
Abstract
Since their inception, Institutional Review Boards (IRBs) have been charged with protecting the vulnerable in research. More recently, attention has turned to whether IRBs also have a role to play in ensuring representative study samples and promoting the inclusion of historically under-represented groups. These two aims—protecting the vulnerable and including the under-represented—can pull in different directions, given the potential for overlap between the vulnerable and the under-represented. We conducted a pilot, online national survey of IRB Chairs to gauge attitudes and practices with regard to protecting the vulnerable and including the under-represented in research. We found that IRBs extend the concept of vulnerability to different groups across various contexts, are confident that they effectively protect vulnerable individuals in research, and believe that IRBs have a role to play in ensuring representative samples and the inclusion of under-represented groups.
Background
While a need to protect participants from research risk is fundamental to the origins of IRBs and the federal regulatory structures within which they operate, in recent years, both have been criticized by the research community for being overly protective of research participants, poorly calibrating protections with research risk, and introducing unnecessary impediments to research (Assembly, 1996; Baylis & Kaposy, 2010; Beauchamp, 2008; Charo, 1993; Council for International Organization of Medical Sciences, 2017; King, 2005; Koski, 2014; Rhodes, 2010; Sherwin, 2005). This may be partly due to the fact that, in addition to ensuring that individuals provide voluntary consent for research participation, regulations and guidance also require IRBs to determine whether the risks of research are minimized and reasonable in relation to benefits before studies may proceed (45 CFR 46.111; Council for International Organization of Medical Sciences, 2017). IRBs are required to apply even higher thresholds for study approval when research involves groups deemed vulnerable within existing regulatory frameworks. For example, the United States regulations contain additional criteria that must be met before children, pregnant women, or prisoners may be enrolled in research (45 CFR 46, Subparts B, C, D). Furthermore, the regulations instruct IRBs to apply ‘additional safeguards’ for other groups who may be considered vulnerable to coercion or undue influence, including individuals with impaired decision-making capacity and economically or educationally disadvantaged persons (45 CFR 46.111(b)). The content of these ‘additional safeguards’ is left unspecified, creating further potential for over-protective measures from IRBs.
Protectionist IRB tendencies could be due to several sources, such as the rigidity of the regulatory framework or an over-reaction to research scandal and the exploitation of the vulnerable in research in the twentieth century. Whatever its source, a culture of protectionism can be seen as having baleful effects for the inclusion of vulnerable and diverse populations in research. Recently, awareness of the intentional or inadvertent exclusion from research of historically under-represented and understudied populations, especially those viewed as vulnerable to research risk or warranting additional safeguards, has given rise to the suggestion that IRBs may have a role to play in promoting inclusion of certain groups (Bayer & Tadd, 2000; Bierer et al., 2021; Bierer et al., 2020; Caplan & Friesen, 2017; Epstein, 2008; Goldstein & Walensky, 2019; Johnson & Beaudet, 2013; Lau et al., 2008; Oberman & Frader, 2003). These include pediatric populations, older people, women, individuals from communities of color, and individuals with disabilities. Such inclusion efforts stem from recognition of the ethical importance of providing equal access to the short and long term benefits of research, and the scientific value of a more inclusive research enterprise with diverse trial populations that reflect the demographics of the populations affected by the conditions and/or for whom investigational treatments are intended (Strauss et al., 2021).
These two general features of IRBs and IRB review—a protectionist stance toward the vulnerable and the impetus to include under-represented groups—may sometimes pull in different directions. The groups that are often considered vulnerable by IRBs at least sometimes overlap with the groups that have historically been under-represented in research (Friesen et al., 2022). This poses a potential challenge to IRBs, who may be forced to balance the competing goods of protection versus inclusion with respect to certain populations in particular cases.
There has been little systematic inquiry in the academic literature concerning IRB views and practices with regard to these issues. We therefore conducted a pilot, online national survey of IRB Chairs to fill this gap. Specifically, we sought to understand the views of IRB Chairs along three axes. First, we set out to identify the views of IRB Chairs with regard to the concept of ‘vulnerability,’ including relatively fine-grained judgments about which groups count as vulnerable in which contexts and what the regulatory concept of ‘additional safeguards’ might involve across different types of research situations. Second, we sought to understand the views of IRB Chairs with respect to the role of the IRB in ensuring or promoting the inclusion of historically under-represented groups. Finally, we sought to understand how IRBs think about and navigate the potentially competing values of protecting the vulnerable and facilitating the inclusion of under-represented groups, who often overlap with the vulnerable, in clinical research. Our study was descriptive in nature, seeking to understand and document the views of IRB Chairs on this topic without pre-specifying any formal hypotheses for evaluation. The ultimate aim of this work is to identify areas of uncertainty and need across these axes toward which future analysis and guidance can be targeted, in the hopes of improving practice.
Methods
Sample
We identified IRB Chairs through a publicly available file maintained by the US Office for Human Research Protections (OHRP), which was accessed in 2018. This list includes all registered IRBs and rosters of IRB Chairs in the United States and is regarded as “the best available metadata on IRB activity in the United States” (Berry et al., 2019). We chose IRB Chairs as the sample given their proximity to IRB decision-making and our desire to understand actual IRB practices concerning protecting vulnerable populations and ensuring inclusion of under-represented groups. After international, duplicate, and non-functioning email addresses were excluded, the OHRP list yielded 3,014 IRB Chairs to whom the survey was sent.
Survey and Vignette Development, Testing, and Administration
Development of the survey was informed by previous work on diversity in research done by members of the study team in connection with the Multi-Regional Clinical Trials Center of Brigham and Women's Hospital and Harvard (MRCT Center, 2020). Survey content was refined with input from two different groups of senior IRB administrators, the Harvard Catalyst Regulatory Foundations, Ethics, and Law program, and the Consortium to Advance Effective Research Ethics Oversight (AEREO) at the University of Pennsylvania. These groups proved especially useful in helping us to recognize the full complexity of the issues and confirmed our decision to develop three short case-scenarios or vignettes, which varied in potential risks and benefits, as a way of generating more fine-grained and accurate opinions from respondents. Survey questions were further pre-tested with two IRB Chairs for clarity.
The final survey contained 20 main questions, not including demographic questions, and took approximately 20 minutes to complete. The final form of the survey was embedded into RedCap and a consent form and link to the survey was emailed to each of the IRB Chairs on the refined list. The survey was open from September 1 to October 8, 2020, with one reminder email sent during this time. No incentive was offered to respondents. Human subjects/IRB review and approval was granted by the IRB at Massachusetts General Brigham. Responses were exported from RedCap to Microsoft Excel and analysis was conducted using SAS (version 9.4).
