
Abstract
Background
Retained surgical items (RSIs) represent a significant patient safety concern in minimally invasive surgery (MIS) due to the limitations of conventional detection methods. This study evaluated the technical feasibility of a novel triple-detector radiofrequency identification (RFID) system integrated into a laparoscopic port for automated, real-time tracking and directional differentiation of surgical gauze during procedures.
Methods
We developed a prototype system integrating three RFID detectors (134.2 kHz) longitudinally into a standard 12-mm laparoscopic port. In a controlled laboratory setting, 118 pieces of RFID-tagged gauze were systematically inserted and retrieved through the port, generating 236 events. The study evaluated detection accuracy across outer, middle, and inner channels, alongside directional discrimination capability and temporal tracking performance using a laparoscopic training model.
Results
Detection rates exceeded 99% across all three channels (99.58% for the outer channel and 99.15% for middle and inner channels). Directional differentiation accuracy, based on sequential detection patterns, was 94.92% for insertion and 95.76% for removal. Anomalous patterns (4-5%), such as channel omission or duplicate detection, were observed due to passage speed or angle, but they did not impact the final determination of gauze presence or absence.
Conclusions
This proof-of-concept study demonstrates that an RFID-integrated laparoscopic port can achieve high detection (>99%) and directional accuracy (∼95%). These findings support its technical feasibility as an automated safety mechanism for potentially reducing the risk of RSIs in laparoscopic surgery; however, further validation through animal studies and clinical trials is required to confirm these results.
Backgrounds
The widespread adoption of minimally invasive surgery (MIS) has revolutionized surgical practice over the past decades, offering patients substantial benefits, including reduced postoperative pain, shorter hospital stays, and improved cosmetic outcomes.1-3 Despite these advantages, however, the risk of retained surgical items (RSIs), including surgical gauze, remains a critical patient safety concern. Recent studies suggest that the retainment of surgical items occurs in approximately 1 in 1000-5000 surgical procedures, with surgical gauze accounting for approximately 70% of all retained items.4-6
Although radiopaque-marked surgical gauze is now predominantly used, its detection during laparoscopic surgery still presents several challenges. This is particularly problematic in patients with a high body mass index (BMI) or in patients with significant bleeding, in which surgical gauze may be obscured by abdominal organs or adipose tissue. Traditional detection methods such as manual counting and radiographic imaging have proven insufficient in certain clinical scenarios, and these limitations can lead to potential oversight, resulting in serious postoperative complications.7-9 Notably, retained surgical gauze can cause severe complications. In mild cases, patients experience postoperative pain and infection, whereas in severe cases, patients can progress to intestinal obstruction, bowel perforation, and fistula formation.10-12 These complications frequently necessitate reoperation and prolonged hospitalization and, in some cases, can lead to significant morbidity. Furthermore, cases involving RSIs often result in medical litigation, affecting both healthcare providers and institutions.
To address these limitations, we developed a novel prototype system that integrates radiofrequency identification (RFID) technology into laparoscopic ports and surgical gauze. Unlike conventional radiopaque markers, the use of RFID technology enables automated real-time counting and tracking, thereby preventing oversight that may occur during manual counting and increasing both surgical safety and efficiency.
The objective of this proof-of-concept study was to evaluate the technical feasibility and performance of this prototype system in a controlled laboratory setting. Specifically, we assessed two key metrics: (1) the detection accuracy of RFID-tagged surgical gauze and (2) the reliability of directional discrimination using a triple-detector array. This preliminary investigation serves as an initial technical validation phase, and further verification through animal studies and clinical trials is needed for actual clinical application. Nevertheless, our findings suggest that RFID technology may provide an effective solution for preventing the retainment of surgical items during laparoscopic surgery.
