
Abstract
There is limited literature on the opinions and perspectives of researchers on the ethical issues in biobank research in South Africa. This study aimed to explore researchers’ perspectives on informed consent and ethical review of biobank research in South Africa. An online survey was conducted among researchers and scientists at Stellenbosch University and the University of Kwazulu-Natal. The majority of researchers opined that broad consent is appropriate for biobank research. However, there was no consensus on the necessity for re-consent. Researchers were also in agreement that issues concerning informed consent and future use of samples require thorough discussions during the ethical review process. Overall, the attitude of researchers on informed consent and ethical review of biobank research was positive and ethically informed.
Background
Research is needed in Africa to address the numerous health challenges confronting the continent (Boatin et al., 2012; Sylla & Wild, 2012). This need for research has made the use of human biological materials (HBM) such as tissue, organs, blood and genetic material/data for biomedical research, an area of high interest to researchers, bioethicists, philosophers, lawyers, and various regulatory bodies (Hansson, 2009). In this era of globalization, there are profound ethical, legal, and societal issues (ELSI) for the evolving nature of this research. Stakeholders in research involving human specimen resource repositories (biobanks) face several challenges in ethical review and informed consent processes especially in Africa where it is an emerging field. Over the years, several allegations of breach of biobank governance norms and standards by researchers from developed countries have been highlighted in literature (Emanuel, Wendler, Killen, & Grady, 2004; Emerson, Singer, & Upshur, 2011; Mello & Wolf, 2010; Mudur, 2002; Upshur, Lavery, & Tindana, 2007; Zhang et al., 2010). In addition, large quantities of HBM whose fate is unknown have been shipped from low resource countries to developed countries (Staunton & Moodley, 2013). This has partially been attributed to weak regulatory systems (Whitney et al., 2008). Studies show that guidelines regulating the acquisition, storage, use, and transfer of HBM in several African countries are inadequate, conflicting, and at worst nonexistent (Sathar & Dhai, 2012; Staunton & Moodley, 2013).
Studies on the attitudes of researchers regarding the informed consent process have drawn mixed reactions. Whereas some researchers are highly critical of research ethical review systems, others are appreciative, especially concerning the protection of human participants (Whitney et al., 2008). Previous studies in South Africa (SA) have reported nonadherence of researchers and sponsors from developed countries to ethical guidelines with regard to the acquisition and use of HBM in international collaborative research (Sathar, Dhai, & van der Linde, 2013). There is limited literature on the opinions and perspectives of researchers and scientists on the ethical issues in biobank research in SA (Moodley & Singh, 2016). Therefore, as a prelude to streamlining of biobank activities in the country, there is need to obtain the views and perspectives of the various stakeholders in the biobanking industry.
Although the first biobank in SA (Africa Centre for Health and Population Studies) was established more than two decades ago, it is only in the last few years that research-involving biobanks has gained prominence. The number of biobanks in SA is growing and so are the ethical challenges associated with biobank governance. If biobank research is to succeed in SA and Africa as a whole, it has to be embraced and appreciated by all stakeholders; thus, the need to explore the opinions of the different stakeholders in biobank research. Although a lot of research has been conducted to document research participant perspectives on biobanking (Hansson, Dillner, Bartram, Carlson, & Helgesson, 2006; Igbe & Adebamowo, 2012; Kettis-Lindblad, Ring, Viberth, & Hansson, 2006; Moodley, Sibanda, February, & Rossouw, 2014; Tindana et al., 2012; van Schalkwyk, de Vries, & Moodley, 2012; Wendler et al., 2005), not much has been done to document other stakeholders’ experiences and perspectives concerning informed consent and the ethical review process in this field of research (Cambon-Thomsen, Rial-Sebbag, & Knoppers, 2007). Scientists manage biobanks and are the end users of HBM and thus are important resources with vital information on biobank functioning. They play a vital role in the informed consent process and offer an invaluable and necessary viewpoint that should help to inform consent policy (Master, Campo-Engelstein, & Caulfield, 2015). Most of the empirical research in this area has been conducted in high-income countries with limited contribution from sub-Saharan Africa. This study, therefore, set out to explore researchers’ perspectives on some of these issues, particularly, informed consent and ethical review of research involving human resource repositories (hereafter referred to as biobanks) in SA.
For the scope of this study, pathological archives and institutional professional laboratories where HBM from research activities (e.g., clinical trials) are stored were also considered as biobanks. “Researchers” denoted investigators, scientists, clinicians, pathologists, laboratory or repository personnel, and managers who design and implement biomedical research.
