
Abstract
The objectives of this study were to evaluate the impact of educational interventions during prenatal care on public trust for newborn screening and consent preferences for the retention and use of leftover newborn screening dried blood spots. Women who were 30 to 36 weeks pregnant were recruited, and outcomes were measured by telephone survey 2 to 4 weeks postpartum (n = 901). Approximately 40% of the sample chose the opt-out approach but those who watched educational interventions delivered during prenatal care were significantly associated with higher levels of trust and support for an opt-out consent approach. Providing education during prenatal care about newborn screening and the storage and use of leftover dried blood spots along with brochure-based education provided in the hospital when the baby is born is associated with improved trust for the program and support for research with the leftover blood spots.
Keywords
Introduction
Newborn screening (NBS) is one of the most successful public health programs in the United States in the past 50 years (Centers for Disease Control and Prevention [CDC], 2011). The program has improved the lives of thousands of infants and their families through early treatment and medical management of infants who have been identified with a variety of serious genetic, congenital, infectious, and endocrine conditions. For the most part, NBS is a mandatory program and only parents who have philosophical or religious objections can opt-out of NBS. The mandatory nature of NBS is based on parens patriae doctrine and dependent on public trust that the programs will be conducted in an effective and ethical manner.
When NBS is conducted after the birth of the child, enough blood is collected in case re-analysis needs to be conducted. The leftover dried blood spots (DBS) are then stored by state health departments for various lengths of time for almost all infants born in the United States. The leftover DBS are important for quality assurance of NBS tests and for biomedical research. For the most part, this research has been conducted with de-identified DBS and without parental consent under past federal human subjects regulations (45CFR46.102(f)). However, criticisms have increased because of the retention and use of leftover DBS for research outside of NBS. Three lawsuits by parents over the lack of adequate information and parental permission of this practice have occurred (Lewis, 2015). More importantly these lawsuits have raised concerns about the loss of the public’s trust for NBS programs.
Recent changes to the laws by the Newborn Screening Saves Lives Reauthorization Act (2015) now require parental consent for the storage and use of leftover DBS. In addition, the Notice of Proposed Rulemaking is proposing similar changes to the Common Rule. Both require or recommend broad consent for future, unlimited research of biospecimens whether or not they are de-identified. These changes reflect the growing importance of communicating with the public about research practices that extend beyond NBS and other clinical settings that collect biospecimens.
The use of informed consent for the retention and use of leftover DBS has raised concern among some NBS stakeholders. One concern in particular is the lack of available samples for the development of new screening tests. California state NBS program implemented a pilot supplemental screening program to evaluate the effectiveness of using tandem mass spectrometry (MS/MS; Feutchbaum, Cunningham, & Sciortino, 2007). This was considered pilot research by the California legislation and, as such, parental consent was required. Participation by hospitals throughout the state of California varied. Some hospitals refused to participate (20%, n = 63), and only 23% of hospitals offered the supplemental screening to greater than 75% of newborns. This resulted in only 52% of the babies born were invited to participate, and only 47% agreed to participate (CDC, 2012).
Furthermore, if hospitals do offer consent, it is not guaranteed that the information presented during the consent process is given in a meaningful manner that promotes an informed decision. The literature provides substantial evidence that the current process to informed consent process is seriously flawed (Falagas, Korbila, Giannopoulou, Kondilis, & Peeppas, 2009). This means that many individuals sign a consent form without an adequate understanding of the study purpose, procedures, risks, and benefits. Within the context of NBS, these challenges to comprehension are magnified because of the timing of NBS from the demands of labor and needs of a newborn. If an informed consent process is implemented within hospitals, but the process does not promote meaningful opportunities for comprehension then that in itself may actually cause a decline in public support (O’Neill, 2004).
Besides the logistics of offering consent in the hospital, there are other factors that influence participation such as trust (Eyal, 2014; Gikonyo, Bejon, Marsh, & Molyneux, 2008). The literature has demonstrated that distrust among subpopulations have resulted in lack of participation in research (Braunstein, Sherber, Schulman, Ding, & Powe, 2008; Kennedy, Mathis, & Woods, 2007). With the recent lawsuits by parents, maintaining public trust with NBS programs is paramount. Thus, it is equally important to identify effective education efforts for parents about the retention and research use of leftover DBS that promote adequate understanding to make a choice about consent with these important public health programs.