Methods
Experimental Design and Equipment
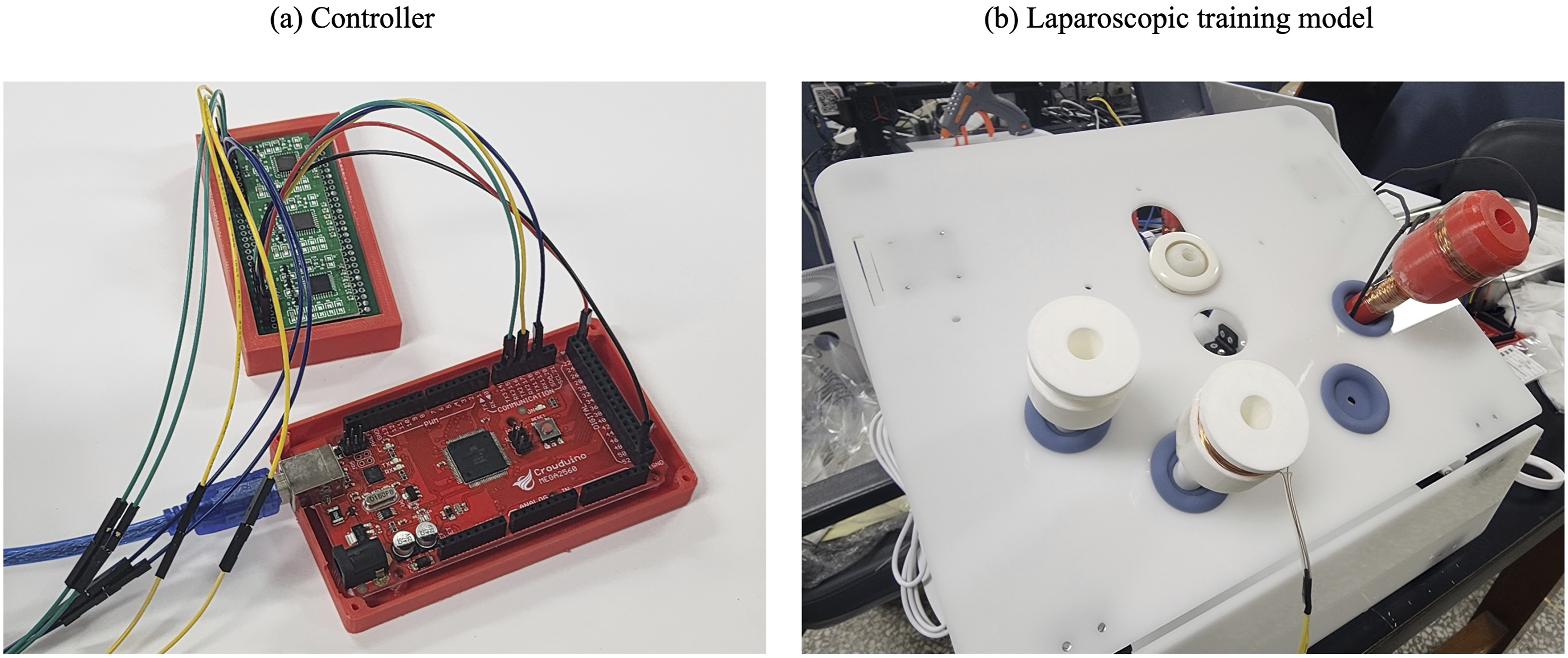
Three RFID detectors were integrated longitudinally into a standard 12-mm laparoscopic port, with each detector designated as the outer, middle, or inner detector from the external to internal direction of the port. Each detector consisted of a circular antenna coil (15 mm diameter) and an RFID reader module operating at 134.2 kHz frequency (Figure 1). This experiment was conducted using a laparoscopic training model to simulate the laparoscopic surgical environment (Figure 2). Schematic illustration of the RFID-based gauze detection system. (A) System diagram with outer, middle, and inner channels used to determine the direction of gauze movement. (B) Structure of the RFID port incorporating the three detection channels. (C) RFID-tagged gauze with a radiopaque marker, a polymer coating, and an embedded RFID tag Prototype controller and laparoscopic experimental setup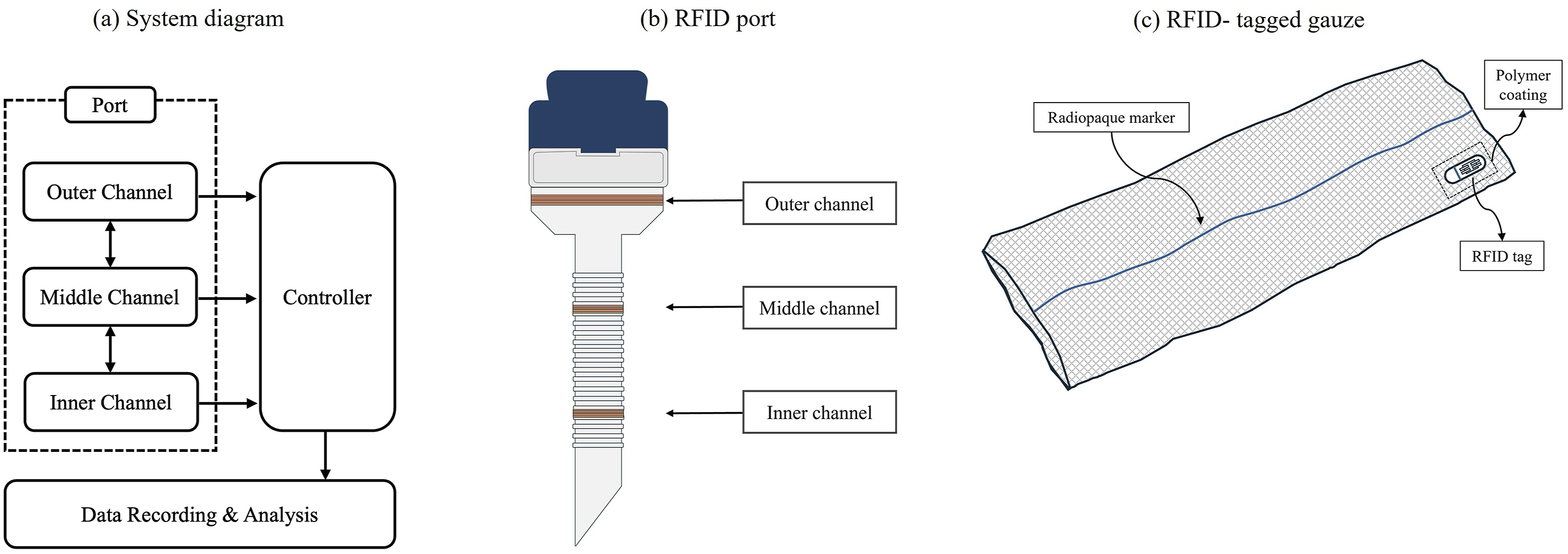
The detected signals were processed in real time through a microcontroller, with an RFID tag ID, a detection channel, and millisecond-precision timestamps for each event automatically recorded to a computer via USB serial communication. This multidetector configuration was designed to generate sequential detection patterns as gauze passes through the port, enabling accurate determination of movement direction.
Experimental Materials and Procedures
A total of 120 pieces of surgical gauze were initially prepared for the experiment, each affixed with a passive RFID tag (12 mm diameter, 0.5 mm thickness). Tags were secured 5 mm inward from the gauze edge using medical-grade silicone adhesive, and each piece of gauze was assigned a unique identification number. Prior to the experiment, all the tags were individually verified for proper functionality; two pieces of gauze were excluded because of detection errors during this verification process, resulting in 118 pieces of gauze for the final experiment.