Method
This was a cross-sectional study that was carried out between June 2015 and January 2016 at Stellenbosch University (SU), the University of KwaZulu-Natal (UKZN), and UKZN-affiliated research institutions such as the Centre for the Aids Programme of Research in South Africa (CAPRISA), the Africa Centre for Health and Population Studies, and the KwaZulu-Natal Research Institute for Tuberculosis and HIV (K-RITH). The estimated sample size was 142 basing on the assumption that 50% of respondents would be well conversant with ethical issues in biobank research, as there had been no previous web-based research on this topic in SA. This sample size was calculated using Open Source Epidemiologic Statistics for Public Health (OpenEpi; n.d.), an online sample size estimator basing on an estimated population of 1,000 researchers at both Universities, a design effect of one for a power of 80%. The survey was distributed to more than 400 individuals so as to maximize responses. At UKZN, the names and e-mail contacts of potential respondents were obtained from the respective official institutional websites, and a list of 396 members was generated. Invitation e-mails were sent to all members on the list. At SU, no list was generated; instead, the link to the surveys was included in a weekly e-mail newsletter, impromptu, that is distributed to all staff members; and this was done consecutively for 1 month.
Data were collected using an online self-administered survey instrument that was developed from several studies in literature that reported on the perspectives of researchers and research ethics committee (REC) professionals (Edwards et al., 2011; Edwards et al., 2012; Lemke et al., 2010) (available in the supplimental material). The survey instrument comprised different types of response categories that varied based on the questions and included yes/no/uncertain options, Likert-type scales (e.g., 5-point scales rating agreement with a sixth “don’t know” option), categorical responses, and open-ended questions. The instrument covered four general topic areas: demographic information, REC review process, informed consent (both for adults and minors < 18 years), and human participants’ protection. Open-ended questions facilitated in-depth probing for further information. Data scales (Likert, 1932) were used to determine attitudes and perspectives, whereas the open-ended questions were used to acquire more in-depth information about challenges to ethical review of biobank research and sample/data sharing. The instrument was pretested and adjusted accordingly to ensure that all questions were clear and understandable. Internal consistency and reliability were ensured by item analysis of the questionnaire during pretesting. Respondents included clinicians, researchers, pathologists, and laboratory or biobank managers who were purposively selected. Selection was based on active participation in biomedical research and/or health care. The survey was distributed to researchers using online survey programs. An invitation e-mail was sent to all potential respondents. Included in the mail was a brief introduction of the investigators, the sponsor, a summary of the purpose of the study, links to the informed consent form and the survey, and a description of the confidentiality policy. The survey was distributed using LimeSurvey® and SurveyMonkey® online programs. Completion of the survey implied consent, and the study was conducted according to the principles outlined in the Declaration of Helsinki. Responses were anonymous and delinked from e-mail addresses. On average, five reminders were sent.
Ethical approval was obtained from UKZN BREC (BE412/14) and SU Health Research REC (S15/04/076); administrative clearance was obtained from all institutions.
Descriptive summary statistics were used to summarize the data. For each Likert-type scale, five categories were collapsed into three, combining “strongly agree/somewhat agree/very likely/somewhat likely,” “neutral and don’t know,” and strongly disagree/somewhat disagree/very unlikely/somewhat unlikely.” This was done to facilitate analysis and interpretation. The two-sample t test was used to assess differences in opinions between respondents who had ever participated in biobank-related research and those who had not. A p value of <.05 was considered significant. In this article, we present results of the closed-ended survey.
