 3D imaging as a valuable tool for preoperative navigation and decision-making in selected complex peritoneal surface malignancies—an area that should be further investigated. The current study described the most extensive experience reported in the literature on the use of 3D reconstructions in PC; this study should be interpreted as an exploratory, hypothesis-generating analysis rather than a definitive assessment of diagnostic performance.
The 3D reconstruction method yielded a median absolute difference of 2.0 points from the surgical PCI (range: −7 to 28). Meanwhile, the CT-based estimates yielded a median absolute difference of 3.0 points (range: −7 to 30) (P = 0.101). This finding indicates a trend toward a higher accuracy with 3D modeling. The Bland-Altman analysis further supported these findings. In particular, CT scan was more likely to underestimate the PCI, with a median of 6.2 points (range: −11 to +23). Meanwhile, 3D reconstruction had a slightly lower median overestimation of 5.3 points (range: −11.2 to +24).
According to an analysis of 546 surgically confirmed peritoneal regions, 3D reconstruction had a good detection rate for peritoneal metastases. However, specific regions remained problematic: the mesenteric root (region 10) and small-bowel serosa (region 12) had a persistently low sensitivity despite having a specificity of 100%.
Finally, an accurate preoperative stratification is essential in the management of peritoneal surface malignancies. Patients are often selected for cytoreductive surgery and HIPEC based on the disease extent, which is significantly difficult to assess with conventional imaging alone. In this context, 3D reconstruction has emerged as a promising tool that can enhance preoperative staging and guide clinical decision-making. Its ability to spatially reconstruct disease burden may facilitate a better surgical planning and reduce the number of futile laparotomies.
Three-dimensional modeling may represent the future gold standard for preoperative visualization in complex oncologic cases. This is because it enables the integration of data from multiple imaging modalities into a single, coherent reconstruction. Its actual value lies in the precision and quality of the different imaging modalities, and in the ability to combine anatomical, functional, and—in the future—molecular data. To achieve a truly reliable diagnosis and surgical roadmap, these models must incorporate information, including clinical findings, intraoperative observations, and histopathological data, to the greatest extent possible. This integrative approach enhances the accuracy and completeness of the models, moving closer to a 100% reliable diagnostic and planning tool.
Based on our opinion, 3D reconstruction in PC is beneficial in cases requiring multivisceral resections. The integration of all available imaging data into a single 3D model offers exceptional anatomical accuracy, thereby effectively serving as a surgical GPS for the operating team and improving intraoperative safety. Simultaneously, this level of detail reinforces the quality of preoperative patient counseling, facilitating a clearer communication and more realistic expectations regarding the surgical procedure.
Equally important, providing patients access to 3D reconstruction fosters a deeper understanding of their condition—which is particularly valuable in complex pathologies such as this—and the extensive surgical treatment it requires. This improved understanding enhances the overall quality of care, promotes adherence to treatment plans, and fosters active participation in shared decision-making. Being well-informed enables patients to approach the postoperative period with greater assurance and fewer uncertainties.
In the future, radiomics and artificial intelligence represent the next frontier in imaging-based precision medicine. Their integration into 3D modeling has significant potential for quantitatively characterizing tissue heterogeneity, thereby improving the assessment of tumor metastasis and response to neoadjuvant therapy.18,19 Radiomic features extracted from standard imaging sequences could be objective biomarkers that can support individualized treatment strategies.
Moreover, the incorporation of clinical, intraoperative, and histopathological data into artificial intelligence-based neural networks may enable advanced pattern recognition and segmentation, thereby allowing the detection of subtle peritoneal metastases often missed by conventional radiology. These developments can ultimately reduce or eliminate the need for invasive diagnostic procedures—such as exploratory laparoscopies—by offering a standardized, reproducible, and noninvasive assessment of peritoneal diseases.
In this context, novel imaging techniques such as PET with fibroblast activation protein inhibitors (FAPIs) represent a promising advancement that can be integrated into a 3D model. Unlike traditional FDG PET, FAPI PET targets the fibroblast activation protein overexpressed in cancer-associated fibroblasts, which are abundant in several gastrointestinal tumors. This approach may improve lesion detection in tumors with a low metabolic activity or small size. Preliminary studies have reported that FAPI PET/CT scan may significantly outperform FDG PET/CT scan in identifying PC (97.7% vs 72.1%). 20
This study has several limitations that should be acknowledged. First, the relatively small sample size limited the statistical power and generalizability of the results. Second, the retrospective nature of data collection might have introduced selection bias and limited the standardization of imaging protocols across patients. Despite these limitations, this study performed first substantial series showing the potential clinical application of 3D reconstruction in a disease as complex as PC.
Conclusion
Three-dimensional reconstruction can potentially enhance preoperative PCI estimation and improve the spatial mapping of peritoneal metastases compared with conventional CT scan.
Supplemental Material
Supplemental Material
Footnotes
Ethical Considerations
The Ethics Committee of Sanchinarro Hospital approved the current study. All experiments were performed in accordance with the relevant guidelines and regulations (such as the Declaration of Helsinki).
Consent to Participate
Informed consent was obtained from all study participants.
Author Contributions
Eduardo Diaz, Emilio Vicente and Yolanda Quijano conceived the study and supervised all stages of the project. Hipolito Duran, Isabel Fabra, Luis Malave, Pablo Ruiz, and Gabriel Garabote contributed to patient recruitment and clinical management. Luca Ballelli, Alessandro Broglio, Gianvito Varvaro, and Alessandro Sirotti contributed to surgical data collections Lina García Cañamaque and Laura Arrieta contributes to specialized expertise in radiological assessment, and imaging interpretation. Riccardo Caruso and Valentina Ferri performed the statistical analyses and drafted the initial version of the manuscript. All authors critically revised the manuscript, contributed with substantial intellectual input, and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the data collected for this study, requests to access the dataset from qualified researchers trained in human subject confidentiality protocols may be sent to Valentina Ferri at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.