The experiment was systematically conducted by dividing the 118 pieces of gauze into sets of 10-20 units. Each experimental set consisted of an entry phase and an exit phase. During the entry phase, the pieces of gauze were sequentially passed through the port from the external to the internal direction, maintaining a constant velocity to ensure complete port traversal. An interval of 2 s was maintained between the pieces of gauze to minimize signal interference. During the exit phase, the same pieces of gauze were passed in the opposite direction (internal to external) while maintaining identical velocities and intervals.
For data analysis, events were defined as follows: normal entry was classified as sequential detection of the same tag in the order of outer → middle → inner, whereas normal exit was classified as detection in the order of inner → middle → outer. Cases with detection failures or sequence abnormalities were recorded as abnormal events. Through this protocol, data from a total of 236 events (118 entries and 118 exits) were collected, and the system’s detection accuracy and directional discrimination reliability were evaluated.
Statistical Analysis
All the statistical analyses were performed using Python 3.8 and associated libraries (pandas, numpy, matplotlib). The primary performance metrics included the overall detection success rate, channel-specific detection success rate, and directional discrimination accuracy. The detection success rate was calculated as the ratio of successfully detected events to total expected events and is presented with 95% confidence intervals. Entry and exit events were treated as independent events for channel-specific detection analysis, while entry-exit pairs from the same piece of gauze were used to evaluate directional discrimination accuracy.
