
Abstract
Background
Artificial intelligence (AI) and machine learning are transforming neurosurgical research and practice, yet the programming barrier has excluded most clinicians from building customized digital tools. Vibe coding — generating functional software through natural language instructions to large language models — has substantially lowered this barrier since its formalization in 2025. No study has examined its applications specifically within neurosurgery.
Methods
A narrative review of the literature was conducted using PubMed, Google Scholar, and preprint repositories through April 2026, supplemented by the author’s direct clinical experience developing vibe-coded tools in a tertiary neurosurgical unit.
Findings
Existing literature on vibe coding in medicine is sparse and limited to non-surgical specialties; no prior publication addresses it in a neurosurgical context. Three practical domains of application are identified: (1) research data collection and multi-scale patient classification, illustrated by a personally developed integrated scoring tool for aneurysmal subarachnoid hemorrhage (Figure 1); (2) clinical workflow optimization including documentation and follow-up automation; and (3) educational tool development and literature engagement.
Conclusion
Vibe coding represents an accessible paradigm enabling neurosurgical trainees to develop purpose-specific digital tools without programming expertise. The field lacks specialty-specific guidance on this approach. This review aims to address that gap and encourage adoption of vibe coding as a practical complement to institutional digital health infrastructure.
Keywords
Introduction
The integration of artificial intelligence (AI) and machine learning (ML) into neurosurgical practice has accelerated markedly over the past decade. Applications span preoperative imaging analysis, intraoperative navigation, postoperative outcome prediction, and resident education.1,2 Despite this momentum, a persistent gap remains between the availability of AI tools and their practical accessibility to individual clinicians — particularly trainees operating within resource-constrained environments.
A fundamental obstacle has been the programming barrier. Neurosurgery, despite its position at the intersection of technology and medicine, has paradoxically lagged behind other medical specialties in the adoption of clinician-built digital tools. Cardiologists annotate arrhythmias with custom ML pipelines; radiologists deploy departmental AI screening tools; endocrinologists now publish vibe-coded classification models. 3 The neurosurgical trainee, meanwhile, continues to calculate Hunt-Hess grades by hand, transcribe the same patient data into four separate scoring instruments, and draft discharge summaries from memory — not because these tasks cannot be automated, but because the path from clinical need to functional software has historically required programming expertise that training programs do not provide and residents do not have time to acquire. 4
In February 2025, AI researcher Andrej Karpathy coined the term “vibe coding”5 to describe a fundamentally different approach: the user communicates intended software behavior in plain natural language, and a large language model (LLM) generates, tests, and iteratively refines the corresponding code4. The user need not understand the underlying syntax — only the desired outcome. This paradigm has since been recognized as a transformative development in biomedical software development, and preliminary evidence from non-surgical specialties suggests it can enable clinicians without formal programming backgrounds to implement machine learning pipelines, build interactive clinical calculators, and automate data workflows within hours rather than months.3,5 Crucially, the barrier to entry is lower than neurosurgeons may assume: a functional, validated clinical tool can be produced in a single afternoon, using only a browser and natural language — no programming knowledge required.
Neurosurgery, as a specialty defined by high decision-making complexity, demanding documentation requirements, and a rapidly expanding evidence base, stands to benefit considerably from this approach. Yet the neurosurgical literature has not addressed vibe coding. This narrative review synthesizes the emerging evidence, identifies the current literature gap, and presents concrete applications drawn from direct clinical experience — with the aim of providing a practical foundation for neurosurgeons and trainees seeking to harness this technology.
State of the Literature: An Identified Gap
A narrative review of the literature was conducted through searches of PubMed, Google Scholar, and major preprint repositories (bioRxiv, medRxiv) from inception through April 2026, using terms spanning vibe coding, LLM-assisted software development, AI-generated clinical tools, and their intersections with clinical medicine and neurosurgery; citation tracing supplemented electronic search. Given that the term itself entered scientific discourse in February 2025, the field is not yet amenable to formal systematic synthesis, and PRISMA reporting criteria were not applied. The resulting body of literature is strikingly sparse: as of early 2026, peer-reviewed publications on clinician-oriented vibe coding in medicine number fewer than ten, none of which address a surgical specialty. This nascent evidence base reflects the chronological novelty of the field rather than a gap in the present review’s scope.
