
Abstract
Purpose
This study aimed to compare the outcomes of laparoscopic Ladd’s procedure (LL) and open Ladd’s procedure (OL) for the treatment of intestinal malrotation in infants and children, focusing on operative parameters, postoperative recovery, and complications through a systematic review and meta-analysis.
Methods
A comprehensive literature search of PubMed, Embase, Web of Science, and the Cochrane Library was conducted up to June 2025 following PRISMA guidelines. Studies comparing LL and OL in pediatric patients (<18 years) were included. Data were analyzed using Review Manager 5.4. Mean differences (MD) and odds ratios (OR) with 95% confidence intervals (CI) were calculated using fixed- or random-effects models depending on heterogeneity.
Results
Eighteen studies including 3479 patients (LL: 928; OL: 2551) met the inclusion criteria. There was no significant difference in operative time between LL and OL (MD = 9.14, 95% CI: −4.01–22.28; P = 0.17). However, LL showed shorter time to full intake (MD = −2.64 days; P < 0.001) and shorter hospital stay (MD = −3.19 days; P < 0.001). LL was associated with lower rates of adhesive bowel obstruction (OR = 0.44; P < 0.001) and overall complications (OR = 0.39; P < 0.001), but higher rates of postoperative volvulus (OR = 3.26; P = 0.002) and reoperation (OR = 1.67; P = 0.03).
Conclusions
Laparoscopic Ladd’s procedure offers advantages in postoperative recovery and reduced complication rates compared with the open approach, though it may carry a higher risk of volvulus and reoperation.
Introduction
Intestinal malrotation is a congenital anomaly resulting from abnormal rotation and fixation of the midgut during embryologic development.1-3 It can lead to life-threatening complications such as midgut volvulus and intestinal ischemia if left untreated. The Ladd’s procedure, first described by William Ladd in 1936, remains the standard surgical treatment for this condition.4,5 Traditionally, this operation has been performed via an open approach, allowing direct visualization and correction of the malrotation. However, with the advancement of minimally invasive techniques, laparoscopic Ladd’s procedure (LL) has increasingly been adopted in pediatric surgery as an alternative to the conventional open Ladd’s procedure (OL).6,7
Several studies have reported the potential benefits of the laparoscopic approach, including smaller incisions, reduced postoperative pain, faster recovery, and shorter hospital stays.8,9 Nonetheless, concerns remain regarding its technical complexity, longer operative time, and a possibly higher risk of postoperative volvulus or reoperation. 8 Due to the relative rarity of intestinal malrotation and the predominance of single-center retrospective studies, evidence comparing LL and OL in infants and children remains inconsistent.
To address these inconsistencies and provide a comprehensive evaluation, we conducted a systematic review and meta-analysis comparing laparoscopic and open Ladd’s procedures in infants and children with intestinal malrotation. By pooling data from available studies, this analysis aims to assess perioperative outcomes, postoperative recovery, and complication profiles between the two techniques.
Materials and Methods
Literature Search Strategy
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was performed across PubMed, Embase, Web of Science, and the Cochrane Library databases to identify relevant studies published up to June 2025. The search terms included combinations of “Ladd’s procedure,” “intestinal malrotation,” “laparoscopic,” “open surgery,” “infants,” and “children.” Reference lists of relevant articles were also manually screened to identify additional studies. After removing duplicates, titles and abstracts were reviewed, and full texts were retrieved for articles that met the initial inclusion criteria.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: (1) patients were infants or children (<18 years) diagnosed with intestinal malrotation; (2) the intervention compared laparoscopic Ladd’s procedure (LL) with open Ladd’s procedure (OL); (3) at least one of the following outcomes was reported: operative time, time to full intake, length of hospital stay, postoperative complications, adhesive bowel obstruction, postoperative volvulus, or reoperation; and (4) the study design was randomized controlled, prospective, or retrospective cohort. Studies were excluded if they (1) lacked comparative data between LL and OL, (2) included adult patients, (3) were case reports, reviews, or conference abstracts, or (4) had incomplete or overlapping data. Data extraction and selection were performed independently by two reviewers, with discrepancies resolved by consensus or a third reviewer.
Data Extraction and Statistical Analysis
From each included study, data on author, publication year, study design, country, sample size, patient demographics, surgical approach, and reported outcomes were extracted. The primary outcomes were operative time, time to full intake, and length of hospital stay; secondary outcomes included adhesive bowel obstruction, postoperative volvulus, reoperation, and overall complications. Meta-analyses were performed using Review Manager (RevMan) version 5.4. For continuous variables, mean differences (MDs) with 95% confidence intervals (CIs) were calculated; for dichotomous variables, odds ratios (ORs) with 95% CIs were used. Heterogeneity among studies was assessed using the I2 statistic, with I2 > 50% indicating significant heterogeneity, in which case a random-effects model was applied; otherwise, a fixed-effects model was used.