This study assessed whether improved education during prenatal care about NBS and leftover DBS (as opposed to only hospital education around the birth of the child through brochures) influenced perceptions of trust and consent preferences (opt-in/opt-out) for the storage and use of leftover DBS. This study was part of larger study that conducted a randomized controlled trial of prenatal NBS education interventions in obstetric clinics (n = 901) (1R01HG006266-02).
Method
The larger study was designed to assess prenatal education about NBS and DBS retention by state health departments following NBS. Institutional review board approval was obtained prior to any research activity. In the parent study, participating women in Utah, New York, and California who were 32 to 38 weeks pregnant were randomly assigned to one of three study groups with each group receiving different education materials. There were three groups and of them all received the usual care that included information about NBS and the storage and use of leftover DBS provided by their prenatal care providers and from the hospital after birth. The two intervention groups additionally viewed educational videos and were given a companion brochure. The NBS group watched one video intervention that was approximately 5 min in length about NBS. The other intervention group watched the video about NBS and an additional video about the storage and use of leftover DBS that was approximately 7 min in length. The video education tools were developed by the Genetic Science Learning Center (GSLC) at the University of Utah.
A total of 901 participants were randomized to the three groups. The participants were surveyed over the telephone 2 to 4 weeks after the due date of their babies about their knowledge and attitudes about NBS and blood spot retention (approximately 7 weeks after the intervention). Both the videos and the surveys were pilot tested with a separate group of respondents for validity and reliability prior to implementation in this randomized controlled trial. For this study, there was an overall follow-up rate of 70% (n = 633) (Botkin, et al., 2016).
Measures
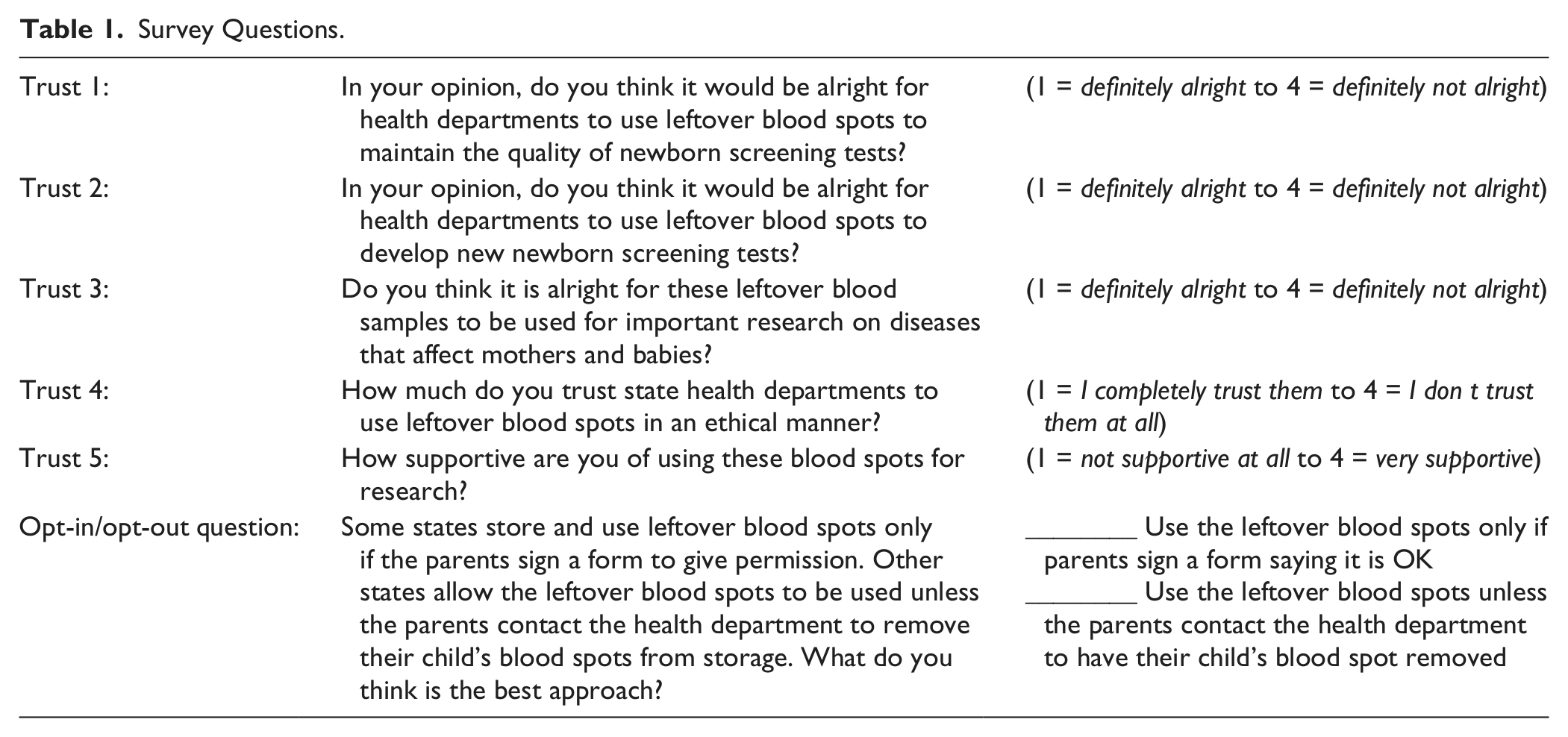
Trust was assessed with a five-question survey. Participants were asked about their level of support and trust for the retention and use of leftover DBS for research purposes (Table 1). Questions were scored and summed to create a measure of trust ranging from five to 20 with higher scores indicating more trust. Reliability of the trust survey was good with a Cronbach’s alpha = .83 for the sample. Opt in/opt out was assessed with a single item. Participants choose between (a) “Use the leftover blood spots only if parents sign a form saying it is OK” and (b) “Use the leftover blood spots unless the parents contact the health department to have their child’s blood spot removed.”