The most substantive contribution is that of Lee and Huh, 3 who demonstrated in an endocrinology context that clinicians without Python expertise can use LLM-driven vibe coding to implement supervised ML classification pipelines on clinical datasets. Pesce and Cheungpasitporn 6 similarly demonstrated vibe coding’s utility in nephrology education, developing four open-source, AI-assisted web-based applications — including clinical calculators and pathophysiology visualizers — through a clinician-led, natural-language-to-code workflow without formal programming training. Moore and Tatonetti 5 described vibe coding as a paradigm shift for biomedical software development broadly, arguing that it compresses the development cycle from concept to functional prototype. Abgrall et al, 7 writing in The Lancet, introduced the complementary concern of “vibe caring” — the risk that clinicians may accept AI-generated outputs without scrutinizing the underlying reasoning — and proposed institutional safeguards.
The broader neurosurgical AI literature, while substantially larger, has not converged on the question of individual clinician-built tools. Reviews by Dagi et al 1 and Celtikci 8 provide authoritative overviews of ML applications in neurosurgery but address institutional and research-grade systems rather than tools built by individual trainees for immediate clinical use. Yangi et al 2 and others survey deep learning applications across neurosurgical subspecialties with similarly large-scale framing. The gap is consistent: AI in neurosurgery is discussed at the systems level, not at the level of the individual clinician who needs a scoring calculator, a discharge template, or a follow-up tracker by tomorrow morning.
This absence is not merely a bibliographic curiosity. It reflects a structural disconnect between the AI tools that neurosurgical research celebrates and the digital tools that neurosurgical residents actually use — or more precisely, lack. The present review is, to the author’s knowledge, the first to address vibe coding specifically within a neurosurgical context.
Vibe Coding: Definition and Available Platforms
Vibe coding is formally defined as a goal-oriented software development process in which the user specifies desired functionality through natural language, and an LLM generates, tests, and refines the corresponding code through iterative feedback loops. 3 The critical distinction from conventional AI-assisted coding — in which programmers use LLMs to accelerate writing code they already understand — is that vibe coding requires no prior programming knowledge. The user communicates intent; the AI handles implementation.
A practical taxonomy of available platforms is useful for clinicians approaching this field for the first time. Web-based conversational AI systems (such as ChatGPT, Claude, and Gemini) allow a user to describe desired functionality and receive complete, deployable code in a single exchange. GUI-based development environments (such as Replit and Bolt) add an interface layer that allows non-programmers to run, test, and iterate on generated code without command-line interaction. AI-augmented code editors (such as Cursor and Visual Studio Code with Copilot) offer the greatest flexibility but require basic familiarity with development environments. For most neurosurgical trainees, web-based platforms represent the lowest barrier to entry and are sufficient for the majority of clinical tool development described in this review.
A typical vibe coding session for a clinical tool begins with a natural language specification: “Build an HTML page that calculates the Hunt-Hess grade, WFNS grade, Fisher grade, modified Fisher grade, and SAFIRE score from a shared set of clinical inputs, and displays all scores simultaneously.” The LLM generates a complete, functional prototype. The user reviews the output, identifies refinements — clinical logic errors, interface preferences, additional features — and communicates them in plain language. The cycle repeats until the tool meets clinical requirements. A complete, validated clinical scoring application can typically be produced in 2 to 4 hours by a first-time user.3,5
Applications in Neurosurgical Practice
Research Data Collection and Patient Classification
Neurosurgical research is disproportionately dependent on accurate retrospective classification of patients according to multiple overlapping severity scales. Aneurysmal subarachnoid hemorrhage (aSAH) exemplifies this challenge with particular clarity. Standard practice requires simultaneous or sequential application of the Hunt-Hess grading scale, the World Federation of Neurosurgical Societies (WFNS) grade, the Fisher grade, the modified Fisher grade, and increasingly the SAFIRE score 9 — each derived from overlapping but distinct clinical and radiological parameters, alongside Glasgow Coma Scale (GCS) assessment. Performing these calculations sequentially using reference texts or isolated online calculators introduces transcription latency between instruments, increases the risk of inter-rater inconsistency arising from shared input variables entered independently into separate tools, and consumes time that is structurally unavailable during acute assessment.
