
Abstract
Phase I testing of investigational drugs relies on healthy volunteers as research participants. Many U.S. healthy volunteers enroll repeatedly in clinical trials for the financial compensation. Serial participants are incentivized to ignore restrictions on their participation, and no centralized clinical trial registry prevents dual enrollment. Little is currently known about how healthy volunteers participate in studies over time, hampering the development of policies to protect this group. We detail a methodology developed as part of a longitudinal study to track in real-time healthy volunteers’ Phase I participation. Illustrating these data through three case studies, we document how healthy volunteers use strategies, such as qualifying for studies at more than one clinic and traveling significant distances, to maximize their participation. Our findings suggest that “clinical trial diaries” can generate critical information about serial research participation and point to ethical issues unique to healthy volunteers’ involvement in Phase I clinical trials.
Keywords
Phase I testing of new pharmaceuticals relies primarily on healthy volunteers as research participants. These clinical trials are designed to assess the safety of investigational drugs and help to establish doses for later-phase, efficacy trials. In the U.S. context, most of these clinical trials are conducted at dedicated in-patient clinics owned and operated by contract research organizations, independent research companies, or pharmaceutical companies (Fisher, 2009). Healthy volunteers are recruited through advertising and word-of-mouth, with the promise of stipends in exchange for their participation (Almeida, Azevedo, Nunes, Vaz-da-Silva, & Soares-da-Silva, 2007). Payments range considerably based on the length of the study, but clinics typically compensate volunteers at the rate of US$100 to US$300 per day (Camporesi & McNamee, 2014). For studies that require a 30-day stay in the clinic, participants can earn nearly US$10,000. Healthy volunteers can also receive nominal payments for screening visits (e.g., US$25) or for being an “alternate” (e.g., US$100), which is a term used to describe someone who checks into a clinic for a study in case any of the confirmed participants cannot be enrolled and need to be replaced on the day of dosing (Abadie, 2010).
Motivated by these financial incentives, most healthy volunteers in Phase I clinical trials are serial participants who enroll repeatedly in studies (Fisher, 2014, 2015; Tishler & Bartholomae, 2003). Some healthy volunteers become “professional” research participants, treating Phase I trials as full-time work and travel around the United States to maximize the income they earn (Abadie, 2010). Others are regular participants who use stipends to supplement their household income, some of which is frequently used to purchase expensive consumer goods (Tolich, 2010). Although healthy volunteers are often assumed to be young, White university students, U.S. Phase I trials enroll diverse participants, including what might be considered an overrepresentation of racial and ethnic minorities (Fisher & Kalbaugh, 2011). Men, nonetheless, predominate as healthy volunteers, either because of self-selection or inclusion–exclusion criteria that restrict the types of studies in which women of childbearing potential can enroll (Corrigan, 2002; Fisher & Ronald, 2010; Wood, 2009; Yang et al., 2009).
Typically, Phase I trials require a 30-day washout period before participants can enroll in a new study. There is, however, no single central registry of trial participants, so healthy volunteers can generally avoid restrictions on how often they enroll in studies by participating in multiple clinics (Resnik & Koski, 2011). Although Phase I investigators estimate the rate of serious adverse events to occur in fewer than 1% of healthy volunteers (Hedgecoe, 2014; Kumagai et al., 2006; Sibille, Donazzolo, Lecoz, & Krupka, 2006), dual enrollment in clinical trials can increase participants’ risk of harm as well as raise validity concerns (Kupetsky-Rincon & Kraft, 2012). There are no published data on the extent of dual enrollment in Phase I trials, but 10% of participants in one empirical study admitted to enrolling simultaneously in more than one study (Kass, Myers, Fuchs, Carson, & Flexner, 2007).
The evidence base for why healthy people enroll in Phase I trials is solid, but virtually nothing is known about healthy volunteers’ serial participation in medical research over time. Even if healthy volunteers are financially motivated to enroll in clinical trials, this does not explain how they make decisions about participating in certain studies or specific clinics and over what timeframes. Although some scholars voice concern about healthy volunteers’ subversive behaviors (Abadie, 2010; Dickert, 2013; Dresser, 2013), there is little evidence of the prevalence of rule breaking in Phase I trials (Devine et al., 2013). Similarly, little is known about how various aspects of participation in Phase I studies such as experiencing adverse effects may influence subsequent behaviors related to study participation. Because of a dearth of available data to help policymakers create appropriate policies for the protection of Phase I participants, this group is uniquely vulnerable in clinical research. This article reports on a research tool we developed as part of a larger study to collect such data by tracking in real-time healthy volunteers’ participation in Phase I trials, and it illustrates the kinds of data this tool can provide.
Method
We developed a web-based “clinical trial diary” (CTD) to capture information on every Phase I clinical trial for which healthy volunteers screen while enrolled in the HealthyVOICES Project (N = 180). This longitudinal, mixed-methods study is designed to measure the relationship over time between healthy volunteers’ perceptions of the risks and benefits of Phase I participation and their decision making and behaviors surrounding enrollment in specific clinical trials. The study was designed with two arms—“full participation” and control—to which all participants were randomized after enrollment. The full-participation arm includes completion of CTDs and participation in five semi-structured interviews (at enrollment, at 6 months, 1 year, 2 years, and 3 years) over 3 years. The control arm includes two semi-structured interviews only (at enrollment and 3 years). The purpose of the control group is to evaluate whether the CTDs and additional interviews have an unintended interventional effect on volunteers over the course of the study. Participants in our study were assigned to groups based on their level of experience in clinical studies using a randomization module developed in REDCap (Harris et al., 2009) that allocated 20% of the participants to the control group. Participants receive compensation for participation in interviews at scheduled time points; however, they are not compensated for completing CTDs so as not to encourage enrollment in Phase I trials.
