
Abstract
Proposals for research concerning fetal and/or placental tissue may be refused institutional review board (IRB) review, effectively preventing the research from occurring. We conducted an anonymous electronic survey of IRB chairs to determine their assessment of the likely response to research projects using fetal/placental tissue obtained from various procedures. We found that proposals concerning tissue obtained from diagnostic procedures or miscarriage were anticipated to be considered at most institutions. Tissue obtained after abortion was likely to be refused consideration by more than 25% of respondents. Additional consultation during review was anticipated for up to 30% of scenarios. Responses for fetal and placental tissue were similar. The most frequently anticipated reason for refusal was institutional policy.
Introduction
Placental and fetal tissues are used in a variety of research activities, including research on gene expression, control of differentiation and growth, and drug and vaccine development. There is widespread opinion that fetal tissue research is appropriate and valuable (Boonstra, 2016; Gelber et al., 2015; Ostrer et al., 2006; Seifert, 1997; Tuch et al., 2003), and the results of fetal tissue research are widely used. In the United States, fetal tissue research is associated with controversy because of both the type of tissue and the origin of the tissue (Charo, 2015). There may be barriers to fetal tissue research, including statutory restrictions, funding prohibitions, and denial of institutional approvals; human subjects research in the United States must be approved by an institutional review board (IRB) prior to initiation, and an IRB can determine whether or not a study can be initiated.
Fetal and placental tissue may be obtained as extra tissue from diagnostic procedures, from miscarriage, from induced abortion, or from cultured cell lines. Each type of tissue has some limitations to collection. Diagnostic procedures produce very little cellular material or tissue as only the minimum amount is collected from an ongoing pregnancy for safety reasons. Tissue from miscarriage may not be viable or may be abnormal, and cultured cell lines may have genetic differences from normal tissue. Therefore, induced abortion of apparently normal pregnancies is a source of much of the tissue ultimately used for research.
Multiple anecdotes of IRB responses to research proposals that involve fetal or placental tissue suggest both gaps in knowledge and contradictory practices. Some IRBs have refused to consider such proposals altogether, regardless of scientific merit. In other instances, delayed review or other barriers may threaten funding or result in additional delay, expense, or waste of resources. Barriers may extend to other areas of research. As an example, an IRB refused to consider research on commercially available cell lines, as the origin of the cell line was uncertain and it was possibly of placental origin (personal communication, March 2014). Another proposal to study decidual tissue (which is produced by a woman in response to pregnancy and is not of fetal origin) resulted in an extended delay due to concern that the tissue was a product of conception (personal communication, April 2014). These and other anecdotes are consistent with situations described by Harris (2013).
Some of the delays and refusals appear to result from board-specific policies, and some appear to be determined by the educational or medical institution to which the IRB belongs. These decisions and policies, in turn, can be further traced to federal or state statutes and regulations, which have been cited as reasons for institutional restrictions. In addition, there may be inconsistencies in the way that regulations or policies are interpreted by IRBs (Abbott & Grady, 2011).
To further explore expected IRB responses to research proposals concerning tissue resulting from human pregnancy, we conducted a survey of IRB chairs and directors. The survey was limited to expected IRB responses to proposals involving tissue that was removed during pregnancy for diagnostic procedures or resulted from termination of pregnancy, and to procedures related to obtaining tissue. This was an anonymous survey that was intended to require no more than 10 to 15 min to complete.
Method
An electronic survey was developed specifically for this project (Appendix A). The introduction to the survey informed potential respondents that it was voluntary and anonymous. The project was deemed exempt from human subjects review by the Boston University Medical Campus IRB. The survey was first completed by a pilot group of 20 IRB members, and minor changes were made to the wording.
The survey was administered to IRB chairs and directors. A list of the email addresses of all IRB chairs was obtained from the federal Office of Human Research Protection in response to a Freedom of Information Act request, dated October 28, 2014. Similar information was not available for IRB directors, nor was there any other systematic source of email addresses. Instead, domain names identified from the list of chairs were used to access the parent institution of the IRB. The website was manually searched to identify email addresses of IRB directors. For many sites, the IRB director was not named, or there was no institutional IRB office; IRB offices were more likely to be identified in universities or medical schools than in hospitals. Not every domain name was searched, and the sample of IRB directors was thus considered a convenience sample.
The survey was administered and results were compiled by the Slone Epidemiology Center at Boston University. Survey invitations were sent up to three times. Addressees could opt out of subsequent invitations and were removed from the mailing list upon request. Repeat survey invitations were sent to all addresses that were not opted out, as replies were not linked with addresses to maintain anonymity. Upon opening the survey, respondents were asked whether they were an IRB chair or director, or a vice- or associate chair or director. They were also asked whether their IRB considered protocols concerning pathologic specimens. If they did not answer both items affirmatively, they were considered ineligible.
Eligible respondents were asked a limited number of demographic and professional questions such as age, their position on the IRB, and the type of institution. The next segment of the survey contained nine questions about types of tissue that might be used in research (Figure 1). The respondent was asked whether an otherwise meritorious application would be considered or not reviewed. The range of possible initial responses (Figure 1) and reasons for refusal to consider (Figure 2) were the same for each item. The following section (Figure 3) contained questions about the classification of studies of discarded tissue. In addition to the categorical response options, comments were encouraged in open text fields that accompanied each question. Four additional questions were related to procedure technique and are not considered in this report.