Results
Participant Characteristics
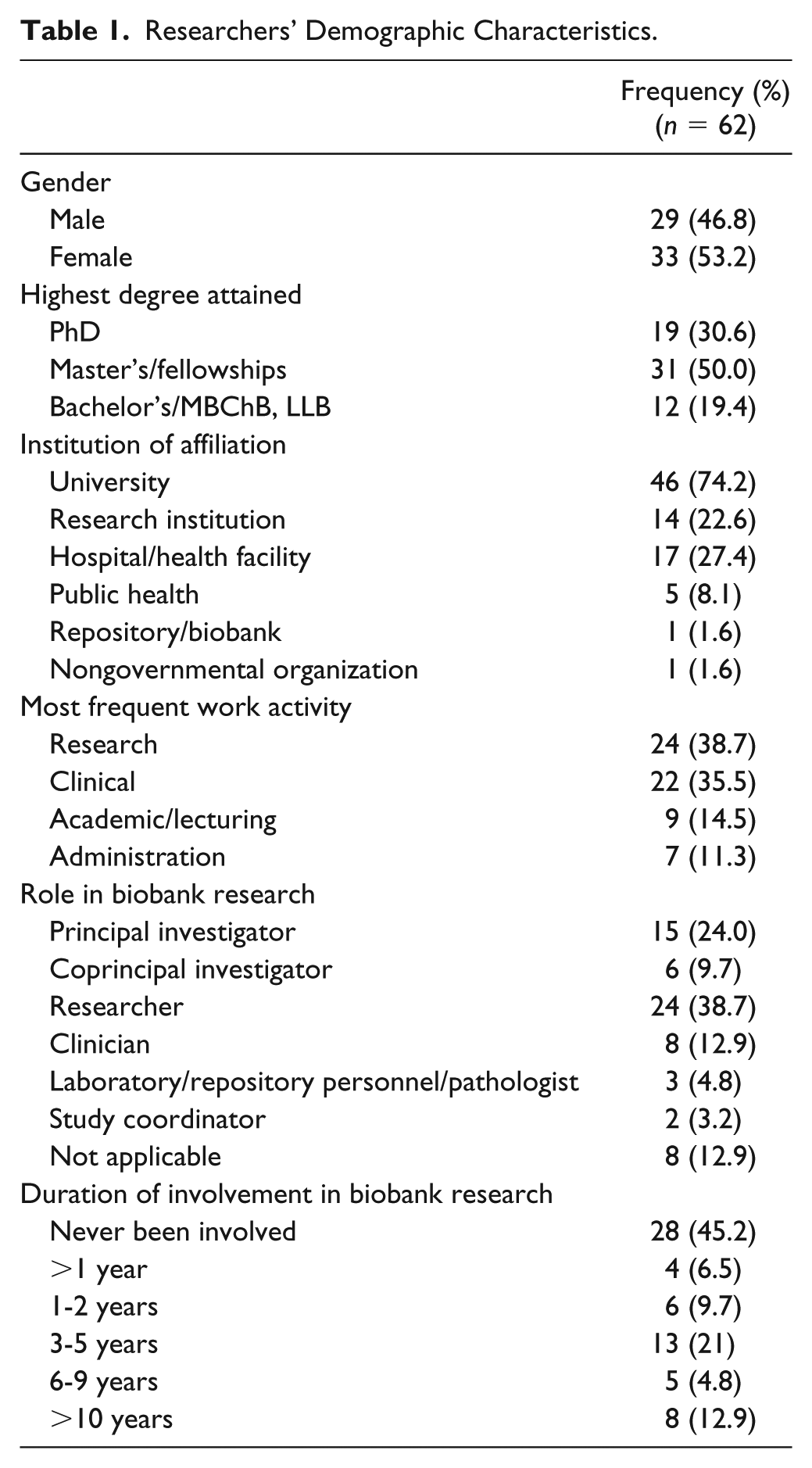
Sixty-two individuals responded and completed the survey. The response rate could not be calculated as the exact number of researchers who had access to the survey link is not known. Slightly more than half of respondents were female (53.2%) and a majority (80.6%) had at least attained a master’s degree or fellowship. More than half of respondents (58.1%) had ever participated in research involving the collection, storage, and future use of HBM. Participant characteristics are summarized in Table 1.
Researchers’ Demographic Characteristics.
Perspectives on the Consent Process
Respondents were asked for their opinion on the acceptability of broad consent and general consent for biobank research compared with specific consent (Table 2). General or “blanket” consent was defined as the consent given by participants at the time of sample collection for the use of their samples in any and all future studies, with no restrictions on the purpose of the research. Broad consent was defined as the consent given by participants at the time of sample collection for the use of their samples in the current study and a wide range of future research studies based on a broad category, such as HIV research or cancer research. Only 66.1% agreed that broad consent is permissible, while 61.3% opined that general consent should only be acceptable when samples are anonymous. There was no difference in opinion between respondents who had ever participated in biobank-related research and those who had not (p = .38).
Researchers’ Perspectives on the Type of Consent Applicable to Biobank Research.
