
Abstract
Keywords
Introduction
Community-engaged research (CER) has a complex evolutionary history with roots in commerce, education, and social justice (Strand et al., 2003). “Action research” evolved out of Kurt Lewin's recognition of the importance of “democratic participation” of community members in crafting relevant research questions and the means to answer them (Adelman, 1993). Lewin's work underscored that the intended recipients of the benefits of research possessed unique knowledge and perspectives on social problems and that this knowledge provided a means to improve those problems. Freire (1970) sought to change education's role as a tool that reinforced oppressive socio-political power dynamics. Social justice researchers similarly critiqued positivist research methods, replacing them with participatory action strategies that shed light on unemployment, malnutrition, poverty, and environmental harms in under-resourced cultures and communities (Strand et al., 2003).
CER brings community members and academics together to identify, study, and implement solutions to problems affecting the community. Foci are typically local and collaboration ideally begins at the study design stage. Since its beginnings, CER research has expanded in terms of definition and reach; research designs span a continuum from no community involvement to studies that are initiated and led by community members (Key et al., 2019). Academic researcher roles range from designing and fielding the study, to which community members respond, to community members serving those roles supported by researchers (Healthy City CBPR Toolkit, 2011).
Institutional models of CER training, such as the North Carolina Translational and Clinical Sciences Institute Community and Stakeholder Engagement Program (UNC, 2020) exist to inform stakeholder engagement at all stages of research. Many of these models focus on building networks between systems (UNC, 2020; WHO, 2022) in order to address problems that require input from a variety of stakeholders (e.g., medical providers, policy-makers, community members, and other significant constituents). Many medical and social problems necessitate multi-level remedies, such as policy change to support practice innovations. Community participation models engage an array of stakeholders that offer unique insights into problems based on lived experience. Guidelines for effective stakeholder engagement ask reviewers to consider whether stakeholder engagement is surface-level or meaningful (“tokenism”), whether the level of stakeholder engagement fits the study purposes (tailoring), and to establish IRB review criteria for evaluating stakeholder engagement in studies (Wilkinson et al., 2022).
Examples of illnesses necessitating broad community engagement and streamlined IRB review include highly contagious, lethal illnesses such as Ebola. Similarly, prevention and treatment studies of socially stigmatized conditions, such as HIV/AIDS, require sensitive engagement of community, medical, and academic organizations that touch upon human health. Our work represents a unique subset of these models in that we engaged community members with specialized training in the delivery of animal-assisted therapy to implement a hospital-based intervention in the context of a randomized controlled trial. Engaging community members with specialized training who are not academic faculty requires a mechanism for training them in principles of human subjects research that they would not otherwise have acquired. In that respect, our community-engaged researcher training fits a unique niche adjacent to existing community and stakeholder engagement programs.
The Role of IRBs in Traditional and CER Research
An Institutional Review Board (IRB) is an oversight body, usually embedded in an organization, including universities, health care systems, and other institutions that regularly conduct research involving human subjects. In the United States, the IRB is tasked with reviewing research proposals against federal regulations for the protection of human subjects, state and local laws, ethical principles, and institutional standards. The federal regulations most usually applicable to research are those put forth by the Department of Health and Human Services (DHHS), located at 45 CFR 46, and broadly referred to as the “Common Rule”. For research conducted outside the U.S., readers can refer to the International Compilation of Human Research Standards (2021).
Under U.S. regulations, institutions engaged in research must
Provide written assurance to DHHS that the institution will comply with the regulatory requirements put forth in the Common Rule for non-exempt human subjects research (45 CFR 46.103(a)). This written assurance is generally referred to as a Federal-Wide Assurance (FWA). Certify to DHHS that any research conducted at the institution has been approved by an IRB designated in the assurance (45 CFR 46.103(b)).
In the context of traditional research, this means that investigators must prospectively submit research proposals to their institution's IRB and obtain approval from the IRB prior to initiating any research activities. In general, research proposals submitted to an IRB identify the key individuals who are conducting the research, and in most traditional research projects, these individuals are usually all employees of the same institution. The assurance and certification requirements in the Common Rule are the reason that IRB review is always institution-specific, rather than project-specific. Institutions conducting research can only make the assurances required by an FWA for their own agents and employees, because an institution does not have authority or control over agents and employees from other institutions. This is why research projects that are conducted at multiple institutions typically involve the collaborating sites entering into an agreement to cede IRB review to a single identified site, in a process typically referred to as single IRB (sIRB) review. But, in most traditional research contexts, each collaborating institution holds its own FWA, and each research team member is affiliated with one of the collaborating sites.