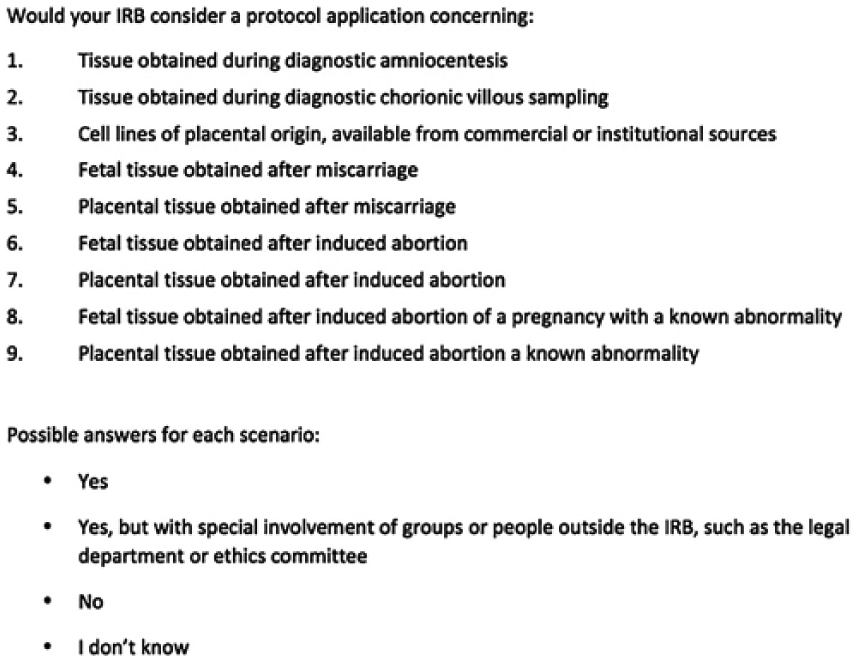
Survey questions for tissue scenarios.
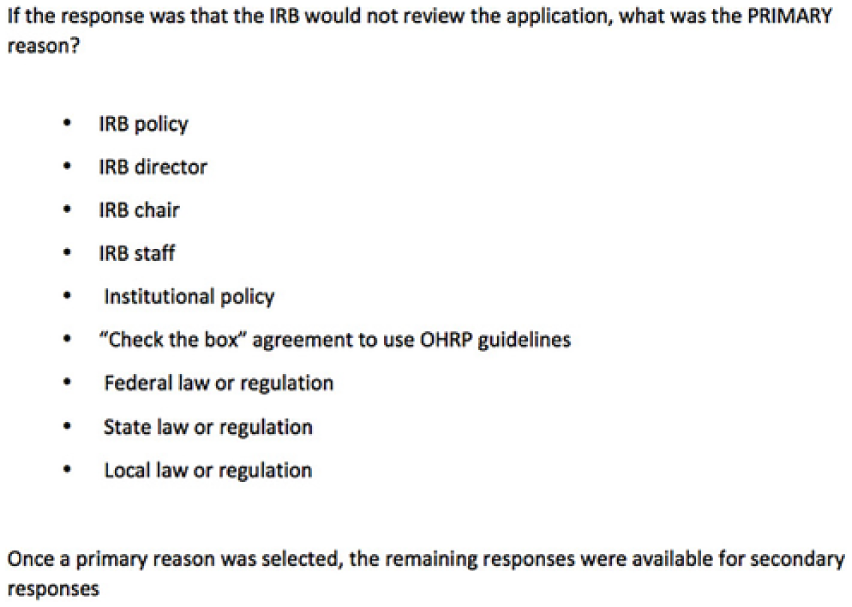
Reason for refusal of consideration for tissue scenarios.
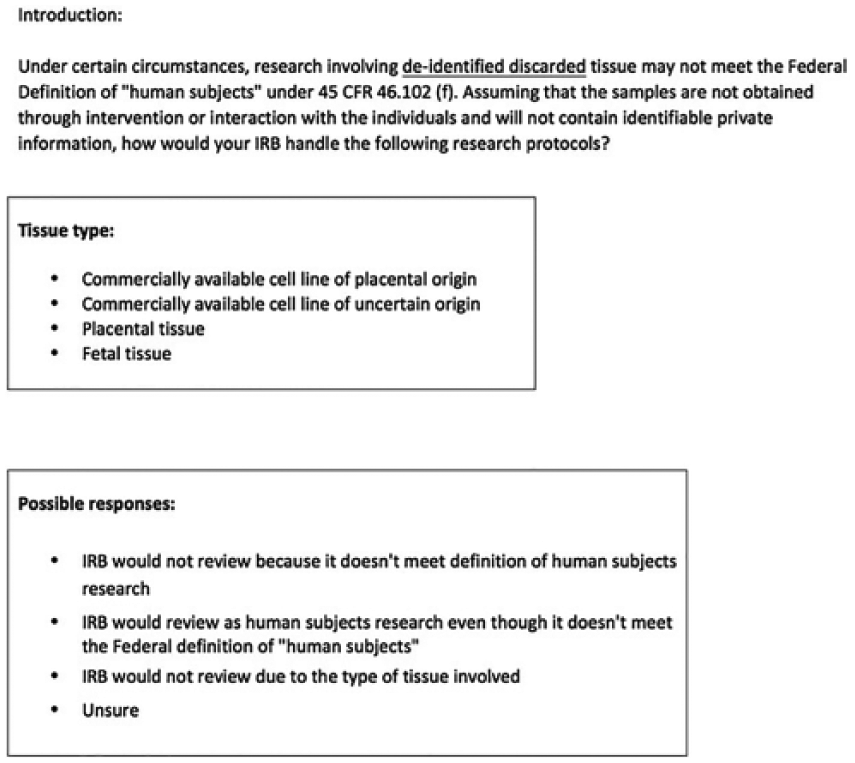
Survey questions for de-identified discarded tissue.
The survey questions were restricted to tissue research and did not address transplantation of fetal or placental tissue. We did not include procedures involving fetal surgery, umbilical cord blood banking or research, or research on embryos created as a result of assisted reproductive technologies. Placentas obtained after childbirth were also not considered.
Differences were assessed by comparison of frequencies of the various responses and, where relevant, odds ratios (ORs) with 95% confidence intervals. The primary outcome of interest was refusal to consider a protocol.