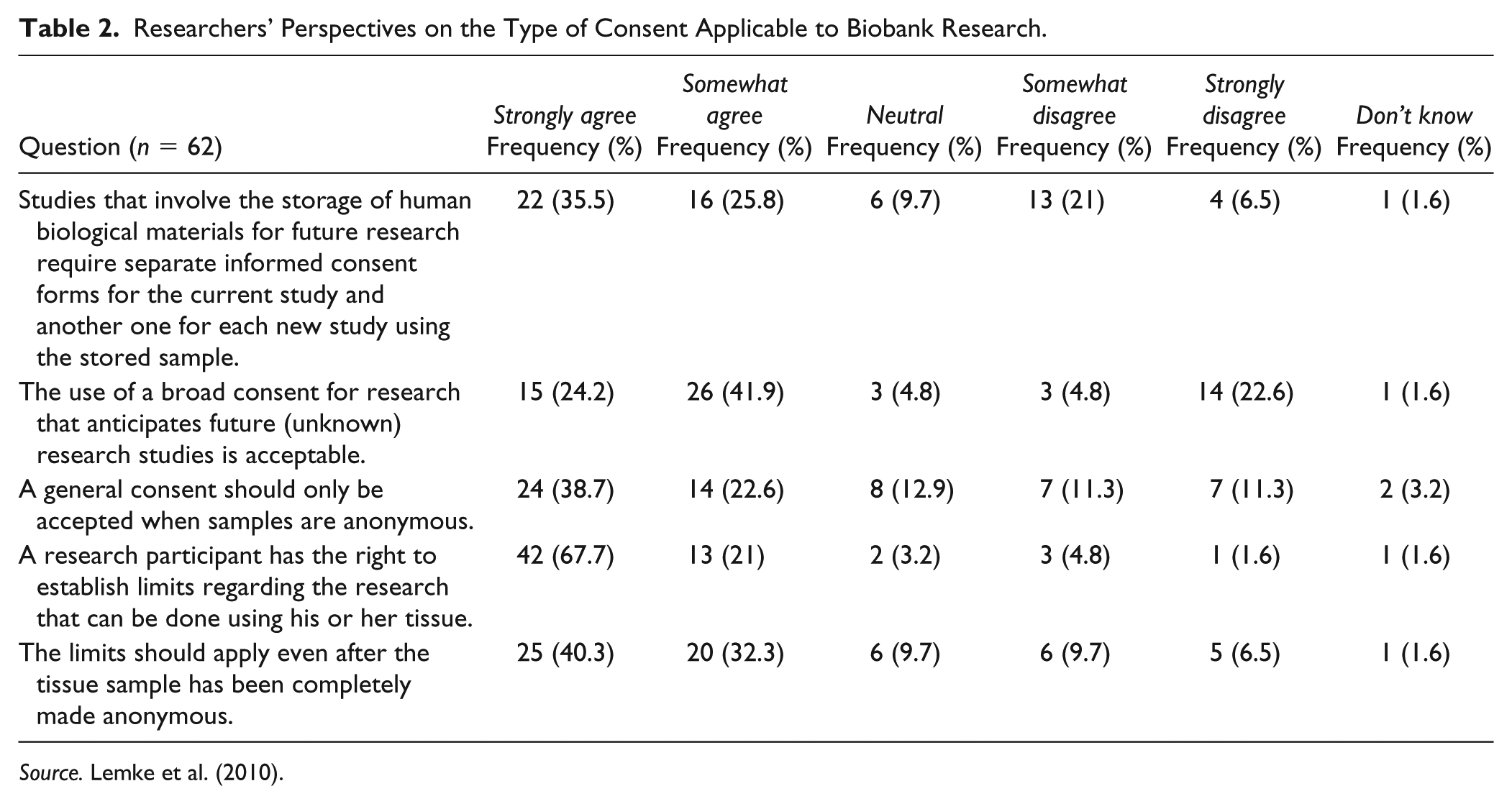
Source. Lemke et al. (2010).
Respondents were also asked to rate their level of agreement with regard to informed consent and assent for minor participants. A large majority (83.9%) believed that parental consent is sufficient for storage of biological samples for genetic research of any child who cannot assent because he or she cannot understand the nature of research. However, an overwhelming majority (92%) opined that children should be given the opportunity to assent once they are in position to understand the implications of HBM storage and genetic research. The same majority (92%) were also of the view that young participants should be given the right to withdraw their biological specimens/data when they reach 18 years of age (Table 3). Further inquiry was made on the age at which children are able to understand the implications of genetic research and the storage of HBM for this type of studies. Slightly less than half of the respondents (45.2%) thought that children are able to understand the implications of sample storage for future use. The age range is 16 to 18 years for storage of HBM for future genetic research. Whereas half of the respondents (50%) thought that children are able to understand the implications of genetic research at 16 to 18 years of age. There was no significant difference in opinion between respondents who had ever participated in biobank research and those who had not (p = .57).
Opinions on Re-Consent of Research Participant and Consent/Assent of Minors in Research.
