
Abstract
Objective
This study is conducted to evaluate the clinical value of a modified ureteral stent placement technique in patients undergoing ureteroscopic surgery.
Methods
A total of 138 patients with renal or ureteral calculi were randomized to receive either conventional or modified ureteral stent placement following ureteroscopic lithotripsy (69 per group). The primary outcome was the duration of postoperative hematuria, and the secondary outcomes included operative time, hospital stay, White blood cell count (WBC) and procalcitonin (PCT) levels, Ureteral Stent Symptom Questionnaire (USSQ), Generic Quality of Life Inventory-74 (GQOLI-74), stone clearance rate, postoperative complications, and 30-day readmission rates.
Results
Compared with the conventional group, the modified group had shorter hematuria duration, lower WBC and PCT levels at 2 weeks, lower USSQ scores for urinary symptoms, physical pain, and sexual life at 2 weeks, and higher GQOLI-74 scores for physical, psychological, and social function at 6 weeks (all P < .05). Operative time, hospital stay, stone clearance rate, and complication and readmission rates were similar between groups (all P > .05).
Conclusion
The modified ureteral stent technique alleviates postoperative hematuria and stent-related symptoms, reduces early inflammatory responses, and improves quality of life without increasing adverse outcomes.
Keywords
Introduction
Renal or ureteral calculi are prevalent urological disorders worldwide, characterized by high incidence and recurrence rates.1,2 Symptoms such as acute renal colic, hematuria, urinary tract infections, and potential renal impairment impose substantial suffering and health burdens on patients. With advancements in minimally invasive surgical techniques, ureteroscopic lithotripsy has emerged as a first-line standard treatment for such stones, particularly those located in the upper/middle ureter and selected renal stones. 3
However, the routine postoperative placement of a ureteral stent, while maintaining upper urinary tract drainage, promoting healing, and preventing obstruction, 4 has itself become a significant source of complications. 5 The indwelling presence of this foreign body within the bladder is a primary cause of considerable patient morbidity postoperatively, commonly referred to as stent-related symptoms. These symptoms, including urinary urgency, frequency, dysuria, pelvic/flank pain, 6 and negative impacts on daily activities and quality of life, are reported in a substantial proportion of patients. The physical irritation caused by the distal bladder coil is a key etiological factor for these discomforts 7 and may also contribute to local inflammation.
Consequently, there is a persistent clinical need to develop and refine stent technologies and placement techniques that minimize patient discomfort without compromising the essential functions of the stent. Various modifications have been explored, including alterations in stent material, 8 coating, 9 design (eg, length, diameter, and coil shape),10,11 and the development of drug-eluting stents. 12 While some show promise, issues related to cost, manufacturing complexity, or inconsistent clinical outcomes limit their universal application. A conceptually straightforward yet under-investigated approach involves physically modifying the standard double-J stent post-placement. This technique entails surgically excising the distal bladder coil and a portion of the straight segment after stent insertion, replacing it with a soft, externalized traction suture. 13 This modification aims to eliminate the primary source of mechanical irritation within the bladder while preserving the stent’s proximal (renal) coil and ureteral segment to ensure adequate drainage and positional stability. By confining the stent material to the upper urinary tract, this technique theoretically targets the root cause of many stent-related symptoms, potentially reducing inflammation and bladder overactivity.
Despite its logical premise, high-quality clinical evidence comprehensively evaluating this modified ureteral stent placement technique remains limited. Therefore, this study was designed to conduct a randomized controlled trial to systematically evaluate the clinical application value of the modified ureteral stent placement technique compared to traditional stent placement following ureteroscopy. The findings from this work aim to provide evidence-based insights to optimize postoperative stent management and improve the overall patient experience after ureteroscopic stone surgery.
Materials and Methods
Ethics Statement
The study was approved by The Affiliated Hospital of Xuzhou Medical University’s ethics committee. All patients signed an informed consent form for ureteroscopic lithotripsy and stone removal with ureteral stent placement prior to surgery.
Sample Size Calculation
The sample size calculation was based on the results of our preliminary study. The median duration of postoperative hematuria was 1.5 days (interquartile range [IQR], 1.0-2.0 days) in the modified group and 2.5 days (IQR, 2.0-3.0 days) in the conventional group. The pooled standard deviation was estimated to be 0.79 days. Assuming a two-sided significance level of 0.05 and a statistical power of 90%, calculations conducted using PASS 2020 indicated that a minimum of 57 patients per group was required. Allowing for a potential attrition or exclusion rate of up to 20%, the final sample size was increased to 69 patients per group, yielding a total of 138 participants, which ensured adequate statistical power.
Study Population
The patients with renal or ureteral calculi treated between October 2022 and October 2024 were recruited. The detailed inclusion and exclusion criteria and withdrawal criteria were as follows.
Inclusion Criteria
① Patients clinically diagnosed (eg, flank pain, hematuria) and confirmed by imaging studies (urinary tract ultrasound, CT) as unilateral renal calculi (≤ 2.0 cm in diameter) or upper/mid-ureteral calculi (≥ 0.6 cm and ≤ 1.5 cm in diameter) 14 ; ② Patients aged 18-70 years; ③ Patients were classified as ASA grade I–II and were able to tolerate ureteroscopic surgery and general anesthesia; ④ Patients showed no active urinary tract infection on preoperative urinalysis (clean midstream urine white blood cells <10/HP); ⑤ Patients were conscious, had no severe cognitive or psychiatric disorders, and were able to communicate effectively with investigators, and were willing to complete all questionnaire assessments and follow-up visits.