Results
The survey was conducted between March and May of 2015. Invitations were sent initially to 3,642 addresses (3,231 IRB chairs and 433 directors, with 22 on both lists); 312 were invalid, leaving 3,330 addresses. There were 51 opt-out responses and 15 who responded by email that they were not eligible, leaving 3,264 who probably received an invitation and did not opt out. Of these, 760 recipients (23.3%) responded initially. Twenty-four were not eligible as the respondent was neither a director nor a chair, and 392 IRBs did not review tissue research. Two hundred twenty-five surveys were received from respondents who identified themselves as chairs or vice-/associate chairs. Of these, 36 opened the survey but did not submit answers, leaving 189 completed chair responses. Ninety-one surveys were opened by self-identified directors or vice-/associate directors, with 68 complete director responses. As the sampling method for directors was different, and the anonymity of the responses did not permit identification of chair and director responses from the same institutions, we chose to confine the present analysis to chairs.
Of the chair responses, 81 (43%) were associated with academic institutions, 73 (39%) with medical centers or hospitals, 14 (7.4%) with military or government facilities, and 21 (11%) with independent IRBs. The majority were male (61%), and almost all had either an MD (57%) or PhD (38%) degree; the median age was 58 years. Thirteen (7%) identified themselves as vice- or associate chair, and their responses are combined with those of chairs.
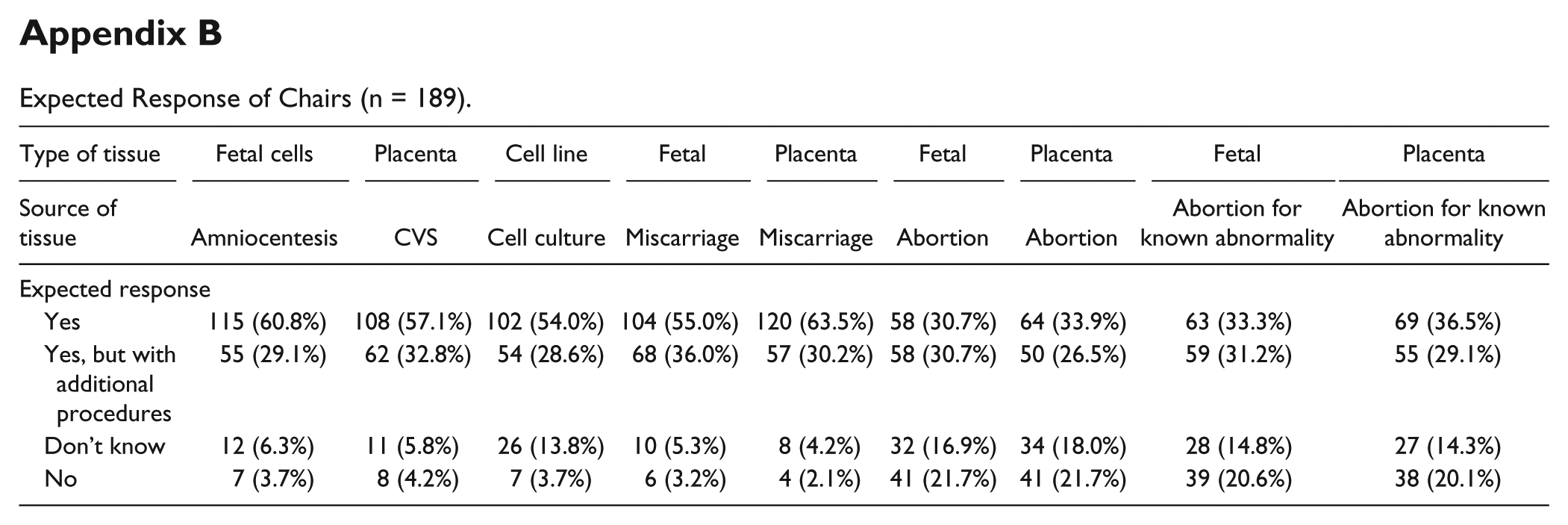
The responses to the questions about research on tissue obtained under various scenarios are shown in Figure 4 and Appendix B. Overall, for tissue from diagnostic procedures (amniocentesis and chorionic villus sampling [CVS]) or miscarriage, 50% to 60% of respondents said they expected usual review procedures, while less than 5% thought the protocol would not be reviewed at all. Results were similar for research on placental cell lines. Approximately 30% of respondents indicated that they would seek additional consultation for the review. For tissue obtained from diagnostic procedures, there were a total of 17 comments related to additional consultation: Nine indicated that they would seek more information from outside experts, while two indicated that they would seek outside legal advice.
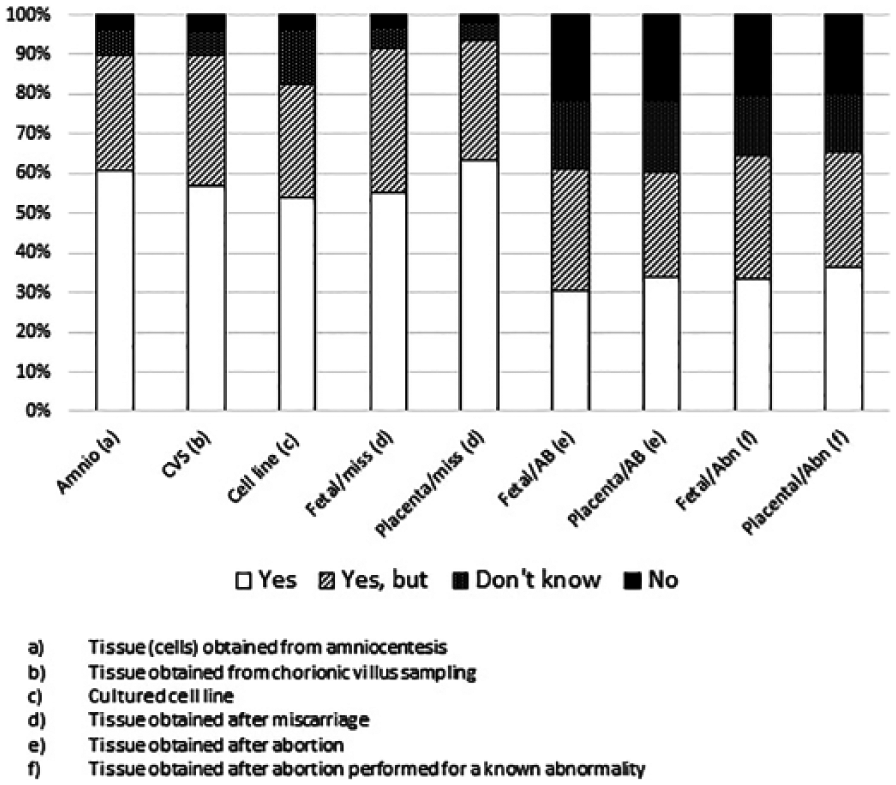
Responses of chairs.