Where CER can add a layer of complexity to IRB review typically falls into two domains:
Whether or not any individuals from the community are engaged in the research If community members are engaged in the research, how to “extend” an institution's FWA to cover those community members
“Engagement” in Research and its Impact on IRB Review of CER
The Common Rule requirements only apply to institutions that are engaged in research. It is important, therefore, to understand what is meant by “engagement,” particularly as it applies to CER. In the Office of Human Research Protections (OHRP, 2008) guidance document, “Engagement of Institutions in Human Subjects Research,” it is explained: In general, an institution is considered engaged in a particular non-exempt human subjects research project when its employees or agents for the purposes of the research project obtain: (1) data about the subjects of the research through intervention or interaction with them; (2) identifiable private information about the subjects of the research; or (3) the informed consent of human subjects for the research. (A. Institutions Engaged in Human Subjects Research, paragraph 1.)
Under this definition, depending on the level of community engagement in CER, members of the community can easily become “engaged” in a research project. Because IRB review must cover all activities conducted by individuals engaged in the research, when individuals outside the reviewing institution become investigators, their involvement may need to be included in the considerations made by the reviewing IRB. When community members are not otherwise affiliated with an institution covered by an FWA, the IRB must then consider strategies for “extending” an FWA to cover the involvement of those engaged community members.
The discussion above applies specifically to IRBs in the United States. A set of human subjects protections guidelines has been developed by the Council for International Organizations of Medical Sciences (CIOMS) (van Delden & van der Graff, 2016) with respect to community engagement. Those guidelines suggest that community-engaged researchers have proactive and sustained engagement in all aspects of research, including study design, informed consent, study implementation and monitoring, and dissemination of findings (van Delden & van der Graaf, 2016). Many research projects engage social systems at multiple levels to address physical illness and social problems. As noted above, our project occupies a unique niche within this area of research that requires CER training methods specifically tailored to the project.
“Extending” an FWA to Cover non-Affiliated Community Members in CER
Under OHRP guidance, institutions may extend an FWA to cover an individual investigator, provided that an appropriate agreement is executed, outlining the responsibilities of the FWA-holding institution and the individual investigator. OHRP guidance (2005) defines individual investigators as an individual who is:
not otherwise an employee or agent of the assured institution; conducting collaborative research activities outside the facilities of the assured institution; and not acting as an employee of any institution with respect to their involvement in the research being conducted by the assured institution.
Individuals meeting this definition can be covered by an institution's FWA, provided an appropriate agreement is executed. The guidance document provides a list of responsibilities to which the institution and the individual investigator must agree. There are many responsibilities covered in the guidance document, but most relevant to this article is the requirement that “the collaborating individual investigator agrees to complete any educational training required by the assured institution.”
Need for Adaptation of IRB Review Models to Allow for Flexibility Required by CER Methods
While the regulations themselves do not strictly require investigators to obtain training in the protection of human subjects in research, the terms of an institution's FWA state that an institution is responsible for ensuring that its investigators understand and act in accordance with the regulatory requirements. Therefore, in the Terms of Assurance for an FWA, OHRP strongly recommends that institutions develop training requirements for investigators. Typically, most institutions in the United States fulfill this requirement through training programs such as the Collaborative IRB Training Initiative (CITI) training program. CITI training is just one option for institutions to ensure its investigators are adequately trained, but it is widely used due to its comprehensiveness, customizability, and ease of implementation.
However, several limitations of CITI render it less feasible for community-engaged researchers. The modules are targeted towards an academic audience, are lengthy, and may be ill-suited to training community investigators engaged in CER. In addition, most IRBs review protocols from a biomedical perspective that does not adequately incorporate community engaged research methods (Flicker et al., 2007). Depending on the level of engagement of the community members in a given research project, training programs like CITI may, at best, constitute information overload, resulting in a lack of meaningful understanding of how to best protect research participants; or, at worst, serve as a barrier to the participation of community investigators in CER.