Exclusion Criteria
① Patients with severe cardiac, pulmonary, hepatic, or renal insufficiency, or uncontrolled systemic diseases such as diabetes or hypertension, presenting a high surgical risk; ② Patients had active urinary tract infection, urinary tuberculosis, or tumor; ③ Patients had coagulation disorders or were on long-term anticoagulant/antiplatelet therapy that could not be safely discontinued before surgery; ④ Pregnant or lactating women; ⑤ Patients had urinary tract anatomical abnormalities; ⑥ Patients with a history of allergy to contrast agents, anesthetics, or stent materials used in the study; ⑦ Patients with a history of urological-related surgeries.
Withdrawal Criteria
① Patients could not successfully complete ureteroscopic lithotripsy and stent placement due to various intraoperative reasons (such as ureteral stricture preventing scope advancement, severe intraoperative bleeding, ureteral perforation, etc.); ② Patients failed to retain the stent for the required duration (2 weeks) as per the study protocol, or removed the stent prematurely on their own; ③ Patients required major treatment for non-study-related diseases during follow-up that could affect outcome assessment (eg, high-dose steroids or immunosuppressants for other conditions); ④ Patients experienced serious adverse events related to the study intervention (eg, severe septic shock, sepsis), which in the investigator’s judgment required study termination and emergency management; ⑤ Patients voluntarily withdrew informed consent at any time point, or were unable to complete all study follow-up and data collection due to loss of contact, relocation, death, or other reasons.
Randomization
Randomization was carried out by a researcher not involved in the study. Randomization software (Microsoft Excel) was utilized to generate a sequence of random numbers. Eligible participants were randomly allocated to one of two groups in a 1:1 ratio: the conventional group or the modified group. We maintained allocation concealment during the randomization process. Slips of paper indicating treatment allocation were placed in sequentially numbered, sealed, opaque envelopes, which were then opened one by one after obtaining informed consent from participants. The research assistant notified participants of their assigned study arm.
Blinding
This was a single-blinded trial. Baseline and post-intervention measurements, along with assessment procedures, were conducted by an outcome assessor who was unaware of the group assignments. The statistician responsible for the statistical analysis was also blinded to the group allocation and treatment details. Due to the nature of the interventions, it was not feasible to blind the participants.
Interventions
(1) Patients in the conventional group underwent postoperative placement of a conventional ureteral stent. All patients received flexible ureteroscopic lithotripsy and stone extraction under combined intravenous–inhalational general anesthesia. All procedures were performed by the same senior surgeon with extensive experience (annual caseload >200 cases). Patients were placed in the lithotomy position and prepared using standard sterile techniques. Under Zebra guidewire guidance, an F12/14 ureteral dilation sheath (COOK Medical, USA) was advanced transurethrally to the renal pelvis. Subsequently, an Olympus electronic flexible ureteroscope was introduced along the sheath to inspect the renal pelvis and calyces and to locate calculi. A 200-μm holmium laser fiber (Lumenis, USA) was connected to a holmium laser generator (Lumenis, USA), with energy settings of 0.8-1.0 J and a frequency of 10-15 Hz, to fragment or dust the stones. Smaller fragments were flushed out by irrigation, whereas larger fragments were retrieved using a stone basket (COOK Medical, USA). After confirming satisfactory stone clearance, absence of active bleeding, and no obvious mucosal injury, an untrimmed standard double-J ureteral stent was placed under guidewire guidance. Stent length was selected according to patient height (typically 22-26 cm), ensuring that the proximal coil was positioned within the renal pelvis and the distal coil was entirely located within the bladder. A urinary catheter was routinely retained for 24 h postoperatively. (2) Patients in the modified group underwent postoperative placement of a modified ureteral stent. The surgical procedure, anesthesia, operating surgeon, and equipment were identical to those used in the conventional group; the only difference lay in the management of the postoperative ureteral stent. After confirming the need for stent placement, a conventional double-J stent of appropriate length was selected based on patient’s height. Under strict aseptic conditions, the distal (bladder-side) coil and a portion of the straight segment were excised using sterile scissors, leaving only the proximal (renal-pelvic) coil and an adequate length of the ureteral segment. A sterile surgical suture (2-0 silk) of equal length to the excised portion was prepared. A knot was tied at one end of the suture, and this knotted end was securely sutured to the cut end of the stent to serve as a traction line retained within the bladder. The knot-free end of the suture was exteriorized through the urethra and securely fixed to the medial thigh skin. Through this modification, the bladder segment of the ureteral stent was replaced by a soft silk thread, while the stent body itself was confined to the renal pelvis and ureter. A urinary catheter was likewise retained for 24 h postoperatively.
Both groups routinely received prophylactic antibiotics [Cefuroxime axetil, 0.25 g (1 tablet) each time, twice daily] for 24-48 h following surgery. All patients had a ureteral stent placed preoperatively for 2 weeks to passively dilate the ureter, and this preoperative protocol was identical in both groups. The postoperative ureteral stents (complete stents in the conventional group and trimmed stents in the modified group) were removed at the outpatient clinic 2 weeks post-surgery. In the conventional group, the stent was removed using a cystoscope under topical anesthesia, while in the modified group, it was removed by pulling the suture outside the urethral orifice. The suture site was disinfected with iodophor.