Results
RFID Detection Performance
RFID Detection Performance Summary
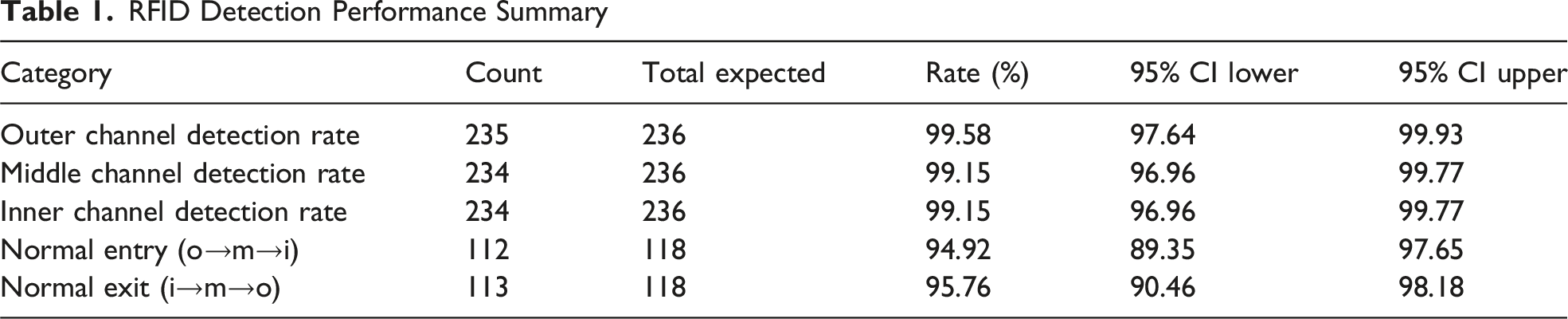
The channel-specific detection rates demonstrated excellent performance. In the outer channel, 235 out of 236 expected events were detected, yielding a detection rate of 99.58% (95% CI: 97.64-99.93). In the middle and inner channels, 234 out of 236 events were detected, with identical detection rates of 99.15% (95% CI: 96.96-99.77). All three channels demonstrated detection accuracies exceeding 99%, confirming minimal channel-specific detection failures.
Tag Detection Patterns and Anomaly Identification
Visualization of tag-specific movement patterns revealed diverse RFID tag detection sequences (Figure 3). In the representative normal movement pattern (Figure 3A), the tags were sequentially detected across the three channels. During the gauze entry phase, detection occurred in the sequence of outer → middle → inner channels, followed by a gauze retention phase, where the gauze remained within the operative field. In the gauze exit phase, detection occurred in the reverse order (inner → middle → outer channels), confirming the successful removal of the gauze. RFID-tagged gauze movement patterns through the triple-channel detection port. Representative time-channel trajectories. (A) Normal pattern (B) Duplicate outer channel detection suggesting tag re-entry attempts (C) Outer channel omission during exit indicating rapid removal or transient detection failure (D) Compound channel omission with direct outer-to-inner transition suggesting rapid manipulation or detection angle limitations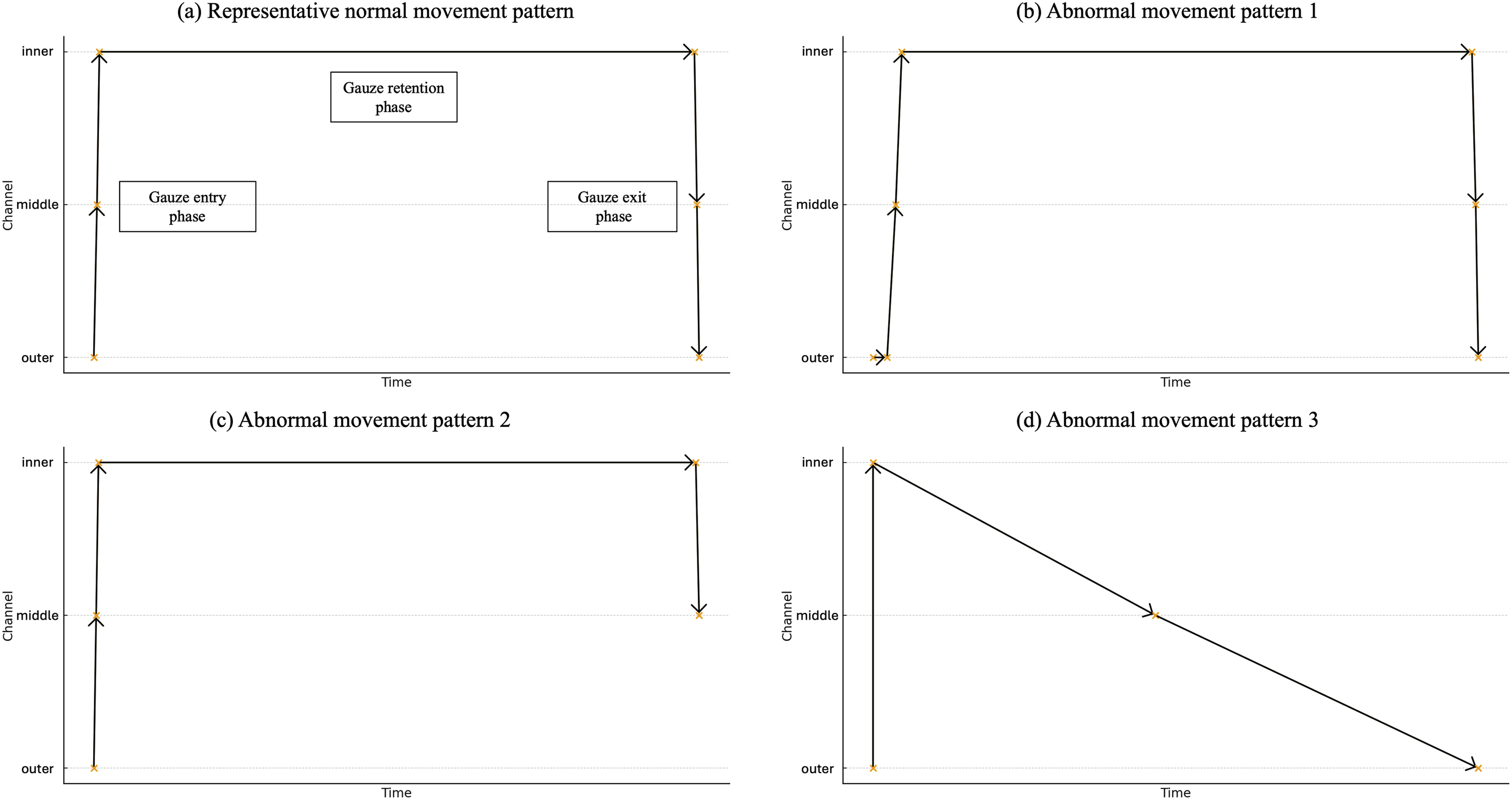
