
Abstract
The informed consent/assent process during enrollment in pediatric research is integral to protecting children from possible harm. Here we explored parents’ perceptions about the informed consent/assent process in Jordan. Therefore, focus group interviews were conducted that focused on the importance of consent/assent, the quality of the information provided during consent process, and the parents’ perceptions toward written/verbal informed consent. Content thematic analysis approach was adopted in the transcription and translation processes of the interviews. The majority of parents have an ethically acceptable understanding of many of the aspects related to consent/assent; however, some views were not consistent with the proper conduct of research. For example, some parents believed that informed consent is not required for questionnaire studies. Discrepancies were also noted regarding the appropriate age of a child’s assent. Some parents would force their child to participate. Thus, the development of Jordanian, culturally sensitive pediatric research guidelines is required.
Introduction
Pediatric research is vital for understanding the behavioral and social characteristics of children as well as for the advancement of knowledge in health, disease, and therapeutic strategies for children (Davidson & O’Brien, 2009; Tromp, Zwaan, & van de Vathorst, 2016). One important element of pediatric research is the informed consent process, including guardian permission and child assent, which are both prudent agreements to participate in research (Allmark, 2002; Hein et al., 2015). Consent is a legal agreement between the researcher and a potential study subject or an authorized representative. Similarly, assent is an active affirmation of a desire to participate in research by someone who is too young to give legal consent yet mature enough to understand the study. Consent/assent is usually obtained after sufficient information about the study procedures, possible risks/benefits, and expectations are provided (De Lourdes Levy, Larcher, Kurz, & Ethics Working Group of the Confederation of European Specialists in Paediatrics, 2003; Roth-Cline & Nelson, 2013). Therefore, assent is an opportunity for children to decide whether or not to take part in a study (Giesbertz, Bredenoord, & van Delden, 2014). The guardian consent and child’s assent should be obtained prior to a child’s participation in research (Leibson & Koren, 2015; Unguru, 2011). This process is crucial to preserve children’s rights during their participation in research, including protection from possible harm, violation of privacy, legal risks, and psychological or emotional stress (De Lourdes Levy et al., 2003; Ngui, Warner, & Roberts, 2014).
Despite numerous publications that address ethical issues, very little is known about pediatric research in the Arab region (Alahmad, Al Jumah, & Dierickx, 2015). One study has shown positive attitude and perception of Lebanese parents toward pediatric research (Nabulsi, Khalil, & Makhoul, 2011). Participants in the “Abu Dhabi Cohort Study” (El Obaid et al., 2016) reported satisfaction with the informed consent process. Conversely, a study by Arabiat (2014) reported some ethical challenges while obtaining children’s assent in cancer research in Jordan. One of these challenges was providing sufficient information for children who were unaware of their cancer diagnosis (Arabiat, 2014). Another study, which examined the Jordanian prospective about biobanks, showed that the majority of the sample did not seem to be concerned about the existence of an informed consent process as much as the benefits of the study (Ahram, Othman, & Shahrouri, 2013). The later study recommended that education programs be conducted to enhance public knowledge about the importance of consent in research.
In Jordan, research that involves children is growing rapidly; however, the available ethical guidelines/research policies have been adopted from other countries without sufficient considerations of local culture/religion. Thus, more studies related to ethics in pediatric research are needed. Therefore, the aim of the present study was to explore parents’ perceptions about the informed consent process in Jordan. To achieve this aim, focus group interviews were conducted to evaluate parent perspectives of guardian consents and child assents during pediatric research.