Outcome Measures
The primary outcomes included the duration of postoperative hematuria. The secondary outcomes included operative time, postoperative hospital stay, inflammatory markers (white blood cell count (WBC), procalcitonin (PCT)), Ureteral Stent Symptom Questionnaire (USSQ), Generic Quality of Life Inventory-74 (GQOLI-74), stone clearance rate, complications, and the proportion of readmissions. (1) Perioperative time-related outcomes: Perioperative time-related parameters were recorded and compared between the two groups, including operative time (defined as the interval from ureteroscope insertion to completion of the procedure and scope withdrawal), duration of postoperative hematuria (calculated as the number of days from the end of surgery until complete resolution of gross hematuria), and length of hospital stay (defined as the total number of inpatient days from the first postoperative day until fulfillment of discharge criteria). (2) Inflammatory markers: Venous blood samples were obtained under fasting conditions from all participants at two predefined time points: prior to surgery and 2 weeks after the procedure, immediately before ureteral stent removal. To assess inflammatory status, peripheral blood was divided for hematological and biochemical analyses. Specifically, 2 mL of whole blood was drawn into EDTA-containing tubes for determination of the WBC, while a separate 2 mL aliquot was collected in serum preparation tubes for PCT analysis. For hematological evaluation, EDTA-anticoagulated samples were analyzed within 2 h using a fully automated blood cell analyzer (XN-9000, Sysmex, Japan), which applies fluorescence-based flow cytometric techniques according to the manufacturer’s validated procedures and reagents. For biochemical assessment, serum samples were prepared by allowing blood to clot at ambient temperature for 30 min, followed by centrifugation at 3000 rpm for 10 min using a refrigerated centrifuge (5804 R, Eppendorf, Germany). Serum PCT concentrations were subsequently determined via chemiluminescence immunoassay on an automated detection platform (ARCHITECT i2000SR, Abbott, USA), employing commercially available assay kits with an analytical sensitivity of 0.02 ng/mL. All laboratory measurements were carried out under standardized quality assurance conditions by the same experienced laboratory team to ensure methodological consistency and minimize inter-assay variability. (3) USSQ
15
: Stent-related symptoms were evaluated at 2 weeks postoperatively (prior to stent removal) using the USSQ. This questionnaire consists of 38 items across six domains: urinary symptoms (11 items), bodily pain (9 items), general health (6 items), work performance (3 items), sexual matters (4 items), and other problems (5 items). Most items are rated on a 5-point Likert scale (0-4), while selected psychological perception items are scored using a 7-point Likert scale (0-6). Each domain is scored independently, with higher scores indicating greater symptom severity or poorer quality of life within that domain. (4) GQOLI-74: Health-related quality of life was assessed before surgery and at 6 weeks postoperatively (4 weeks after stent removal) using the GQOLI-74 questionnaire. This instrument evaluates quality of life across four domains: physical function, psychological function, social function, and material well-being. Domain scores were standardized on a 0-100 scale, with higher scores indicating better quality of life. (5) Stone clearance rate, complications and readmission: Four weeks after stent removal, all patients underwent a plain urinary CT scan to assess residual stones, and the stone clearance rate was calculated. All stent- or surgery-related complications occurring from the postoperative period until 4 weeks after stent removal were recorded. These included, but were not limited to: ① Severe hematuria, defined as gross hematuria requiring pharmacological intervention (eg, hemostatic agents) or rehospitalization; ② Symptomatic urinary tract infection (UTI), characterized by clinical manifestations such as fever (body temperature >38.5°C), chills, or flank pain, accompanied by positive urine culture results or significantly elevated WBC or PCT levels requiring antimicrobial therapy; ③ Stent-related pain, defined as intolerable lumbar or suprapubic pain necessitating treatment with nonsteroidal anti-inflammatory drugs or opioid analgesics; ④ Stent migration or dislodgement, confirmed by imaging examinations (eg, plain kidney–ureter–bladder radiography); ⑤ Vesicoureteral reflux, evaluated using voiding cystourethrography (VCUG) before stent removal on postoperative day 14 (At this point, the intravesical pressure was at its maximum), with grade III or higher reflux considered positive; ⑥ Other complications, including stent encrustation, fracture, and urinary retention. In addition, the rate of rehospitalization within 30 days for any cause directly attributable to the surgical procedure or ureteral stent (eg, refractory pain, severe infection, obstruction, or major hemorrhage) was calculated.
