
Abstract
Through strengthened biobank governance, broad consent has been widely accepted as a means to replace donors’ discretion based on the information of individual research protocols. Trust and other ethical and social notions, such as reciprocity and solidarity, are key concepts that support biobank governance. The types of allowed broad consent are several; however, they remain unclear, and whether these ethical and social notions are associated with public attitudes toward the consent model is not fully understood. This quantitative study examined two hypotheses: narrower and limited broad consent are more accepted by the public, and acceptance rates for broad consent increase with established measures related to biobank governance. This analysis supported both hypotheses, implying that the limited type of broad consent should be considered an important option, and that a specific type of governance is critical in promoting trust, reciprocity, and solidarity between biobanks and the public.
Keywords
Introduction
Biobanks—that is, systems that collect human tissues, blood, cells, and related items, to be used for biomedical research over a long period—are constantly changing their role and nature (Coppola et al., 2019). Simeon-Dubach and Watson (2014) have proposed the concept of “Biobanking 1.0–3.0,” wherein they described three stages of biobanking: primary focus on the number of biospecimens and data (Biobanking 1.0), primary focus on the quality of biospecimens and data (Biobanking 2.0), and a new focus on the need of activities, products, and services provided by the biobank that relate to external stakeholders (Biobanking 3.0), which represent the change in the implications of biobanks depending on changes in science and society. The changing concept of biobanks is largely due to the changes in the content and methods of life science research and partly due to people's changing attitudes regarding scientific research, researchers, and the treatment of human specimens and data. Therefore, to maintain sustainability, it is necessary to continue following the attitudes of various stakeholders.
Several empirical studies examining stakeholder attitudes toward biobanks and research use of human biological samples have been conducted, with several review articles on such empirical studies (D’Abramo et al., 2015; Domaradzki & Pawlikowski, 2019; Garrison et al., 2016; Master et al., 2012; Rachul et al., 2012; Tindana & De Vries, 2016; Wendler, 2008). The issue of consent is a major topic in the ethical, legal, and social issues related to biobanks (Caulfield, 2007; Coppola et al., 2019; D’Abramo et al., 2015; Hoeyer, 2012) and is an important target for such empirical studies. The main findings on consent in the review articles revealed different understandings of consent models. However, limited consent models, such as study-by-study consent, are more likely to be accepted compared to broad consent (that is, consent for an unspecified range of future research) with certain limitations and process restrictions, such as prior approval from a relevant research ethics committee; this is less specific than consent for a particular use but narrower than open-ended permission without any limitations (Grady et al., 2015). Few studies have examined the attitudes of Japanese public on consent models. A population-based quantitative study (Oikawa et al., 2023) demonstrated that the Japanese public prefers specific (study-by-study) consent, including dynamic consent, meaning an interactive personalized communication interface that allows donors to engage as much or as little as they choose (Budin-Ljøsne et al., 2017; Kaye et al., 2015; Thiel et al., 2015; Prictor et al., 2018).
Although broad consent remains the most widely accepted form of consent in current biobanks (Coppola et al., 2019; Grady et al., 2015; Steinsbekk et al., 2013), it is partly considered problematic concerning donor autonomy and has been a topic of extensive discussion over time (Árnason, 2004; Caulfield, 2007; Caulfield & Murdoch, 2017; Hoeyer, 2012; Hofmann, 2008; Karlsen et al., 2011; Shickle, 2006). This is mainly because broad consent does not provide the donor with sufficient information about the details of individual studies, which may not guarantee the donor autonomy. However, the concept of autonomy in medical and research ethics is not always clear. The theory of autonomy presented by Beauchamp and Childress (2019) requires intentionality, understanding, and non-control as conditions for autonomous action. This theory is widely known as the default conception of autonomy in bioethics, but the above interpretation is often criticized as not being an essential understanding of autonomy. Particularly, this view of autonomy does not require any consideration of the actions’ content or substance but only of the process or procedure by which they were decided (Dive & Newson, 2018; Walker, 2009). Critics of this point consider autonomy to be more comprehensive and have often highlighted relational perspectives. For instance, Jennings (2016, p. 13) asserted, “The challenge of respecting the autonomy of persons is not to avoid relationality, but to distinguish those forms of relationship and life worlds that are functional for the maintenance of communal meaning and integrity from those that are not, those that are conducive to the creative activity of individual self-discovery and self-realization from those that are not.” The focus of the criticism of broad consent is that it does not guarantee donor autonomy; however, if the concept of autonomy is considered in this broad way, it may not necessarily mean that autonomy is at risk.
