
Abstract
Background
Breast tumors located in the lower inner quadrant remain challenging in oncoplastic surgery due to limited tissue volume and the risk of unsatisfactory cosmetic outcomes. This study describes a surgical technique developed to address these challenges while maintaining oncologic principles.
Methods
A retrospective descriptive analysis was performed on 5 consecutive patients with lower inner quadrant breast tumors who underwent breast-conserving surgery between January 2025 and March 2026 using this technique. The approach is based on a triangular design, mobilization of a superior glandular flap, and placement of the incision within the inframammary fold without manipulation of the nipple–areola complex.
Results
The planned surgical design was achieved in all cases. Negative surgical margins were obtained in all patients. No major postoperative complications, including wound complications or nipple–areola complex ischemia, were observed. Early postoperative assessment demonstrated satisfactory breast contour and symmetry.
Conclusion
This technique may be considered a feasible option for selected patients with lower inner quadrant tumors. The initial findings suggest favorable early oncologic and aesthetic outcomes. Further studies with larger cohorts and longer follow-up are needed to confirm these results.
Keywords
Background
Oncoplastic techniques in the treatment of breast cancer have expanded the indications for breast-conserving surgery while improving cosmetic outcomes. 1 Oncoplastic surgery has also been shown to provide favorable cosmetic and patient-reported outcomes while maintaining acceptable oncological safety, making it an increasingly important approach in breast surgery. 2 Despite these advantages, the success of oncoplastic reconstruction depends largely on tumor location, breast size, parenchymal distribution, and the expected extent of skin or glandular resection. However, in patients with small breast volume and relatively large tumors, achieving clear surgical margins while preserving satisfactory aesthetic outcomes remains a major challenge. 3
In particular, tumor location is a key factor in both surgical planning and aesthetic outcomes, as different quadrants require tailored reconstructive approaches. 4 Breast tumors located in the lower inner quadrant present additional challenges for oncoplastic surgery, as volume deficiency in this region may more easily result in unsatisfactory aesthetic outcomes. 5
Given these challenges, we present a novel oncoplastic technique for lower inner quadrant tumors that prioritizes patient satisfaction while aiming to overcome the reconstructive limitations associated with this region.
Method
Study Design and Patient Selection
This study was designed as a single-center, retrospective descriptive analysis evaluating a novel oncoplastic technique (Dogan Technique) for breast tumors located in the lower inner quadrant. Between January 2025 and March 2026, 5 consecutive patients with lower inner quadrant breast tumors who underwent breast-conserving surgery using this technique were included. Eligible patients had unifocal breast tumors located in the lower inner quadrant (4-5 o’clock in the right breast and 7-8 o’clock in the left breast), at a sufficient distance from both the nipple–areola complex and the inframammary fold, such that closure of the defect would not require displacement or repositioning of the nipple–areola complex, and requiring skin resection. The technique was considered suitable only when adequate residual breast tissue was present between the tumor and the inframammary fold to allow creation and mobilization of a glandular flap. Patients with multicentric disease, tumors extending to or immediately adjacent to the inframammary fold, prior breast surgery in the same quadrant, inflammatory breast cancer, or contraindications to breast-conserving surgery were excluded. No specific restrictions regarding histological subtype were applied.
The study was conducted in accordance with the Declaration of Helsinki, and ethical approval was obtained from the Institutional Research Ethics Committee (approval number: AEŞH-BADEK-2025-447).