Statistics
All statistical processing was implemented with SPSS software (version 27.0). Variables were analyzed according to their data type and distribution characteristics. Categorical variables were summarized as counts and proportions [n (%)], and intergroup differences were assessed using the χ2 test or Fisher’s exact test. For continuous variables, data distribution was first examined using the Shapiro–Wilk test, with a P value greater than 0.05 indicating conformity to normality. Continuous data meeting normal distribution criteria were reported as mean ± standard deviation (
Results
Demographic Data
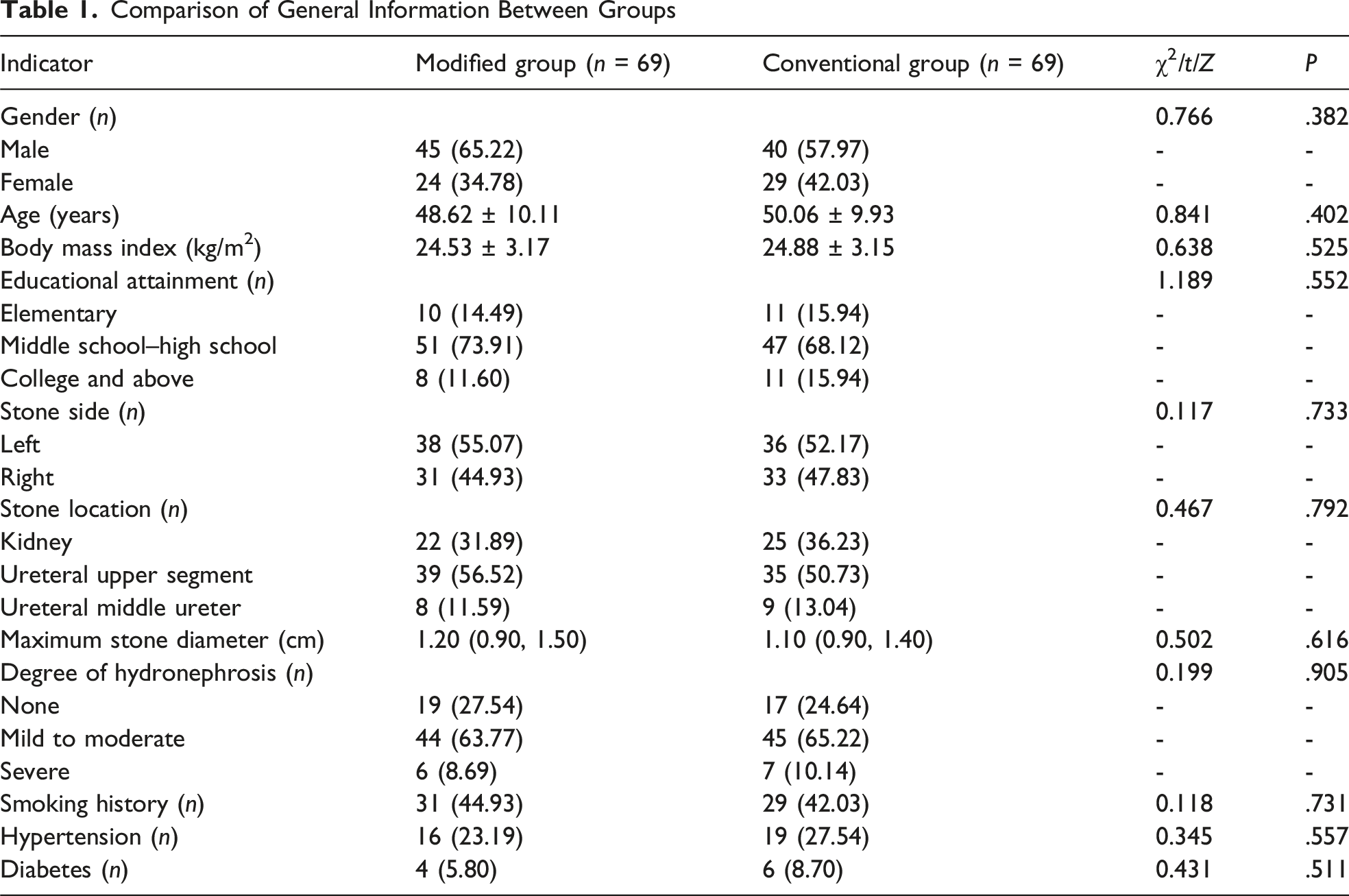
A total of 138 patients were initially randomized. During follow-up, 2 patients in the modified group were withdrawn because of loss to follow-up, and 4 