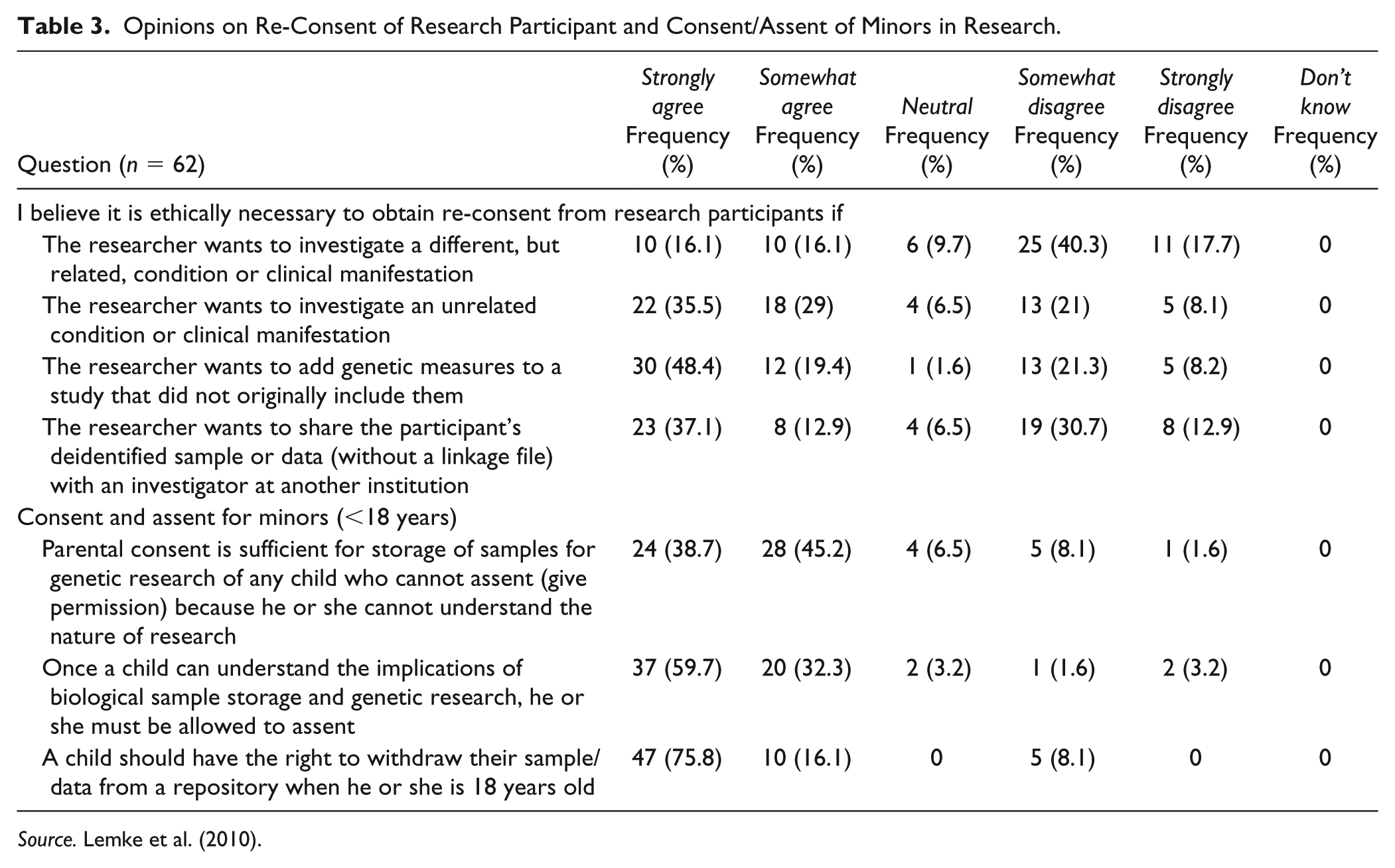
Source. Lemke et al. (2010).
There were varying views on the ethical necessity to obtain re-consent for the secondary use of HBM. A majority of respondents agreed that re-consent is an ethical obligation in a number of scenarios: (a) if the researcher wants to investigate an unrelated condition or clinical manifestation (64.5%) or (b) if the researcher wants to add genetic measures to a study that did not originally include them (67.7%). Conversely, 58% believed that it is unnecessary to obtain re-consent if the researcher wants to investigate a different but related condition or clinical manifestation. Respondents were evenly split with respect to whether it is necessary to obtain re-consent if the researcher wants to share the participant’s deidentified sample or data (without a linkage file) with an investigator at another institution (Table 3). Eighty-two percent indicated that REC approval would suffice in cases where re-consent of participants is not possible.
Perspectives on Ethical Review and Regulation of Biobank Research
Respondents were asked for their views on the storage and use of HBM for future research. A majority (67.8%) agreed that the use of coded HBM constitutes human participant research (when the researcher does not have access to the link between identifiers and biological samples). Seventy-nine percent agreed that storage of HBM and data for future genetic studies is acceptable as long as the samples are anonymized.