Survey Content
In addition to providing standard demographic information (age, sex, gender, race, ethnicity, degree/credentials), respondents were asked to report the number of years they had served on an IRB and the type of IRB to which they belong (university, government, hospital, independent). As we anticipated that some recipients may no longer be active in the role of IRB chair, we also asked about respondents’ current position and relation to the IRB or Human Research Protection Program (HRPP) at their institution.
The first part of the survey asked respondents about their attitudes and perceptions of IRB practices with respect to the notion of vulnerability and research protections. Respondents were asked about their understanding of the concept of ‘vulnerability’; their views on how effectively IRBs protect vulnerable subjects from risk; and whether their IRBs have written policies or procedures regarding what counts as ‘additional safeguards.’ Next, survey respondents were asked to review three hypothetical research studies that differed according to level of risk, benefit, and research aims. Case 1 described a minimal risk interview and focus group study; Case 2 was a greater than minimal risk, placebo-controlled Phase 3 randomized controlled trial with a prospect of direct benefit; and Case 3 was a greater than minimal risk imaging study with no prospect of direct benefit (Table 2). Respondents were asked to identify subject populations that their IRB would consider vulnerable in each hypothetical research study, and identify ‘additional safeguard’ measures that the IRB would take to protect them from research risk.
The second part of the survey focused on the inclusion of historically under-represented groups in research. We asked respondents about the extent to which their IRB seeks to ensure representative study populations with respect to the condition under study, as well as about whether respondents themselves felt this was an important role for IRBs. We then presented respondents with the list of vulnerable populations used in the earlier part of the survey and asked them which groups their IRB affords special attention so that they are not unnecessarily excluded from research, and what measures are taken in this respect. Finally, we asked about the demographic data IRBs review and collect throughout the course of a study.
Results
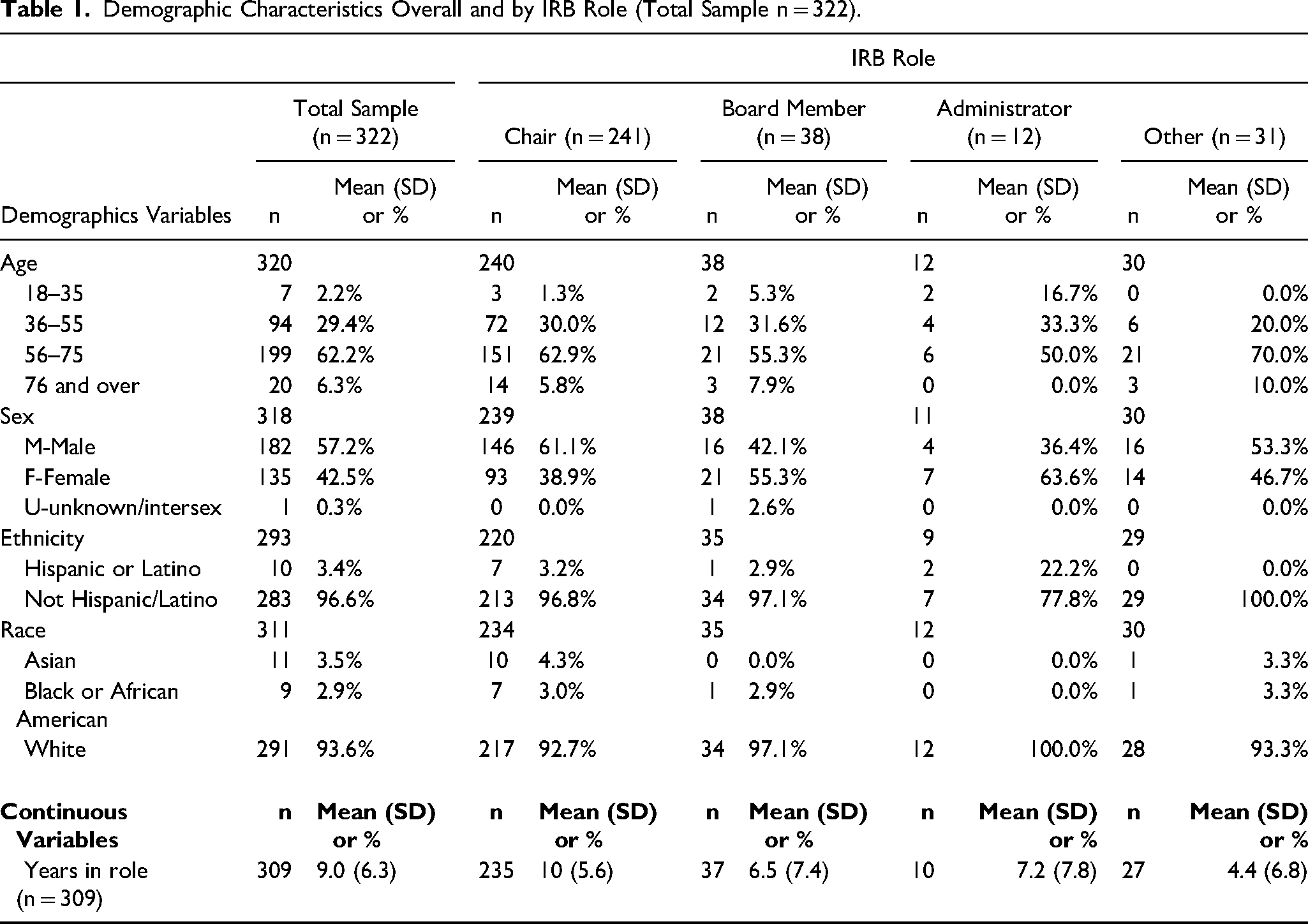
We received 355 survey responses. Thirty-three participants did not respond to any of the survey questions, including demographic ones, and were thus removed from analysis. This left us with 322 completed surveys, for a response rate of 11.1%. 241 respondents were IRB Chairs, 38 were other board members, 12 were IRB administrators, and 31 endorsed “other.” A small number of respondents self-identified as having more than one role. Of the Chairs, 61% of were men; 63% were in the 56–75 years of age; 93% were White, 4% were Asian, and 3% were Black or African American; 3% were Hispanic or Latino (Table 1).
Demographic Characteristics Overall and by IRB Role (Total Sample n = 322).
Vulnerability and Additional Protections
With respect to their understanding of “vulnerable,” 85% of respondents understood the concept to apply to contexts beyond those specified in the regulatory definition—i.e., beyond situations characterized by a risk of “coercion” or “undue influence”—and 52% endorsed all three alternative understandings of “vulnerability” presented (Figure 1). Strikingly, in response to the question of how effectively their IRB protects vulnerable subjects, 74% of respondents indicated their IRB always effectively protects vulnerable subjects and 21% indicated their IRB often did (Figure 2a).