patients in the conventional group were excluded (one due to intraoperative ureteral stricture preventing completion of the procedure and three due to loss to follow-up). Consequently, 132 patients completed the study and were included in the final analysis (67 in the modified group and 65 in the conventional group) (Figure 1). Baseline demographic and clinical characteristics remained comparable between groups (P > .05), indicating good comparability (Table 1). The flowchart of the study Comparison of General Information Between Groups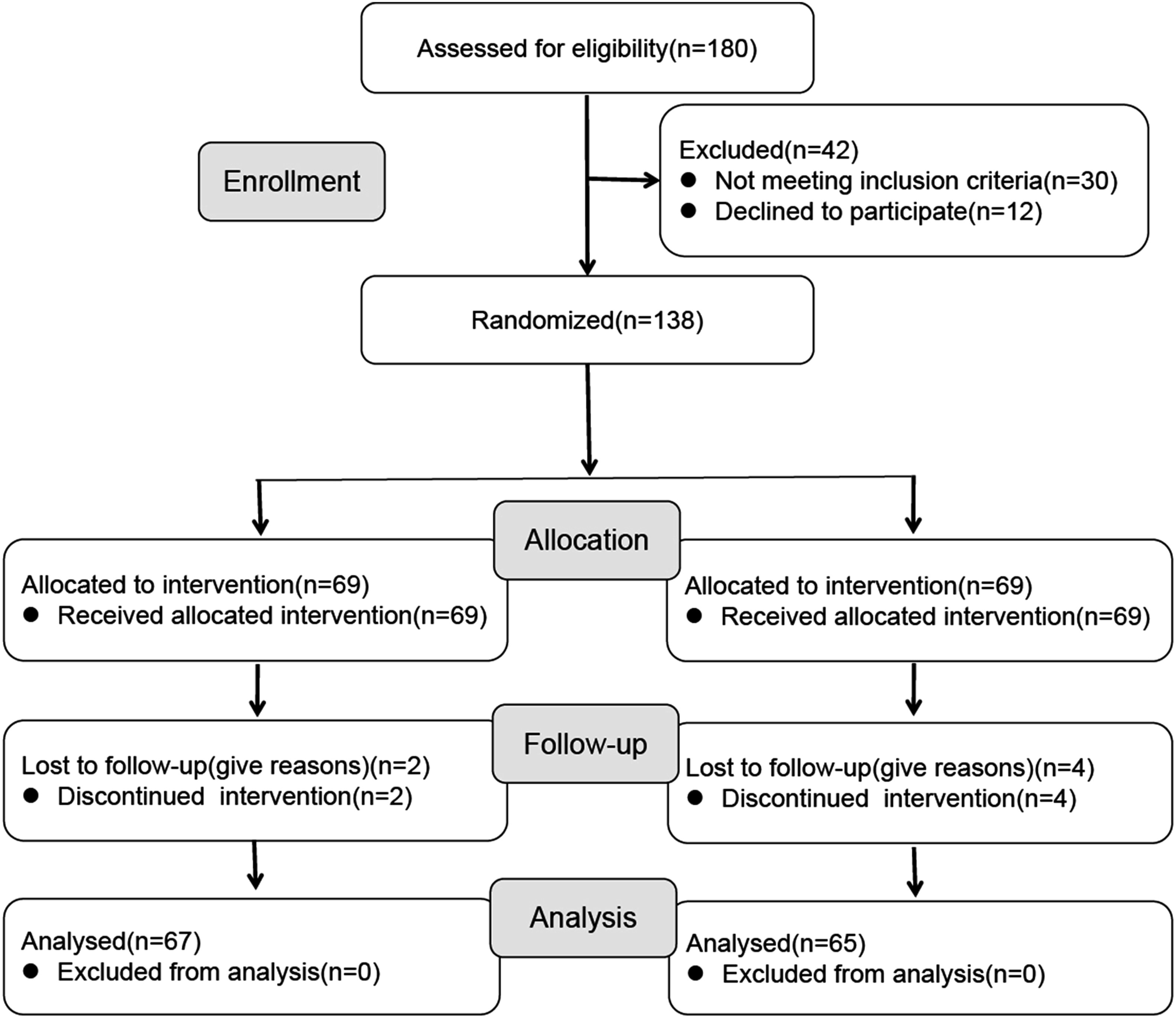
Time-Related Outcomes
Comparison of Time-Related Outcomes Between Groups

Inflammatory Markers
Comparison of Inflammatory Markers Between Groups
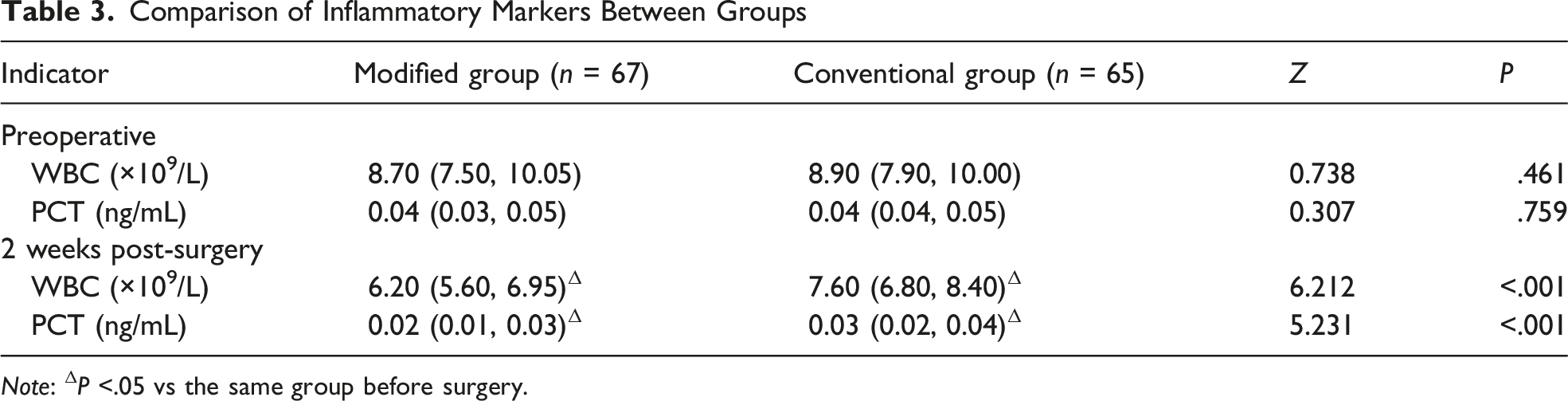
Note: ΔP <.05 vs the same group before surgery.