Using vibe coding, the author developed a browser-based integrated scoring application for aSAH that consolidates all of the above instruments within a single interactive interface. The application accepts a unified clinical input set — GCS components (eye, verbal, motor), presence of focal motor deficit, CT-based blood volume and distribution, and intraventricular hemorrhage status — and simultaneously computes all relevant scores with real-time display. Crucially, the tool also generates an estimated probability of poor functional outcome (modified Rankin Scale 4-6) at 2 months via the SAFIRE algorithm, providing immediate prognostic context at the point of data entry. The tool required no manual code writing, was developed through iterative natural language prompts to a web-based LLM, and was refined over approximately 3 hours to match the input conventions and display preferences of the clinical team (Figure 1). Browser-based integrated aneurysmal subarachnoid hemorrhage (aSAH) scoring application developed through vibe coding. (A) Individual scale input interface, illustrated using the Hunt-Hess grading screen; clinical parameters are entered once and propagate across all instruments. (B) SAFIRE multi-parameter calculation screen, demonstrating simultaneous input of aneurysm size, patient age, and WFNS grade. (C) Integrated summary view displaying all six scoring instruments simultaneously with real-time computed values and prognostic output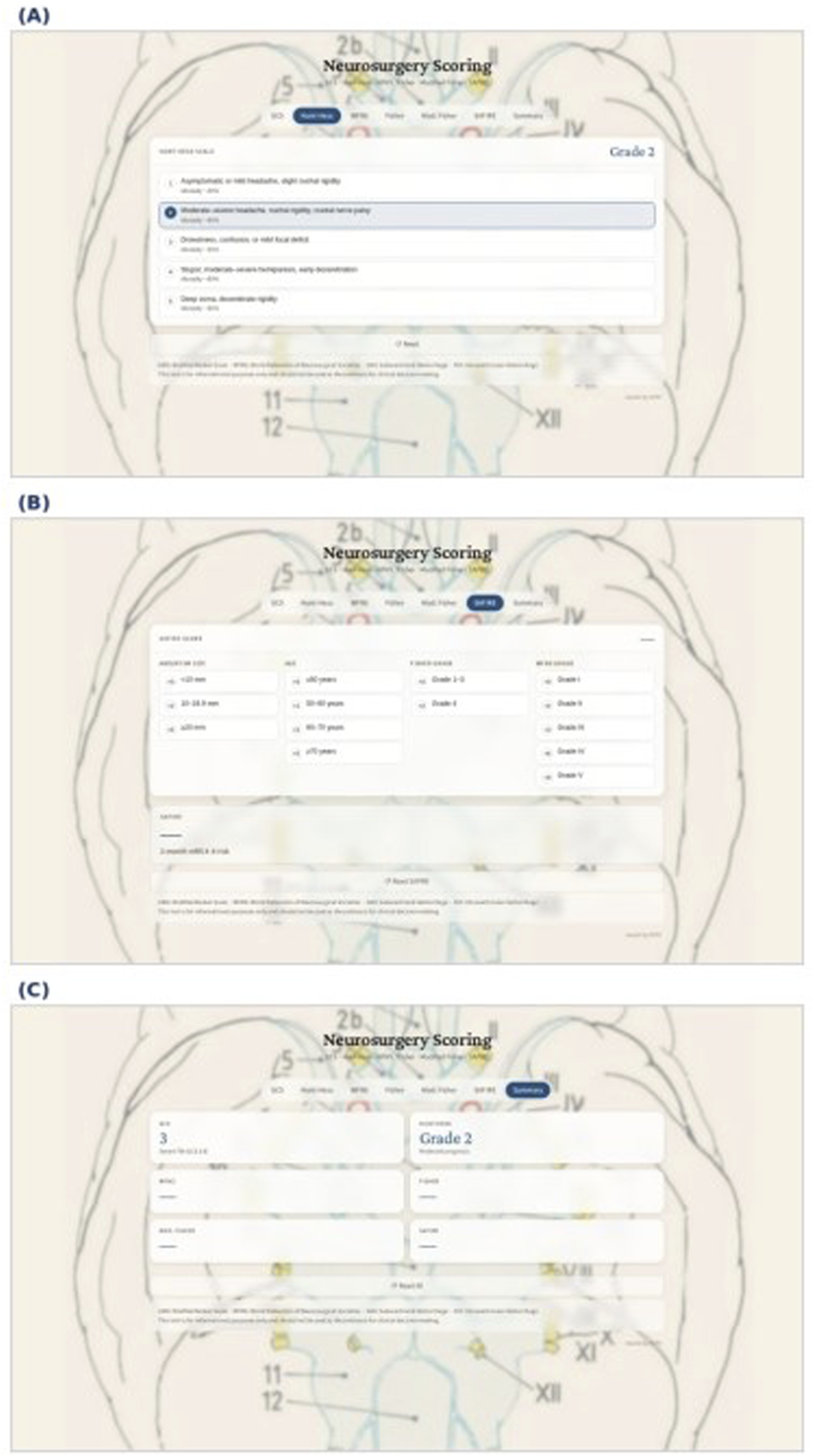
The research utility of this tool extends beyond speed. By enforcing a shared input set, the application prevents the category of inconsistency that arises when GCS-derived variables — particularly the motor component, which contributes to both GCS and WFNS grade — are transcribed independently for each instrument and differ between entries due to rounding or re-assessment. For retrospective dataset construction, this internal consistency constraint materially improves data quality. The approach generalizes readily: similar integrated tools can be constructed around spinal cord injury classification (ASIA, AO Spine TLICS), tumor grading, intracranial pressure management thresholds, or any domain requiring simultaneous multi-scale patient classification.
Clinical Workflow Optimization
The administrative burden on neurosurgical trainees is substantial and well-documented. 4 Discharge documentation, operative note templates, post-craniotomy patient instruction sheets, consent documentation, and follow-up scheduling each require time that is structurally diverted from operative training and direct patient care. Many of these tasks share a common characteristic: they are repetitive, template-driven, and highly amenable to automation — yet institutionally provided digital solutions are frequently absent, generically designed, or encumbered by procurement timelines incompatible with the pace of clinical need.