The results are particularly important for several reasons. The population of children in Arab countries, including Jordan, is among the highest in the world (Abdul Salam, Elsegaey, Khraif, AlMutairi, & Aldosari, 2015). In addition, Jordan is considered among the advanced countries in the Arabic world in medical research, which is mainly regulated by local institutional review boards (IRBs) and based on the Helsinki declaration (Zyoud, Al-Jabi, & Sweileh, 2015). Furthermore, it is a primary site for pharmaceutical development, with over 20 companies for manufacturing and exporting generic drugs to neighboring countries (Bowman, 2014; Lafi, Robinson, & Williams, 2012). The Jordanian pharmaceutical industry has attained contracts with several national research organizations to conduct clinical drug trials and related human research (Al-Shaikh, Torres, Zuniga, & Ghunaim, 2011). Finally, the Jordanian law regulates clinical research, but guardian consent/assent in clinical studies is largely ignored. Furthermore, the legal rights and welfare of children participating in research have, unfortunately, not been declared (Ramahi & Silverman, 2009). Thus, in Jordan, there is no clear regulation for pediatric research, with the exception of the Jordanian law that considers individuals below 18 years as minors (Jordanian Civil Law, 1976, p. 43). Therefore, until the age of 18 years, parents/guardians are legally and morally responsible for managing the child’s affairs, including making suitable decisions on behalf of the child.
Method
This was a descriptive and qualitative study aimed at understanding parents’ perceptions about the informed consent and assent process in research involving children. Two focus groups, one for fathers and another for mothers, were conducted to achieve the purpose of the study. The children of interest in the current study included school-age children from 6 to 18 years.
The random recruitment of parents was facilitated by inviting two schools from the Irbid district in the Northern part of Jordan. The 1st Irbid (boy) and Ramtha (girl) schools were randomly selected from a list containing all schools from the indicated district. Invitation letters, describing the purpose and details of the study procedures, were sent to parents via the aid of the school principals. The first eight parents who agreed to participate were included in the study. Informed consent was obtained from the participants according to the approval obtained from the Institutional Research Committees of Jordan University of Science and Technology and the Ministry of Education. Permission was obtained from all participants to audio-record the focus group interviews to be transcribed later.
In Jordan, public high schools are unisex; accordingly, the parents were invited to the children’s perspective schools. The participants were middle aged (35-50 years). All fathers and only two mothers were employed. The vast majority of parents belonged to low or middle socioeconomic classes. The focus groups were conducted in the participating schools in an unoccupied room using a round table setting. While the focus groups were conducted, only participating parents and the researchers were in the room to ensure confidentiality. Recruited parents were not necessarily aware of the research process or research methods, but this was not an inclusion criterion of recruitment. Thus, at the beginning of the focus group, the researcher explained the purpose, procedures, benefits, and risks of the research protocol to avoid misunderstanding. In addition, the researchers asked parents whether they had participated in previous research. In addition, the questions proposed to be asked in the focus groups were pilot tested on four parents to make sure the parents understood the questions. These parents were not included in the focus group.
The discussion in the focus groups was facilitated by asking probe questions that were centered on three domains. Interactions between focus group members were allowed and encouraged; however, the researchers interfered when the debates strayed away from the purpose of the focus group.
The domains focused on the following: (a) the importance of parents’ consent and children’s assent, (b) the quality and depth of the information provided during the informed consent process, and (c) the parent’s perception toward written/verbal informed consent. Systematic and consistent data collection during the discussions was guided by the predetermined themes’ questions. A professional researcher in qualitative research (N.S.) moderated the discussion, and another individual took notes and aided in the discussion when required. In addition to presenting discussion questions, the moderation process also included encouraging all parents to participate in the discussion, reframing, and repetition for validating the participants’ points of view, and expansion of the questions as required, which increased the credibility of the collected data (Peterson-Sweeney, 2005; Tobin & Begley, 2004). Probing questions were selected based on previous literature in this area as well as the field experience of the researchers. Collected data from the focus groups were transcribed by a third researcher who was not present in the discussion room to enhance the objectivity of the study.
The interviews were transcribed verbatim in Arabic and then translated into English by a member of the research team who was fluent in both languages. Validation of the accuracy of the transcripts was done by the focus group researchers who were also fluent in both Arabic and English languages. The standard procedures that involved the content thematic analysis approach were adopted in the transcription and translation processes as follows: (a) important statements were categorized into different labels; (b) the transcripts and translations were confirmed by exchanging notes, categories, and domains to ensure the credibility of data; and (c) if discrepancies arose, researchers continued deliberating until a resolution was attained. This included additional coding and re-coding of data until the final identified codes and themes were agreed upon. For example, the selection of data extracts, which was achieved by reading the whole transcript for patterns that resulted in several themes (seven labels), was carefully chosen manually by the co-PI (N.S.). These preliminary themes were then labeled and categorized/clustered into three major themes based on similarities.