Results
Study Selection and Characteristics
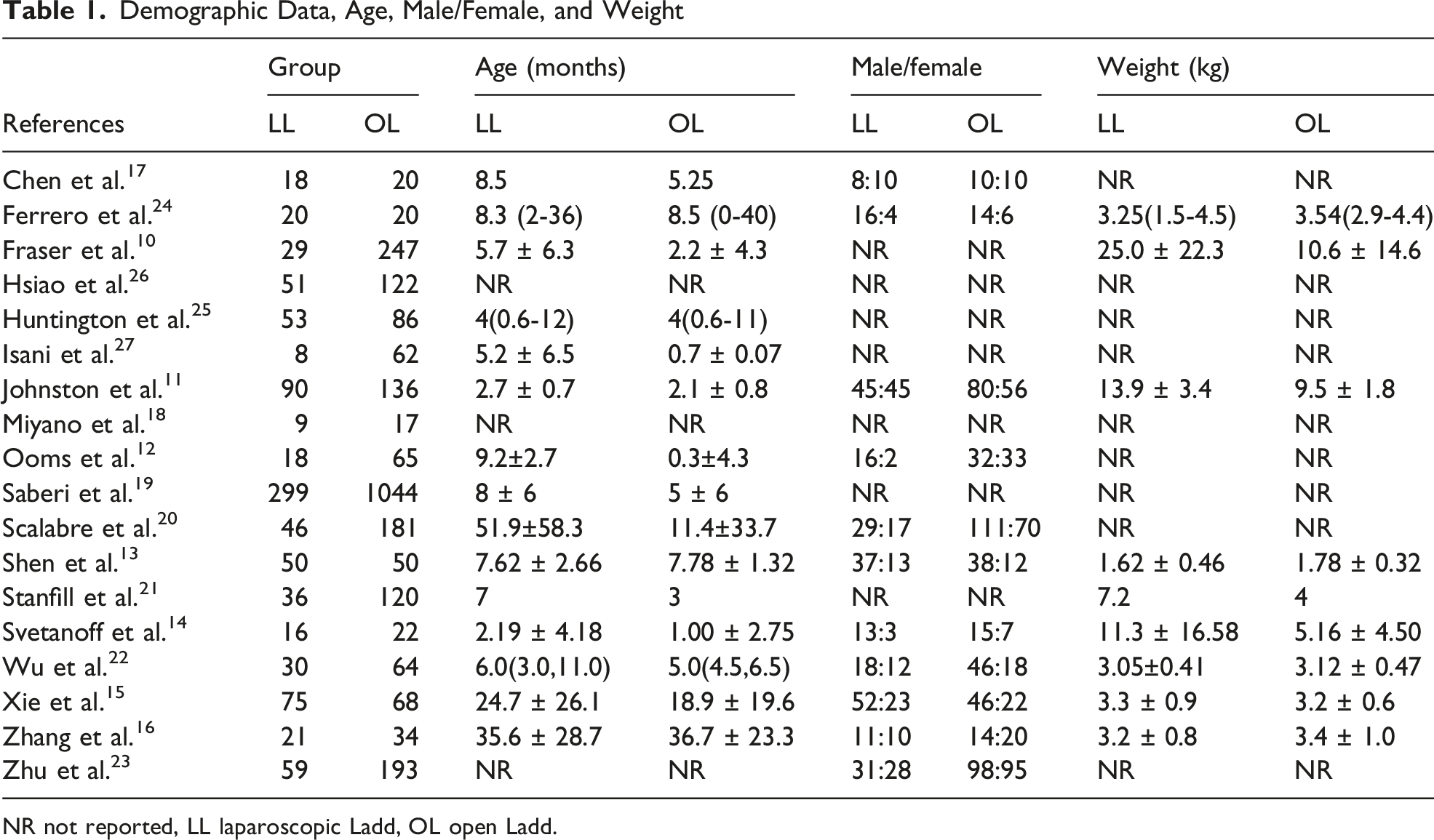
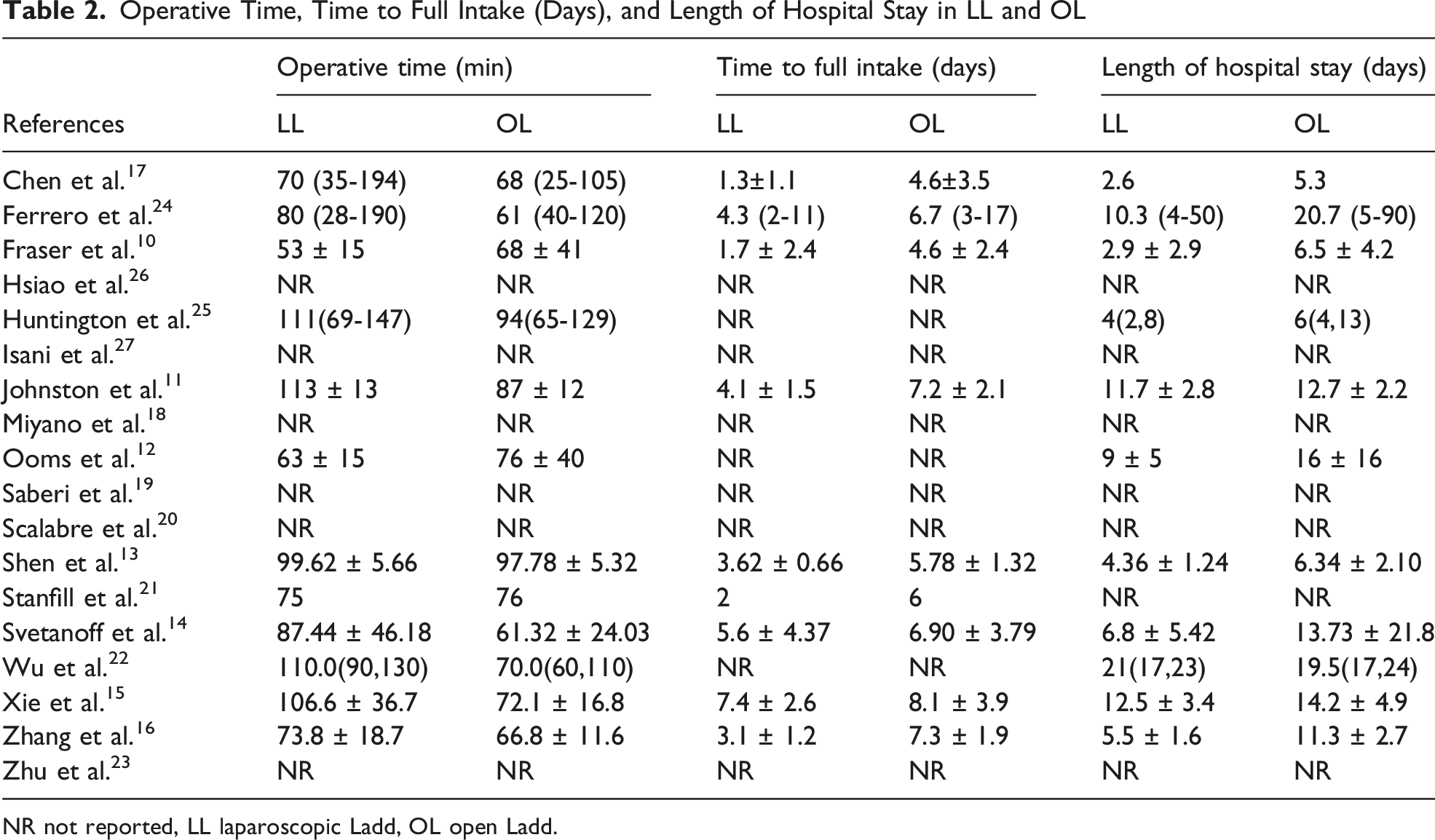
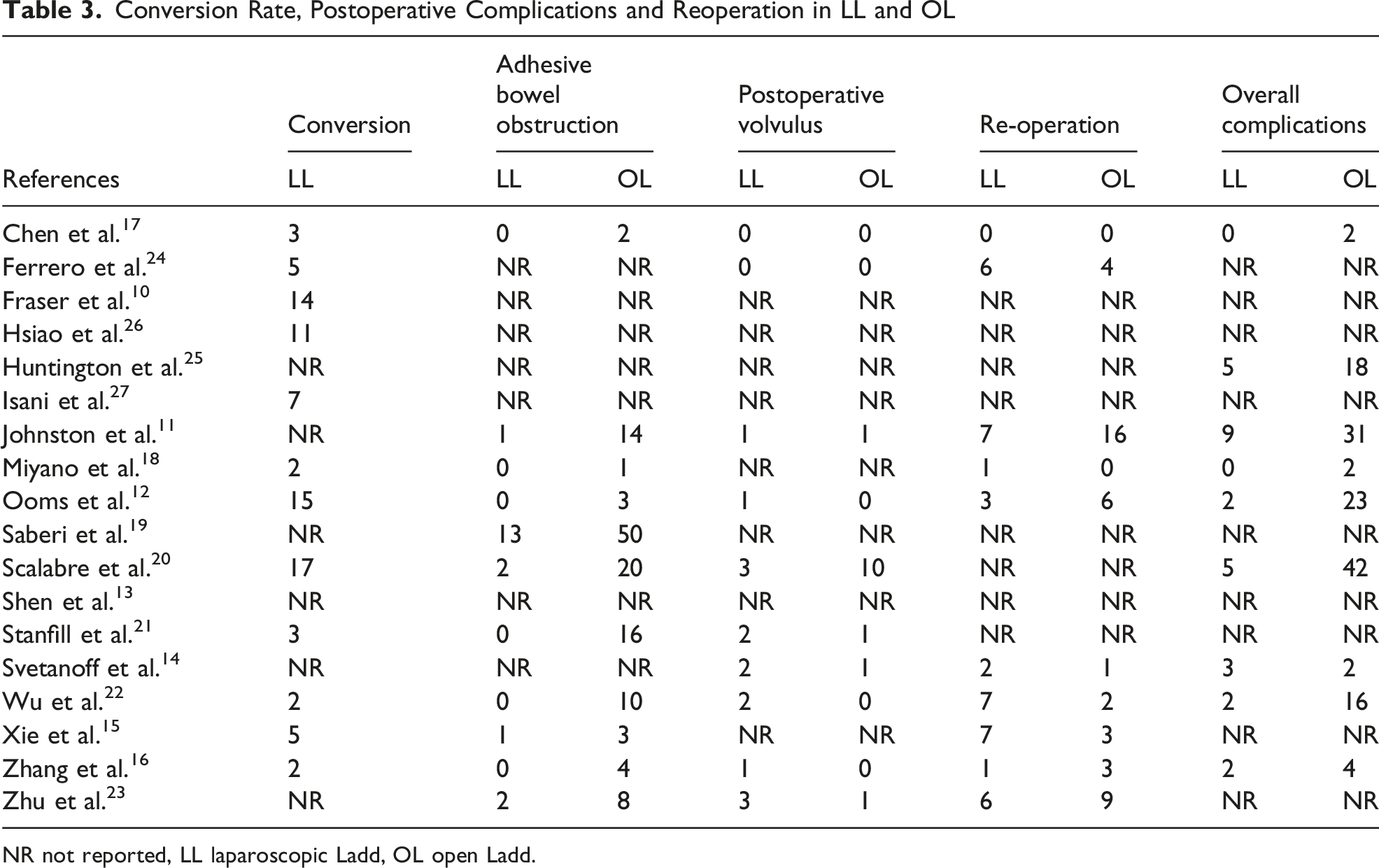
As shown in Figure 1, a total of 185 studies were initially identified through the database search. After screening titles and abstracts, 27 full-text articles were reviewed for eligibility. Ultimately, 18 studies met the inclusion criteria,10-27 encompassing a total of 3479 participants, of whom 928 underwent LL and 2551 underwent OL. The baseline demographic