Vibe-coded tools address these gaps at the individual or departmental level without infrastructure investment. A trainee can generate a neurosurgical discharge summary template pre-populated with diagnosis-specific fields and institutional formatting conventions, a patient-facing post-craniotomy or post-aneurysm coiling instruction sheet calibrated to an appropriate reading level, or a follow-up tracking dashboard that flags patients overdue for imaging or neurology review. Each represents a need that institutional IT systems do not reliably meet but that can be addressed in an afternoon using current LLM platforms.
The clinical significance is not purely logistical. Tools that reduce cognitive load during administrative tasks may indirectly preserve attentional resources for patient-facing decisions — a consideration of particular relevance in a specialty where cognitive fatigue and documentation burden have been identified as contributing factors in adverse events. 4 As the neurosurgical literature on ambient AI documentation systems grows, individual-scale vibe-coded tools represent a complementary, immediately accessible tier of the same overall strategy.
Surgical Education and Literature Engagement
Neurosurgical education demands simultaneous mastery of complex anatomy, operative technique, and a continuously expanding scientific evidence base. Vibe coding enables trainees to create interactive educational tools — anatomy quiz applications, surgical decision-making simulators, visual mnemonics for classification systems, and case-based learning platforms — that would previously have required collaboration with a software developer. A trainee who recognizes a personal knowledge gap can now build a targeted learning tool to address it within hours and share it with peers facing the same challenge.
The literature engagement problem is equally tractable. The volume of neurosurgical publications has grown substantially, and systematic engagement with the evidence base is increasingly difficult within training time constraints. Vibe-coded interfaces to AI-powered literature summarization services, structured critical appraisal tools organized around PICO frameworks, or custom reference management dashboards can be tailored to the specific topics a resident is studying — providing a level of personalization that commercial platforms rarely offer.
Lee and Huh 3 demonstrated that clinicians without Python expertise can, through vibe coding, implement complete ML classification pipelines on clinical datasets. The broader implication — that the bottleneck in clinician-driven research is shifting from technical skill to data quality — applies with particular force in neurosurgery, where large imaging and outcomes datasets are increasingly available but analytical capacity remains unevenly distributed. The ability to build custom data preprocessing, visualization, and preliminary analysis tools without formal programming training represents a meaningful and democratizing shift in research accessibility.