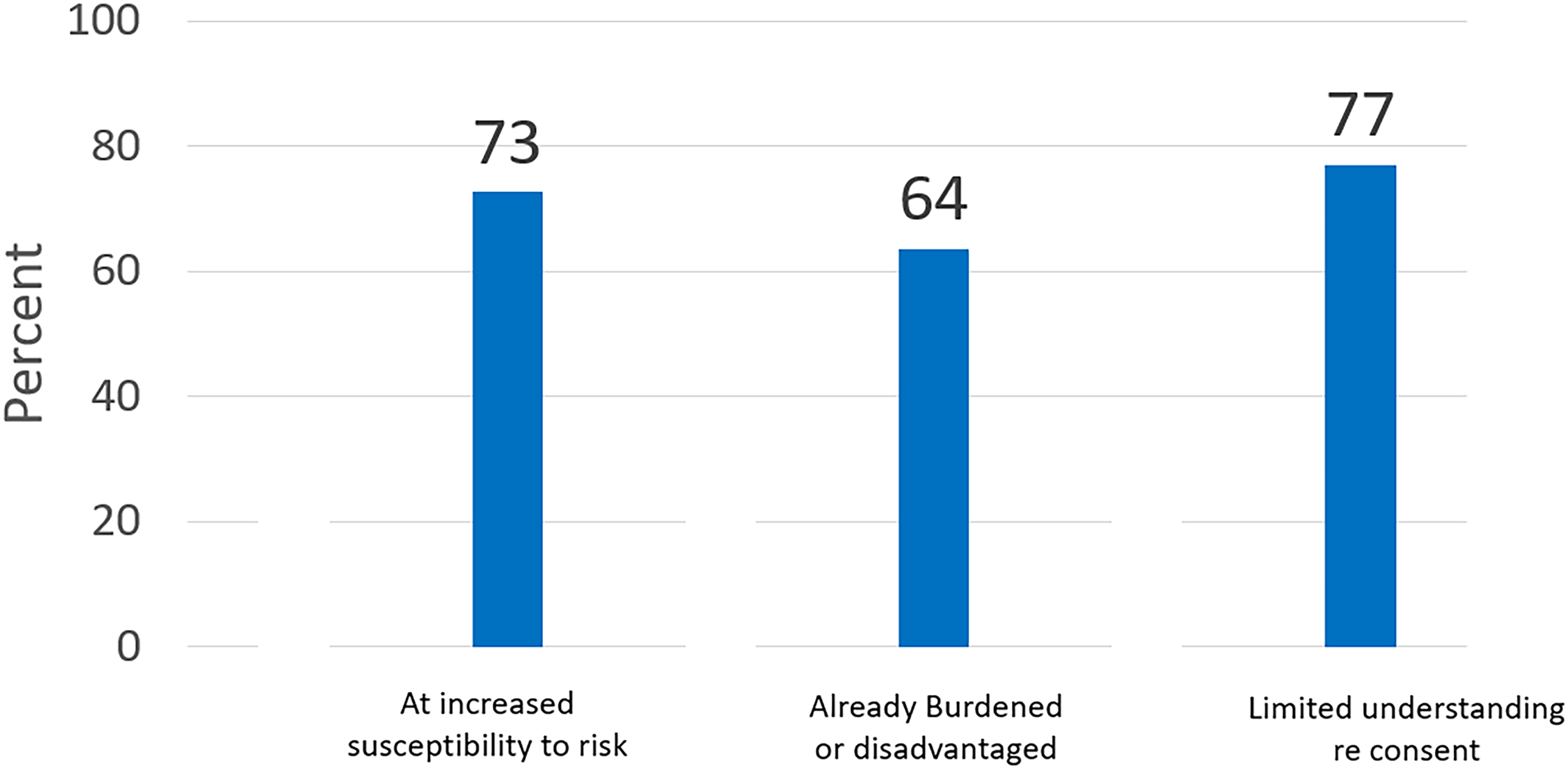
Does your IRB routinely consider any of the following groups to be “vulnerable”?
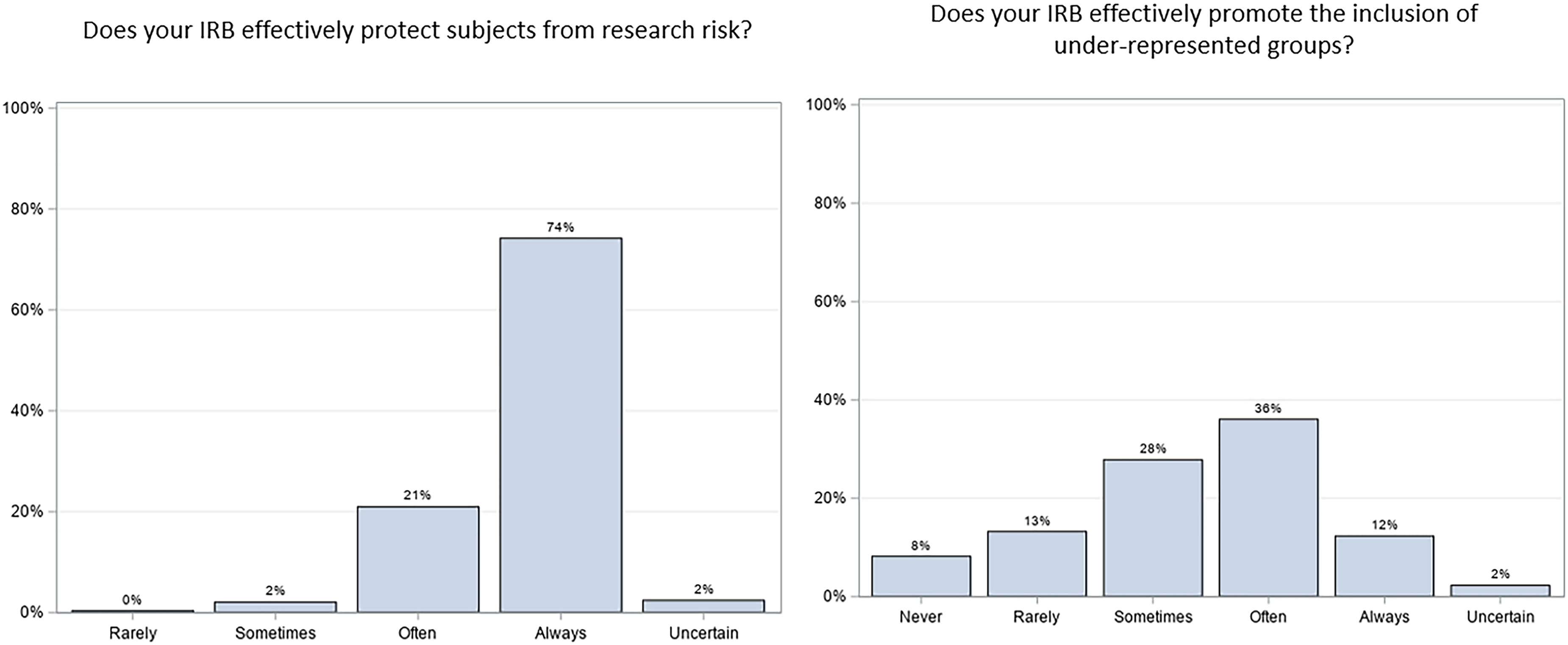
Perception of IRB effectiveness at protection and promoting inclusion.