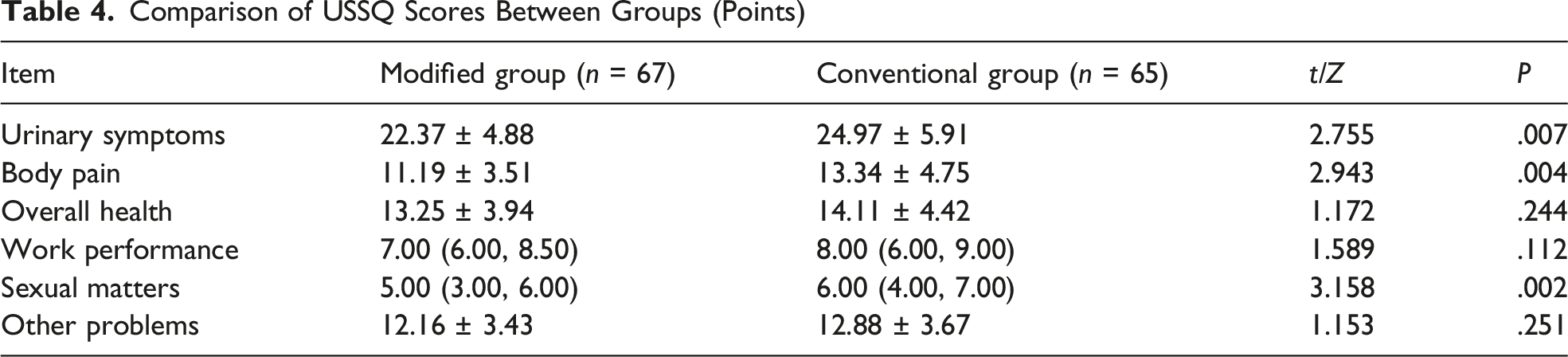
USSQ Scores
Comparison of USSQ Scores Between Groups (Points)
GQOLI-74 Scores
Comparison of GQOLI-74 Scores Between Groups (Points)
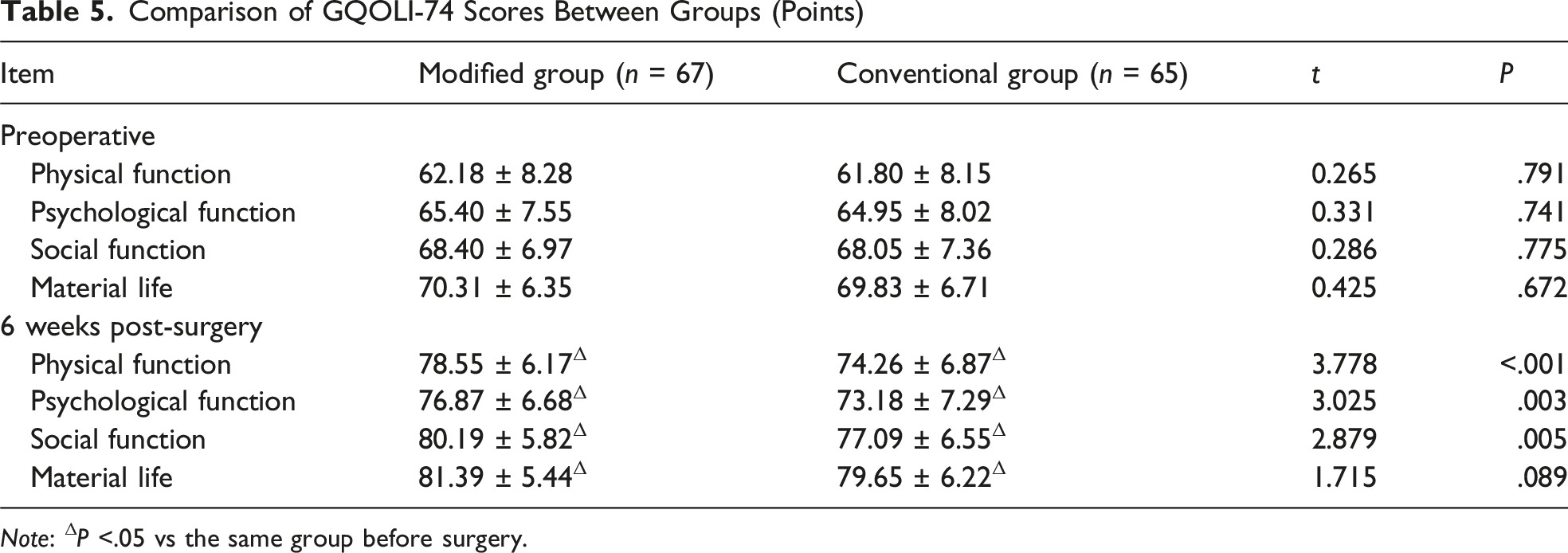
Note: ΔP <.05 vs the same group before surgery.