characteristics, including age, sex, and weight, are summarized in Table 1. The primary and secondary outcomes extracted from the included studies are presented in Tables 2 and 3, respectively. Diagram of workflow in the systematic review and meta-analysis Demographic Data, Age, Male/Female, and Weight NR not reported, LL laparoscopic Ladd, OL open Ladd. Operative Time, Time to Full Intake (Days), and Length of Hospital Stay in LL and OL NR not reported, LL laparoscopic Ladd, OL open Ladd. Conversion Rate, Postoperative Complications and Reoperation in LL and OL NR not reported, LL laparoscopic Ladd, OL open Ladd.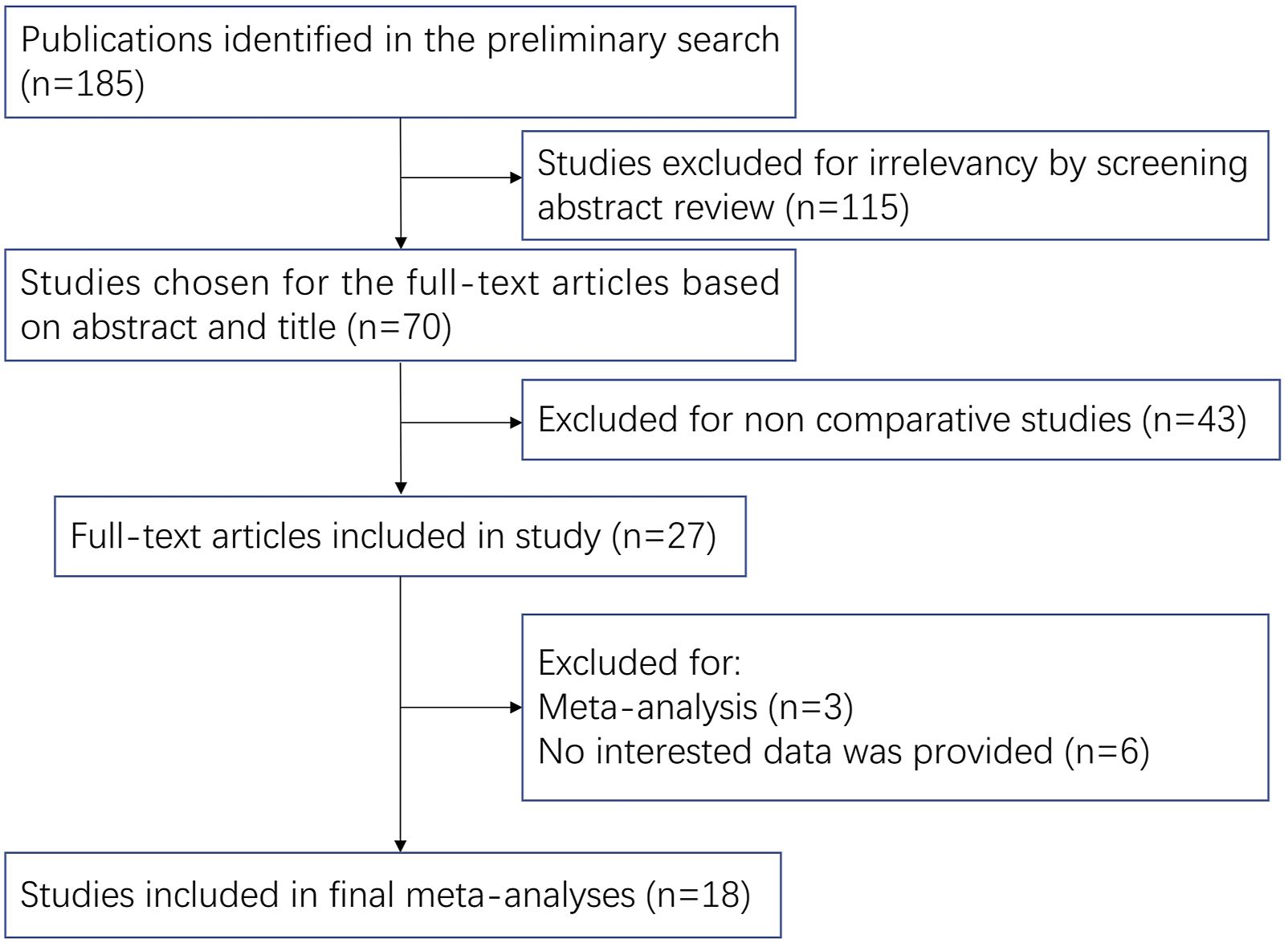
Primary Outcome Measures
Operative Time (Min)
Twelve studies reported operative time, of which seven were eligible for meta-analysis.10-16 The pooled analysis revealed no significant difference in operative time between the LL and OL groups (Mean Difference [MD] = 9.14, 95% Confidence Interval [CI]: −4.01 to 22.28; P = 0.17), although there was substantial heterogeneity among studies (I2 = 97%) (Figure 2A). Forest plot comparing