Survey Questions.
Analysis
General linear mixed modeling was conducted with SPSS 22 (SPSS, 2006) to assess the relationship of the outcome measure of trust with race, education, and intervention. Race and education were included due to previous research (Boulware, Cooper, Ratner, LaVeist, & Powe, 2003; Richardson, Allen, Xiao, & Vallone, 2012). Logistic regression was used to analyze the relationship of the dichotomized outcome variable of opt in/out with race, education, and educational intervention. Statistical significance was set with an alpha = .05, no corrections for multiple comparisons were made.
Results
Results from mixed modeling indicated the fixed effects of Intervention (F = 19.68, p < .001), Race (F = 11.01, p < .001), and Education (F = 4.60, p < .001) were significantly associated with trust (Table 2). Within Intervention, results show that the NBS and leftover dried blood spot video group was significantly higher in trust than both the NBS group only (p < .001), and the Control group (p < .001) indicating that those who received the most education (NBS and DBS) reported higher trust scores (means and standard errors are reported in Table 2).
Mixed Model, and Logistic Regression Results.
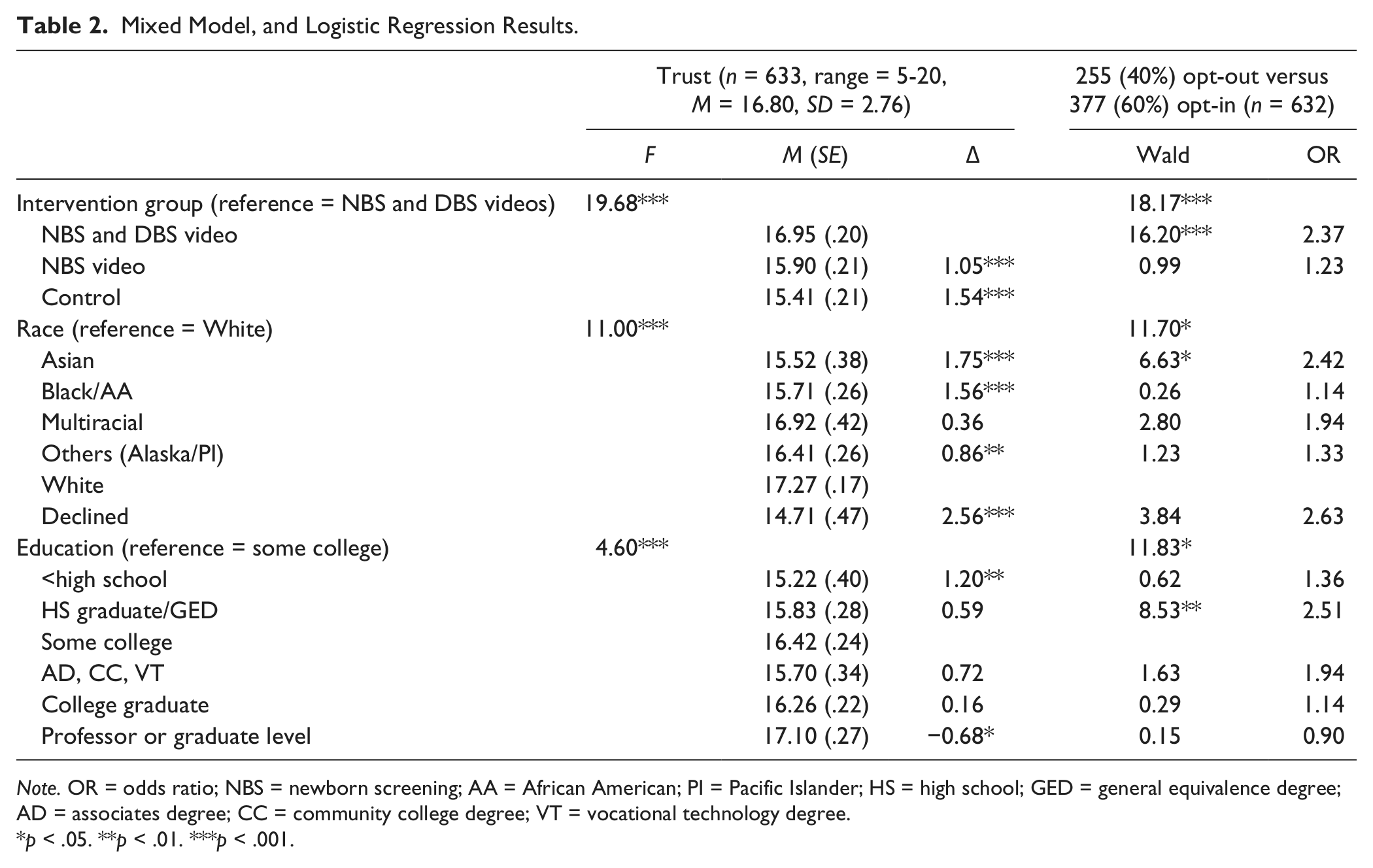
Note. OR = odds ratio; NBS = newborn screening; AA = African American; PI = Pacific Islander; HS = high school; GED = general equivalence degree; AD = associates degree; CC = community college degree; VT = vocational technology degree.
p < .05. **p < .01. ***p < .001.
Analysis of estimated marginal means (post hoc) indicates that within race: Whites reported the highest trust scored compared with Blacks, Asians, Others, and those who declined to answer their race (all p < .01). Within Education, post hoc analyses show that participants with high self-reported educational levels had significantly higher levels of trust; some college education was significantly higher in trust than participant’s with less than high school education (p = .009), while participant’s with professional or graduate-level education had higher levels of trust when compared with the some college education participants (p = .041).
Opt In/Out