77% of respondents indicated that their IRBs have written policies or standard operating procedures that guide IRB review or deliberations regarding additional safeguards for vulnerable populations. 56% of respondents indicated that additional guidance delineating measures for identifying and protecting vulnerable groups would be very or extremely helpful. 1
In the hypothetical research study scenarios (Table 2), regardless of level of study risk or benefit, individuals suffering from cognitive impairment and serious mental illness were most frequently considered in need of additional protections. 67% of all respondents felt that cognitively impaired individuals would be vulnerable in the minimal-risk scenario involving a focus group (Case 1), with that falling to 54% in the Phase 3 clinical trial scenario with a prospect of direct benefit (Case 2) and 52% in the higher-risk imaging scenario without a prospect of direct benefit (Case 3). Along similar lines, 48% of all respondents felt that individuals with a serious mental illness would be vulnerable in Case 1, with 35% finding them vulnerable in Case 2 and 40% in Case 3.
Survey Protection Categories by Case.
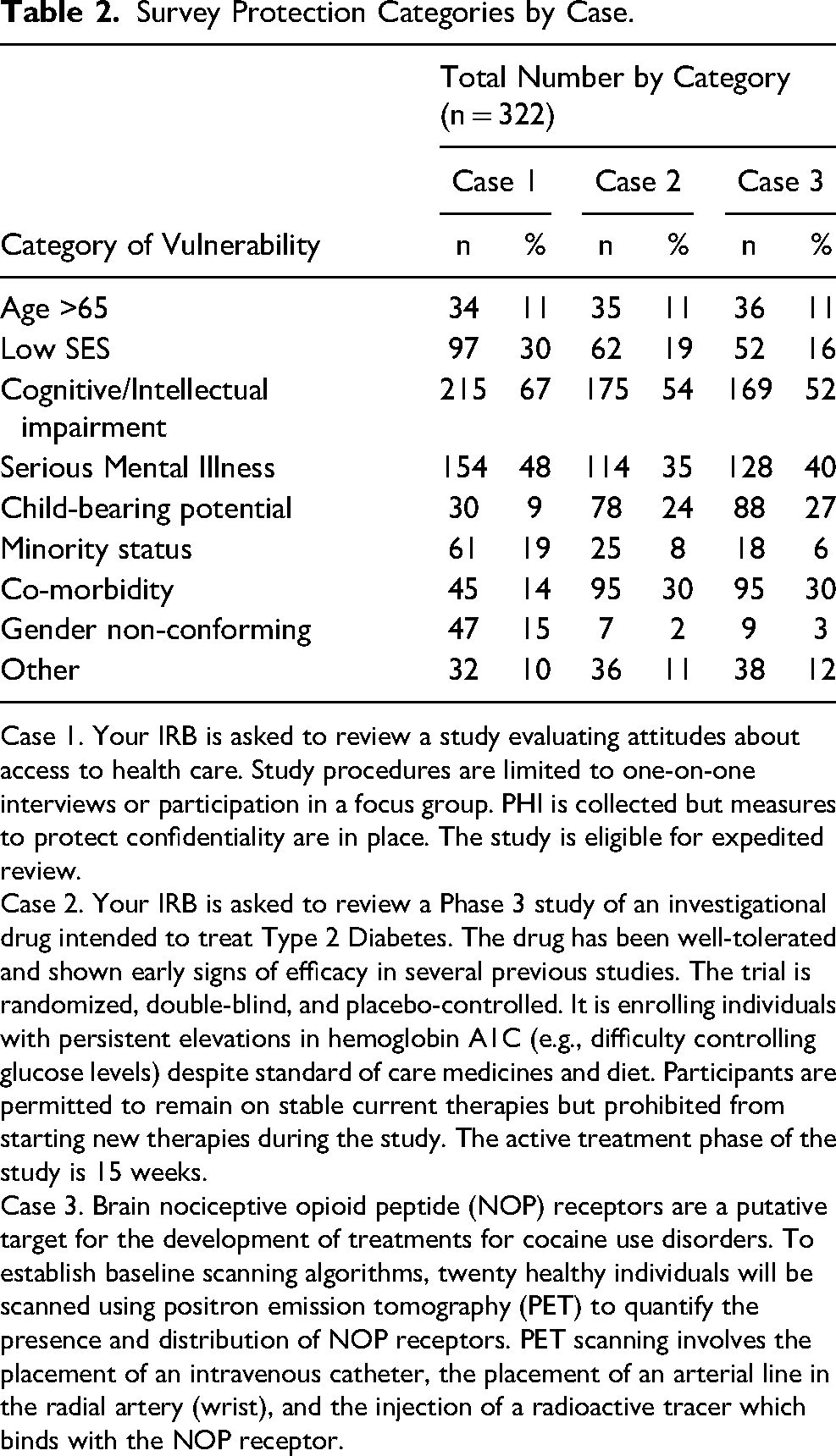
Case 1. Your IRB is asked to review a study evaluating attitudes about access to health care. Study procedures are limited to one-on-one interviews or participation in a focus group. PHI is collected but measures to protect confidentiality are in place. The study is eligible for expedited review.
Case 2. Your IRB is asked to review a Phase 3 study of an investigational drug intended to treat Type 2 Diabetes. The drug has been well-tolerated and shown early signs of efficacy in several previous studies. The trial is randomized, double-blind, and placebo-controlled. It is enrolling individuals with persistent elevations in hemoglobin A1C (e.g., difficulty controlling glucose levels) despite standard of care medicines and diet. Participants are permitted to remain on stable current therapies but prohibited from starting new therapies during the study. The active treatment phase of the study is 15 weeks.
Case 3. Brain nociceptive opioid peptide (NOP) receptors are a putative target for the development of treatments for cocaine use disorders. To establish baseline scanning algorithms, twenty healthy individuals will be scanned using positron emission tomography (PET) to quantify the presence and distribution of NOP receptors. PET scanning involves the placement of an intravenous catheter, the placement of an arterial line in the radial artery (wrist), and the injection of a radioactive tracer which binds with the NOP receptor.
In Case 1, the next most frequently selected vulnerable groups were individuals of lower socio-economic status (SES) (30%), minority status (19%), and transgender or gender non-conforming (15%). In Cases 2 and 3, both of which involve higher risk research, the next most frequently selected vulnerable groups were individuals with a co-morbidity and those of child-bearing potential. 32% of all respondents thought that individuals with a comorbidity would be vulnerable and in need of additional protections in both Cases 2 and 3. 24% of respondents felt that individuals of child-bearing potential would be vulnerable in Case 2, with that increasing to 27% in Case 3.