Results
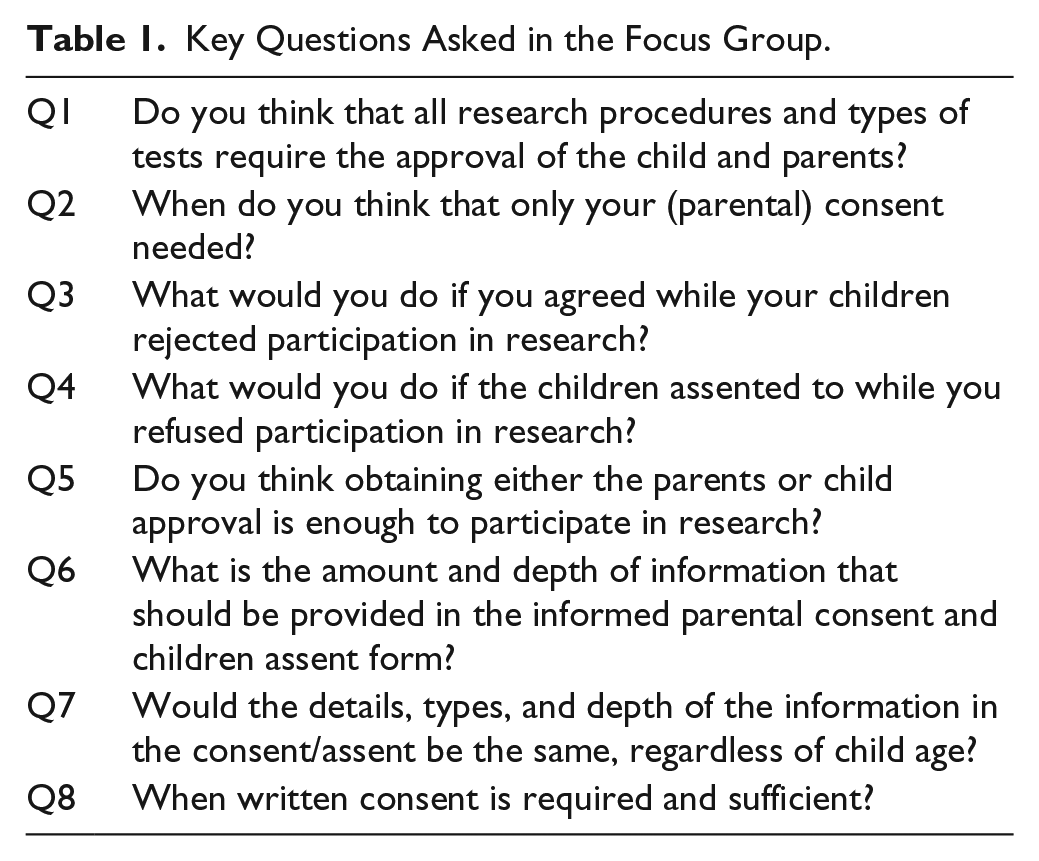
In this study, the focus groups used three predetermined domains to explore parents’ perceptions and understanding of informed parental consent and child assent in pediatric and adolescent research. Table 1 shows the questions/domains asked to the parents. Deliberation continued until a saturation stage was reached, in which repetition of the same themes occurred for each domain.
Key Questions Asked in the Focus Group.
Theme 1: Parent Versus Child Approval to Participate
The parents were asked, “Do you think that all research procedures and types of tests require the approval of the child and parents?”
A majority of the parents emphasized and agreed on the importance of seeking parental and child approval during pediatric research. Some mothers, however, indicated that parental approval is not essential for noninvasive procedures, such as questionnaires, weight and height analysis, and interviews. In addition, one father emphasized that obtaining the father’s consent is pivotal and that it should be required for pediatric research that involves invasive procedures, such as blood withdrawal, and for providing sensitive information, such as the disease history of the family.