By contrast, for the four scenarios involving tissue obtained after an induced abortion, a markedly lower proportion, about a third of respondents, would review the protocol by usual procedures. About 20% of respondents anticipated refusal to review the protocol at all (Figure 4). Responses were similar regardless of whether fetal or placental tissue was the subject of the study, and whether the abortion was related to a fetal anomaly or not. Although 25% to 30% of respondents for these items anticipated additional consultation, only a few provided comments about the types of consultation that would be sought; these indicated that such additional consultation would frequently consist of gynecologic expertise or technical expertise related to the type of research. This response was more common than anticipating additional legal, regulatory, or other ethics opinions.
For the scenarios not related to induced abortion, the number of anticipated refusals to review ranged from four to eight out of 189 responses for each item (Table 1, Scenarios 1-5). Of the refusals for these scenarios, 13/32 (41%) were attributed to the IRB chair or IRB policy. The five attributed to federal law were cited by the same respondent. Institutional policy was cited for several items; one subject commented that this was because the institution was Catholic. Several respondents said that they were from institutions with limited practice (i.e., Veteran Affairs [VA] hospital or cancer institute) and would be unlikely to ever have to consider such a scenario.
Primary Reasons for IRB Chairs to Anticipate Refusal to Consider a Protocol.
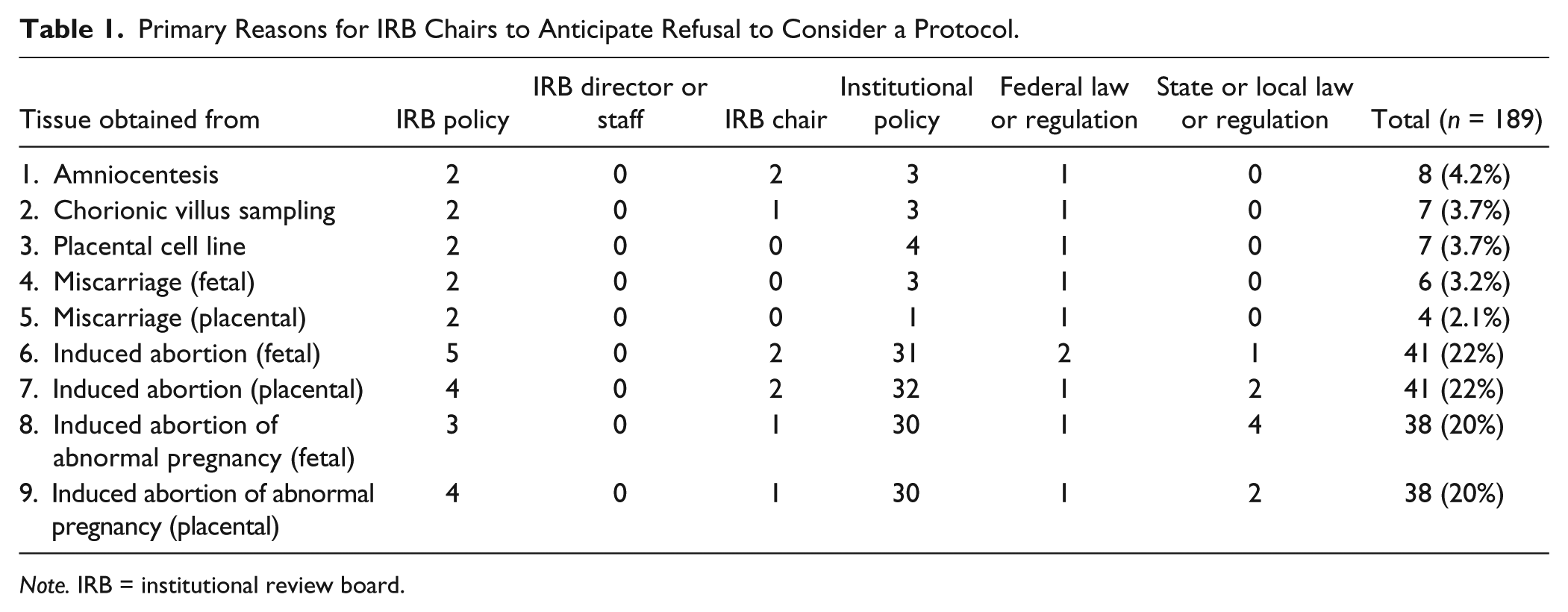
Note. IRB = institutional review board.
The most common reason for refusal of research related to tissue obtained after abortion was institutional policy (Table 1, Scenarios 6-9), accounting for more than 75% of all anticipated refusals. The rationale for the institutional policy was not asked in the survey, but 10 respondents commented that the institution was Catholic. Several others said that abortions were not done at their institution. Several respondents ascribed refusal either to the IRB chair or to IRB policy. Only one person consistently attributed refusal to federal regulations (the same individual who gave that answer for the nonabortion scenarios). Several attributed refusal to state regulations; the states cited were Connecticut, Oklahoma, and Texas. Of these, only Oklahoma has such a state regulation.