All participants in our study were recruited while enrolled in clinical trials at seven Phase I clinics across the United States. The clinics were selected to represent a sample of for-profit and academic clinics of various sizes, study volumes, and geographic locations, each with a clinical research portfolio dedicated to early-phase pharmaceutical research. We recruited our sample from May to December 2013 in roughly equal portions from the East, Midwest, and West. Although our recruitment strategy was limited to seven clinics, our participant population circulates among a larger number of clinics, enabling us to capture information on nearly all Phase I facilities in the United States and expanding the representativeness of our sample as well as the generalizability of our findings (see case studies below for extent of participant travel to various U.S. clinics).
Participants were enrolled in eight cohorts during 2- to 5-day recruitment visits to each clinic (with a return visit to one clinic), enabling us to stagger data collection into discrete time points for each cohort. In total, we enrolled 180 participants in our study. Table 1 shows the characteristics of our sample, which is representative of U.S. Phase I healthy volunteers more broadly (Fisher & Kalbaugh, 2011). Our sample is predominantly male with more than 60% of participants between the ages of 30 and 49. Few participants (n = 6) are aged between 18 and 21 years, indicating that Phase I healthy volunteers are not predominantly college students (in spite of the fact that six of our seven recruitment clinics were located in cities with one or more large universities). Forty percent of participants are Black, whereas roughly 30% are non-Hispanic Whites and 20% are Hispanic. The level of experience in clinical studies varied across our sample. Roughly 20% were participating in their first clinical trial during enrollment in our study, and almost 30% had participated in 2 to 4 studies, whereas approximately 25% had participated in 5 to 10 studies and another 25% had participated in 11 to 200 studies. At the time of this writing, 14 participants (7.8%) had voluntarily withdrawn, been removed from the study, or lost to follow-up. 1
Characteristics of Healthy Volunteers Sample (N = 180).
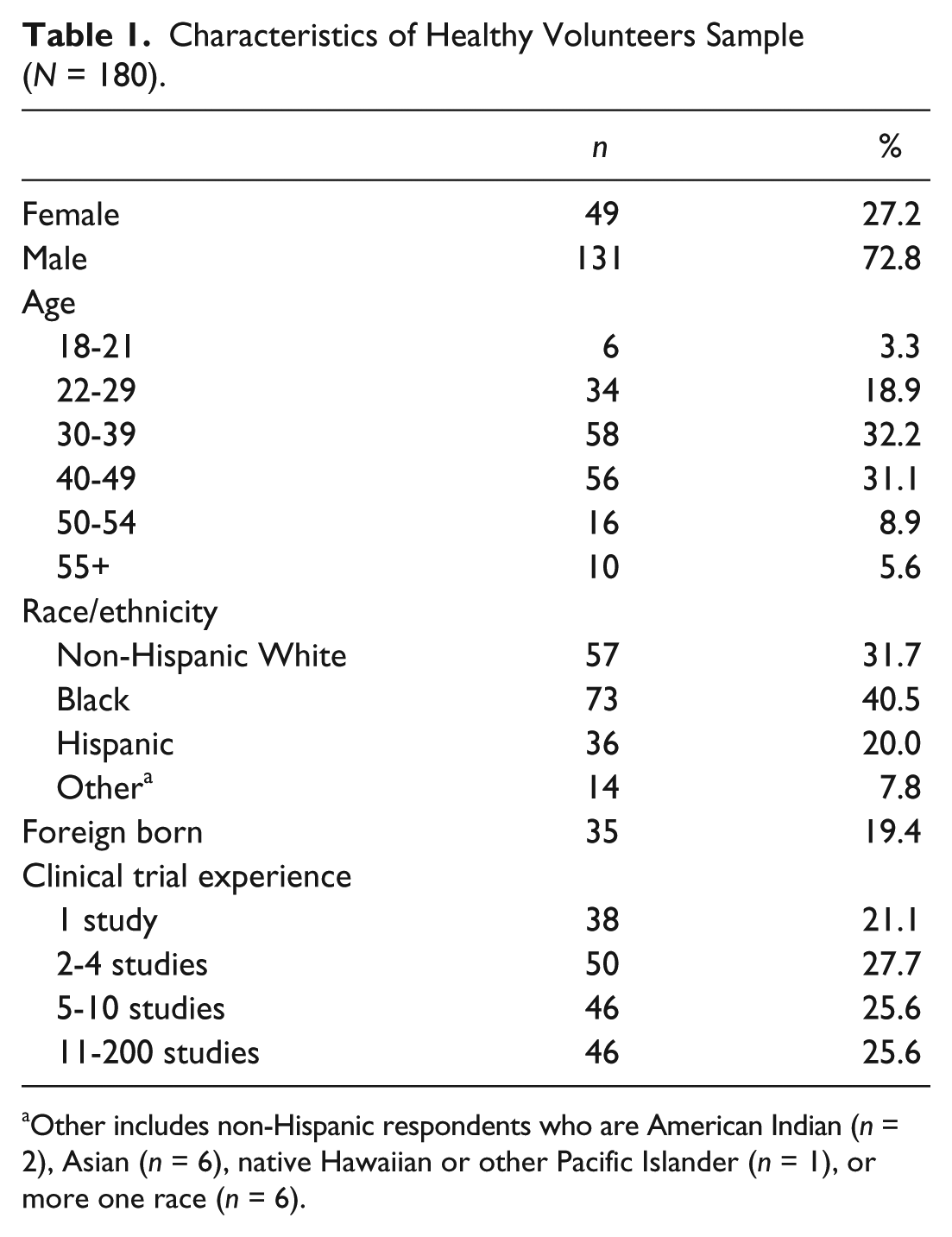
Other includes non-Hispanic respondents who are American Indian (n = 2), Asian (n = 6), native Hawaiian or other Pacific Islander (n = 1), or more one race (n = 6).