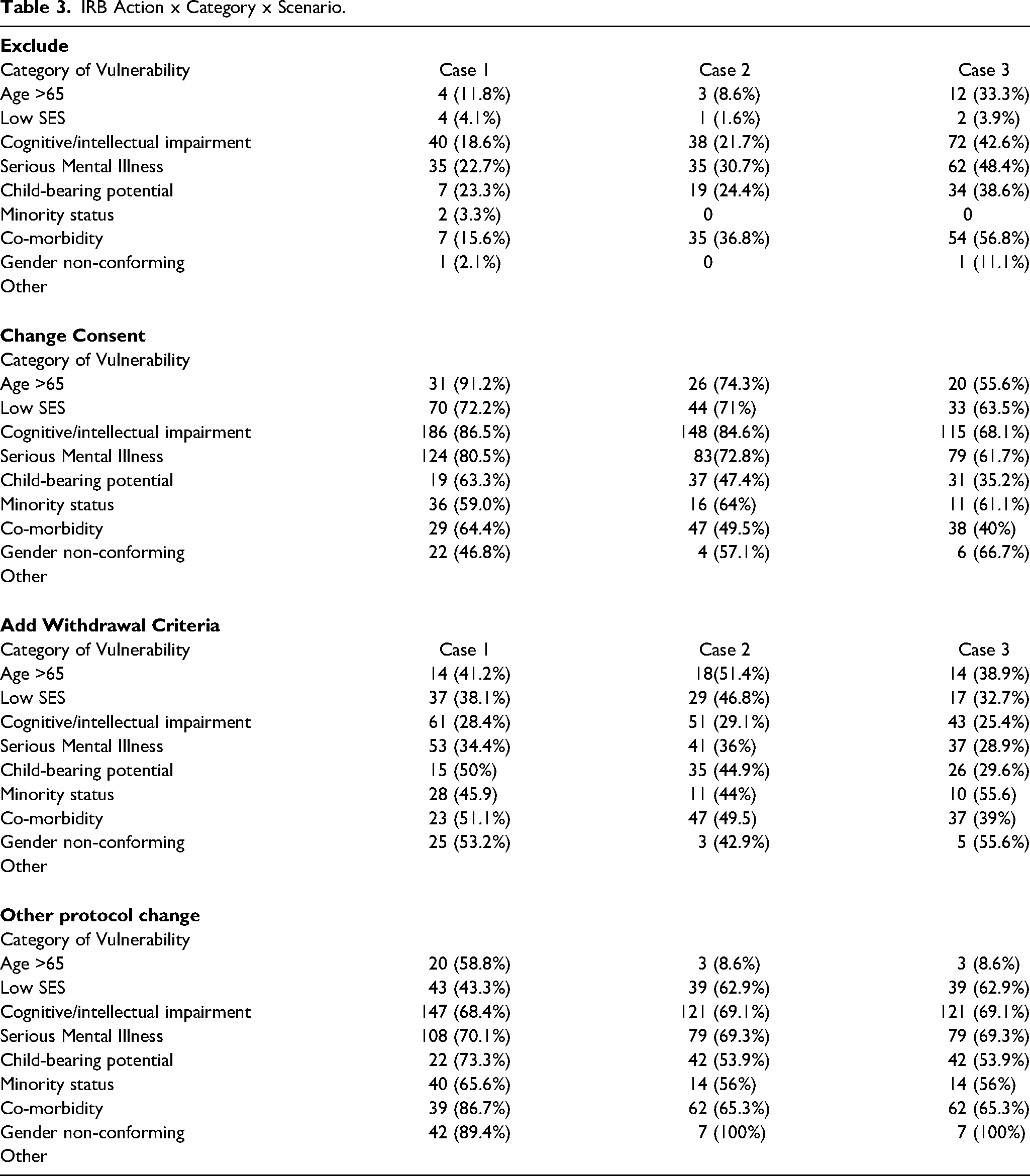
Of note, in terms of safeguards (Table 3), individuals with cognitive impairment and serious mental illness were most frequently “protected” by excluding them from participation altogether, regardless of the scenario. Of those respondents who considered these groups vulnerable, 19% felt that cognitively impaired individuals should be excluded in Case 1, with that increasing to 22% in Case 2 and 43% in Case 3. Similarly, 23% felt that individuals with a serious mental illness should be excluded in Case 1, with that rising to 31% in Case 2 and 48% in Case 3. Perhaps strikingly, a significant minority (39%) of respondents who felt that individuals of child-bearing potential were vulnerable in Case 3 indicated that excluding them would be an appropriate protection. Further, even in the minimal risk Case 1, some respondents who found individuals of child-bearing potential (23%), people with comorbidities (16%), and individuals older than 65 years of age (12%) vulnerable thought excluding them would be appropriate. See Table 3 for a more complete breakdown of the protections deemed appropriate for each group and scenario.
IRB Action x Category x Scenario.
Diversity and Inclusion
87% of respondents indicated that, in their view, it is important or somewhat important for IRBs to seek to ensure that study populations reflect the demographics of the condition being studied (Figure 3), and 58% said their IRBs often or always do so (Figure 4). In contrast to respondents’ very high degree of optimism about IRBs effectively protecting the vulnerable (where 95% said they often or always did), only 48% indicated that their IRBs often or always effectively promote inclusion of under-represented groups (Figure 2b).