Academic IRBs were considered the least likely to completely refuse to consider abortion-related protocols (range across the four scenarios, 9%-10%), and hospital-based IRBs the most likely (34%-37%), with the other IRB types intermediate (Table 2). Most respondents gave the same answer for all four scenarios. ORs comparing hospital with academic IRBs, ranged from 5.4 to 6.2, with lower confidence limits 2.2 or higher.
Refusal to Consider Protocols Related to Abortion According to IRB Type.
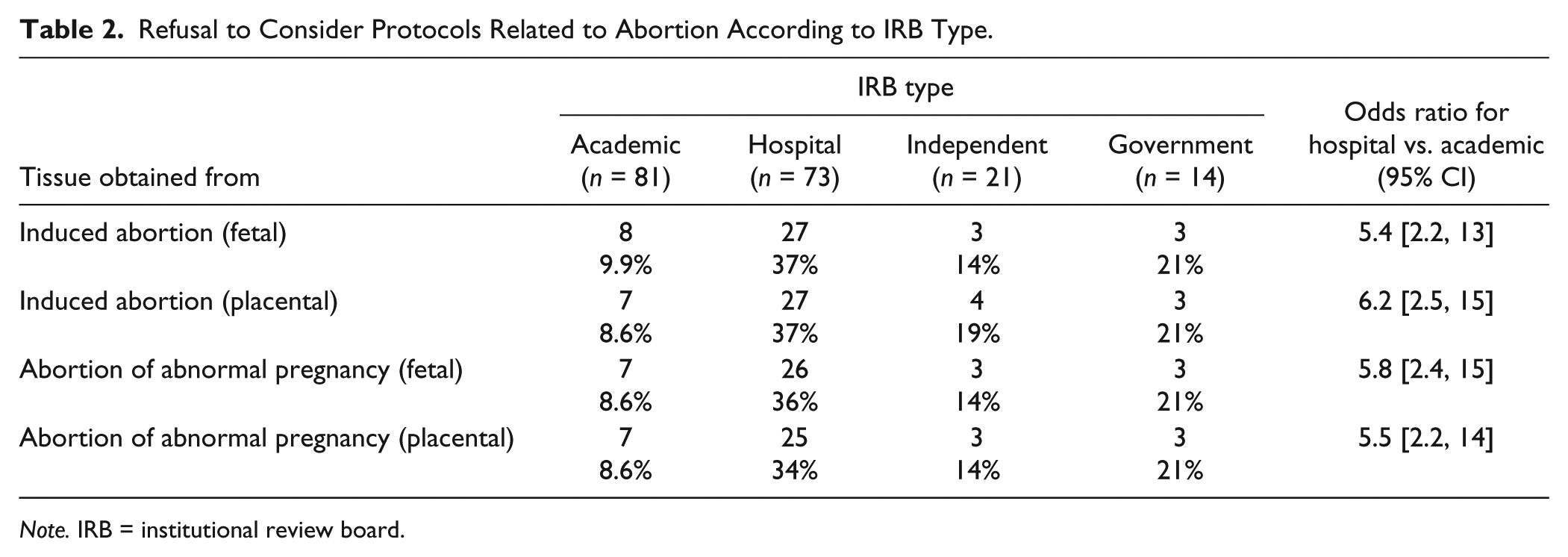
Note. IRB = institutional review board.
When research projects involve discarded de-identified tissue, an IRB may determine that the research proposal does not need review because it does not involve human subjects (“not human subjects research” [NHSR], 45 C.F.R. 46.102). Alternatively, an IRB can decide to review such proposals as “human subjects research.” Overall, placental cell lines were the most likely to be considered NHSR (46%) and fetal tissue the least likely (26%), with intermediate values for cell lines of unknown origin and placental tissue (41% and 35%, respectively; Table 3). Few respondents (2%-9%) said that their IRB would not review the protocol. In the comments section, some respondents were concerned about the ability to re-identify “de-identified” tissue by genomic analysis, and therefore, questioned whether tissue could truly be de-identified. Compared with academic IRBs, hospital IRBs were significantly less likely to consider each type of tissue as exempt from human subjects review, with ORs ranging from 0.2 to 0.4 (Table 3).
Responses to Questions About De-Identified Discarded Tissue.
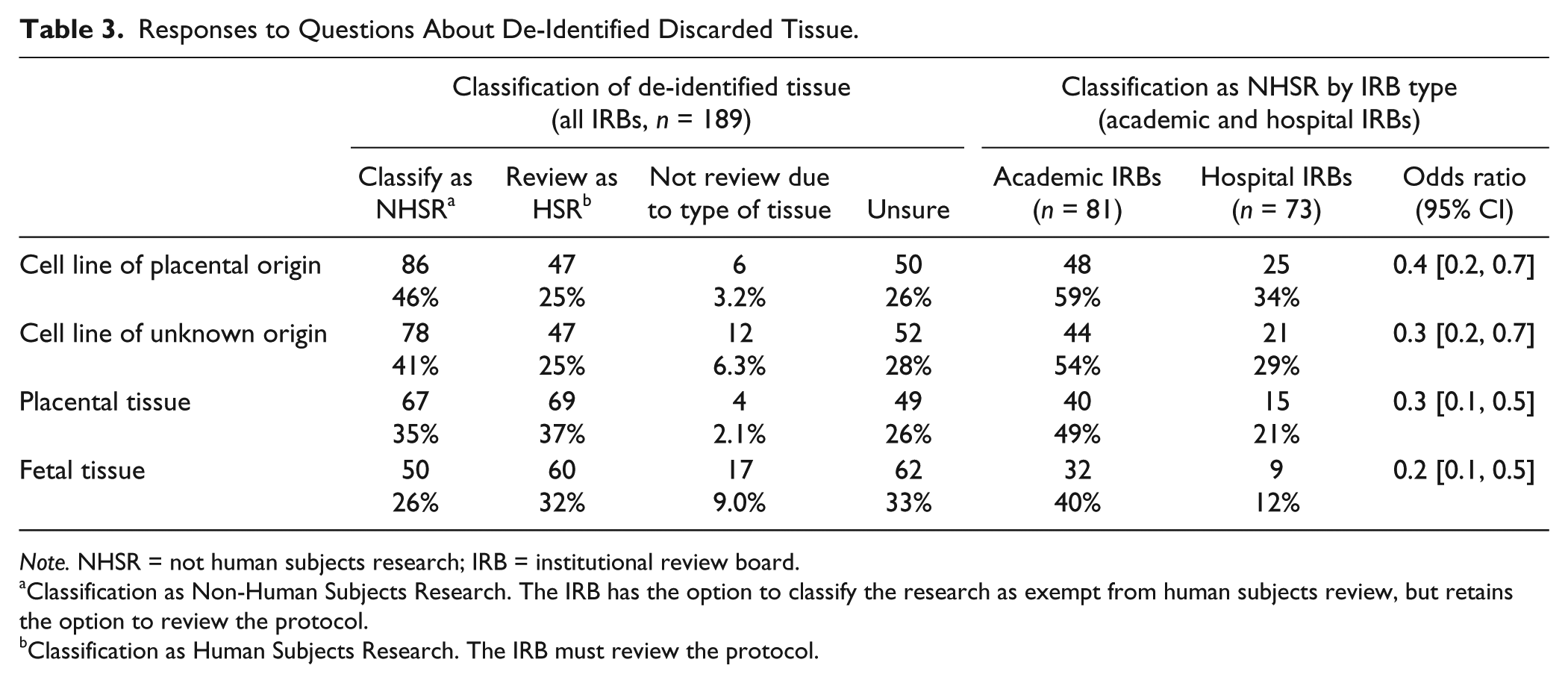
Note. NHSR = not human subjects research; IRB = institutional review board.