Design of CTD System
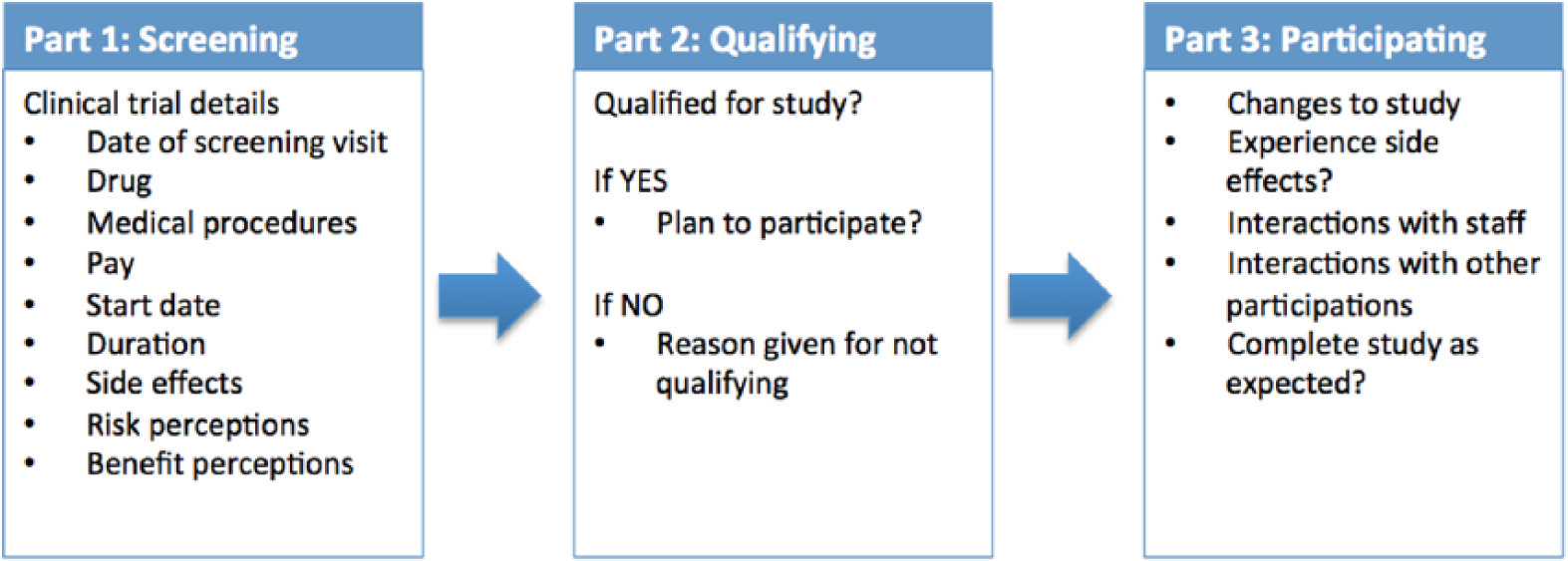
The HealthyVOICES Project is ongoing, but here we focus on the completed design and implementation of the CTD system and report preliminary data from three participants’ CTDs. The CTD is a secure, web-based data collection tool, where participants in the full-participation arm of our study enter information about clinical studies in which they have screened during the 3 years they are participating in our study. The CTD was developed to provide detailed information about the clinical trials they are screening for and participating in. Participants can access the CTD system on a smart phone or computer by logging into a password-protected online “CTD portal” using their email address and birthdate and can create new CTDs whenever they have a new study to report. The CTD itself is a three-part survey designed to mirror participants’ stage in the study participation process: (a) screening, (b) qualifying, and (c) participating (Figure 1). Part 1 collects information from the participants’ screening visit for a new clinical trial. In addition to collecting data about the clinical trials themselves, participants report how they found out about the clinical trial, their motivations to participate, and their perceptions of the likelihood of them participating in the study. Part 2 collects information about whether the participant qualified for the study. This part uses branching logic. If the participants did not qualify, they are asked the reason. If participants qualified, they are asked if they intend to participate in the study. If they do not intend to participate, they are asked why they have declined participation. The CTD is concluded at this stage for participants who did not qualify or decided not to participate in the study at hand. For those participants who report that they qualified and intend to participate, they fill out Part 3 of the CTD. This part allows them to report their experiences in the study in terms of adverse effects and interactions with research staff and other participants, as well as how willing they would be to participate in a similar clinical trial in the future.
Design of clinical trial diary (CTD) system.
The CTD system is designed to automate receipt of Parts 2 and 3 based on information healthy volunteers report in Part 1 and relies on a timeline typical to Phase I clinics. Specifically, if at the end of Part 1, participants respond that they do not yet know whether they qualify, the survey generates an email with a 3-day delay. When participants receive the email, they can click on hyperlinks that will let them start Part 2 if they know whether they have qualified for the study or will trigger a second email to be delivered 1 day later. If participants report in Part 2 that they intend to participate in the study, an email requesting them to complete Part 3 is sent to them 2 days after their last study visit using dates they provided for the clinical trial and the reported study duration. We also included questions that will allow participants to complete all three parts of the CTD if they initiate it after the clinical trial is already completed.