To learn more about researchers’ exchanges with RECs, respondents were asked to identify the issues that necessitate “considerable discussion” between researchers and their REC in the review of applications involving the future use of HBM. Considerable discussion was defined as “more than two or three back-and-forth rounds and/or more than a one-hour conversation.” A majority (66.1%) indicated that issues concerning re-consent for use of sample/data for a new study or change in the study objectives cause considerable discussion. Other issues that often resulted in requests from RECs for additional information or clarification included procedures for protecting participants’ personal information or samples (56.5%), informed consent process and documentation (56.5%), the need for additional ethical review of new studies on stored samples (45.1%), and plans, or lack of plans, to deal with community harms or benefits (35.5%).
Questions were also asked on the control research participants should have on the use of their donated samples. A majority (88.7%) opined that research participants have the right to establish limits regarding the research that can be done using their tissues, while 45 respondents (72.6%) agreed that the limits should apply even after tissue samples have been completely made anonymous (Table 2).
Discussion
This study set out to explore researchers’ perspectives on informed consent and ethics review of research involving human specimen resource repositories/biobanks in SA. Overall, the attitude of researchers on the need for participant informed consent and ethical review of biobank research was positive, ethically informed, and had several areas of agreement.
Ethical Review and the Protection of Research Participants
Researchers were in agreement that issues concerning informed consent documentation, sample deidentification, and re-consent for the use of HBM and associated data or change in purpose require thorough discussions during the ethics review process. However, only 36% felt that having provisions for dealing with community harms or benefits requires considerable discussion. This seems to reiterate Emanuel, Wendler, and Grady’s (2000) observation that existing ethical regulatory policies and guidelines emphasize immediate risks to the individual and tend to ignore potential harms to those not participating in research. Researchers must recognize and appreciate that the risks of biobank research can affect the general community; and should, therefore, ensure that measures are put in place to protect the community. RECs also must critically evaluate biobank studies for the likelihood of psychological, social, or physical risks to individual participants, groups, or the community (Emanuel, Crouch, Arras, Moreno, & Grady, 2003). The perceived lack of emphasis in this study on community risk/benefit assessment during ethics review discussions calls for enhanced awareness among researchers and REC members regarding the importance of ensuring adequate stakeholder and community engagement strategies in the context of biobank research, so that communities are given an opportunity to be active players in both determining appropriate research agendas and identifying potential community harms. Although physical harm is rare, possible risks may not only affect the individual, but also involve the society to which participants are associated. There also is the risk of identifying individuals and population groups (Hansson, 2005). The risks are usually social and dignitary (Sharp & Foster, 2002; Van Assche, Gutwirth, & Sterckx, 2013). Among the social risks are stigmatization and genetic discrimination that often affect groups and affect both participants and nonparticipants. Social harm could arise when research findings indicate that certain population groups or ethnic groups are genetically predisposed to certain disease conditions (Hansson, 2011; Rothstein, 2005). Dignitary harms “involve violations of collective rights or disrespectful treatment of the affected community” (Sharp & Foster, 2002, p. 145). For example, improper handling of collected HBM in a way that is perceived as desecrating the values, beliefs, and cultural norms of a population group can constitute dignitary harm not only to the individual participant, but also the entire subpopulation. For this reason, many ethical guidelines advocate for a participatory community-based approach to research through its entire life cycle (Reid, Brief, & LeDrew, 2009). Consideration of potential harm to those not participating in research and socially identifiable societies is a demonstration of respect for social and cultural diversity, and an appreciation that research findings can disrupt harmony within societies.
Applicability of Consent for Biobank Research
There were varying views concerning the most ideal type of consent for biobank research. About 66% of researchers agreed that broad consent was acceptable for biobank research. Globally, consensus is growing on the use of broad consent in biobank research (Denny, Silaigwana, Wassenaar, Bull, & Parker, 2015; Garrett, Dohan, & Koenig, 2015; Grady et al., 2015; Master, Nelson, Murdoch, & Caulfield, 2012; Moodley & Singh, 2016; Rothwell et al., 2015) because it allows donors a degree of control over the use of their HBM in research, while avoiding the potential burden of obtaining re-consent for each new study. Broad consent also provides for participant consent for certain types of future research (Helgesson, 2012; Steinsbekk, Kåre Myskja, & Solberg, 2013; Steinsbekk & Solberg, 2011), review of all new studies utilizing HBM and/or data by an independent REC, an ongoing consent process with the possibility of consent withdrawal at any time, the opportunity to re-consent if anything changes in the framework (Steinsbekk et al., 2013), and allows donors the choice of category of research to contribute samples to (Foe, 2014). Opinions were also obtained on the applicability of general consent for the use of anonymous samples. About 61% of researchers agreed that it is acceptable; however, this type of consent is not recommended by the South African ethical guidelines because it is not easy to implement and contravenes important ethical principles particularly that of respect for autonomy (Republic of South Africa Department of Health [DoH], 2015). Several other studies among scientists have also documented that scientists prefer general consent (Colledge, Persson, Elger, & Shaw, 2014; Master et al., 2015). They justified their choice of preference to the importance of scientific advancement and the practical difficulties of obtaining re-consent. But, there is a possibility that some researchers do not distinguish general from broad consent, as was reported by de Vries et al. (2015) in the proceedings of a workshop with members from 40 RECs from across Africa.