Stone Clearance Rate, Complications and Rehospitalization Rates
Comparison of Stone Clearance Rate, Complications and Rehospitalization Rates Between Groups [n (%)]
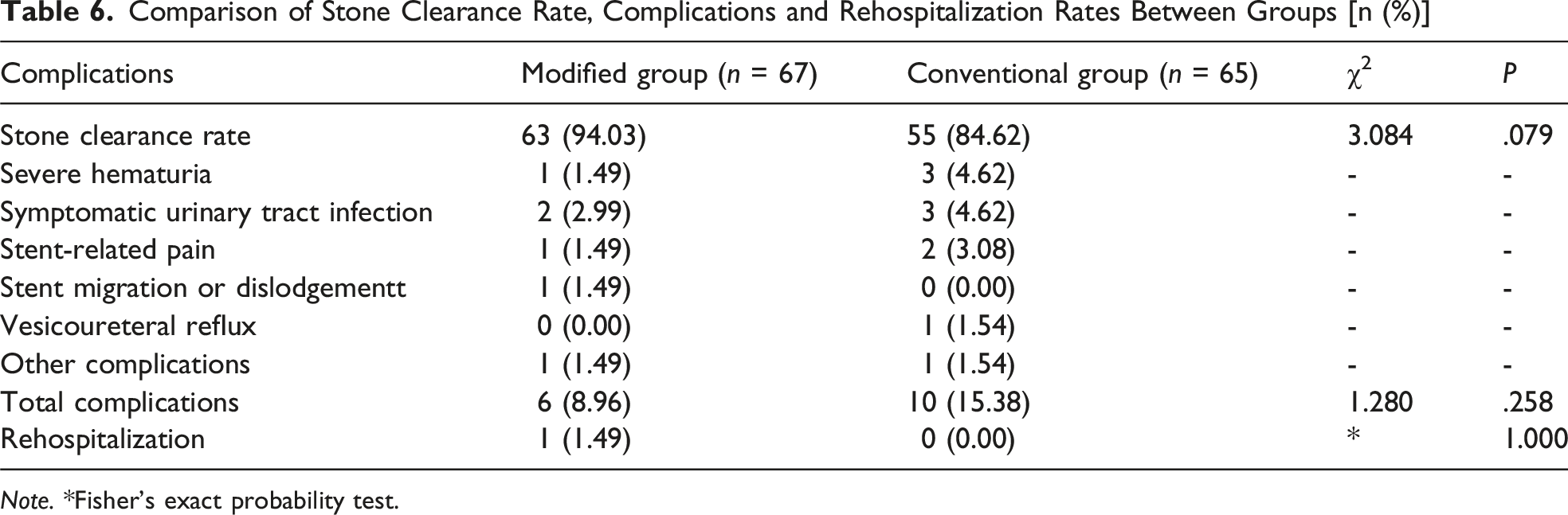
Note. *Fisher’s exact probability test.
Discussion
Urolithiasis continues to represent a substantial and growing global health challenge, driven by increasing disease prevalence and escalating healthcare expenditures. 16 Ureteroscopic lithotripsy has consequently become a mainstay of minimally invasive management for renal and ureteral calculi. However, the routine use of postoperative ureteral stents, although clinically justified for maintaining drainage and preventing obstruction, remains a major contributor to postoperative morbidity. 5 In this prospective randomized study, we demonstrate that a targeted modification of the conventional double-J stent configuration provides meaningful clinical benefits following ureteroscopic lithotripsy, without compromising procedural safety or therapeutic efficacy.
One of the earliest and most objective improvements associated with the modified stent technique was the reduction in postoperative hematuria duration. This observation is biologically plausible given the anatomical and physiological characteristics of the bladder trigone, which is densely vascularized and highly susceptible to mechanical stimulation. 17 In conventional stenting, the rigid distal coil resides within the bladder lumen and repeatedly contacts the recently instrumented urothelium, potentially interfering with early clot stabilization and epithelial regeneration. 8 By eliminating this rigid intravesical segment and replacing it with a flexible, low-profile suture, direct mechanical irritation to the bladder mucosa is substantially reduced. Supporting this interpretation, prior investigations have shown a close association between the length and stiffness of the intravesical stent segment and the severity of postoperative microscopic hematuria, suggesting that minimizing bladder contact facilitates more rapid mucosal recovery. 18
Beyond local bleeding control, the modified technique was associated with a significant attenuation of systemic inflammatory responses, as reflected by lower white blood cell counts and procalcitonin levels at the 2-week postoperative assessment. Standard polymer stents are known to provoke a foreign body reaction within the bladder, characterized by inflammatory cell recruitment and cytokine release, which may extend beyond local tissues and manifest systemically. 19 Experimental evidence further supports this mechanism, with animal studies demonstrating pronounced inflammatory infiltration in tissues adjacent to intravesical stent coils. 20 By confining stent material to the upper urinary tract—an anatomical environment with reduced contractile activity and distinct functional demands compared with the bladder—the modified approach likely dampens this inflammatory cascade. Clinical observations from Taguchi et al similarly revealed higher inflammatory marker expression surrounding the bladder coil relative to ureteral segments, reinforcing the role of intravesical stent components as a primary driver of inflammation. 21 In laparoscopic adrenalectomy, Xu et al achieved the goals of reducing postoperative inflammatory response, shortening hospital stay, and avoiding complications through an innovative central vein isolation combined with tubeless technique. 22 Additionally, after ureteroscopy, an elevated PCT level often indicates potential pyelonephritis, bacteremia, or occult infection caused by biofilm formation on the stent.23-25 Therefore, the lower PCT levels in the modified group in this study may not only confirm the inhibitory effect of this technique on postoperative inflammatory response but, more importantly, provide objective evidence suggesting that the modified stent placement technique may reduce the risk of bacterial colonization and retrograde infection by minimizing ureteral mucosa injury, avoiding excessive friction between the stent and urothelium, or offering better stent biocompatibility. This finding holds significant clinical importance.