The parents were asked, “What do you think we should do when parental approval was obtained while the child refused to participate?”
All parents agreed upon acknowledging and complying with the child’s decision, though they would try to convince them to participate, especially if the study/procedure is deemed beneficial for the child. The parents, however, debated the age at which they would give “full” opportunity to the child to decide without forcing him or her. The parents indicated that 9 years seemed to be the age at which the child can make “conscious” decisions. In addition, half of the mothers and one father agreed that they would persuade the child to participate. On the contrary, most fathers and about half of the mothers said that they would force their young child using their power, including threatening them.
One father said, “The decision of the ones who are above 9 years old should be respected but that the ones under 9 years old have no right to refuse. Those under 9 years should be forced, even threatened to participate.”
They were then asked, “What do you think we should do when parental approval was not obtained while the child agreed to participate?”
All mothers agreed that the child should not participate in the study if the parents disapprove of the child’s enrollment. They also indicated that the researchers will bear all the responsibility if they involve children in a study without parental consent. The fathers had varying opinions. Some fathers agreed with the mothers that the child should not participate in the study if the parents disapprove of the child’s enrollment. On the contrary, some said that parents should convince the child not to participate, while others suggested that if the child insisted and wanted to participate, then the parents should respect the child’s decision, especially if the child is mature enough. Some fathers said opening discussion channels would be better, since some of the children might enroll without informing the parents.
One mother said,
If I refused and my child wants to participate, he might do it without telling me. In this case, it is better to let him participate, especially if he is mature enough. Either I convince him, or he convinces me. The opinion of the child is very important . . . it’s his right.
Another mother said,
It’s absolutely unacceptable to enroll the child in the study while I am refusing . . . It’s the researcher’s responsibility not to enroll the child if the parents aren’t consented, even if the child is 15 or even 20 years old.
Theme 2: Depth of Information in the Consent and Assent Forms
The parents were asked, “What do you think of the extent of the information/content and the depth of the details that need to be provided in the consent/assent forms?”
The thematic analyses showed that all parents believed that the consent/assent should include detailed information about the research topic, such as possible benefits and harms, aims of the project, research team qualifications, and researcher contact information.
When they were asked whether oral consent was sufficient to replace written consent, all mothers believed that oral consent is sufficient when the study involves a questionnaire/survey or when the procedure in the research study is noninvasive, such as body weight and height, if enough details about the study are given. The majority of the mothers, however, stressed the need for written consent in studies that require taking human samples, such as blood. They also indicated that written consent is preferred in all types of studies, as it is safer for all, the researcher, child, and parents.
One mother said, “general procedures don’t usually need our consent . . . I only expect my child to ask for my permission if the research requires things like blood samples, etc . . . ”
Theme 3: Age Required to Provide Child Assent
The parents were asked, “Beside parental consent, in your opinion, what is the age of the child that you think is appropriate to provide adequate information to the child, and thus, the child can provide assent?”
The parents, especially the fathers, debated the age issue at different phases of the interviews. Parents from both genders believed that assent should be taken from all children irrespective of age; however, they disagreed on whether to force the child or to respect the child’s opinion about their participation in research, especially if the procedure/study was deemed beneficial for the child. Some indicated that children should be assented if they are 15 to 16 years or older, whereas one father said 18 years is the appropriate time to ask for the child’s assent. Some parents asserted that parental consent and child assent should both be considered when the research can potentially cause harm to the child; however, if there is no perceived harm to the child, then parental consent is enough.
One father said: “I guess, 15 or 16 is the age where the child can make his own decisions . . . ” One mother said: “it depends on the procedure of the study . . . I mean, if it’s important, then I’ll use all possible ways to convince my child to participate . . . ” One mother said: “if the study involves no harm, then I can make the decision on behalf of my child regardless of his age . . . ”
Discussion
In this study, we investigated parental perceptions of the informed consent process in pediatric research. Overall, the majority of parents have an ethically acceptable understanding of many of the aspects related to parental consent and child assent in research studies; however, some views were not consistent with the proper conduct of pediatric research and, thus, require further attention and actions.