Abnormal detection patterns were observed in 4-5% of events and were classified into three types. The first abnormal pattern (Figure 3B) involved duplicate detection events in the outer channel during gauze entry. This phenomenon suggests temporary stagnation or re-entry attempts at the port entrance, where the tag remained within the outer channel’s detection range, resulting in repeated signal acquisition.
The second abnormal pattern (Figure 3C) involved no detection in the outer channel during the gauze exit phase. While normal events were detected in the inner and middle channels, the tag was not detected in the outer channel, potentially indicating rapid gauze removal or transient detection failure in the outer channel.
The third abnormal pattern (Figure 3D) involved compound channel omission. During entry, the gauze was not detected in the middle channel, with a direct transition from the outer channel to the inner channel, whereas the gauze was not detected in the inner channel during the exit sequence. These patterns suggest rapid gauze manipulation velocity or detection angle limitations in specific channels.
This analysis demonstrates that the entry/exit status and retention duration of each piece of gauze could clearly be identified. Despite the observed channel omissions or duplicate detections in select events, the detection success rate of the system exceeded 99%, and these anomalous patterns did not compromise the determination of the presence of gauze. The RFID system demonstrated robust tracking capability for surgical gauze despite various detection pattern anomalies. Even in the presence of anomalous detection patterns, visual analysis of the tag-specific detection sequences confirmed that the direction of gauze movement—entry or exit—could still be identified. The observed abnormalities, including channel omissions and duplicate detections, did not render the detection patterns uninterpretable with respect to gauze entry and exit status.