Classification as Non-Human Subjects Research. The IRB has the option to classify the research as exempt from human subjects review, but retains the option to review the protocol.
Classification as Human Subjects Research. The IRB must review the protocol.
Discussion
Each scenario presented in this survey had a wide distribution of responses. Amniocentesis and CVS are invasive diagnostic procedures with low morbidity performed during pregnancies; there may be additional fetal cells (in the case of amniocentesis) or placental tissue (CVS) remaining for research. In general, most IRBs would consider a research project using tissue obtained from an amniocentesis or CVS. However, there were some that expected refusal to review, and institutional policy was most frequently cited.
All other scenarios postulated tissue obtained after a pregnancy had ended. Most respondents stated that their IRBs would review a research proposal concerning tissue obtained after miscarriage. However, when the tissue was obtained from an induced abortion, fewer respondents expected that the protocol would be reviewed, and more than 20% felt that it would not even be considered.
In all scenarios, up to 30% of respondents indicated that consultation or input from someone outside the usual IRB process would be solicited. The type of consultation was not specifically asked about in the survey; some commented that they would request a consultation from an obstetrician-gynecologist. This suggested to us that some of the respondents were unfamiliar with the issues raised by the survey, or felt they did not have enough information to make a determination. We expected that some IRBs would request legal or other ethics opinions, but we do not know how often this was anticipated. Additional procedures may be appropriate; they might aid in consistency of IRB determinations, and may be protective to the IRB if a decision is anticipated to be controversial.
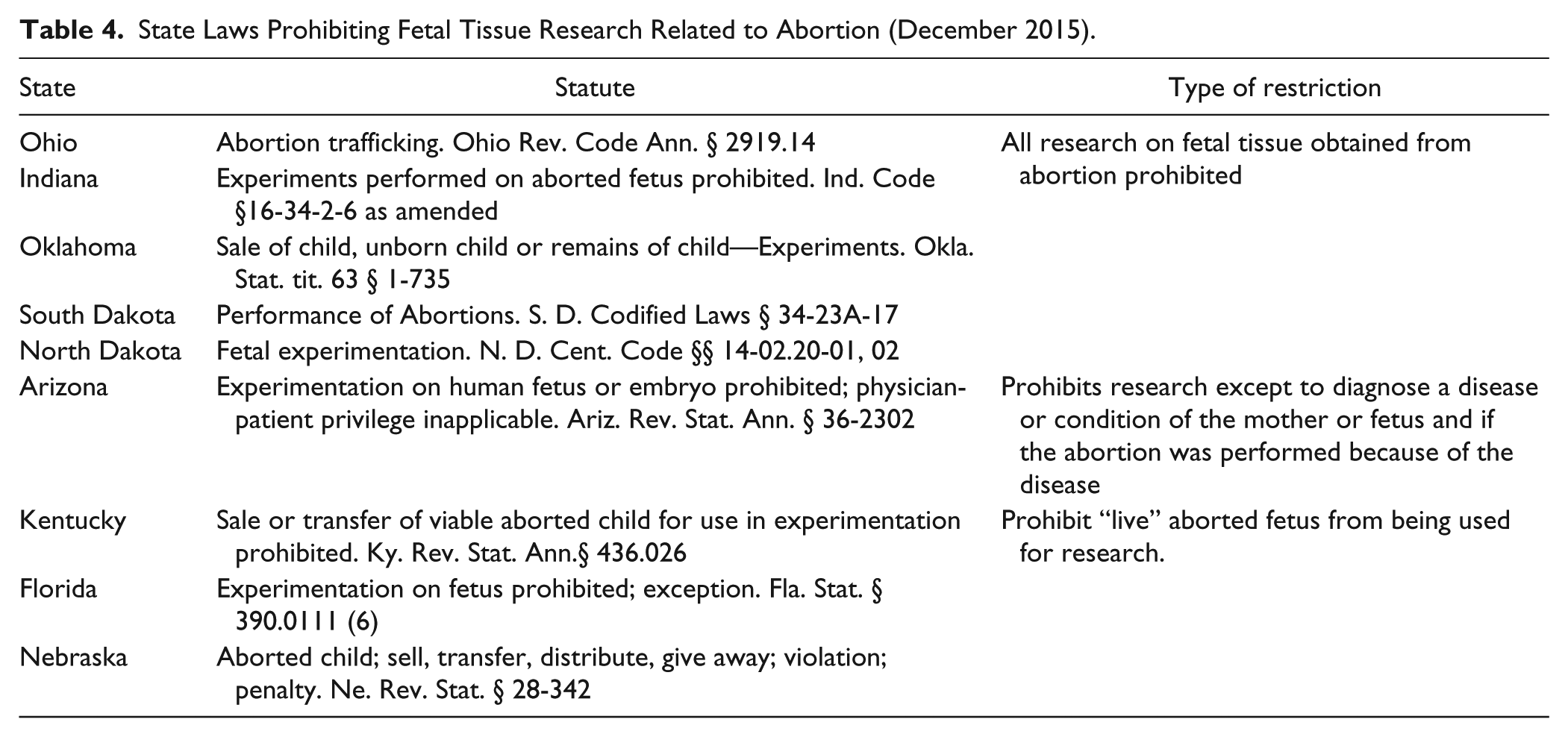
Federal law governing fetal tissue research is limited (Figure 5). In reinstating the capacity of the federal government to fund research involving fetal tissue, the NIH Revitalization Act of 1993 (Pub L, U.S.C. 1993, 2006) essentially prohibits the purchase or sale of the products of conception. Federal regulations, referred to as Subpart B, delineate standards of allowable risk and demarcate the extent of researcher involvement in the clinical care of the patient who has agreed to make available such tissue for research (45 C.F.R. § 46.204). Importantly, these federal regulations explicitly recognize the authority of states to regulate in this area (45 C.F.R. § 46.206). At the time of writing, at least five states forbid any research with aborted tissue, irrespective of the transfer of value (Table 4), and at least three others forbid research on a “live” aborted fetus. Additional proposed legislation seeks to further restrict related research. Boonstra (2016) has summarized the restrictions on fetal research existing at the end of 2015.