operative time (A), time to full intake (B) and length of hospital stay (C) for children treated with LL vs OL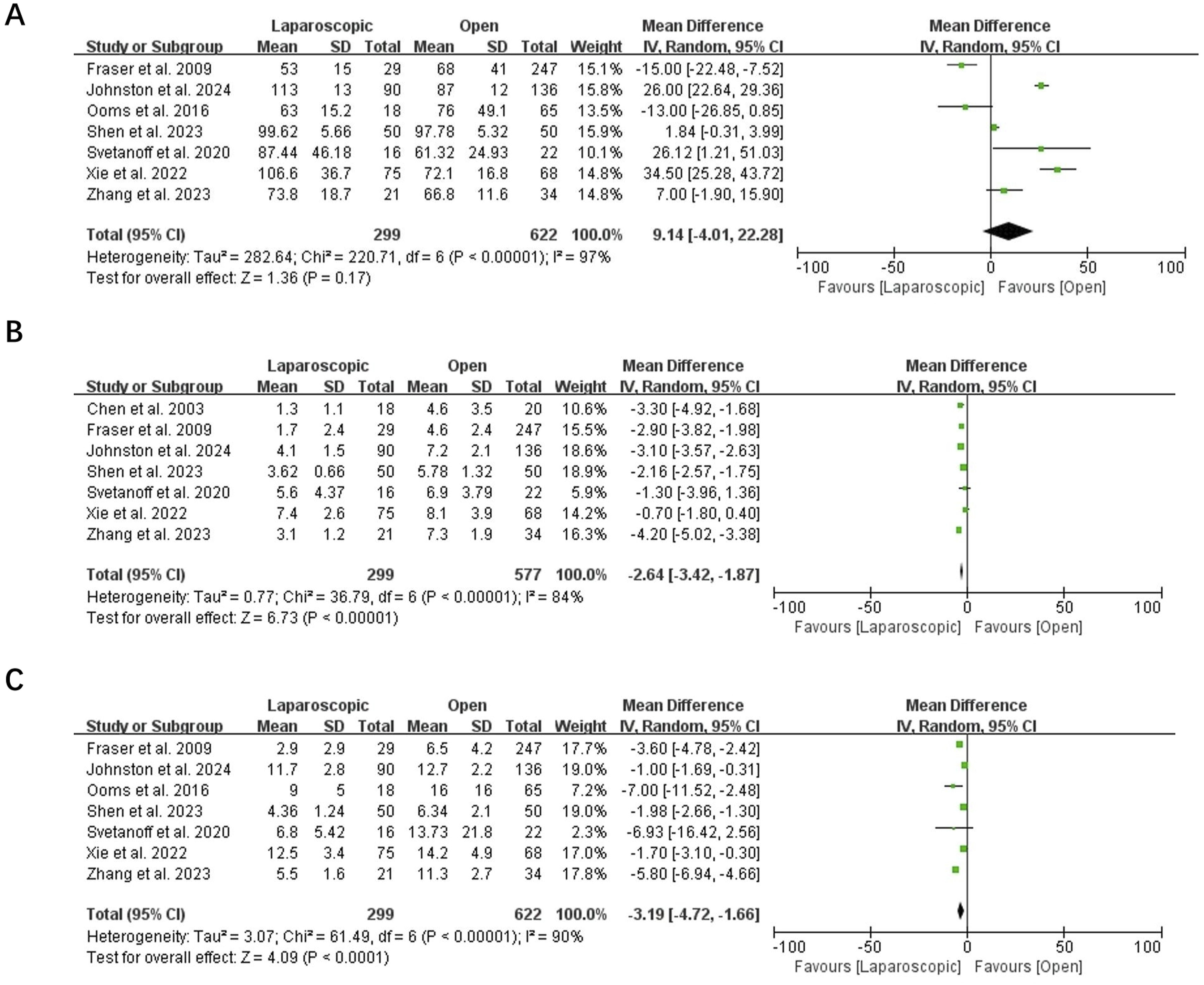
Time to Full Intake (Days)
Nine studies reported the duration to achieve full enteral intake, with seven studies included in the quantitative synthesis.10,11,13-17 The pooled results showed that time to full intake was significantly shorter in the LL group compared to the OL group (MD = −2.64, 95% CI: −3.42 to −1.87; P < 0.001), despite notable heterogeneity (I2 = 84%) (Figure 2B).