Gauze Retention Time Analysis
Analysis of the retention time distribution for 118 pieces of RFID-tagged gauze demonstrated the continuous tracking capability of the system (Figure 4). The entire experiment was conducted over approximately 55 minutes, with tags forming 6-7 distinct temporal clusters corresponding to the experimental sets of 10-20 pieces of gauze, as per the protocol. Retention time distribution of RFID-tagged gauze. Temporal tracking of 118 RFID-tagged pieces of gauze over 55 minutes. Each horizontal line represents an individual’s gauze retention time. The tags formed 6-7 clusters corresponding to experimental sets of 10-20 pieces of gauze, with a mean retention time of 3-5 minutes. A small subset (2.5-3.4%) showed shorter retention times, but all entry and exit events were successfully detected, demonstrating the ability to track multiple pieces of gauze simultaneously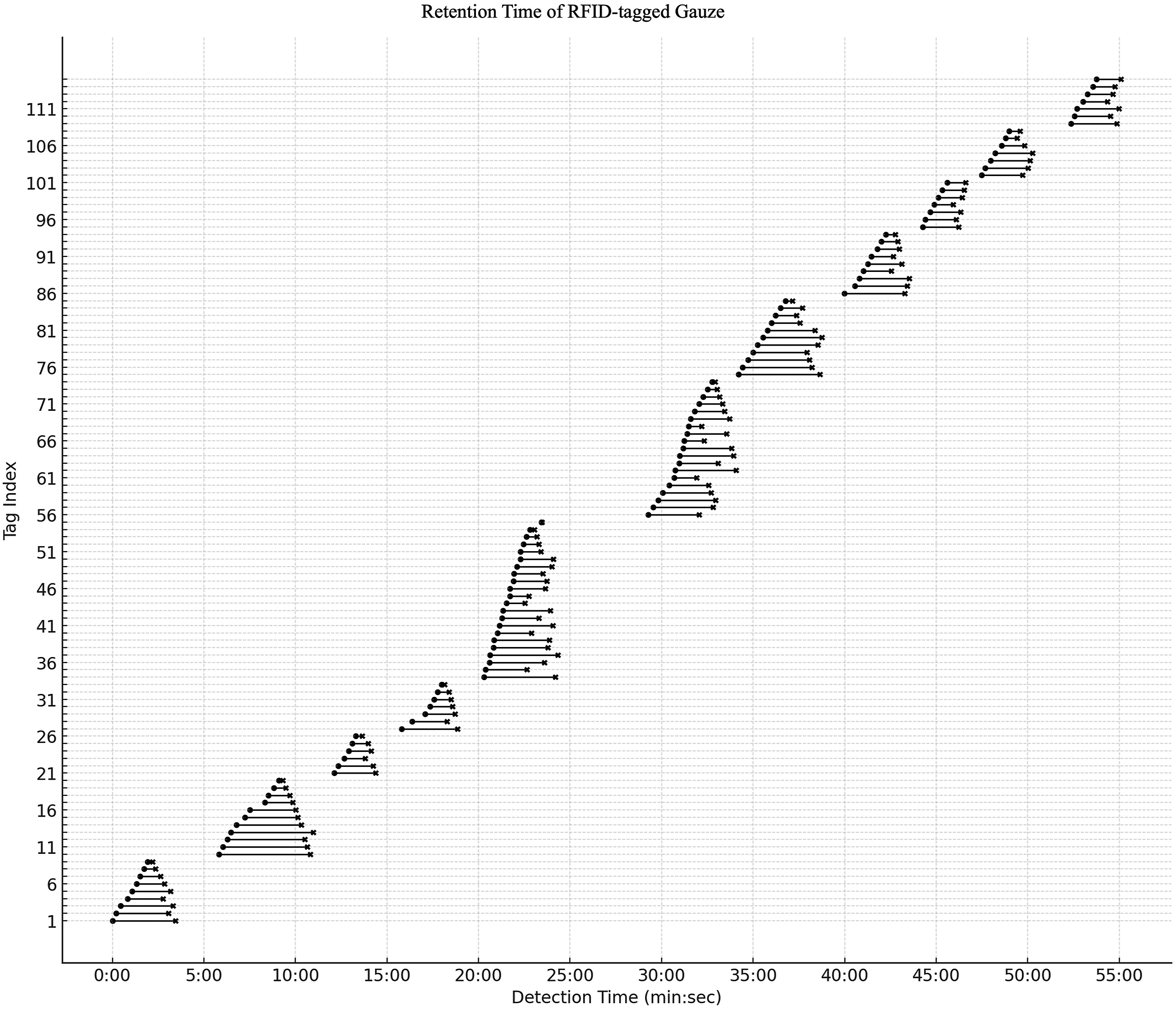
The mean retention time for each piece of gauze remained consistent at 3-5 min, indicating stable system performance under standardized experimental conditions. The pieces of gauze within the same experimental set showed near-simultaneous entry and exit patterns with similar retention durations, confirming the proper execution of the sequential insertion protocol with 2-second intervals.
Notably, only a small subset (approximately 3-4 pieces of gauze, 2.5-3.4%) of the 118 tags exhibited shorter-than-average retention times. These deviations occurred primarily near Tags 21, 36, and 56; however, entry and exit events were successfully detected in all the cases.