The informed consent process in pediatric research is essential, as it reflects respect to individuals and to protect the participating children from all possible harm that could be caused by their enrollment in the research (De Lourdes Levy et al., 2003; Ngui et al., 2014).
The majority of the parents stressed the importance of obtaining parental consent and child assent in all types of pediatric research; however, some of the mothers mentioned that parents’ consent is not important for studies that involve only questionnaires and interviews. In addition, one father said that father consent is the one that should be required. The belief, by some mothers, that the questionnaire and interview studies do not require parents’ consent may be based on the assumption that such studies will not expose the child to any harm. Questionnaire and interview studies may cause harm to children in several ways, including the violation of privacy through the collection of data about socially questionable behaviors. In addition, there might be legal risks associated with collecting data related to illegal behaviors, and questions that raise sensitive issues may cause psychosocial stress to the participants that might extend to the child’s family members (Allmark, 2002). In addition, parents’ consent is very important to neutralize the unbalanced power relationships between the adult researcher and child participant, preventing children’s potential vulnerability to misuse, while interacting with adult researchers (Edwards & McNamee, 2005).
In some countries, regulations allow for the consent of only one parent for lower-risk studies. Other countries have provisions for a waiver of informed consent by the IRBs for some low-risk studies, such as questionnaires. In this case, assent would not be required. Moreover, in some instances child disagreement may be overridden irrespective of age, especially if the child is not capable of providing assent or when no treatment is available except one that is only available through a clinical study (Joseph, Craig, & Caldwell, 2015; Rose & Kummer, 2015). The opinion of one father (one out of eight) that father consent is the one that should be required might reflect male dominancy in Arabic culture (Abdul Salam et al., 2015). According to Islamic Fatwas (which is a learned interpretation that a qualified jurist can give on issues relating to the Islamic law), getting parental/guardian informed consent is required prior to conducting any research on children (Alahmad & Dierickx, 2015). Thus, waiving informed consent/child assent might be a sensitive issue in Jordanian culture. The IRB committees should consider this when approving research proposals. In addition, if an IRB approved a waiver of informed consent for some studies, then every effort should be made by researchers to respect the parents’ involvement in such studies.
With respect to the child’s assent, most parents agreed that they would respect the adolescent’s decision if he or she refused to participate, even if the parents’ consent was obtained. The parents, however, were divided, as some of them said they will try to convince them or even to force them to participate. The latter opinion contradicts the respect of person principle and voluntary participation in research. The participants even have the right to withdraw from the study at any time. In Arabic culture, it is considered inappropriate to disagree or to oppose the parents’ opinion, especially in public. In addition, the Islamic religion asked the descendants to respect the parents’ decisions and to obey them in all aspects, except if it is against Sharia (Islamic law; Al-Mateen, 2004; Dhami & Sheikh, 2000). In addition, none of the Fatwas about inclusion of children in research has mentioned anything about child’s assent (Alahmad & Dierickx, 2015). These discussed factors may have contributed to the opinion by some parents to force their children to participate in pediatric research.
Discrepancies in the opinions of parents regarding the appropriate age of a child to assent was observed, and an age range of up to 18 years was suggested. In Jordan, the legal age of adulthood is 18 years; thus, individuals below 18 years are considered minors and legal control over their persons, actions, and decisions are assumed by their parents/guardians (Jordanian Civil Law, 1976, p. 43). The discrepancy reflects the parents’ personal opinions regarding the age at which the child can understand research procedures, benefits, and risks, and thereby make decisions. While the appropriate age of child’s assent is still under debate (Davidson & O’Brien, 2009; Hein et al., 2015; John, Hope, Savulescu, Stein, & Pollard, 2008; Kuther & Posada, 2004), according to U.S. regulations, “adequate provisions are made for soliciting the assent of the children, when in the judgment of the IRB, the children are capable of providing assent, in taking into account the ages, maturity, and psychological state of the children involved” (45 CFR 46.408). In addition, in most regulations, irrespective of age, assent is not required from children who are deemed incapable of providing it (Joseph et al., 2015; Rose & Kummer, 2015).