Beyond the aSAH application, the same vibe coding approach has been extended within the authors’ department to produce bedside scoring calculators integrating additional neurological and intensive care instruments — including tools relevant to traumatic brain injury classification and post-operative neurological monitoring — each built through iterative natural language prompts without manual code authorship. Separately, early exploratory work has been undertaken toward three-dimensional anatomical visualization of operative approaches using publicly available model-hosting platforms; this work remains in development, and no validated educational product has been produced to date. These efforts, while preliminary, illustrate that the vibe coding paradigm extends naturally across the range of educational and clinical domains encountered in neurosurgical training.
Technical Considerations and Limitations
Enthusiasm for vibe coding in clinical settings must be tempered by clear-eyed awareness of its limitations. Applications handling patient-identifiable information must comply with applicable data protection legislation; browser-based tools should be evaluated for whether patient data is transmitted to external servers, and offline-capable or locally hosted implementations should be preferred for clinical applications involving sensitive data. Institutional information governance teams should be consulted before deploying vibe-coded tools in formal clinical workflows.
The LLM-generated code underlying vibe-coded tools is not inherently validated for clinical use. Logical errors may be non-obvious to a clinician reviewing only the interface rather than the underlying implementation — a phenomenon directly relevant to the “vibe caring” concern articulated by Abgrall et al 7 Tools computing prognostic scores that influence clinical management must be independently verified against published scoring criteria by a clinical expert before deployment. For research applications, outputs should be cross-validated against manually calculated reference values on a sample of cases before the tool is used for dataset construction.
There is also a risk of departmental fragmentation: an environment in which each trainee independently develops overlapping tools may generate an unmaintained informal software ecosystem. Establishing lightweight peer review norms — sharing tools through departmental repositories, version-tagging validated releases, and documenting the clinical logic verification process — can mitigate this risk without imposing the overhead of formal software governance. Professional societies may usefully develop guidance on minimum verification standards for clinician-built clinical tools.