CTD Data Quality and Compliance
Although self-reported data are imperfect, the CTD has a number of mechanisms to ensure that the information captures a full spectrum of outcomes in Phase I trial participation. For example, there are several questions that ask the respondent to confirm that data they entered in previous sections of a CTD are accurate (see online appendix, available at jre.sagepub.com/supplemental). In addition, in Part 3 of the CTD, respondents are asked to confirm that the study they participated in began on the start date they noted in Part 1. If the start date changed, branching logic allows an updated start date to be given. As Phase I clinics often invite more people to participate than dictated by the protocol to ensure full enrollment in studies, qualifying and being selected for a study do not guarantee participation. For example, “alternates” typically check into the clinic for Phase I trials, but they are only used if other participants do not or cannot proceed with the study. To allow for this contingency, Part 3 begins with a question about whether the healthy volunteer participated as planned and completed the study. If they did not complete participation, they are asked for the reason, including the option to report that they were an “alternate” for the study and were not selected to participate. As the CTD system is designed to ascertain various pathways of participation that are sensitive to the dynamics of Phase I studies, CTD data can provide an accurate picture of behaviors related to study enrollment. Study participants are also encouraged to use clinical trial informed consent documents when completing their CTDs to provide more accurate and complete information about those studies. Scheduled interviews at specified time points in our 3-year study provide another opportunity to verify the accuracy of CTD data.
As part of compliance efforts, project staff follow up with participants via email and phone to ensure that completion of CTDs matches the actual screening and enrollment behaviors of participants in our study. To accommodate participants with limited Internet access, we developed a pared-down version of the CTD (the “CTD Lite”) that staff complete with participants over the phone. As of this writing, we have collected a total of 625 CTDs, which have been completed by 92% (n = 134) of participants enrolled in the full-participation arm of the study (n = 146). Although participants in the full-participation arm of the study are required to complete a CTD every time they screen for studies, continued enrollment in Phase I studies is not a requirement of our study.
The structure of the CTD data allows us to compute various metrics that help us understand patterns of participation for healthy volunteers. Because participants list the clinic name for each clinical trial, we can use these data to calculate distances between clinics and from their home address each time participants screen for studies. This allows us to systematically track geographical patterns of participation for healthy volunteers in our study to provide a clearer picture of the ways in which travel may inform these behaviors. Similarly, although compliance with washout periods represents a concern for those who conduct clinical studies with healthy volunteers, little is known about the degree to which this behavior exists. Dates of participation in studies allow us to compute estimated compliance with the washout period for participants in our study. Over time, CTD data will allow us to assess trends in participation among healthy volunteers in our study and the ways in which their experiences in studies inform their future behaviors.
Ethical Considerations
Our study was reviewed and approved by the Biomedical Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill. The identities of the participants in our study are confidential. Although we enrolled healthy volunteers while they were participating in a clinical trial, we do not share with the Phase I clinics any information about who enrolled in our study or the information they provide in interviews or CTDs. In addition, we hold confidential any information about participants’ dual enrollment in clinical trials or their failure to observe washout periods between studies. This level of confidentiality is important for participants to trust us with information about their trial participation. Because Phase I studies provide intensive monitoring of healthy volunteers’ health and wellness, we do not believe that preserving participants’ confidentiality endangers them.
Results
To illustrate the capabilities of our tool for reporting Phase I participation, we provide examples of the kinds of data that can be collected with the CTD system. Using a case study approach, we focus on CTD data over a 6-month period for three participants who were enrolled in the same cohort of our study in 2013. We selected these participants because they had a higher than average rate of screening for new clinical trials in a 6-month period and can illustrate more Phase I activity in a short span of time. Pseudonyms are used to protect the confidentiality of our participants, and we label the clinics they visited using the letters A to H instead of their proper names. When enrolled in our study, all three were participating in a drug interaction study at a clinic in the Midwest noted as “Baseline” at Clinic A in Figure 2. This study lasted 10 days and nights and paid US$2,500. As is typical of Phase I trials, this study had a washout period of 30 days during which time participants were prohibited from enrolling in new clinical studies. The trajectories of each of these three participants after departing from this shared study provide a glimpse into how healthy volunteers participate serially in clinical trials.