Length of Hospital Stay (Days)
Eleven studies reported hospital stay, and seven studies were included in the meta-analysis.10-16 The pooled analysis demonstrated that LL was associated with a significantly shorter hospital stay than OL (MD = −3.19, 95% CI: −4.72 to −1.66; P < 0.001), with substantial heterogeneity (I2 = 90%) (Figure 2C).
Secondary Outcome Measures
Adhesive Bowel Obstruction
Eleven studies evaluated the incidence of adhesive bowel obstruction.11,12,15-23 Among them, 19 cases (2.7%) occurred in the LL group (19/701), compared to 131 cases (6.7%) in the OL group (131/1942). Meta-analysis showed a significantly lower incidence of adhesive bowel obstruction in the LL group (Odds Ratio [OR] = 0.44, 95% CI: 0.28-0.69; P < 0.001), with low heterogeneity (I2 = 11%) (Figure 3A). Forest plot comparing postoperative adhesive bowel obstruction (A), and postoperative volvulus (B) between LL and OL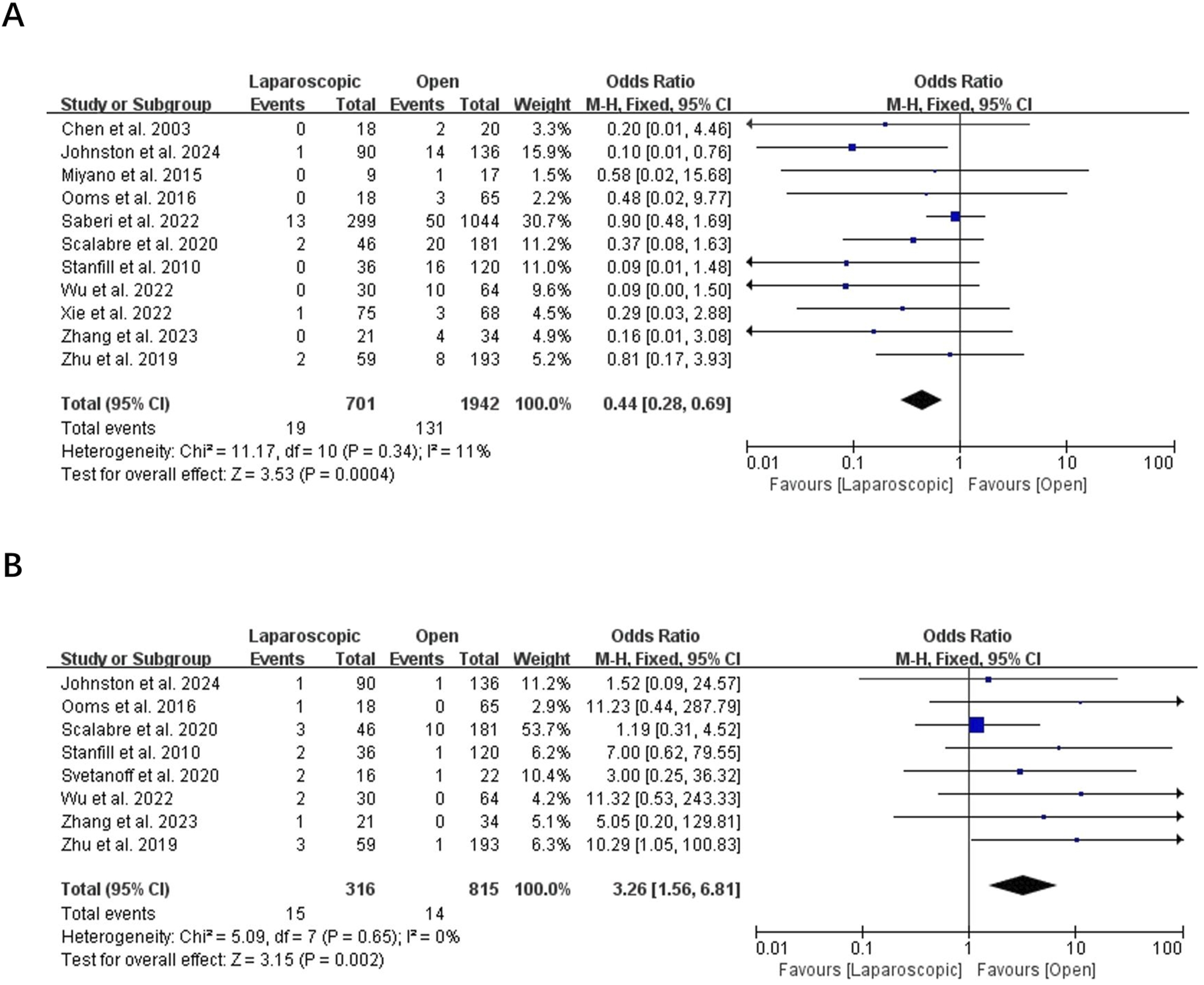
Postoperative Volvulus
Eight studies reported postoperative volvulus.11,12,14,16,20-23 LL was associated with 15 cases (4.7%) (15/316), while OL had 14 cases (1.7%) (14/815). The pooled analysis revealed that postoperative volvulus occurred more frequently after LL (OR = 3.26, 95% CI: 1.56-6.81; P = 0.002), with no heterogeneity (I2 = 0%) (Figure 3B).