Therefore, it behooves institutions that frequently review CER to develop flexibility in policies regarding required training programs, particularly in the context of training requirements for community investigators engaged in CER. This paper discusses one potential model for addressing the need to train community investigators engaged in CER on the protection of human research participants in a way that is suited to the community investigators’ role in the research. This model uses human-animal interaction research involving therapy dogs and their volunteer handlers delivering an animal-assisted intervention to hospitalized older adults as a vehicle to explore collaborative engagement between a university IRB, academic researchers, and community-based volunteers.
Human-animal interaction research focuses on how the bond between people and animals can improve health and well-being for both species. The field has evolved from anecdotal observations of human-animal interaction benefits to deploying methodologically rigorous clinical trials to better understand the effects of the human-animal bond on health outcomes. A literature search for CER studies in the human-animal interaction field yielded only one study that outlined the collaboration of human-animal interaction researchers with elementary school teachers to design a classroom-based, animal-assisted literacy intervention for children (Steel et al., 2022). As human-animal interaction research methods continue to evolve, integrative collaboration between researchers and community members may proliferate, necessitating an human-animal interaction-specific framework for CER studies. We hope that this paper can provide an initial roadmap for increased engagement between human-animal interaction researchers and community members as well as a prototype for researcher/IRB collaboration in fielding human-animal interaction and other intervention or interaction studies that are rigorous in their scientific and ethical approach to research.
Materials and Methods
The CER training we describe below was developed in the context of a randomized controlled trial (RCT) examining the impact of therapy dog visitation on a number of patient mental health and physiological outcomes in a hospital setting.
“Dogs on Call” Community Member Volunteers
Our community member volunteers were all registered therapy dog handlers who provided animal-assisted interventions in the context of the Dogs on Call program. Dogs on Call is a hospital-based, therapy dog visitation program that provides support to inpatients and outpatients at an academic medical center. The program consists of over 60 human-therapy dog teams registered with either Pet Partners or Alliance of Therapy Dogs. The program was established in 2001 and has become an integral part of medical staff support and patient care. Most of the human volunteers are white females over the age of sixty. Together, Dogs on Call teams (consisting of a human handler and their registered therapy dog) provided 3,761 visits to patients in 2022. A subset of 14 human-dog teams volunteered to deliver an animal-assisted intervention to research participants as part of a randomized controlled trial evaluating the efficacy of animal-assisted intervention for reducing loneliness, depression, and anxiety in older adults hospitalized for serious health conditions. Demographic information for the human-dog teams is provided in Table 1.
Demographic and Breed Characteristics of Dogs on Call Research Teams.
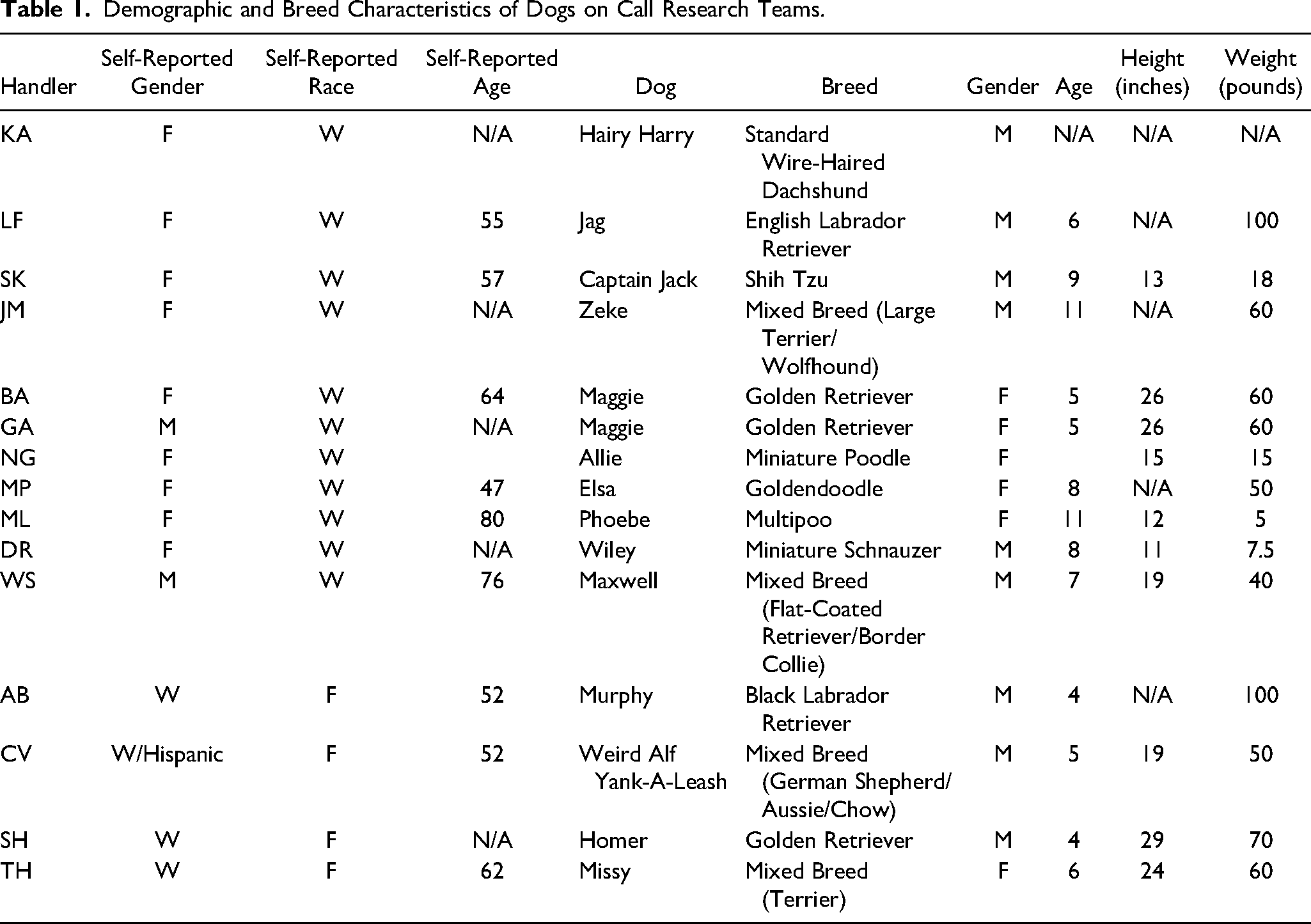
Dogs on Call teams provide in-depth situational knowledge and expertise to animal-assisted intervention research. The teams offer extensive familiarity with hospital surroundings and the daily activities of patients and staff. They work seamlessly with medical providers to deliver support to patients in the busy context of an inpatient environment. The dogs and handlers work effectively amidst medical equipment, personnel, and a cacophony of sounds associated with intensive medical care. The teams are sensitive to the emotional and physical needs of patients and family members. Importantly, teams provide comfort and support to hospital staff as well and are welcome, established colleagues threaded into the daily routine of hospital care. Therefore, involving the teams in delivery of the animal-assisted intervention being studied in the RCT was a logical choice in terms of their experience with patients and acceptance by medical staff.