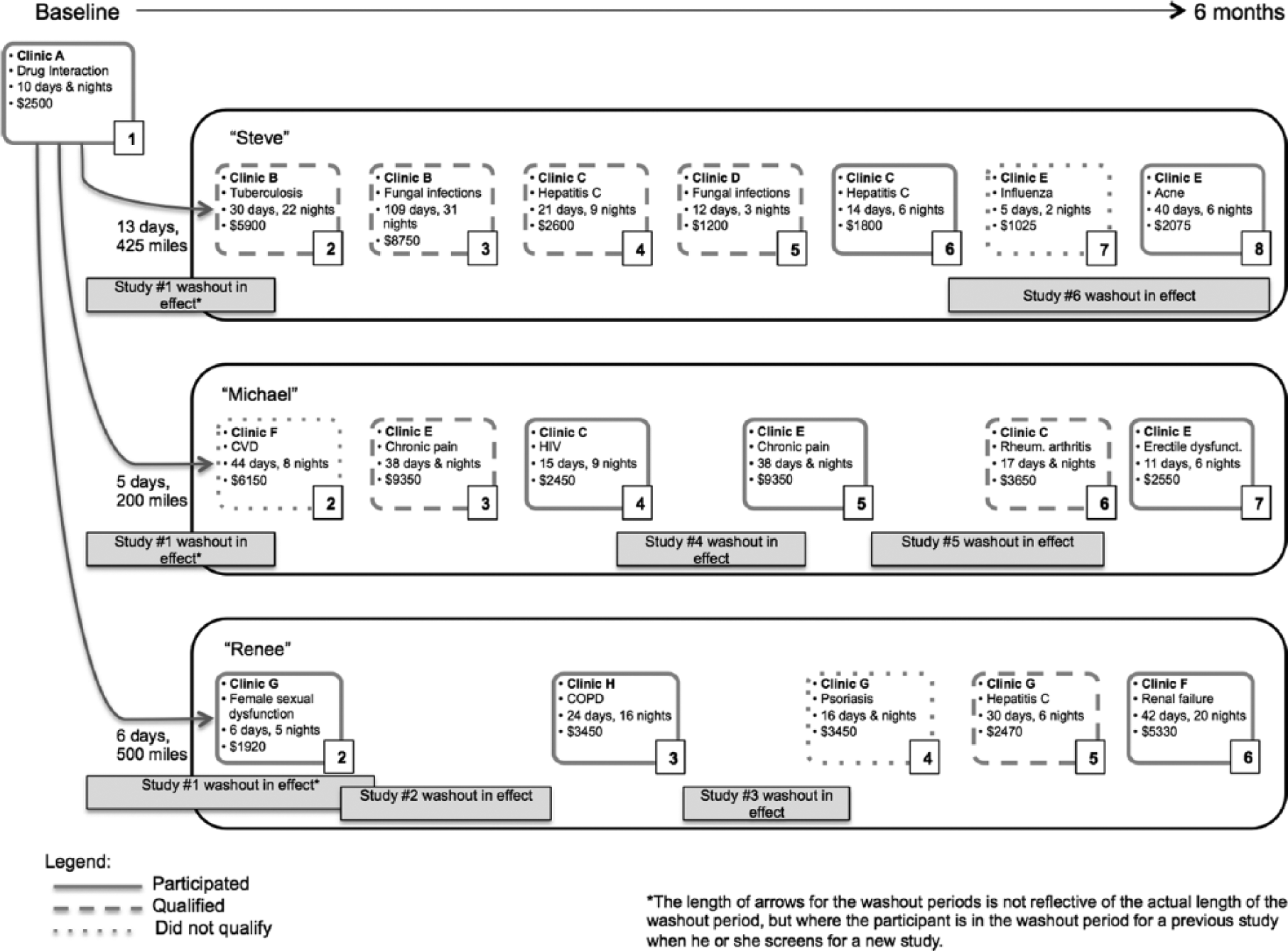
Clinical trial participation trajectories.
Participant 1
“Steve” is a single White male is his late 40s who estimated that he had participated in 70 clinical trials since he started participating in studies in the early 1990s. He has traveled extensively to participate in Phase I trials in the United States and even participated in one overseas. During his baseline interview, he also revealed that he had moved to a new area in the Midwest primarily because he liked a particular Phase I clinic there and thought the location would be convenient to other clinics in nearby states. Although he works as a handyman on occasion, income from Phase I studies represents his primary source of income.
In the first 6 months of his participation in our study, Steve completed seven CTDs for new studies, providing information on where he screened, for what types of Phase I trials, the outcome of his screening visits, and whether he participated in those studies for which he qualified (Figure 2). These CTDs reveal his movements through the Midwest in pursuit of clinical trials as well as offer insights into his decision-making process.
Thirteen days after finishing his baseline study (noted as “Study 1” in Figure 2), Steve screened for a study at a Clinic B located 425 miles from Clinic A. This Phase I study involved an investigational drug for tuberculosis (Study 2). It paid US$5,900 and required 22 overnight stays over a period of 30 days. Steve qualified for this study and proceeded to the clinic to check in on the scheduled start date. At check-in, however, he was informed that he was an alternate, and he was dismissed from the study the following day after the required number of participants was dosed with the study drug. Six days later, Steve screened at the same clinic for Study 3, a Phase I trial of a drug for fungal infections. This study paid almost US$9,000 but was much longer than the other, spanning 109 days with 31 overnight stays. After screening for the study, Steve wrote in his CTD, It’s a lot longer and drawn out than I’d prefer, with 3 outpatient visits over 3 months after checkout. But since I didn’t get used for the $5,900 [study] I checked into a week ago, I need to grab this one. All my other options are too small.
Steve qualified for this study and checked in to the clinic to participate. He was again discharged from the study the day after check-in, this time because his labs were out of range and the clinic opted to use an alternate instead.
The next day, Steve traveled 150 miles to Clinic C to screen for the Hepatitis C Phase I trial, a 21-day study involving 9 overnight stays and paying US$2,600. Steve qualified for this study, but he noted in his CTD that he might be an alternate, so 2 days before it was to begin, he screened for a different study 375 miles away at Clinic D. Study 5—a different fungal infection study—paid US$1,200 and was relatively short, lasting only 12 days with 3 overnight stays. Steve also qualified for this study and explained in his CTD, “This is my back-up plan in case I’m an alternate and not used at the [Clinic C] trial that I’m scheduled to check in to 2 days earlier.” Returning to Clinic C for Study 4, Steve checked in, and he was again an alternate and was discharged from the study. Clinic C offered Steve a study spot in a later cohort of the same study scheduled to begin 10 days later. In the meantime, Steve returned to Clinic D for Study 5, but he was again an alternate and was discharged from the study. He indicated in his CTD that he was “frustrated, upset, stressed, and disappointed” with the outcome.