Overall our sample indicated that 40% (n = 255) choose the opt-out approach whereas 60% (n = 377) choose the opt-in approach. Results from logistic regression showed that the Video Intervention (Wald = 18.17, p < .001), Race (Wald = 11.70, p = .039), and Education (Wald = 11.83, p = .037) were significantly associated with the opt-out choice (Table 2). Participants who watched both the NBS and DBS video were more than 2 times more likely to choose opt-out versus the Control group (odds ratio [OR] = 2.367, p < .001). Participants viewing only the NBS video were not statistically different from the Control group (OR = 1.232, p = .321). Within Race, Asians were significantly more likely to choose opt-out versus Whites (OR = 2.42, p = .010). Within Education, those with “high school or GED level of education” were more likely to endorse opt-out versus participant’s with “some college education” (OR = 2.51, p = .009).
Discussion
The results of this study indicate that the video educational inventions delivered in this study about NBS and leftover DBS were associated with significantly higher levels of trust and support for an opt-out consent approach for the storage and use of leftover DBS. These results are consistent with the primary outcomes of the main study (Botkin et al., 2016) in that improved education efforts (education about NBS and leftover DBS during the third trimester of pregnancy along with brochure-based education in the hospital during the birth of the child) are significantly associated with higher levels of knowledge, and support for NBS and the storage and use of leftover DBS for biomedical research.
Interestingly, participants who received both NBS and leftover DBS video education interventions reported significantly higher support for NBS itself, and for the retention and use leftover DBS in research than those who just received NBS video education only. This is an interesting finding in that more education about NBS along with education about what happens with the leftover blood spots after NBS is complete is associated with more positive outcomes for both practices. There were concerns that educating parents about what happens with the leftover blood spots after NBS, along with education about NBS alone, may cause a decline in support and participation within this important public health program (Rothwell et al., 2011). Reasons for this skepticism are that in addition to quality control and assurance purposes, the DBS are used for other biomedical research that are not directly related to NBS. Using leftover DBS for research outside of NBS and without parental permission for NBS itself, might raise concerns among parents and they may object to NBS all together. Yet, the primary outcome of this research is that when educated about NBS and leftover DBS at the same time, and provided a choice, parents are more supportive of an opt-out consent approach for the storage and use of leftover DBS for research and higher trust for NBS.