Researchers also opined that it is necessary to obtain re-consent if the proposed new study falls outside the scope of the initial consent or intends to add genetic measures. Such opinions have also been reported by other studies among researchers and REC professionals (Goldenberg et al., 2015; Lemke et al., 2010). Another ethical issue that has aroused a lot of public debate and may require re-consent is the return of results of genetic testing (Botkin et al., 2015; Wolf et al., 2015). Return of individual genomic results is influenced by their clinical utility, interpretation and understanding, access to trained clinicians and genetic counseling services, potential for psychological harm, and potential loss of confidentiality (Ramoni et al., 2013; Ziniel et al., 2014). The ethical and legal implications of genetic testing not only affect the participants or patient as individuals, but also could extend to involve the entire family (Ayuso, Millán, Mancheno, & Dal-Ré, 2013; Borry, Goffin, Nys, & Dierickx, 2008; Botkin et al., 2015; Green et al., 2013; Knoppers, Zawati, & Sénécal, 2015; Ross, Rothstein, & Clayton, 2013; Zawedde-Muyanja et al., 2018). There remains uncertainty on how best to ethically utilize genomic data and how to communicate it to patients and research participants in these settings (Appelbaum et al., 2014; Jarvik et al., 2014). This is an issue of importance that requires further exploration especially with the advent of personalized medicine. Section 32 of the Declaration of Helsinki (The World Medical Association, 2013) delegates to RECs the responsibility of determining whether donors should be recontacted and re-consented for secondary uses of their HBM or return of their genetic results (Sutton et al., 2019), however, should obtaining re-consent be untenable, then the responsibility still is on the REC to make a considered determination on this issue.
Consent/Assent in Research Involving Minors
Perspectives on consent for pediatric research were also obtained. The vast majority of respondents in this study believed that parental consent is sufficient for the storage of HBM for genetic research of any child who cannot assent because of inability to comprehend the nature of research. The need for parental consent and assent for minors is a legal requirement in SA and is consistent with ethics literature (Hens, Cassiman, Nys, & Dierickx, 2011; Master et al., 2015; Petersen, Desmedt, Harris, Buffa, & Kollek, 2014). In SA, the age limit for legal competence for medical treatment is set at 12 years and that for giving informed consent for research at 18 years (South African Child Act 38 of 2005). Pediatric biobank experts recommend ongoing provision of sufficient information to parents and children about the storage and intended use of HBM and associated data in addition to the consequences to the parent and child (Dove, Avard, Black, & Knoppers, 2013; Gurwitz, Fortier, Lunshof, & Knoppers, 2009). This is important because research suggests that parents do not always fully understand all aspects presented during the initial informed consent process (Klima et al., 2013). They tend to overrate individual benefits and underrate the risks associated with their children’s involvement in research (Klima et al., 2013). Other issues that raised unanimous agreement were the necessity to obtain re-consent and the right to withdraw HBM/data on attainment of majority age. Several authors have argued that minor participants must have the choice whether to re-consent or withdraw earlier parental consent on attainment of the age of majority (Brisson, Matsui, Rieder, & Fraser, 2012; Hens, Cassiman, Nys, & Dierickx, 2011; Kranendonk, Ploem, & Hennekam, 2016). This is on the premise that the original proxy consent provided by the parent was made in the best interest of the child, while consent allows the adult child to express his or her own wishes and autonomy (Hens, Levesque, & Dierickx, 2011). Researchers also opined that children be given the chance to assent once they are in position to appreciate the implications of HBM storage and of genetic research. Recontacting mature children is an essential requirement for regulations on biobanking in children (Kranendonk et al., 2016), but the exact age for this requirement should primarily be debated at national level. South African law and ethical guidelines are not clear on this issue, and this should be a source of research and national debate. In the event that recontacting is impracticable or the sample or data are anonymized, an REC should be in position to give guidance basing on national and/or institutional guidelines governing research on human participants.