Returning to Clinic C for the second Hepatitis C study, Steve checked in and completed Study 6, a 14-day study with 6 overnight stays and a washout period of 45 days. He received US$1,800 in compensation. Twelve days after that study ended, Steve traveled 100 miles to screen for Study 7 at Clinic E. He was told that his electrocardiogram (ECG) was out of range and did not qualify. Returning to the same clinic 5 days later, he screened for Study 8. He qualified for and participated in that 40-day acne study with 6 overnight stays and was paid US$2,075. In the final part of his CTD, he reflected, “It was a very short study with 3 different 2-night stays. Not my preferred type. But if I still can’t find longer, higher paying studies, I may have to do one like this again.”
Over this 6-month window and including the baseline study, Steve screened for eight new Phase I trials, but participated in only three of those studies. Although he qualified for four additional studies, he was an alternate without the clinic needing him on three, and he failed to pass all the laboratory tests at check-in for the fourth. He earned more than US$6,000 by participating in clinical studies and traveled more than 1,400 miles to screen for studies. He used specific strategies, such as qualifying for more than one study at a time and traveling within a wide swath of the Midwest, to maximize his chances of participating in studies and earning the compensation that comes with participation. For the most part, his screening behavior was not in compliance with the specified 30- or 45-day washout periods for studies because he sought new studies at a different clinic shortly after completing participation in each study.
Participant 2
“Michael” is a single Black male in his late 30s who had participated in 22 studies when he enrolled in our study. Michael enrolled in his first Phase I trial in 2008 and, like Steve, currently participates in studies full-time. Michael sees himself as an entrepreneur, and he uses his income from clinical trials not only to pay his household expenses but also to buy and renovate houses as investment properties.
In the first 6 months in our study, Michael completed CTDs for six new Phase I studies. He was enrolled in the same drug interaction study as Steve at Clinic A, which was located 350 miles from his home address. During that study, he was already lining up new screening visits by calling other clinics and making plans to carpool to those appointments with a few other participants in the study. Five days after completing Study 1, Michael traveled 200 miles to screen for a cardiovascular disease (CVD) study at Clinic F (Study 2). He did not qualify for this study because his blood pressure was too high, and ECG results were out of range for the inclusion criteria of the study. In his CTD, Michael reflected on his test results, “I hadn’t gotten a lot of sleep the night before, and I know one of the things that can affect your blood pressure is not getting enough rest. I know I’m healthy.” His next screening visit was 13 days later at Clinic E, a clinic 425 miles from Clinic F. Study 3 involved an investigational drug for chronic pain, lasted 38 days and nights, and paid US$9,350. Michael qualified for this study, but the clinic had more qualified healthy volunteers than it needed and he was not selected to participate. Having already lined up for another screening visit, Michael screened for his next study 1 week after his prior screening (and 1 day after Study 3 would have begun). For this study, he traveled 100 miles to Clinic C for a 15-day HIV study with 9 overnight stays and paying US$2,450. He qualified for this study and participated.
Two days after Study 4 ended, he returned to Clinic E for Study 5 because the clinic had invited him to participate in a new cohort of the chronic pain drug study. He had to re-screen, but he qualified for and participated in it. When asked in his CTD for this study whether he would participate in an identical study in the future, he indicated that he was unsure and offered the following observations: There were quite a few AE’s (Adverse Events) in this particular study depending on if you got the drug or not that I witness[ed]. I personally myself don’t think I got the drug [and got the placebo instead,] but just seeing some of the people going through it, their reaction and how our meals were I’m not sure if I would or not [participate in an identical study].
Two days after Study 5 ended, Michael screened and qualified for a 17-day rheumatoid arthritis study that paid US$3,650 at Clinic C where his washout period from Study 4 was now over. He checked in to participate for this study, but he was not selected to dose and was discharged on the third day when the clinic knew they would not need him. About not being selected, Michael wrote in his CTD,
Study was full, I was told all my labs and everything was fine just wasn’t enough room in study . . . I would of [sic] liked to attend the study especially when you fill [sic] like you know the staff and they know you as a good participant. But sometimes this happens with [a] study and [it’s] just the business we deal with.
Two weeks later, Michael returned once again to Clinic E and screened for Study 7. By this point, his washout period for Study 5 had expired by 2 days, so he was eligible to participate in a new study there. He qualified and participated in this 11-day study for an erectile dysfunction drug that paid US$2,550.
Over 6 months and including the baseline study, Michael screened for seven studies, out of which he qualified for six, participated in four, and earned almost US$17,000. To screen for and participate in these clinical trials, Michael rotated between four clinics and traveled at least 1,100 miles. By using this strategy, he was able to avoid complying with the required washout period between studies during this 6-month time frame.
Participant 3
When “Renee” enrolled in our study, she had participated in nine studies in 2 years. Renee is a divorced biracial female in her late 30s who is the primary caretaker for her two children. To participate in the drug interaction study at Clinic A, she had traveled 500 miles from home. During her baseline interview, she revealed that she had recently quit her full-time job to participate in Phase I clinical trials. She also expressed some reticence about enrolling in studies with longer term confinement periods because she worries about being away from home for too long. At the same time, however, she has traveled extensively throughout the East Coast and Midwest to screen for studies.