Early Collaboration with Local IRB
A project of this nature necessitated adaptation of usual IRB application procedures given that Dogs on Call volunteer handlers were not academic researchers by training and thus did not have the human subjects certification required of academic personnel. Discussions with IRB members suggested that a condensed version of the CITI human subjects training could be developed and tailored to the specific educational needs of the Dogs on Call volunteers. This adapted training made it feasible for the volunteers to receive human subjects training and deliver the intervention in the context of the study. Subsequently, IRB members and the researchers worked together to develop a streamlined version of the CITI modules that covered concepts relevant to the volunteer handler role in intervention delivery. The IRB provided guidance regarding the essential elements of human subjects protection education, which the researchers used to develop a video-based training module. An initial outline of key concepts was reviewed by the IRB and successive iterations were jointly developed by IRB members and the researchers until a final training outline was solidified. Subsequently, this outline was used to develop an interactive video of approximately 45 min in length. The details of the training tools are provided below.
CER Role in Intervention Delivery
The CER volunteer dog handlers performed a unique role in the research project by delivering the intervention in two of the study arms. They were listed as community engaged researchers on the IRB protocol, along with their individual training completion certificates and training assessments. The context was an RCT that evaluated the efficacy of animal-assisted intervention, conversational control (CC), and treatment as usual (TU) for ameliorating symptoms of loneliness, depression, and anxiety in hospitalized older adults. CER volunteers delivered the animal-assisted intervention and CC interventions, which consisted of three 20-min visits with individual study participants either with or without their dog over three days. The volunteers used the same conversation guidelines they would otherwise follow for regular hospital visits; these guidelines provided suggested topics (their dog, the participant's pets, the weather, sports, etc.). Research staff included School of Medicine faculty and research assistants, all of whom completed the Collaborative Institutional Training Initiative (CITI) human subjects protections training as required by the university IRB. They screened potential study participants, obtained initial informed consent, and collected baseline measures. The intervention spanned three consecutive days and was structured such that a research assistant initiated the study visit and collected pre-intervention measures. The research assistant then introduced the CER volunteer, who led the visit alone with the participant while the research assistant waited outside the room. At the twenty-minute mark, the research assistant signalled the end of the intervention and the CER volunteer closed the conversation and exited the room. During the intervention itself, the CER volunteers monitored and responded to research participant needs with particular attention paid to reaffirmation of consent. Consent reaffirmation was especially relevant to this clinical trial given that study participants were often extremely ill or had suffered injuries associated with significant pain. The CER training module provided information on non-verbal withdrawal of consent so that handlers could offer to end or reschedule the visit if needed.