Procedure
This technique was designed for tumors located in the lower inner quadrant (at the 4-5 o’clock position in the right breast and the 7-8 o’clock position in the left breast), distant from both the areola and the inframammary fold, and requiring skin resection. In non-palpable lesions, preoperative skin marking is performed under ultrasound guidance by centering the tumor location and drawing a circular marking with a 1-cm radius. The medial and inferior borders are determined using the sternum medially and the inframammary fold inferiorly as anatomical landmarks. A triangular pyramid design is then planned with its base positioned along the inframammary fold. One of the key principles of the design is the intersection of the peak point of the triangular pyramid with the superior margin of the tumor (Figure 1). Preoperative marking and triangular design
The defined pyramid is divided into two components, resulting in a parallelogram and a triangular segment. The inferior triangular area represents the region designated for de-epithelialization. The superior parallelogram is designed as the resection area (Figure 2). In non-palpable tumors, intraoperative specimen imaging may be performed to confirm adequate tumor resection (Figure 3). A separate mini-axillary incision was used for sentinel lymph node biopsy. Inferior triangular area designated for de-epithelialization Tumor resection within the planned resection area
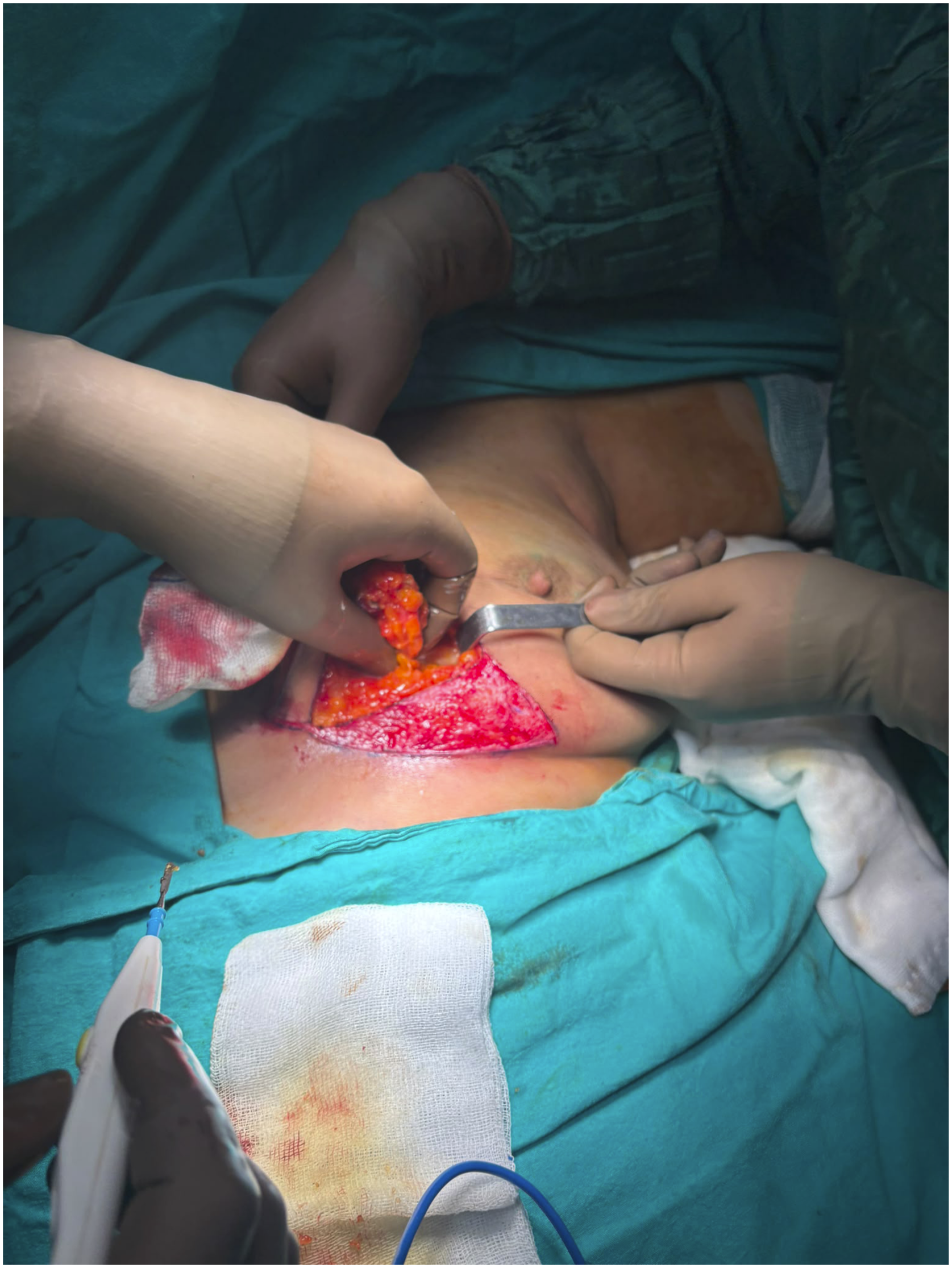
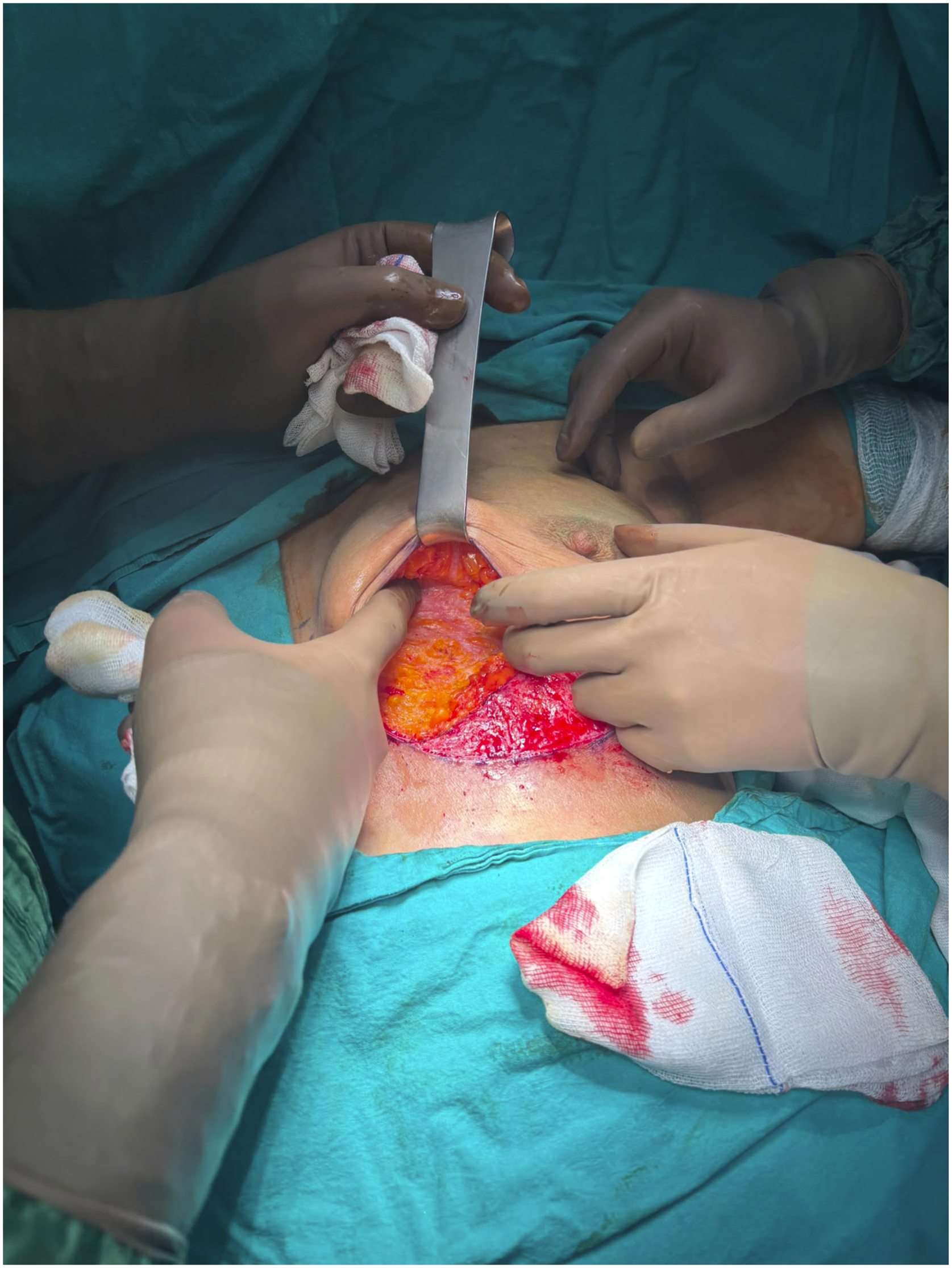
Following tumor resection, a superior glandular flap is created (Figure 4). After achieving hemostasis, the surgical cavity is marked with clips, and a silicone drain may be placed when necessary. The glandular flap is mobilized in the subcutaneous and prepectoral plane to provide adequate tissue mobility (Figure 5). Superior glandular flap prepared after tumor excision Subcutaneous and prepectoral mobilization of the glandular flap
To achieve complete closure of the surgical defect, the glandular flap is sutured to the superior margin of the de-epithelialized area using 2-0 Vicryl sutures. The superior skin incision line is then approximated to the inferior border of the de-epithelialized area using 3-0 rapid absorbable sutures (Figure 6). This technique results in a concealed scar positioned along the inframammary fold (Figure 7). Advancement of the superior glandular flap to obliterate the surgical defect Immediate postoperative appearance with inframammary incision

Cosmetic Assessment