Renee completed five CTDs for clinical trials for which she screened during the first 6 months of her involvement in our study. Six days after Study 1 ended, she screened for a female sexual dysfunction study at Clinic G located 525 miles from Clinic A and 300 miles from her home (Study 2). This 6-day study paid US$1,920 and required five overnight stays. She qualified for this study, and 5 days after screening, she checked into the clinic and participated in the study. Twenty-three days after Study 2 ended, Renee screened for Study 3 at Clinic H located approximately 70 miles from her home. This 24-day study with a 16-night consecutive stay focused on chronic obstructive pulmonary disease (COPD) and paid US$3,450. After qualifying, Renee participated in this study and noted in her CTD that she experienced side effects that included “elevated heart rate, night sweats, muscle twitching in legs, pins and needle pricks, and increased blood pressure.” She rated the severity of side effects as “severe,” or a 3 on a 4-point scale (i.e., mild, moderate, severe, or extreme) and used the comment box below the question to write, “Extremely unusual for me. I never had symptoms like this with any other study I’ve done.” As a result of these side effects, she noted that she considered dropping out of the study, but she continued to participate because the onset of these symptoms was close to the end of the study, and the clinic staff assured her she was not in danger. In a final comment box at the end of the CTD, she wrote, “I will be much more cautious about any studies I decide to participate in.”
In spite of her negative experience in Study 3, Renee returned to Clinic G 11 days later and screened for Study 4, a 16-day psoriasis study. She did not qualify for this study because the study sponsor wanted her to provide “ultrasound proof of a tubal ligation.” Although she had undergone a tubal ligation a few years prior, the sponsor would not accept her medical records and requested that she undergo an ultrasound at her own expense. When she opted not to do this, she was disqualified from the study. Thirty-four days after screening for Study 4, Renee again returned to Clinic G to screen for a Hepatitis C study that paid US$2,470 and required six overnight stays over a 30-day period. She qualified for this study that was scheduled to begin 3 weeks after her screening visit. Before Study 5 began, however, Renee screened for Study 6 at Clinic F located 725 miles from Clinic G. Study 6 was for diabetes renal failure and paid more than US$5,000 and required 20 overnight stays over a 42-day period. After qualifying for Study 6, she decided to participate in this study instead of Study 5 because the study dates overlapped, and Study 6 paid better. She reported that her chosen study was relatively easy and one that she would participate in again as she experienced no problems or side effects. She further commented in her CTD that this clinic was the best facility she had ever been to as a healthy volunteer.
Including her baseline study at enrollment in our study, Renee screened for six clinical trials, qualified for five, and participated in four during her initial 6 months of participation in our study. She earned approximately US$13,000 by participating in clinical studies and traveled at least 1,950 miles to screen for studies during that period. Based on her CTDs, Renee did not observe the washout period between Study 1 and 2, but she completed washout periods—whether intended or not—between the other studies during the remaining time in the 6-month period reported here.
Discussion
The three cases we present here illustrate how a CTD—the tool we created as part of the HealthyVOICES Project—can generate a multidimensional representation of healthy volunteer participation in Phase I clinical trials. As these cases demonstrate, participation in clinical trials is a way of life for these healthy volunteers and can require extensive travel and coordination, but the compensation can make this lifestyle possible. Although the data we present provide a 6-month window into the participation of a small subset of healthy volunteers in our study, they convey how patterns of behavior can emerge in a relatively brief period of time.
An important finding illustrated by these three cases is the extent to which healthy volunteers ignore washout periods between studies. All three participants screened for new studies at different clinics less than 2 weeks after finishing Study 1. Indeed, this was fairly typical for them throughout the 6-month time period reported here. Completing participation in a study at one clinic was often followed by screening for a new study at a separate clinic, demonstrating the degree to which participants intended to disregard the required 30- or 45-day washout periods for studies. Indeed, we found that sometimes washout periods were observed simply because participants were prevented from enrolling in a new study as quickly as they would have liked. Steve adhered to the washout period for the baseline clinical trial only because he was not selected to participate in the four studies for which he screened immediately following that study. Renee and Michael also ended up observing washout periods for previous studies because they failed to qualify for new studies. In this way, observing the washout period is merely an artifact of not successfully gaining quick access to a new study, rather than a conscious adherence to the requirements of a prior study.
Our findings also indicate that healthy volunteers use the strategy of rotating between select clinics. Qualifying for a study at one clinic would provoke another screening at a different clinic in Steve’s case. For Michael, five of the six studies he screened for were at two clinics that were located approximately 100 miles from one another. His washout periods between studies at these two clinics structured his screening behaviors. Specifically, participating in a study at Clinic C during the washout period for a study at Clinic E provided an opportunity to earn income while being temporarily barred from screening at Clinic E. When the washout period for Clinic E expired, Michael returned to that clinic to screen for a study. Rotating between just these two clinics helped Michael maximize his participation in new Phase I trials.
Our data suggest that healthy volunteers create their own system of clinical trial “alternates” or backups to maximize their successful enrollment in Phase I studies. Just like Phase I clinics engage in various practices such as qualifying more participants than needed to meet their study goals, healthy volunteers use specific strategies to meet their primary goal of maximizing their earning potential through participation in Phase I studies. Our results show that healthy volunteers screen for multiple studies at a time to increase their chances of participation, knowing that they might not qualify for one or that they are only an alternate and not guaranteed participation in another. On one hand, Steve’s history of being an alternate in studies for which he qualified catalyzed him to create his own system of clinical trial alternates. The time between finding out about qualifying for a study and the study start date served as an opportunity to develop a “back-up plan” aimed at improving his odds of participation in any study. Renee, on the other hand, qualified for a study scheduled to start 3 weeks later, but decided to screen in the interim for another study that paid better and—because the study dates overlapped—chose to participate in the higher paying one.