These findings demonstrate that the RFID system can simultaneously track multiple pieces of gauze while accurately recording individual retention times with millisecond precision. The clear temporal separation between experimental sets and the simultaneous tracking capability within sets suggest the feasibility of real-time monitoring of multiple pieces of gauze in actual surgical environments.
Discussion
In this proof-of-concept study, the technical feasibility of an RFID-based system with three detectors serially arranged within a laparoscopic port for the automated recognition and recording of the entry and exit of surgical gauze was evaluated, providing clear evidence of technical feasibility and initial performance. Analysis of 236 entry and exit events from 118 pieces of RFID-tagged gauze revealed detection rates of 99.58%, 99.15%, and 99.15% for the outer, middle, and inner channels, respectively, all exceeding 99%. Directional discrimination based on normal sequences yielded reproducibility rates of 94.92% and 95.76% for the entry and exit sequences, respectively. These findings demonstrate that spatial sequence information generated by multiple detectors arranged longitudinally along the port can reliably distinguish gauze entry and exit beyond simple presence detection.
The core innovation of this system is the “automated bidirectional counting” approach achieved through the triple-detector configuration. Conventional radiopaque-marked gauze and manual counting methods are vulnerable to human error, with increased error probability during emergency situations or shift changes.4,13 Additionally, radiographic imaging causes additional radiation exposure and time delays, with markedly reduced detection rates in patients with high BMI or significant bleeding.9,12 In contrast, this RFID system utilizes the 134.2 kHz low-frequency band to minimize signal attenuation from body fluids or tissues, recording both directionality and a unique ID for each piece of gauze passing through the port, thereby enabling automatic reconciliation of insertion and removal counts following the end of surgery.14,15
The observed abnormal detection patterns (4-5% of total events) were classified into three main types: duplicate detection in the outer channel, outer channel omission during the exit sequence, and partial channel omission during the entry or exit processes. These phenomena can be explained by physical manipulation speed, tag-antenna alignment, and minor positional variations at the port boundaries. Importantly, despite these abnormal patterns, directional discrimination was maintained in most cases, with two or more channels being detected in the normal sequence. In practical applications, these variations can be effectively managed through the implementation of duplicate suppression algorithms that process repeated signals from the same channel within a 300-500 ms time window as single events and interpolation algorithms that infer missing channels when detection events are recorded in two adjacent channels in sequence.16,17 With respect to gauze presence and absence determination, the current study confirmed that even when abnormal detection patterns were observed, visual analysis of the detection sequences demonstrated that gauze entry and exit could still be distinguished. The abnormal patterns did not prevent directional interpretation of the data. It should be noted, however, that an automated algorithm for tracking gauze presence or generating missing-exit alerts was not implemented in this study. Based on the demonstrated directional discriminability, we anticipate that future software development could translate this information into an automated retained-item detection system—for instance, by flagging any gauze whose entry is recorded but whose exit is not confirmed by the end of the procedure. Such an algorithm would represent a critical next step toward clinical deployment.
Time-tag index visualization analysis revealed clear interset demarcation and consistent retention times (mean 3-5 min), suggesting that the system can simultaneously track multiple pieces of gauze even in complex surgical environments. Throughout the 55-minute experiment, no systematic errors from signal interference or event overlap were observed despite 118 tags passing through in close temporal proximity, indicating stable system operation even in situations where multiple pieces of gauze frequently enter and exit during actual laparoscopic surgery.
From a clinical perspective, this system can be integrated into existing surgical workflows through real-time dashboard interfaces and appropriate alert strategies. When this system is implemented in parallel with existing management systems based on radiopaque markers and checklists, a multilayered safety system with complementary error profiles can be established. Millisecond-precision time recording enables the analysis of gauze usage patterns during the surgical phase, and automated surgical record management could be realized by integrating the proposed system with electronic medical record (EMR) systems.
Several practical considerations will need to be addressed before implementing this system in a clinical operating room environment. Regarding sterilization, the RFID port is designed as a single-use disposable device and therefore does not require compatibility with repeated sterilization cycles. However, the housing and encasing materials must be biocompatible and sterilization-resistant to ensure that the device can be supplied in a pre-sterilized state, typically achieved through ethylene oxide (EO) gas sterilization, which is well-suited for single-use devices incorporating electronic components. 18 In terms of equipment design, the current prototype functions as a direct replacement for a standard 12-mm laparoscopic trocar, which minimizes the need for additional ports or instruments and facilitates adoption without significant changes to existing surgical setups. The RFID-tagged gauze is intended to be supplied as pre-tagged, single-use disposable items, similar in form to currently available radiopaque-marked gauze, ensuring compatibility with existing sterile supply chains. The data communication interface will need to transition from the current USB serial connection to a wireless solution (eg, Bluetooth or Wi-Fi) to maintain a sterile field and allow seamless integration with OR display systems. Finally, a standardized alert protocol—including visual and auditory notifications for detected anomalies or unresolved gauze entries—will need to be developed and validated in collaboration with surgical teams to ensure that system alerts are actionable and do not disrupt surgical workflow.