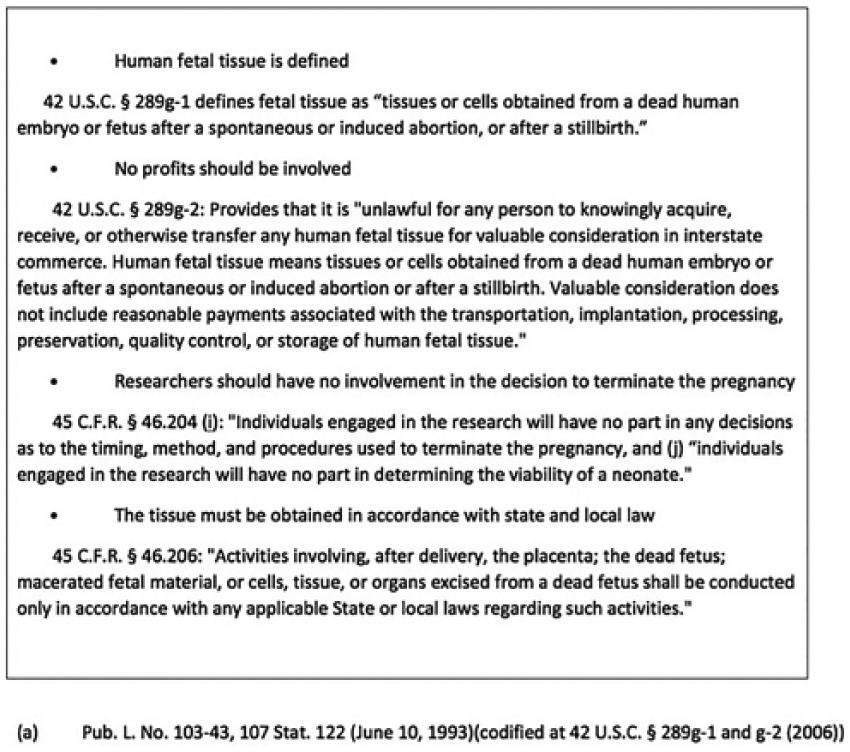
Federal regulations concerning fetal tissue and research.
State Laws Prohibiting Fetal Tissue Research Related to Abortion (December 2015).
The statutory guidance for using pregnancy tissue does not make a distinction between fetal and placental tissue. To our surprise, we found that responses to scenarios using fetal and placental tissue were very similar. Although they are both of fetal origin, we expected that there would be more barriers to using tissue that was identifiably “fetal” as opposed to placental tissue. Similarly, responses were essentially the same when induced abortion for fetal abnormality was compared with induced abortion without a stated indication. We might have expected that abnormal pregnancy, which might yield information about etiology or treatment of abnormality, would be more acceptable as a research topic.
We did not identify any state statutory restrictions on research on fetal or placental tissue resulting from miscarriage. One respondent offered a specific state statute as a reason for refusal, but the language in the statute was not relevant. This indicates that there may be some confusion about the actual language, or misinterpretation of legal opinion. Fetal tissue or cells from diagnostic procedures of amniocentesis or CVS do not meet the definition of fetal tissue (Figure 5); they also do not appear to have specific statutory restrictions related to tissue research; however, C.F.R. 45 46, Subpart B may be applicable in evaluating the procedures in terms of risk of the procedure itself.
Under current Office for Human Research Protections (OHRP) guidelines, an IRB can make a determination as to the type of review required, if any, for de-identified tissue. No special procedures are mandated for de-identified fetal or placental tissue, provided the other restrictions are met. We found that academic IRBs were more likely to determine that such protocols do not involve human subjects; the effect of a “not human subjects research” determination usually means that the research does not require further review and might not require individual consent of the tissue donor.
This survey had a number of limitations. It was unsolicited and unannounced, and to encourage participation, it was brief. The subject matter was irrelevant to IRBs attached to institutions that do not do any pregnancy tissue research. We had no way of targeting IRBs that were likely to be familiar with such research. We believe that medical schools (there are approximately 170 allopathic and osteopathic schools in the United States) and a relatively few independent or commercial research sites, such as those investigating potential therapeutic or diagnostic uses, are the most likely to conduct fetal tissue research. Therefore, the 189 completed chair responses may represent many of the IRBs that actually address fetal research.