Human Subjects Training Module
The final CER training module featured core human subjects protections concepts (Ross et al., 2010), including highlights from the Belmont report, definitions of autonomy, beneficence, and justice, the voluntary nature of participation in research and the importance of consent reaffirmation, as well as examples of coercion and undue influence. Training length was approximately 60 min, with approximately 40 min of didactic instruction interspersed with discussion followed by a test to measure comprehension. The instructor (LT) was present during the training and led the interactive discussion components of the module. Didactics were bolstered by vignettes tailored to reflect real-world scenarios that Dogs on Call teams could encounter when delivering an intervention to inpatients in a research context. A series of best-to-worst response options were provided to learners in a multiple-choice format. The vignettes were discussed and the rationale for the best response provided as well as the reasons why the other choices were not ideal. Following vignette discussions, the comprehension test was administered and scored. Subsequently, correct and incorrect answers were discussed and volunteers were allowed to correct missed items and ask questions regarding test items. Finally, the tests were submitted and rescored. A score of 80% was required to complete the module successfully. This test format mirrored the one used in the CITI training modules.
Results
Fourteen volunteer dog handlers received the training. All passed the training module with a score of 80% or higher. Importantly, the length of our expedited review process (18 days) was similar to metrics published by the Association for the Accreditation of Human Research Protection Programs (2022), which reported an average review time of 17 days across 250 institutions. The CER handlers proved to be a vital asset to the study, consistently providing observations to the research team regarding nuances of study visits. They exhibited a high degree of comfort with the hospital environment and with various types of physical illness and injury. They also served as essential liaisons to healthcare workers, ensuring that medical staff received therapy animal visits before and after study interventions. These spontaneous visits solidified the relationship between the research team and healthcare workers, which was important given that study visits could represent an interruption to their daily routine. Healthcare workers began to associate the study team with the Dogs on Call handlers in a kind of “halo effect”, which also facilitated study activities. Benefits of this included staff receptiveness to the research, integration of the study team into daily activities on the inpatient units, and assistance in talking to potential participants about the study. One example of this is physician involvement in sharing information about the study with patients - one physician found a study team member and facilitated an introduction to his patient, whom he thought would enjoy participating in research to alleviate her boredom, regardless of the condition to which she was assigned. To date, CER handlers have conducted 107 research visits. Study attrition rates have been too low for statistical analysis, another indicator of the beneficial impact of the handlers. Research participant feedback indicates that they report positive experiences with the intervention and some have requested to be contacted again for future participation. These findings are consistent with those of other CER-based studies involving older adult volunteers in settings with patients of similar age in that our volunteers offered “context-specific” understanding that contributed to intervention success (MacLeod et al., 2012).
Importantly, no research participants raised issues related to human subjects protections and no protocol violations, such as breaches of confidentiality, have been detected. This is particularly encouraging given that the volunteer handlers were unfamiliar with the human subjects protections literature prior to receiving the training and nearly all were unaware of the historical backdrop that framed the Belmont Report.
Discussion
The CER volunteers provided unique expertise for the study given their experience with handling their therapy dog while visiting patients in the hospital. This familiarity with ill patients allowed them to respond sensitively to study participant needs during the intervention and to respond gracefully if a visit needed to be rescheduled. This expertise was critical to providing an appropriate and timely response to patients who were very ill or in pain and who might not directly communicate their desire to end or reschedule a visit. The CER volunteers’ sensitivity and judgment was essential to effective conduct of the study given that research staff waited outside the room during the interventions and did not have the extensive experience working with hospitalized older adults offered by the CER volunteers.