The study showed that the parents have good perspectives regarding the information that should be provided during the informed consent/assent process. All parents agreed that detailed information about the topic, including the benefits and possible harms, aims of the project, and research team qualifications and detailed contact information, should be provided. Previous studies have shown that providing enough clear information about the benefits, risks, and study procedures increased parental satisfaction (Kupst, Patenaude, Walco, & Sterling, 2003; Steven, Broadis, Carachi, & Brindley, 2008; Stolt, Helgesson, Liss, Svensson, & Ludvigsson, 2005) and enhanced enrollments of children in pediatric research, to include clinical studies (Bernhardt, Tambor, Fraser, Wissow, & Geller, 2003; Boccia, Campbell, Goldman, & Skinner, 2009; Eder, Yamokoski, Wittmann, & Kodish, 2007; van Stuijvenberg et al., 1998). It is strongly recommended that more studies be conducted on this aspect to evaluate the quality of the provided information and informed consent procedures when conducting pediatric and other types of research in Jordan and the Arabic region.
One might argue that the lack of consensus shown in the data reflects the disagreement in the literature, thus raising challenges for the development of ethical guidelines for pediatric research in Jordan. Notably, having regulatory guidelines is essential for the researchers/IRB to approve the proposed pediatric research before it is presented to the parents. In our opinion, the discrepancy in the parents’ opinions about the consent process in pediatric research highlights the need for regulations regarding the protection of the rights and welfare of children in Jordan. Such regulations should take into consideration the cultural, religious, and educational circumstances in Jordan.
Because the focus groups were conducted in Irbid, Jordan, one might argue that the results are appropriate only for local application; however, given the religious, language, and cultural similarities throughout the country, we believe the current findings can be generalized to all of Jordan. It is worth noting here that the parents were recruited via the schools, and the focus groups were conducted in the schools. Thus, we believe that the parents’ opinions might reflect only children who are in schools (in Jordan, this means an age of 6 and above). In addition, investigating the opinion of parents who experienced enrollment in research themselves, or parents who have enrolled their children in previous research, is interesting and will add more dimensions to the current findings.
Conclusion
In conclusion, many of the opinions of parents in Jordan with respect to informed consent/assent were in agreement with international ethical guidelines; however, some opinions were not acceptable, as they were inconsistent with the proper conduct of research and, thus, require further actions. The discrepancies in some of the parents’ opinions could reflect local culture, religion, and personal factors. Thus, the development of national, culturally sensitive guidelines that regulate the conduct of research in Jordan is needed.
Best Practices
Protecting children rights and welfare is the core of informed consent/assent process during participation in pediatric research; thus, adhering to ethical guidelines is essential in this process. In developing countries such as Jordan, adhering to best practices of child and adolescent research is challenged by cultural norms, and the lack of existing relevant guidelines and regulations. Therefore, adequate training of the research team on responsible conduct of research will significantly limit misconduct in pediatric research. In this regard, the local IRBs can play a central role.
Research Agenda
An evaluation of the quality of the provided information and informed consent procedures during the conduct of pediatric and other types of research in Jordan and the Arabic region is recommended. More research is also required to elucidate parent’s perspectives on other aspects of research, such as privacy, confidentiality, data sharing, incidental findings, and recruitment. It is also important to study children’s perspectives on these issues. Such studies might help in balancing culture and standard ethical codes in a comprehensive guideline that promotes the responsible conduct of research in this country.
Educational Implications
The inconsistency between some of the parents’ opinions with the proper conduct of research suggests the need for educational programs to enhance the knowledge of the population about the importance of consent/assent in research. Because such inconsistencies could reflect the local culture and religion, the development of national, culturally sensitive guidelines that regulate the conduct of research in Jordan is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Grant 5R25TW010026-02 from the Fogarty International Center of the U.S. National Institutes of Health.