Pending specialty-specific consensus, the authors propose a three-stage minimum validation framework applicable to vibe-coded clinical tools (Figure 2). This framework was prospectively applied to the integrated aSAH scoring tool described in this review: algorithmic outputs were verified against manually calculated reference values across ten consecutive cases (Stage 1), outputs were reviewed independently by a senior resident blinded to the developer’s calculations (Stage 2), and intended use was documented as a research data-collection aid within an ethics-approved prospective outcomes study (Stage 3). No discrepancies were identified at any stage. Proposed three-stage minimum validation framework for vibe-coded clinical tools. Stage 1 (Developer Self-Check): Algorithmic verification against primary published sources with case-level cross-validation. Stage 2 (Independent Clinical Review): Blinded assessment by a senior resident or attending physician with attention to interface logic and edge-case behavior. Stage 3 (Use Context Documentation): Explicit documentation of intended use with escalating oversight requirements proportional to patient-facing risk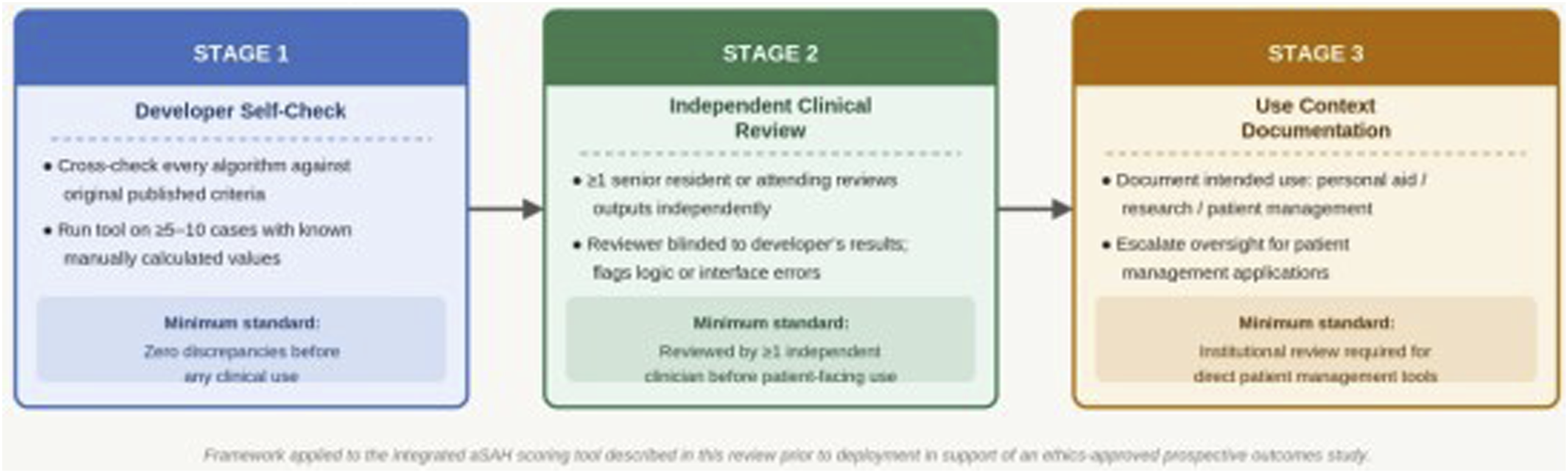
Future Directions
The trajectory of LLM capability suggests that vibe coding will become progressively more accessible and the tools produced progressively more sophisticated. Near-term developments likely to be relevant to neurosurgery include native integration of vibe-coded tools with electronic health record systems through standardized APIs, enabling real-time data ingestion rather than manual entry; multimodal LLM platforms capable of processing radiological images as inputs to vibe-coded classification tools; and LLM-driven quality assurance mechanisms that automatically flag inconsistencies between tool outputs and published reference values.
Applications of Vibe Coding in Neurosurgical Practice: A Domain-Based Overview
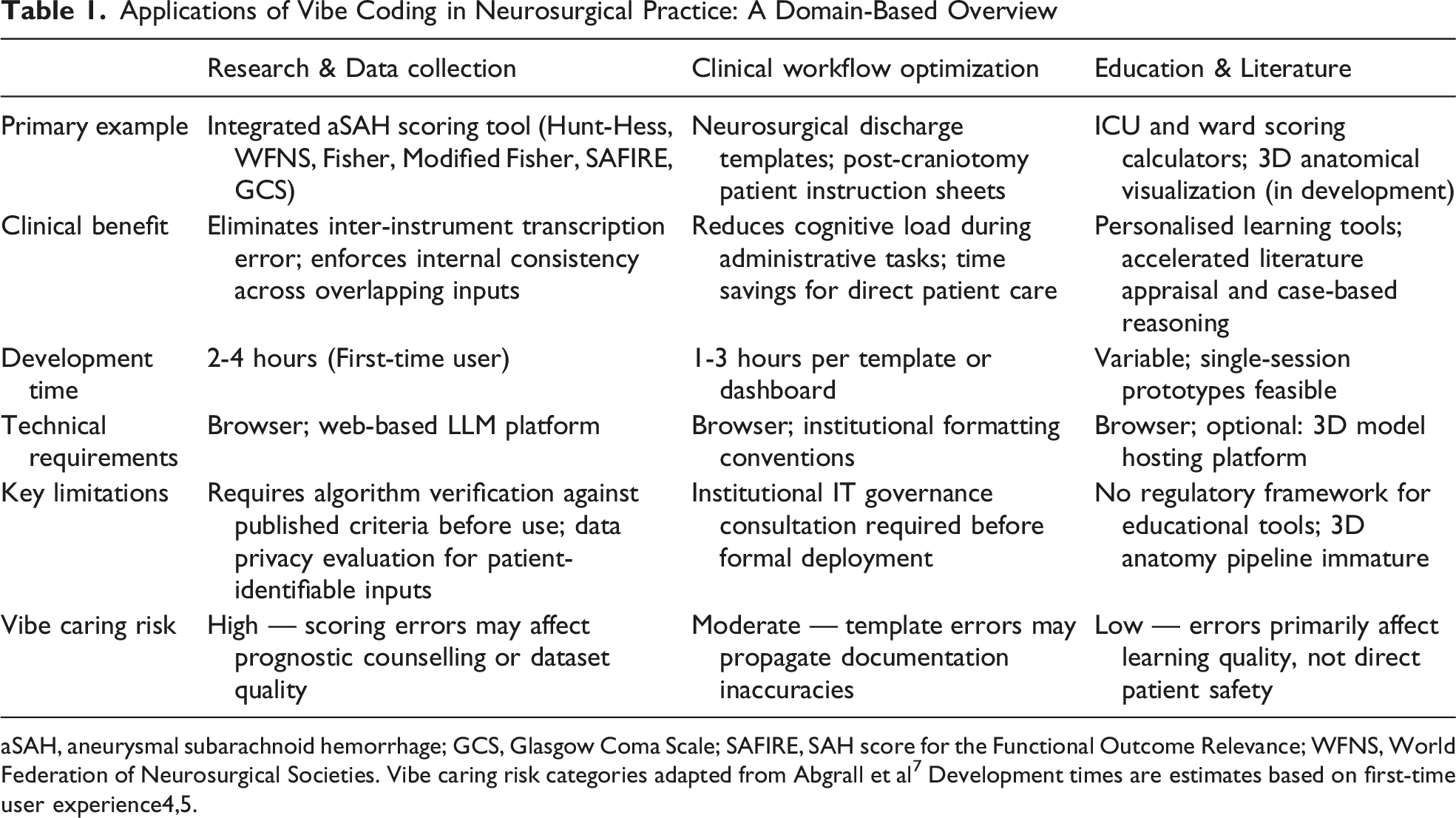
aSAH, aneurysmal subarachnoid hemorrhage; GCS, Glasgow Coma Scale; SAFIRE, SAH score for the Functional Outcome Relevance; WFNS, World Federation of Neurosurgical Societies. Vibe caring risk categories adapted from Abgrall et al 7 Development times are estimates based on first-time user experience4,5.
Conclusion