Trainings such as this one provide a model opportunity for researchers who wish to incorporate animal handlers into their research protocols, as is frequently the case with research on human-animal interactions. In this area of research specifically, animal handlers are almost exclusively volunteers who are already donating their available time to visit individuals in need. It requires a substantial time commitment to ask them to take the full CITI course, which would be a significant barrier to their participation in research projects. The CER training imparts the necessary information for them to be involved in the study, but at a much-reduced time commitment, making it much more likely that they will participate. Many animal-handlers express an interest in being involved in research, but they also make it clear that their available time is limited.
The reality is that requests for Dogs on Call visits exceed the capacity of the program to meet those requests because individual dog handlers only have limited time in their schedules to volunteer, and because there is a 2-h limit on the amount of time their dog may be in the hospital on any given day. This 2-h limit, although not universal, is commonly accepted as an upper limit on daily working time for therapy dogs. This limit is applied to ensure the welfare and wellbeing of the dogs while keeping their overall stress levels low, so they continue to enjoy visitation. Some dogs can tolerate less time in the hospital before becoming fatigued and it is a requirement of the handler that they carefully observe their dog for signs of fatigue or stress and remove their dog from the setting immediately when they notice any of those signs. These time limitations exemplify the need for CER training to be implemented in an efficient and expeditious manner, while balancing the need to impart key learnings. It also exemplifies why a more prolonged approach to training would be a serious barrier to conducting research of this nature.
In addition to the need to reduce barriers to community members’ engagement in CER, it is equally important to ensure that those community members who do engage in CER are trained effectively. In the case of the animal-handlers in this study, the goal of the specially-designed training was not only to use their time efficiently, but also to ensure the importance of engaging in ethical research practices was effectively communicated. The emphasis on practical examples through the vignettes, and the narrowing of the focus of the training on the specific involvement of the animal-handlers, were designed to make the training relevant to the trainees, thus enhancing information comprehension and retention.
Likewise, the bespoke CER model outlined above can be more broadly applied to other intervention approaches. For example, it can be employed when researchers are interested in examining the impact of interventions offered by individuals with specific skills, talents, or training, such as musicians, artists, or chaplains, but those individuals are not directly involved in the broader research protocol or, in some cases, even aware of the research aims and hypotheses. Making it easier for these key people to participate in research projects creates opportunities to explore a wider variety of research ideas in more naturalistic settings. It allows researchers to ask and answer research questions that may have previously been too costly from a time and practicality perspective. It also affords researchers greater freedom to explore ideas and investigate unique interventions that may have the potential to be highly impactful.
Although researchers and the IRB share the same goal, delivering research studies in a safe and ethical way, there are times when researchers have developed an antagonistic relationship with their IRB. These relationships can be stressful and can become non-productive. We found that working in collaboration with members of our IRB was both rewarding and productive. We developed the CER training described above together and have successfully implemented that training in three ongoing studies. This model represents a true collaboration among colleagues who share the same goal and is consistent with recommendations for researcher/IRB collaboration during the CER process (Cross et al., 2015). We hope other researchers will explore this approach with their own IRBs. Strengthening relationships between researchers and IRBs is helpful even outside of CER contexts. Models for close collaboration between academic researchers and IRBs can be used to improve researcher/IRB relationships both within and outside of CER while improving the relevance and quality of research. The shared expertise of IRB members, who bring broad insights about how research methods impact human subjects, combined with the specialized knowledge of researchers, can advance the relevance, integrity, and impact of study findings on people and the problems that affect them. When IRBs and researchers are not seen as partners in the research enterprise, compliance can become perfunctory. Whereas, when researchers view the IRB process as value-added to their research, compliance becomes a shared responsibility and mission. IRBs and researchers can both benefit from collaboration early on in the development of research proposals: first, considering regulatory and ethical issues at the point of study design can obviate IRB concerns further down the review process, thus streamlining the review process for both parties. Second, and more importantly, it ideally results in more meaningful compliance, and more sensitivity to ethical issues, as IRBs and researchers work together towards the shared goal of producing high quality research while protecting the rights and welfare of the participants who generously volunteer their time and effort for the advancement of science.