From the patient perspective, in the USSQ scores at 2 weeks postoperatively, the modified group scored lower than the conventional group in the dimensions of urinary symptoms, physical pain, and sexual issues. These findings are consistent with prior reports examining strategies aimed at reducing intravesical stent irritation.26,27 The distal coil of a conventional double-J stent acts as a persistent mechanical stimulus to bladder afferent pathways, often generating sensations of urgency, frequency, and discomfort that mimic bladder overdistension. 28 Additionally, inappropriate stimulation of the detrusor muscle and distortion of the trigonal region may precipitate involuntary contractions characteristic of bladder overactivity. Removal of this intravesical irritant therefore directly addresses the anatomical and neurophysiological origins of these symptoms, explaining the consistent symptom relief observed in the modified group. It has also been reported that comparing the technique of completely placing the distal end of the stent within the ureter (CIU-SP) with conventional stent placement, the CIU group showed significantly better scores in USSQ urinary symptoms, physical pain, and overall health. 27 The pattern of differences in USSQ scores between our modified and conventional groups is similar to that in this study.
Improvements in symptom burden were subsequently reflected in superior health-related quality of life outcomes at six weeks postoperatively. Patients receiving the modified stent reported higher scores in physical, psychological, and social functioning domains of the GQOLI-74 questionnaire. Persistent pain, nocturia-related sleep disturbance, and anxiety related to urinary urgency are well-recognized contributors to diminished postoperative well-being.29,30 By alleviating these factors during the early recovery period, the modified stent technique appears to support a more complete functional and psychosocial rehabilitation. This finding aligns with an evolving emphasis in contemporary surgical evaluation that prioritizes patient-reported outcomes and quality-of-life metrics alongside traditional clinical endpoints, as increasingly advocated in both urological oncology and endourology literature.31,32
Importantly, these clinical advantages were achieved without sacrificing procedural safety or the fundamental objectives of ureteral stenting. The stone clearance rates, postoperative complications, and 30-day readmission rates were comparable between the modified and conventional groups. Preservation of the proximal renal coil ensured stable positioning within the collecting system and effective upper tract drainage, while external fixation of the traction suture minimized the risk of stent migration. However, while affirming the overall safety, specific procedures in the modified technique still require attention to safety. Regarding the risk of infection, exposed sutures may increase the opportunity for bacterial colonization, but external fixation facilitates local cleaning and disinfection, theoretically not increasing the risk of infection. Regarding suture detachment, one case of stent displacement/detachment occurred in this group, suggesting that the reliability of suture fixation needs to be considered in this technique. Regarding daily comfort, external sutures may cause some inconvenience in activities such as dressing, but since the stent is removed within 2 weeks postoperatively, the negative impact is limited. The findings of this study confirm that, under the premise of ensuring surgical safety and effectiveness, the modified technique may also aim to enhance patient comfort and subjective experience. As demonstrated in Xu et al's study, in modern endoscopic surgeries, whether it is PCNL puncture positioning or ureteroscopic stent placement, the core of technical modification lies in fine-tuning key steps rather than overturning existing operations. 33 This suggests that standardized and reproducible surgical procedures are the foundation for ensuring the safe promotion of techniques, providing methodological references for the clinical promotion of the modified stent in this study.
This study has several limitations. First, the short follow-up period limits the evaluation of late complications such as ureteral stricture and re-intervention. Second, this study was designed as a single-center, single-surgeon study, which, while ensuring operational consistency, limits the external validity of the results. Third, no correction for multiple comparisons was performed, posing a risk of type I error inflation, and some significant results should be interpreted within an exploratory framework. Fourth, all patients underwent preoperative stent placement, which may induce local ureteral inflammation or cause patients to adapt to stent discomfort, partially confounding postoperative intergroup differences. Therefore, the results of this study mainly apply to the patient population undergoing routine preoperative stent placement, and the value of the modified technique for patients undergoing direct ureteroscopy requires further validation.
In summary, excision of the distal intravesical segment of a conventional double-J stent represents a physiologically rational and clinically effective refinement of standard postoperative management following ureteroscopic lithotripsy. By targeting the principal anatomical source of stent-related morbidity, this approach shortens the duration of visible hematuria, mitigates systemic inflammatory responses, significantly reduces lower urinary tract and pain-related symptoms, and ultimately enhances postoperative quality of life. Together with an acceptable safety profile, these findings support the modified stent placement technique as a promising strategy to optimize postoperative recovery in patients undergoing ureteroscopic stone surgery and warrant consideration for broader clinical implementation. In the future, multi-center, long-term follow-up studies should be conducted to verify its long-term safety. Consideration can be given to clarifying its applicability in patient populations without preoperative stent placement, while exploring further optimization of suture fixation methods.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jiangsu Provincial Medical Youth Talent (QNRC2016794).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.