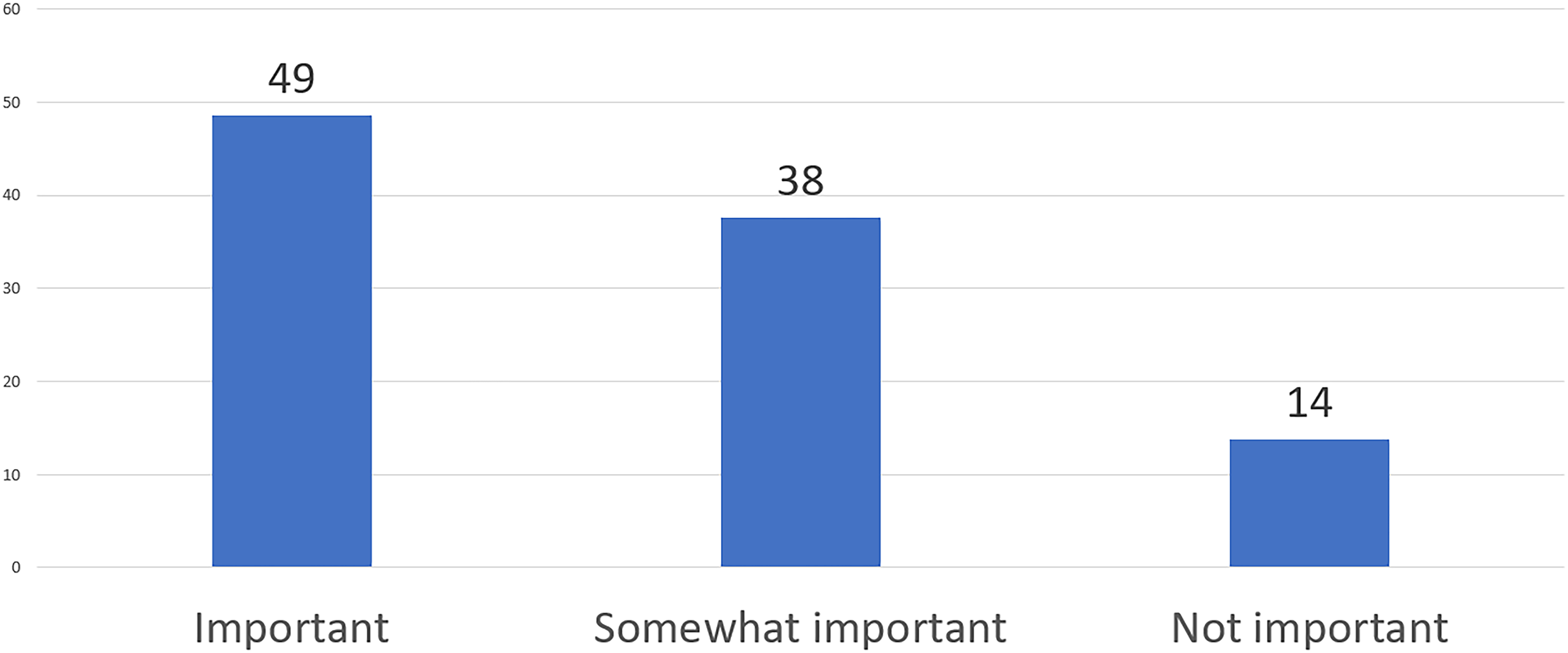
In your personal view, should IRBs seek to ensure inclusion of study populations that reflect the demographics of the condition being studied?
Does your IRB routinely seek to ensure inclusion of study populations that reflect the demographics of the condition being studied?
When asked which groups receive special attention from the IRB to ensure that they are not unnecessarily excluded, respondents most commonly selected racial or ethnic minorities (39%) and socio-economically disadvantaged individuals (34%). The next most frequently selected groups in this regard were individuals of child-bearing potential (22%), cognitively impaired individuals (21%), people aged 65 and older (19%), and transgender or gender non-conforming individuals (16%).
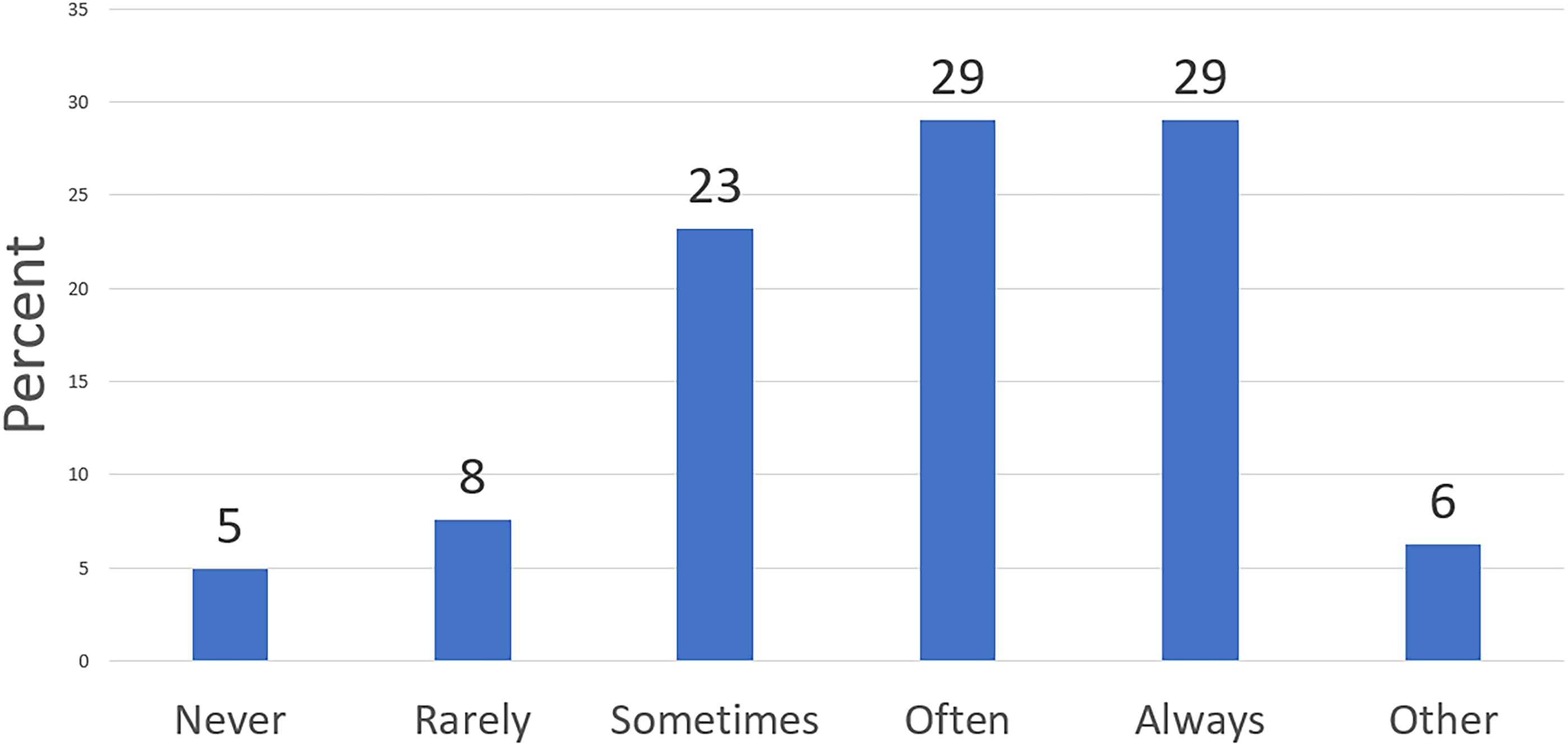
When asked about the specific actions taken to include groups the IRB feels are excluded without justification, 69% of all respondents said their IRB often or always seeks an explanation for the proposed exclusion, with 21% saying they sometimes or rarely do and 5% of respondents saying they never do (the rest being uncertain). 61% of respondents said their IRB often or always requests changes to the study's eligibility criteria when they feel that groups are excluded without justification, with 29% saying they sometimes or rarely do and 6% saying they never do. When asked about the related matter of whether or to what extent their IRB defers or disapproves research when it feels the proposed study sample is not representative, 53% of respondents said it sometimes or rarely does, 27% said it often or always does, 12% said it never does, and 8% were unsure.