Due to proposed changes to the Common Rule and the changes to the Newborn Screening Saves Lives Reauthorization Act, this research raises questions about the best way to maximize limited public health and research resources. The new section in the Newborn Screening Saves Lives Reauthorization Act requires that federally funded research on residual DBS will be considered human subjects research and must include explicit written parental consent. In the state of Michigan, where the state health department created the Michigan BioTrust, there is only a 60% parental consent to allow the samples to be used in research (Michigan Department of Community Health, 2013). This low uptake is not primarily from parental refusal but more from the logistical challenges of obtaining consent at this time in the hospital. Finally, signatures on consent forms can be easily obtained in many clinical circumstances with limited or no comprehension by individuals signing the form.
The question remains regarding the best approach for obtaining consent for the storage and use of leftover DBS. If state health departments focus on improved education efforts with the option to opt-out, will that result in more informed decision making? Or should resources be used to obtain a signature with current education efforts recognizing the difficulties of obtaining consent in the hospital after recovering from birth and with the demands of a newborn? Increased knowledge is associated with increased trust as supported with this research;therefore shouldn’t improving the education be more of a priority than just obtaining a signature for use of leftover DBS for research.
Proposed changes to the Common Rule will require consent for research with prospectively collected biospecimens but it is unknown whether these regulatory changes will be adopted and, if so, how they will be implemented. Within the context of NBS programs, the primary goal is to screen infants for early identification of inherited medical conditions so that a timely treatment and intervention can take place. Efforts now need to include promoting education and transparency about how leftover DBS are obtained through a mandatory public health program and not only obtaining a parent signature at the hospital as the Notice of Proposed Rule Making seems to be suggesting. We also have an obligation to enhance comprehension. The results also support other research in that prior education levels and race influence trust and consent preferences (Richardson et al., 2012). For example, in a study that assessed consent preferences for biobank participation between Black and White women, results indicated that Black participants wanted study specific information about future studies prior and after donating their biospecimens (Brown et al., 2016). Furthermore, Black participants stated they would prefer to be asked for permission before the biospecimens were used in each future study, while White participants preferred only a one-time broad consent approach.
Both the states of California and Michigan demonstrate the challenges of hospital-based efforts to obtain consent beyond NBS itself. It is not that all parents are refusing participation but they are not adequately provided an opportunity to provide a choice. Efforts to promote trust and transparency through improved education across diverse groups as opposed to a signature will ensure the continued use of important biospecimen research for improving the health care of infant and public health.
Best Practices
This study supports the use of video-based prenatal education materials for parents in conjunction with brochures-based education to promote improved trust with NBS. Most importantly, when participants have an adequate understanding about both NBS and the retention and use of leftover blood spots from NBS, increased trust for research occurred. Interestingly, educating parents prenatally about both topics (NBS and leftover dried blood spots) at the same time is associated with an opt-out consent preference for research with leftover dried blood spots.
Research Agenda
More research is needed to further investigate parental attitudes on consent preferences for biomedical research with leftover DBS. This research demonstrated increased support for an opt-out approach when parents received both video education interventions prenatally than just brochure-based education and prenatal video education on NBS alone. Future research will need to examine when an opt-out approach combined with robust educational interventions may be more appropriate and better use of resources especially within public health programs. This future research needs to include a diverse sample of participants to capture differing opinions toward the use of leftover blood spots used in research.
Educational Implications
Video-based education during prenatal care in this study was more effective than brochure-based only education for promoting trust for NBS and support for research with leftover dried blood spots. Communicating complex topics such as NBS and retention and use of leftover dried blood spots for research require more detailed explanations and use of multimedia interventions improve participant comprehension. Exploring methods to deliver this type of intervention on a population level is needed to ensure continued support for NBS and research use of leftover dried blood spots.
Footnotes
Acknowledgements
We would like to thank our colleagues with the parent study of this research and include Louisa Stark, Miriam Kuppermann, Nancy Rose, Siobhan Dolan, and Aaron Goldenberg.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent study was funded by the National Institutes of Health (1R01HG006266-02).