Cosmetic outcomes were independently evaluated by two breast surgeons using standardized postoperative photographs obtained at the 30-day follow-up visit. Breast symmetry, breast contour, scar visibility, and nipple–areola complex position were assessed. Based on the overall aesthetic appearance, cosmetic results were classified as excellent, good, fair, or poor (Figure 8 and 9). Postoperative day 7 Postoperative day 30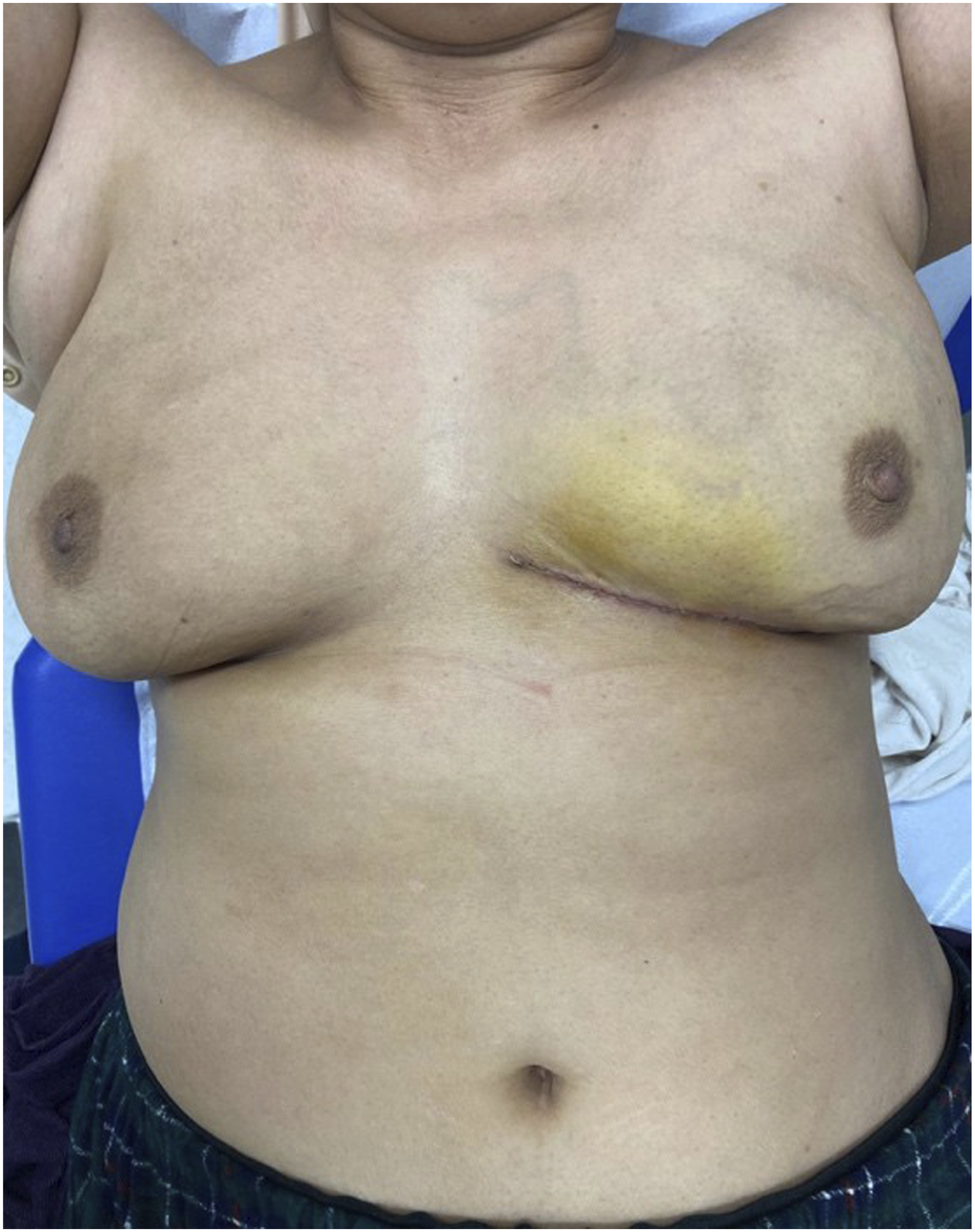

Results
The Dogan Technique was applied to 5 patients with lower inner quadrant breast tumors between January 2025 and March 2026. The planned surgical design was successfully achieved in all cases. Negative surgical margins were obtained in all patients, confirming adequate oncologic resection. No major postoperative complications, including wound dehiscence, infection, or nipple–areola complex ischemia, were observed. Early postoperative evaluation demonstrated satisfactory breast contour and symmetry in all patients (Figure 5, Fig. 6). Cosmetic assessment performed by two independent breast surgeons demonstrated excellent results in 3 patients and good results in two patients. No patient was rated as fair or poor.
Discussion
Variations in breast tissue distribution across different quadrants make it more challenging to achieve both oncologic safety and satisfactory cosmetic outcomes in tumors located in the lower inner quadrant compared to other regions of the breast. Therefore, appropriate selection of the surgical technique is critical. 6 Although several oncoplastic approaches have been described for tumors in the lower quadrants, the Dogan Technique may represent a valuable alternative within the current literature.
In the postoperative period, placement of the incision within the inframammary fold and avoidance of additional breast incisions may contribute to improved cosmetic satisfaction. Satisfactory outcomes have been achieved across all breast sizes. One of the significant challenges of oncoplastic surgery is the risk of ischemia in the nipple–areola complex. When innovative techniques are compared with traditional approaches, they are associated with fewer cutaneous vascular complications and a lower incidence of ischemia. 7
Several volume displacement techniques have been described for lower inner quadrant tumors, including therapeutic mammoplasty, dermoglandular rotation flaps, and glandular advancement procedures. These approaches are effective in restoring breast shape after wide excision; however, many require extensive parenchymal rearrangement, long skin incisions, or repositioning of the nipple–areola complex. Depending on the amount of tissue mobilization and skin resection, changes in nipple position, visible breast scars, and tension-related wound complications may occur.