Our responses suggest that the extent to which demographic data is collected by IRBs, as well as the types of demographic information collected, varies significantly between IRBs (Figure 5). Well under half of all survey respondents indicated that their IRB collects data on age (38%), race (27%), and ethnicity (25%). Only 7% of respondents indicated that information on SES is collected and 8% on educational level. More than half of our respondents (55%) indicated that their IRBs never or rarely review whether the demographic characteristics of the accrued study sample differ from the demographic characteristics of the originally proposed sample at the time of continuing review. 35% of respondents indicated that when the actual vs proposed sample demographics do differ at the time of continuing review, the IRB often or always requires an explanation or corrective action.
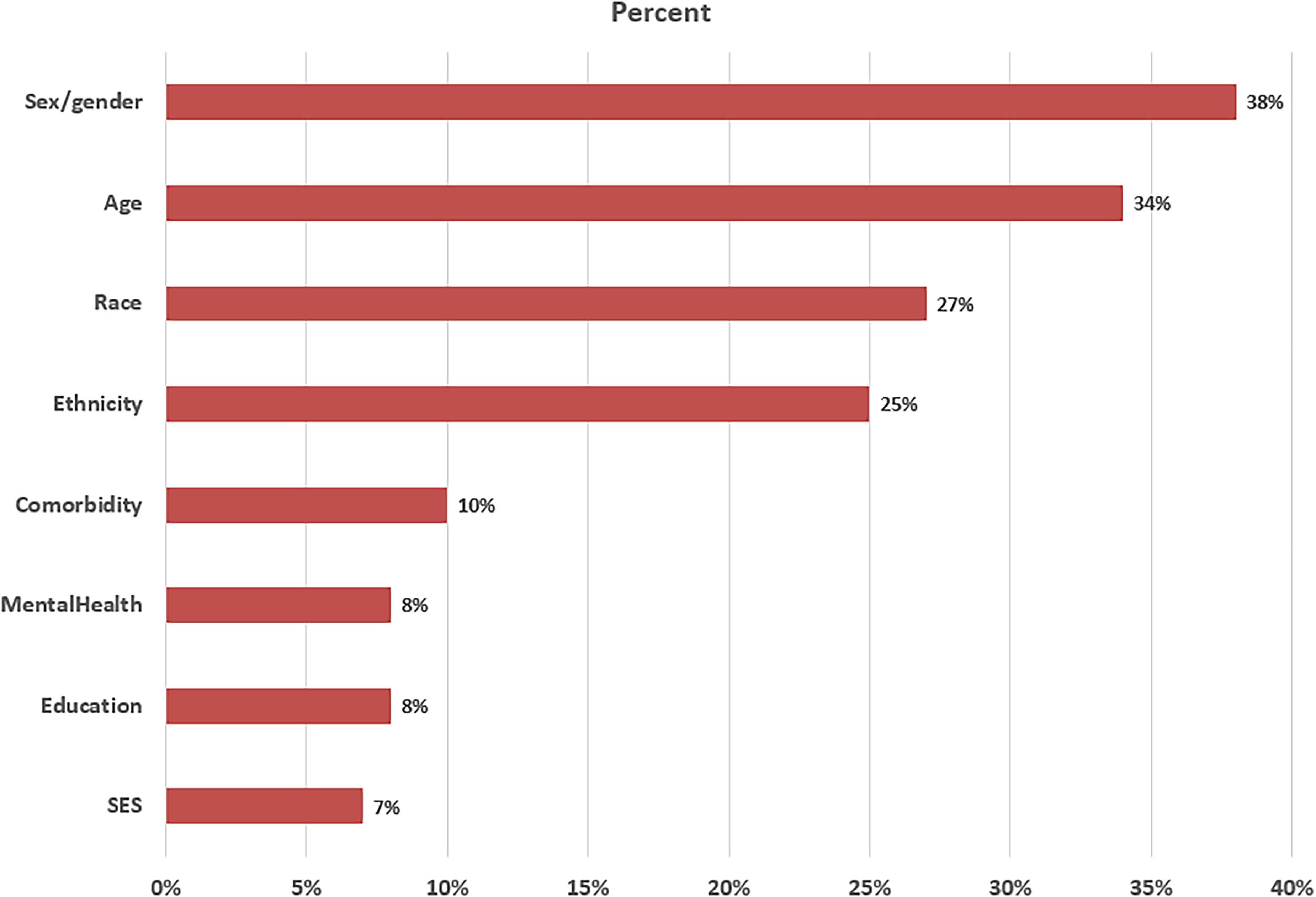
Percent of IRBs collecting demographic data, by category.
Only 35% of respondents indicated that they had written policies that guide IRB considerations of what constitutes appropriate inclusion/exclusion of populations with regard to demographic features. 58% of respondents indicated that additional guidance for IRBs that would delineate methods for identifying, and strategies for including, populations at risk of being under-represented would be very or extremely helpful.
Discussion
While it might be argued that all or at least most research participants are in a position of vulnerability, the US regulations construe vulnerability exclusively in terms of susceptibility to ‘coercion’ and ‘undue influence,’ two concepts whose meaning and application are perennial topics of debate (Gordon, 2020; Luna, 2019). However, respondents widely endorsed alternative definitions that tie ‘vulnerability’ to unique susceptibility to research risk, preexisting disadvantage (e.g., from illness or socio-economic factors), and difficulty comprehending elements of consent (e.g., cognitive impairment), suggesting that our respondents took ‘vulnerability’ to be more multi-faceted than the explicit regulatory definition. In addition, respondents were very optimistic about the ability of IRBs to protect those they consider vulnerable. This finding is perhaps not surprising given, as our results suggest, that IRBs routinely extend their conception of ‘vulnerable’ across many different types of contexts. Further, if the role of IRBs is understood primarily in terms of protection, anything less than high levels of effectiveness at protecting the vulnerable may constitute a self-acknowledged, serious failure in the IRB's mission (Miller & Wertheimer, 2007).
A general protectionist trend is evident in other aspects of the survey. Indeed, for the hypothetical research vignettes, the rates at which certain populations were deemed vulnerable in the different scenarios, and the safeguards applied to them, may provide evidence to support the belief that IRBs are inclined to characterize certain populations as inherently vulnerable and apply additional safeguards regardless of the degree of study risk or other study-specific factors. The degree to which respondents stated their IRBs would exclude potentially vulnerable groups from research, especially low risk research involving a focus group, is striking, given the availability of common protections short of exclusion for many such groups. These include decision supports and use of a Legally Authorized Representative for cognitively impaired individuals (Soofi, 2022); capacity assessment and requirements for ongoing therapy and monitoring for people suffering a serious mental illness; the possibility of requiring pregnancy screens and contraception measures for individuals of child-bearing potential; and carefully crafted eligibility criteria, individual withdrawal criteria, and increased safety monitoring for people with comorbidities.