Neurosurgery is a specialty that leads medicine in technical sophistication yet has, at the trainee level, remained largely dependent on paper forms, manual scoring, and generic documentation templates. The tools to change this have existed, in principle, for years — but the programming barrier excluded most clinicians from using them. Vibe coding removes that barrier. The integrated aSAH scoring application described in this review — consolidating six clinical instruments, providing real-time prognostic estimates, and eliminating inter-instrument transcription errors — was built without a single line of manual code. It is in daily use for both clinical assessment and research data collection. It took one afternoon to build. This is not an exceptional achievement; it is a repeatable one, available to any neurosurgical trainee with a clinical problem and an internet connection. The neurosurgical literature has not yet engaged with this paradigm despite the availability of the technology and the clarity of the need. This review aims to initiate that engagement. The daily burden of manual scoring, redundant documentation, and fragmented administrative tasks is not a fixed condition of neurosurgical training — it is a solvable problem, and vibe coding is a practical tool for solving it.
Footnotes
Acknowledgements
The author gratefully acknowledges the use of Claude (Anthropic, San Francisco, CA, USA), a large language model, for English language editing assistance during the preparation of this manuscript. The author also acknowledges the foundational contributions of Andrej Karpathy in conceptualizing the vibe coding paradigm, and the open-access LLM platforms that enabled the development of the clinical tools described in this work.
Ethical Considerations
This narrative review did not involve patient data and did not require ethical approval. The integrated aSAH scoring tool described herein was developed as a clinical support aid; its subsequent use for structured data collection in a prospective outcomes study was conducted under a separate institutional ethics committee approval obtained for that study.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Artificial Intelligence Use Statement
Artificial intelligence (AI)-assisted tools were used in the preparation of this manuscript. Specifically, a large language model (Claude, Anthropic) provided language editing assistance to improve clarity, grammar, and academic expression in English, a non-native language of the author. Additionally, AI-assisted software development (vibe coding) was employed in the creation of the integrated aSAH scoring tool described herein, as detailed in the manuscript. All intellectual content, clinical judgments, interpretations, and conclusions are the sole responsibility of the author, who reviewed and approved the final manuscript in its entirety. AI tools were not used for data generation, analysis, or the formulation of scientific conclusions.