Reoperation
Nine studies assessed reoperation rates.11,12,14-16,18,22-24 Reoperation was required in 40 cases (11.8%) following LL (40/338) and 44 cases (7.1%) after OL (44/619). Meta-analysis indicated a significantly higher reoperation rate in the LL group (OR = 1.67, 95% CI: 1.06-2.64; P = 0.03), with mild heterogeneity (I2 = 26%) (Figure 4A). Forest plot comparing re-operation (A), and overall complications (B) between LL and OL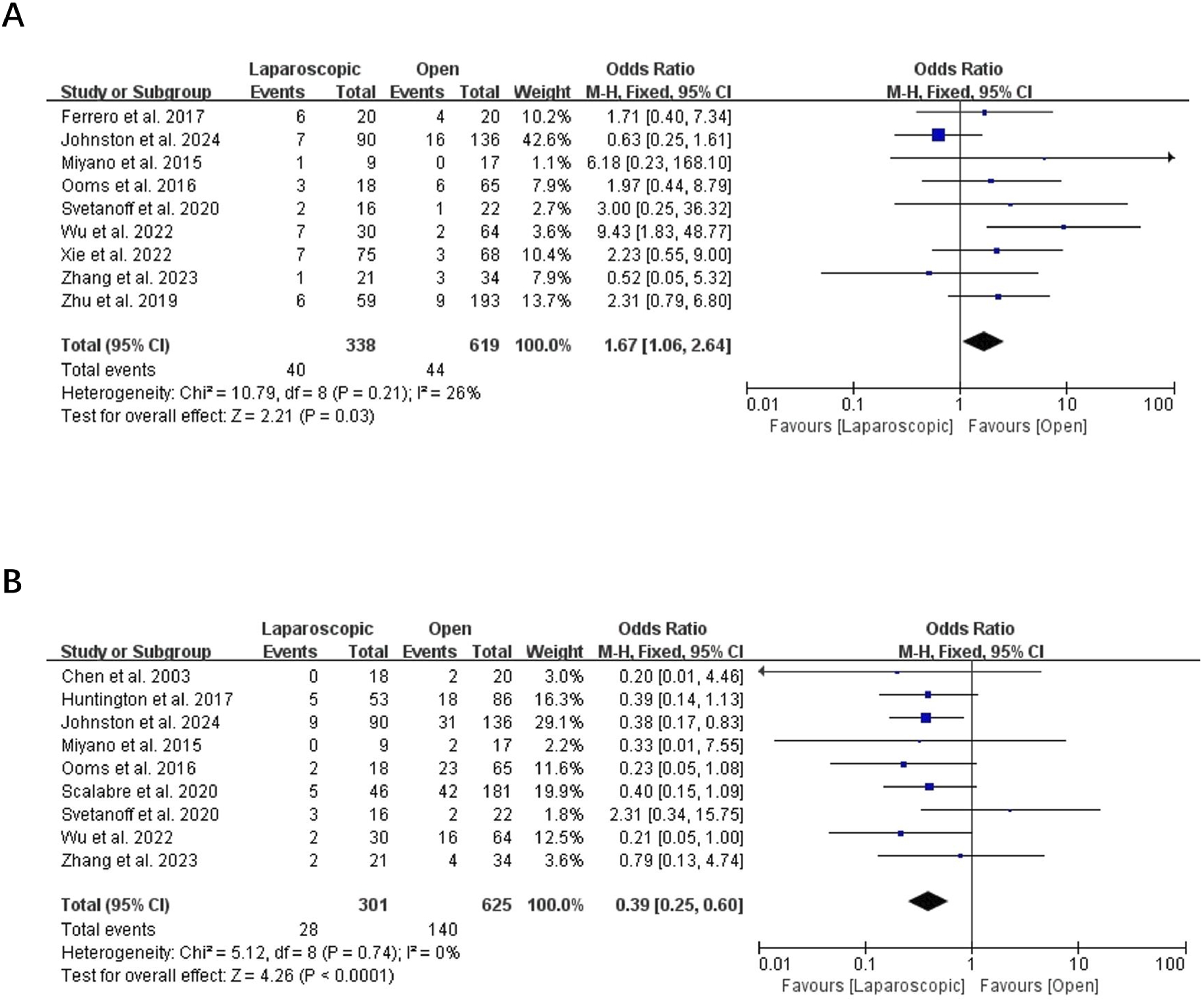
Overall Complications
Nine studies reported overall postoperative complications.11,12,14,16-18,20,22,25 The incidence of complications was 9.3% (28/301) in the LL group and 22.4% (140/625) in the OL group. Pooled results showed that LL significantly reduced the risk of overall complications (OR = 0.39, 95% CI: 0.25-0.60; P < 0.001), with no heterogeneity (I2 = 0%) (Figure 4B).