As with all research, this project has limitations. Most importantly, there was minimal integration of community members and recipients of the intervention in the study design process. Other models exist that engage community stakeholders and systems in the full continuum of research activities to address health and social issues (UNC, 2020; WHO, 2022). The volunteer dog handlers did not develop the study questions or the means to answer them and patients only provided feedback regarding their experience with the intervention. In that sense, the study falls at the low end of the community engagement continuum (Key et al., 2019). However, the process outlined here provides a template for engaging community members in investigator-initiated studies, which still predominate in academia.
As is the case with all training and education, including the CITI training, a limitation of the CER approach is the amount of information retained and the ability of the participant to apply or transfer that learning to actual situations. The accepted approach to addressing this limitation has been to require refresher course work (e.g., CITI refresher courses) and we agree that this should also apply to CER training. In the absence of any other information about the retention of concepts taught in the CER training, we suggest refresher training every three years, to be consistent with the approach taken by CITI.
A final limitation on this approach is that an institution must have flexibility built into its IRB policies on researcher training. The VCU IRB explicitly states in its written Policies and Procedures on investigator and study team training that alternative training curricula can be considered by the IRB on a case-by-case basis. The policy requires the submission of proposed training materials to the IRB and such materials must be approved by the IRB before they can be used in lieu of CITI training. Other institutions may not have such flexibility built into equivalent policies or may outline a different process for the review and approval of the proposed use of alternative training options.
Best Practices
A key feature inherent to the success of this project was open, supportive collaboration between university faculty and the IRB. We highly recommend that faculty, community members, and IRBs create opportunities to connect and discuss CER topics regularly to foster a productive relationship. Having a collaborative relationship forms the foundation for faculty and IRB members to engage one another early on in a study's inception, which saves time and clarifies necessary tasks for the project to move forward. In addition, IRBs should establish their own guidelines for alternative human subjects training curricula. IRB-approved CER trainings can be disseminated within and outside a university to pave the way for future CER studies.
Research Agenda
Many aspects of CER warrant further exploration. These include the degree to which IRBs have established mechanisms and criteria for reviewing CER studies as well as the level of integration that exists between university faculty and IRBs in the conduct of CER research. Additionally, understanding barriers to and facilitators of such faculty/IRB collaboration is vital to promoting CER research. Finally, important outcomes such as information retention on the part of community-engaged researchers and whether bespoke trainings are associated with fewer study participant complaints and improved satisfaction with study participation should be examined.
Educational Implications
Community-engaged research offers an avenue for examining real-world problems while incorporating the perspectives of stakeholders who have first-hand experience living with those issues. IRBs vary in their degree of preparation to review CER studies and their flexibility to consider alternative CER training methods. Lessons learned from successful collaborations such as the one described above can be disseminated more broadly by bringing faculty and IRB members together in academic settings to share ideas and foster communication. Model CER/IRB trainings can be incorporated into CER coursework as well as IRB member continuing education. The Collaborative Institutional Training Initiative (CITI) offers several CER modules that were created by a group of faculty, community partners, and IRB members (CITI, 2019). These provide a foundation for faculty and IRB members to consider alternative training mechanisms to support CER research.
Footnotes
Acknowledgements
The authors would like to thank the Dogs on Call volunteers who completed and provided feedback on the training and played a vital role in the completion of the research.
Data Availability Statement
Data not available - participant consent.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author's partner receives or has received research support, acted as a consultant for, and/or has received honoraria from Acadia, Adamas, Aevi, Afecta, Akili, Alkermes, Allergan, The American Academy of Child and Adolescent Psychiatry, American Psychiatric Press, Arbor, Axsome, Daiichi-Sankyo, Emelex, Gedeon Richter, Genentech, Idorsia; Intra-Cellular Therapies, Kempharm, Luminopia, Lundbeck, MedAvante-ProPhase, Merck, MJH Life Sciences, NIH, Neurim, Otsuka, PaxMedica, PCORI, Pfizer, Physicians Postgraduate Press, Q BioMed, Receptor Life Sciences, Roche, Sage, Signant Health, Sunovion, Supernus Pharmaceuticals, Syneos, Syneurx, Takeda, Teva, Tris, and Validus. The third author has the following financial relationships to disclose: she has received research support, served as a member of the speaker's bureau, acted as a consultant for, and/or received honoraria from Animal-Assisted Interventions Singapore, Mars Petcare, Nestle Purina, Society for Companion Animal Studies, Singapore National Parks, The Human-Animal Bond Research Institute, Wallis Annenberg Petspace, and Waltham Petcare Science Institute.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Waltham Petcare Science Institute, (grant number NA)