Compared to their optimism about the ability of IRBs to protect the vulnerable, respondents were less sanguine about the role of IRBs in ensuring the inclusion of under-represented groups and sample populations that reflect the demographics of the condition under study. This is perhaps to be expected, given that inclusion has not historically been seen as central to the IRB's mission in the same way as protection, and given empirical work suggesting that IRBs may struggle to effectively promote inclusion goals (Taylor, 2009). That said, the fact that over half of the respondents reported that their IRBs always or often seek to ensure a representative sample, and almost half of respondents said that their IRBs always or often seek to ensure inclusion of under-represented groups, suggest that IRBs do believe they have a role to play in diversity and inclusion efforts (Berry et al., 2019; Friesen et al., 2022). This conclusion is further supported by the relatively high rates at which respondents indicated that their IRBs take action, seeking rationale and/or requesting changes to eligibility criteria, when they feel that groups are unjustifiably excluded.
The fact that respondents most frequently selected racial or ethnic minorities and socio-economically disadvantaged individuals as warranting special attention for inclusion deserves comment. The survey was conducted in the fall of 2020, when disparities in the impact of COVID-19 on racial and ethnic minorities in US, and the broader public discourse on societal inequities in the wake of the killing of George Floyd were at their height. In this context, IRBs may have been increasingly alert to the importance of diversity and inclusion in research enrollment and its value in identifying signals of biological difference, social determinants of health, and treatment response. An alternate explanation is that, even apart from scientific reasons for inclusion, IRBs recognize that these groups should have access to the potential benefits of research, a plausible ethical demand of justice.
When asked about their personal opinions, respondents ascribed a very high degree of importance to including under-represented groups and ensuring representative study samples—indeed, a degree of importance that can be taken to exceed the actual performance attributed by respondents to IRBs in this regard. This potential mismatch between the high importance ascribed by respondents to inclusion and the perception of IRBs’ actual performance could simply mean that the views of IRB chairs are not aligned with the views of other IRB members. However, it could also suggest that IRBs possess the general will to facilitate inclusion but are less certain about the extent to which this is their responsibility; or believe that inclusion is their responsibility but lack the means and practical ability to effectuate it.
One potential avenue through which IRBs could systematically and effectively work toward inclusion is with regard to the data they collect about the actual demographics of study populations at continuing review. Such data collection would seem to be a first step in the ability of IRBs to recognize and/or predict specific situations in which populations are at risk of being under-represented. Our finding that few IRBs collect demographic data at continuing review supports the conclusion that IRBs themselves could do more to bolster their role in inclusion. The low incidence of formal IRB policies addressing inclusion may also hinder the ability of IRBs to confidently undertake inclusion efforts. In addition, there are likely to be other explanatory factors for why IRBs do not do more with respect to inclusion, such as the possibility that this could require IRBs to tolerate slightly more participant risk coupled with the existence of incentives toward risk-aversion, and few incentives toward inclusion, for institutions and IRBs (Friesen et al, 2022).
Study Limitations
While we are confident that IRB Chairs are the best target respondent group for the issues addressed by the survey, and likewise confident that the set of individuals to whom the survey was sent (i.e., the denominator) closely approximated the universe of current US IRB Chairs, our 11.1% survey response rate was less than optimal. That said, it is worth noting that the demographics of our sample, at least, strongly resemble the demographics of samples in other completed surveys of IRB Chairs that have more of a claim to being representative due to higher response rates (Berry et al., 2019; Weissman et al., 2018). For example, our sample composition was strikingly similar to the sample from a recent RAND survey of IRB Chairs along axes of age, sex, and race/ethnicity (Berry et al., 2019).
A second noteworthy point stems from the turbulent social context in which the survey was administered. As noted earlier, respondents were asked to complete the survey at a time when existing health inequities were brought into sharp relief by the disproportionate impact of COVID-19 on communities of color. At the same time, discussions of equity and racial justice achieved a prominent place in the public square. While we are uncertain just how these factors impacted survey responses, it seems to us likely that they did.
Best Practices
Because of the preliminary nature of this work, we do not feel that it forms a sufficient basis for specific best practice recommendations. More empirical work is needed to confirm the themes identified here before specific conclusions can be drawn about their ethical and practical relevance. We do believe this work should encourage IRBs to pay closer attention to potential trade-offs between protecting the vulnerable and facilitating inclusion of under-represented groups in their deliberations and what role the IRB can and should play in specific circumstances to promote inclusion.
Research Agenda
The results of our study form a promising basis for future quantitative survey work and/or qualitative data-gathering on IRB approaches to vulnerability and inclusion, and ultimately, a more evidence-based regulatory framework. Such work could be designed to confirm and further explore the themes identified here, including such issues as the extent to which IRBs apply the concept of ‘vulnerability’ beyond contexts explicitly found in regulations; whether IRBs regard certain groups as inherently vulnerable, regardless of context; and what obstacles exist to IRBs more effectively promoting inclusion of under-represented groups. Given the highly contextual nature of many of these issues, qualitative interviews may be a particularly promising way to pursue them. Quantitative work should likely include case scenarios or other mechanisms for capturing the context-specific nature of IRB attitudes and practices on these issues. It would also be important to expand the scope of future research beyond IRB Chairs to include IRB administrators and other members of HRPPs.
Educational Implications
Key concepts from this work can be effectively taught by situating our findings within a discussion of the history of research oversight, which arose in large part as a response to public attention to the exploitation of vulnerable groups by research and inattention to the rights and welfare of underprivileged and marginalized populations. Further, our findings should be situated within an acknowledgment and exploration of the ways in which attention to equity and inclusion in research by IRBs, and by the larger research enterprise, can ultimately serve to reduce disparities in health care. Finally, our work can serve to stimulate the development and dissemination of practical tools and guidelines to enable IRBs to strike a healthy balance between protection and inclusion in ethics review. To this end, our findings should ideally be accompanied by efforts to understand the concept of justice and its potential limitations in the regulatory and applied ethical frameworks in which IRBs operate.
Footnotes
Acknowledgments
We are grateful to the National Center for Advancement of Translational Sciences for their support of this project (Grant#: 3UL1TR002541-02S1). In addition, we are grateful to the Consortium to Advance Effective Research Oversight at the University of Pennsylvania, as well as Harvard Catalyst's Regulatory Foundations, Ethics, and Law group, for permitting us to present a draft survey and providing helpful feedback and discussion. We also thank Evan Sohn for support during survey administration.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences, (grant number 3UL1TR002541-02S1)