However, this study has several important limitations. First, all the evaluations were performed in an in vitro environment that did not fully reflect actual operating room conditions, including the presence of body fluids and blood, organ contact, and the simultaneous use of complex instruments. Second, while the 134.2 kHz low-frequency band offers advantages for body fluid penetration, a systematic evaluation of potential electromagnetic interference from energy devices such as electrocautery or metallic instruments was not conducted. Third, a standardized protocol with gauze passage at a constant velocity with 2-second intervals was employed in the experiment; however, in actual surgery, gauze is inserted and removed irregularly at various speeds and angles. Additionally, situations in which multiple pieces of gauze pass through the port simultaneously or move in partially overlapping states were not evaluated. Fourth, the effectiveness of real-time correction algorithms for the observed 4-5% abnormal patterns was not verified, and optimal parameters for the proposed 300-500 ms time window and channel interpolation rules were not validated across diverse scenarios. Furthermore, empirical data concerning how surgical teams respond to system alarms or warnings and how such interactions impact overall surgical flow remain insufficient.
In future research, performance and electromagnetic immunity should be evaluated across various laparoscopic scenarios, institutions, animal models and clinical environments. Furthermore, software algorithms, including time window-based duplicate suppression, partial channel interpolation, and machine learning-based pattern recognition, should be implemented and optimized to create real-time processing pipelines, which are particularly important. Moreover, standard operating protocols and training systems, including user interfaces, alert policies, and rescan rules, must be established to seamlessly integrate the technology into actual workflows. Clinical evidence can be further strengthened by the presentation of quantitative metrics for cost-effectiveness, impact on surgical time, and RSI prevention efficacy.
In conclusion, the proposed 3-channel RFID port system achieved detection rates exceeding 99% per channel and approximately 95% directional sequence reproducibility in a laboratory environment, with abnormal patterns appearing within manageable ranges, as determined using software and operational protocols. These results clearly demonstrate the technical feasibility of this system as an automated safety device for potentially reducing the risk of gauze retention in laparoscopic surgery, and subsequent clinical validation and optimization of this system will contribute to its clinical translation and enhanced patient safety in actual operating rooms.
Conclusion
This proof-of-concept study demonstrated that a 3-channel RFID system integrated into a laparoscopic port can achieve high technical performance in automated tracking and directional discrimination of surgical gauze. Detection rates exceeding 99% per channel and a directional discrimination accuracy of approximately 95% indicate sufficient potential as a foundational technology for potentially reducing the risk of gauze retention. Abnormal detection patterns were observed in 4-5% of events, and analysis of the characteristics and causes of these patterns provided directions for future system improvements. The results experimentally confirm that RFID technology can be used to distinguish and track gauze entry and exit in real time during laparoscopic surgery. However, the clinical application of the proposed system will require performance validation in in vivo environments, the development and verification of correction algorithms for abnormal patterns, and additional research on integration strategies with operating room workflows.
Footnotes
Acknowledgments
English language editing was provided by American Journal Experts (AJE). During the preparation of this revised manuscript, the authors used an AI language tool (Claude, Anthropic) to assist with drafting and refining portions of the text. The authors have reviewed and take full responsibility for the accuracy and integrity of all content.
Consent to Participate
No human participants/data/tissue were involved.
Author Contributions
Jae Kyun Park: Investigation (data acquisition), Data curation, Formal analysis, Visualization, Writing—original draft. Hwan Yi Joo: Methodology, Device development, Software/Data acquisition support, Writing—review & editing. Dae Hwan Kim: Investigation (data acquisition), Data curation, Writing—review & editing. Tae Yong Jeon: Investigation (data acquisition), Writing—review & editing. Seokyoung Ahn: Conceptualization, Methodology, Supervision, Writing—review & editing, Corresponding author. Chang-In Choi: Conceptualization, Project administration, Supervision, Funding acquisition, Writing—review & editing, Corresponding author. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Biomedical Research Institute Grant (202400700001) from Pusan National University Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.