Another important finding from these three cases is that experiences in past studies can influence how healthy volunteers perceive the risks of studies and shape future decisions regarding participation in Phase I trials. Renee experienced severe side effects that included night sweats, muscle twitching, and the sensation of pins and needles or paresthesia in a COPD study. She considered dropping out of that study due to the severity of these side effects and noted that she would be more careful when making decisions about future studies. Michael had a similar experience while participating in a chronic pain study. His observation of other participants experiencing adverse effects led him to believe that he was dosed with the placebo instead of the study drug and made him question whether he would participate in a similar study in the future. Further data, collected over the course of the HealthyVOICES Project, will be able to document whether and how these concerns affect their decisions about future study participation.
The 6-month participation trajectories of all three healthy volunteers demonstrate active patterns of screening for clinical trials at Phase I clinics. However, the amount of effort it took to enroll successfully in studies and earn compensation varied across our participants. After his baseline study, Steve qualified for four studies before finally participating in one; indeed, he participated in only two of the seven studies for which he screened. He traveled at least 1,200 miles before finally being enrolled in a second study, demonstrating the amount of effort the pursuit of studies can take. Steve noted that the study he finally participated in was not his preferred type given its short duration and relatively low pay, but felt like he had no other options. He earned about US$6,000 from his study participation during this 6-month period. Michael, by contrast, earned almost US$17,000 for participating in four studies and mostly traveled between two clinics located just 100 miles apart. The longer confinement study for the chronic pain drug paid more than US$9,000 and comprised the majority of the income he earned during this time. Renee earned approximately US$13,000 during this time period, but traveled at least 2,500 miles in her pursuit of studies during this time. The lengths to which healthy volunteers go to participate in Phase I trials varied as did the rewards for these efforts.
The case studies represent in-depth examinations of individual patterns of behavior over a 6-month period for three healthy volunteers who were enrolled in the same cohort of our study. The three volunteers we selected had extensive experience in clinical studies and had been participating in studies for a number of years when they enrolled in our study. Their experiences provide a snapshot of possible participation trajectories, but are not meant to be generalizable given the case study approach. Instead, by selecting participants who frequently screen for and participate in studies, we aimed to demonstrate the value of the CTD as a tool that can uncover healthy volunteers’ patterns of participation in Phase I clinical trials. Future analyses of the CTD data can examine not only how individuals’ behaviors might change over time but also how subgroups of participants in our study differ based on their socio-demographic characteristics or their level of clinical trial experience.
Research Agenda
The preliminary findings from these case studies of serial participants in clinical studies suggest that the financial incentives associated with Phase I participation outweigh healthy volunteers’ adherence to restrictions designed to protect their health. What repeated failure to observe washout periods could mean for the well-being of healthy volunteers over time is an open question. This highlights the need for further research on the long-term health consequences of serial participation in clinical trials. A study like ours can provide data on what clinical trials healthy volunteers screen for and enroll in, but as a social science project, we are not monitoring the health outcomes of our participants. A comparative study of healthy volunteers and non-trial participants as “matched controls,” for example, would generate important information about the long-term effects of repeated exposure to investigational drugs. This type of research would also provide critical information to healthy volunteers about the longer term risks of Phase I serial participation.
In addition, repeated failure to observe washout periods has implications for the integrity of clinical trial data and represents a concern for the pharmaceutical companies sponsoring these studies. Some clinics have begun using proprietary participant tracking tools, such as Verified Clinical Trials and clinicalRSVP, to prevent participants from simultaneously enrolling in multiple studies or being noncompliant with washout periods. These databases can provide useful information for research clinics to prevent such occurrences. However, these systems have not been widely adopted, so participating clinics only know about healthy volunteers’ participation in studies at the clinics that have subscribed to each system. In our ongoing study, we are finding that healthy volunteers are aware of which clinics use these systems and factor that information into their participation strategies. Future research, more broadly, should examine the ways in which clinic characteristics and industry changes structure participation for healthy volunteers over time and how to best ensure the validity of clinical trial data.
Educational Implications
Currently, medical researchers and IRBs are trained to evaluate clinical trials as discrete protocols that present specific risks and benefits to research participants. A study like ours suggests that Phase I healthy volunteers create unique challenges for human subject protections because of their serial participation. By acknowledging the broader risks generated by healthy volunteers’ screening and enrollment behaviors, researchers and IRBs should reimagine how risk information is provided to healthy volunteers. Rather than simply stating inclusion criteria that would exclude participants who have recently completed a Phase I trial, there is a need for greater attention to educating participants to the risks of serial participation. Specifically, providing more detailed information about the potential health consequences of ignoring washout periods or other restrictions on their study participation could encourage healthy volunteers to exercise greater caution and provide more honest information during the screening process.
Footnotes
Authors’ Note
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the National Institute of General Medical Sciences (NIGMS) or the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Grant Number R01GM099952 from the National Institute of General Medical Sciences (NIGMS). In addition, the use of REDCap was supported by the University of North Carolina at Chapel Hill through Grant Number 1UL1TR001111 from the Clinical and Translational Science Award program of the Division of Research Resources, National Institutes of Health. General support was also provided by the Carolina Population Center (R24 HD050924).
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.