IRB panels vary greatly in the number of protocols considered (Catania et al., 2008; Wagner et al., 2004). Some IRBs have multiple panels with different chairs, and may have contributed multiple responses to this survey. Given the variation of IRBs, quantitative assessment of restrictions on research may be of limited value. Staffing and board membership may range from the voluntary occasional participant to the full-time professional. In some IRBs, a director or staff member may determine which proposals reach the IRB chair and board members.
Despite the heterogeneity of IRB size and composition, several patterns were evident. Academic and independent IRBs appeared more likely to consider protocols under all scenarios and were more likely to anticipate a nonhuman subjects research determination for de-identified tissue. We speculate that these IRBs may be from larger institutions with more research activities, and hence perhaps more familiar with the issues than hospital IRBs.
This survey supports the impression that responses to fetal and placental tissue proposals are diverse, and that there are frequent barriers. Institutional policy plays a significant role. Affiliation with a religious organization was the most common individual reason volunteered for refusal related to institutional policy, but the questionnaire did not specifically ask about religious affiliation, so it was not possible to determine whether that was the major determinant of institutional policy. In a brief survey, we also were not able to determine whether an institution had a formal policy, or whether the institutional approach was assumed.
Despite the benefits that have accrued from fetal tissue research, it remains controversial in the United States, regardless of the method of obtaining the tissue. In particular, the heated controversy about abortion has complicated the situation. Subsequent to the administration of this survey, widespread controversy over allegations of improper tissue collection procedures produced calls to end all fetal tissue collection, and therefore fetal tissue research (Boonstra, 2016; Charo, 2015).
In conclusion, the present results suggest that there is a spectrum of responses within IRBs about research with fetal and placental tissue. Refusal to consider such research was most frequently attributed to institutional policy. While it was not possible to determine how often religious affiliation influenced policy, it is certainly a factor. The most prominent difference in response was not related to the type of tissue itself, as questions about fetal, placental, and cell culture had similar responses, but rather to the association with abortion. This concern contributes to delay or rejection of research applications for reasons unrelated to scientific merit.
Best Practices
Clarification of the anticipated responses and the reasons for the responses would make IRB consideration more efficient and consistent. Fetal tissue from different sources may be subject to different regulations, and familiarity with applicable statutes and regulations may be helpful to both investigators and IRB staff. If there is an insurmountable barrier, the researcher may be faced with moving or abandoning their research.
Research Agenda
The process of IRB consideration involves internal IRB processes that may determine which proposals reach the IRB board. As IRB structure varies, it would be helpful to clarify the processes that influence whether research concerning fetal tissue reaches board review, and whether or not there are barriers within the IRB itself. As additional review or opinion was anticipated by nearly a third of respondents, it would be helpful to know the type of information or opinion (legal, technical, etc.) that would be requested. While institutional policy was cited as the most frequent barrier, it would be helpful to document whether there are formal policies, or assumptions about policy. The reasoning behind the possible institutional barriers and the contribution of religious restrictions would require more in-depth assessment.
Educational Implications
The diversity of responses and the high rate of anticipating additional consultation may indicate that many chairs are unfamiliar with the issues raised. With concern or anxiety about the subject matter, delay or refusal of consideration may be the easiest response for IRB chairs and personnel. Clarifications of the actual statutory and regulatory restrictions, or lack of restrictions, and examples of possible responses may be helpful to avoid unnecessary barriers. Conversely, knowledge of local constraints may allow more consistent and predictable responses. Resources for investigators may facilitate IRB submissions or avoid situations where the environment is hostile for reasons unrelated to scientific merit.
Footnotes
Appendix A
This is a text of the email that was sent to potential participants. It contained a link to the survey, and an option to opt out of further contacts.
You are invited to be part of a research survey about institutional review board (IRB) practices concerning protocols that may be controversial because they concern pregnancy tissue and/or research related to pregnancy diagnosis, miscarriage, or termination.
Your feedback is important to the success of this study. A high response rate is crucial for ensuring that the results of this survey accurately reflect the range and frequency of practices. Individual responses are anonymous, and data will be analyzed and reported in aggregate form only.
Thank you for your participation.
Appendix B
Expected Response of Chairs (n = 189).
| Type of tissue |
Fetal cells |
Placenta |
Cell line |
Fetal |
Placenta |
Fetal |
Placenta |
Fetal |
Placenta |
|---|---|---|---|---|---|---|---|---|---|
| Source of tissue | Amniocentesis | CVS | Cell culture | Miscarriage | Miscarriage | Abortion | Abortion | Abortion for known abnormality | Abortion for known abnormality |
| Expected response | |||||||||
| Yes | 115 (60.8%) | 108 (57.1%) | 102 (54.0%) | 104 (55.0%) | 120 (63.5%) | 58 (30.7%) | 64 (33.9%) | 63 (33.3%) | 69 (36.5%) |
| Yes, but with additional procedures | 55 (29.1%) | 62 (32.8%) | 54 (28.6%) | 68 (36.0%) | 57 (30.2%) | 58 (30.7%) | 50 (26.5%) | 59 (31.2%) | 55 (29.1%) |
| Don’t know | 12 (6.3%) | 11 (5.8%) | 26 (13.8%) | 10 (5.3%) | 8 (4.2%) | 32 (16.9%) | 34 (18.0%) | 28 (14.8%) | 27 (14.3%) |
| No | 7 (3.7%) | 8 (4.2%) | 7 (3.7%) | 6 (3.2%) | 4 (2.1%) | 41 (21.7%) | 41 (21.7%) | 39 (20.6%) | 38 (20.1%) |
Authors’ Note
Lynn Borgatta is now at Quorum Review, Inc., Seattle, Washington. The views expressed do not necessarily represent the views of Quorum Review, Inc., or Kinetiq, Inc.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded with internal department discretionary research funds and did not have any commercial support.