Sharing/Transfer of HBM
REC oversight for the future use of stored samples helps to guarantee the ethical adequacy and scientific value of such research. Oversight adds further protections because at the time of initial consent, future uses are unknown, cannot be predicted or explained, and participants consent to delegate research institutions and biobanks to make acceptable decisions about secondary research on their behalf (Mongoven & Solomon, 2012). A greater majority of respondents also opined that sample donors have the right to set limits pertaining to the research that can be conducted using their tissues and that those limits should apply even when the samples have been made completely anonymous. Such attitudes are not surprising because over the years, there has been unidirectional export movement of HBM out of Africa to several destinations in the Western world with minimal benefits to the local populace, investigators, and institutions (Staunton & Moodley, 2016). A case in point is a study conducted at a South African institution that exposed major lapses in the regulation of HBM (Sathar et al., 2013). The authors asserted that HBM were leaving SA illegally because 72.2% and 94.7% of protocols reviewed did not have export certificates and MTAs, respectively. In the same study, a majority of researchers neither requested the permission of RECs nor sought the informed consent of research participants to store HBM for future research and export (Langat, 2005; Sathar et al., 2013). Therefore, research regulatory authorities should become more vigilant and ensure that biobank research in SA is adequately monitored. Future research should also be conducted to investigate researchers’ experiences and practices in regard to sample and data sharing in international collaborative research.
The main limitation of the study was the low response rate; however, self-administered e-mail-based surveys have been associated with poor response rates (Burgess, 2001). To try and mitigate this, up to five follow-up e-mails were sent. Results of this study may not be generalizable because the study was conducted at selected academic institutions and the sample size was relatively small. Nonetheless, they give a general overview of the perspectives of researchers that may stimulate inform best practices and stimulate more research in this field.
Conclusion
Generally, the attitudes of researchers on informed consent and ethical review of biobank research were mostly ethically well informed, expressing opinions that were in line with national guidelines. Researchers were unanimously in agreement that issues concerning informed consent are very crucial in biobank research and require considerable discussion during ethical review process. They opined that broad consent is acceptable to biobank research, and research participants should have the right to establish acceptable limits on the utilization of their samples for research. However, there was no consensus on the necessity to obtain re-consent from adult participants in biobank research. Researchers contended that minor research participants should be given the chance to assent once they are in position to appreciate the implications of sample storage and of genetic research. They must also have the choice whether to re-consent or withdraw earlier parental consent on attainment of the age of majority.
Best Practices
The data seem to suggest varying opinions on the type of consent acceptable for biobank research. Some respondents seemed to suggest that general consent was acceptable, for as long as biological samples and associated data are anonymized, which is contrary to the South African ethical guidelines and contravenes important ethical principles particularly that of respect for autonomy (Republic of South Africa DoH, 2015). In addition, only one third of researchers felt that issues concerning plans or lack of plans to deal with community harms or benefits require considerable discussion during ethical review of biobank research. Therefore, RECs should be strengthened to ensure comprehensive research ethical review of biobank research. RECs should also strengthen continuing review and monitoring of approved research. They should be encouraged to make field visits and onsite inspections of research, to ensure that researchers comply with ethical standards.
Research Agenda
More in-depth research should be conducted to explore the perspectives and attitudes of all stakeholders toward biobanking and related research. One area in particular that needs further empirical research regards the attitudes of researchers to obtaining additional ethical approval for new studies once specimens have been deposited in biobanks, especially if researchers will only receive anonymized specimens and data. Future research should also be conducted to investigate researchers’ experiences and practices in regard to sample and data sharing in international collaborative research.
Information from such research may be important in the planning and implementation of continuing professional development activities and could contribute to the harmonization of guidelines for governing biobank research in SA.
Educational Implications
Research and academic institutions, and research regulatory agencies, should organize continuing professional development activities for REC members and researchers, to ensure that they keep abreast with current advances in biobank research and its associated ethical, legal, and social implications.
Supplemental Material
Supplemental – Supplemental material for Researchers’ Perspectives on Informed Consent and Ethical Review of Biobank Research in South Africa: A Cross-Sectional Study
Supplemental material, Supplemental for Researchers’ Perspectives on Informed Consent and Ethical Review of Biobank Research in South Africa: A Cross-Sectional Study by Erisa Mwaka and Lyn Horn in Journal of Empirical Research on Human Research Ethics
Footnotes
Acknowledgements
I would like to acknowledge the effort of my teachers who have imparted on me a wealth of knowledge in my quest to become a leading expert in bioethics. My heartfelt gratitude goes to Professor Douglas Wassenaar and the South African Research Ethics Training Initiative (SARETI) team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this report was supported by the Fogarty International Center of the U.S. National Institutes of Health under award number 3R25TW001599-15 to the South African Research Ethics Training Initiative (SARETI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.