The Dogan Technique was developed to address selected lower inner quadrant defects while preserving the native position of the nipple–areola complex. Unlike many reduction mammoplasty-based techniques, no centralization or transposition of the nipple–areola complex is required. Preservation of the original nipple position allows maintenance of the natural breast appearance and avoids surgical manipulation of the areolar complex. In addition, the incision is located within the inframammary fold, reducing scar visibility on the breast surface and providing a more concealed postoperative appearance.
Another characteristic of the technique is the use of a superior glandular flap with relatively limited tissue rearrangement. Rather than relying on extensive parenchymal redistribution, the defect is closed using mobilized local glandular tissue planned according to a geometric design. This approach aims to restore breast contour while maintaining symmetry and minimizing distortion of the remaining breast tissue.
The Banana Incision technique, previously described by our group for lower inner quadrant tumors, can be applied to a broad range of breast sizes and similarly utilizes volume displacement principles. 8 However, that technique requires de-epithelialization and recentralization of the nipple–areola complex. In contrast, the Dogan Technique preserves the nipple–areola complex in its original position while maintaining adequate tissue coverage of the resection cavity. Although both techniques are based on established volume displacement principles, the Dogan Technique preserves the nipple–areola complex in its native position and allows scar concealment within the inframammary fold without the need for areolar recentralization.
Nevertheless, this technique should not be regarded as a universal solution for all lower inner quadrant tumors. Adequate residual tissue between the tumor and the inframammary fold is required to allow safe glandular flap mobilization and tension-free closure. For tumors extending to or immediately adjacent to the inframammary fold, other reconstructive approaches may be more appropriate. Therefore, careful patient selection remains one of the key determinants of successful surgical and aesthetic outcomes.
This study has several limitations. First, the small sample size and single-center retrospective design limit the generalizability of the findings. Second, the short follow-up period precludes a comprehensive assessment of long-term oncologic outcomes, cosmetic durability, and patient satisfaction. Third, cosmetic outcomes were assessed by two independent breast surgeons; however, validated objective aesthetic assessment tools and patient-reported outcome measures were not used. Finally, the absence of a comparison group prevents direct evaluation of the advantages and disadvantages of the Dogan Technique relative to established oncoplastic approaches. Therefore, the findings should be considered preliminary and hypothesis-generating. The present study is intended primarily as a technical presentation of the procedure. As clinical experience and patient numbers increase, prospective studies with larger cohorts and longer follow-up will be required to further evaluate the oncologic safety, reproducibility, and aesthetic outcomes of this technique.
Conclusion
The Dogan Technique appears to be a feasible oncoplastic option for selected patients with lower inner quadrant breast tumors, a region associated with significant reconstructive challenges. In this preliminary series, negative surgical margins were achieved without major complications, and early aesthetic outcomes were satisfactory. Preservation of the nipple–areola complex and placement of the incision within the inframammary fold may provide advantages in terms of vascular safety and scar concealment. However, given the small sample size, retrospective design, absence of a comparison group, and limited follow-up period, these findings should be interpreted with caution. Further studies involving larger patient cohorts, longer follow-up periods, and comparative analyses are required to confirm the oncologic safety, reproducibility, and aesthetic outcomes of this technique.
Footnotes
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Research Ethics Committee (approval number: AEŞH-BADEK-2025-447)
Consent to Participate
The requirement for informed consent to participate was waived due to the retrospective nature of the study.
Consent for Publication
The images used in this study do not contain identifiable patient information. All procedures were performed in accordance with institutional guidelines, and no additional consent for publication was required.
Author Contributions
Lütfi Doğan: Conceptualization, study design, and supervision.
Yunus Emre Bölükoğlu: Data collection, investigation, and methodology.
Mehmet Furkan Sağdıç: Data analysis, interpretation, and manuscript drafting.
Mahmut Onur Kültüroğlu: Surgical technique development, critical revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient confidentiality but are available from the corresponding author on reasonable request.