Discussion
This meta-analysis provides an updated and comprehensive comparison between LL and OL for intestinal malrotation in infants and children. By pooling data from 18 studies involving 3479 patients, our findings indicate that both surgical approaches are safe and effective, but each has distinct advantages and drawbacks. The results demonstrate that LL offers faster postoperative recovery, reflected by shorter time to full feeding and reduced hospital stay, while OL may be associated with fewer cases of postoperative volvulus and reoperation. These results contribute new evidence to the evolving discussion surrounding the optimal surgical approach for pediatric intestinal malrotation.
Compared with previous meta-analyses, our study represents one of the most comprehensive and up-to-date evaluations of this topic. In particular, our work extends the findings of Zhang et al. 28 by including several additional and more recent studies, thereby increasing the total sample size and improving the reliability of pooled estimates. The inclusion of these newer data sources enhances the statistical power and allows for a more refined analysis of both perioperative and long-term outcomes. Moreover, the current meta-analysis provides an updated perspective on the evolution of laparoscopic techniques and surgical proficiency over the past few years, which may account for some of the differences in findings compared with earlier reviews. Regarding primary outcome measures, our findings on length of hospital stay and time to full feeds were consistent with those of Zhang et al., 28 confirming that LL offers a faster postoperative recovery than OL. However, unlike Zhang et al.’s study, which reported a significantly longer operative time for LL, our updated analysis revealed no statistically significant difference between the two approaches. This change may reflect improvements in laparoscopic technology, increased surgeon experience, and the learning curve effect over time, as minimally invasive pediatric surgery has become more widely adopted. The reduction in operative time difference suggests that LL can now be performed as efficiently as OL in experienced centers.
In terms of secondary outcome measures, our study largely supports the conclusions of Zhang et al. 28 by showing that LL significantly reduces the risk of adhesive bowel obstruction and overall complications, which can be attributed to smaller incisions, minimal tissue handling, and reduced postoperative adhesion formation. Similarly, we observed a higher incidence of postoperative volvulus following LL, consistent with previous literature, possibly due to limited exposure or incomplete widening of the mesenteric base during laparoscopy. However, in contrast to Zhang et al, who found no significant difference in reoperation rates between LL and OL, our analysis revealed that reoperation occurred more frequently in the LL group, with statistical significance. This discrepancy may be related to differences in follow-up duration, case selection, or surgeon experience among the newer studies included in our analysis.
The interpretation of postoperative volvulus and reoperation rates is limited by the lack of standardized reporting of operative techniques among the included studies. Variations in key steps of the Ladd’s procedure, particularly the adequacy of mesenteric base widening, completeness of Ladd band division and adhesiolysis, and the use of fixation, may substantially influence postoperative recurrence and the need for reintervention. These technical elements were inconsistently described and not comparable across studies, especially in retrospective series, and may therefore act as confounders. In addition, surgeon experience and the learning curve for laparoscopic Ladd’s procedure may further contribute to outcome variability. Future prospective studies should incorporate standardized technical descriptions and quality metrics of Ladd’s procedure to allow more reliable comparisons between laparoscopic and open approaches.
This study has several limitations that should be acknowledged. First, most of the included studies were retrospective and non-randomized, which may introduce inherent selection bias and confounding factors, as surgeons tend to choose the operative approach based on patient stability, age, or comorbidities. Second, the completeness of the Ladd’s procedure could not be assessed due to insufficient intraoperative technical reporting, which may bias the comparison of postoperative volvulus and reoperation outcomes. Finally, publication bias cannot be fully excluded, as studies with negative or non-significant findings are less likely to be published. Therefore, large-scale, prospective, multicenter randomized controlled trials are needed to validate our results and better define the optimal surgical approach for intestinal malrotation in infants and children.
In conclusion, both LL and OL are effective and safe treatment options for intestinal malrotation in infants and children, with distinct advantages and risks. Future research should standardize operative reporting and age to better define which patients benefit most from laparoscopy.
Footnotes
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Author Contributions
Yan Lang, MD, conceived and designed the study, collected data, and drafted the manuscript. Qian Chen, MD, conceived and designed the study, collected data, and drafted the manuscript. Mengyu Wu, MD, conceived and designed the study, collected data, and drafted the manuscript. Guo Chen, MD, conceived and designed the study, collected data, and drafted the manuscript. Wenyuan Liu, MD, conceived and designed the study, collected data, and drafted the manuscript. Chen Yuan, MD, conceived and designed the study, collected data, and revised the manuscript. All authors reviewed and approved the final the work as it was submitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The corresponding author can provide the dataset utilized and analyzed for this work upon reasonable request.
Declarations
Compliance with ethical standards.