Whatever the interpretation may be, broad consent is substantially different from specific consent in terms of the information provided to the donors and the manner of donor communication. Dynamic consent is an information-based communication model based on a donor-centered approach that seeks to reflect the donor's wishes as much as possible. Another similar model is called “meta consent,” which combines the broad and dynamic consent models with additional options for blanket consent (agreeing to every use) and blanket disagreement (disagreeing with every use; Ploug & Holm, 2015). According to this model's author, the key idea is that individuals should be able to decide how they want to give consent in the future. Individuals can choose the type of consent for different types of research by filling in a simple “tick box” table online; the options include dynamic consent, broad consent, blanket consent, and blanket refusal. Meta consent considers the differences in personal interests and levels of trust in researchers among the population. The risk of routinization and “consent fatigue” is reduced as individuals can limit the requests they receive to the research categories that matter to them (Ploug & Holm, 2015, 2019).
As such, donor-centered, highly flexible consent models are being considered in the biobank context. In particular, dynamic consent has matured and become popular in some countries over the past decade (Dankar et al., 2020; Teare et al., 2021). In contrast, broad consent has been accepted through the strengthening of biobank governance to complement the lack of options or flexibility for donors. Trust and other ethical and social notions, such as reciprocity and solidarity, have become key concepts in the biobank governance (Hansson, 2005; Knoppers & Chadwick, 2005; O’Doherty et al., 2011; Tutton et al., 2004).
However, empirical studies on broad consent with the general public in the context of biobank governance are limited. The reasons to consider public attitudes on this matter are two. First, as such attitudes reveal the public's lived experience and perspective, this helps to develop the ethical norms of biobanking, the arguments of which are entangled with empirical assumptions of stakeholders and conditions of reasoning (Mihailov et al., 2022). As empirical bioethics exploration entails a process in which the empirical and the normative are seen as mutually informing (Ives et al., 2017), public opinions would bring new perspectives to the argument. Second, biobanking is not a one-time event but instead a long-lasting enterprise, and its sustainability is a critical issue. Biobank sustainability could include a social perspective, which is dependent on public acceptance of potential donors (Abdaljaleel et al., 2019; Seiler et al., 2015; Simeon-Dubach & Watson, 2014; Watson et al., 2014). This means that if the biobank is not trusted by the public and has little social acceptance, its sustainability will decrease. This is the kind of thing that could happen in a real biobank. For example, when it was revealed that blood samples collected for medical research in the Swedish PKU Biobank were used in criminal investigations, about 2,000 donors demanded that their samples be destroyed (D’Abramo, 2015; Gottweis, 2008; Tamburrini, 2011). This implies that the views of the stakeholder, that is, the public, should be reflected in the biobank's norms and governance to enhance its sustainability. With this in mind, we conducted an empirical study on broad consent to clarify the attitude of the Japanese public.
The definitions of broad consent are several based on their range and options (De Vries et al., 2016), and the types of broad consent allowed by the public remain unclear. Furthermore, whether the ethical and social notions mentioned above are associated with public attitudes toward the consent model remains ambiguous. Thus, this study examines the following hypotheses: (1) narrower and limited broad consent is more accepted by the public, and (2) acceptance rates for broad consent increase in the presence of established biobank governance measures.
Methods
We conducted this study in February 2021 as a supplementary survey to a previous study (Oikawa et al., 2023). We commissioned a research firm to recruit 800 respondents, conduct the online survey, and collect the data. Respondents were randomly selected from approximately four million people living in Japan registered with the survey company; distribution was adjusted to reflect the composition of the Japanese population in terms of gender, age, and place of residence. To ensure that the survey represented the attitudes of laypeople, we excluded people from the pharmaceutical industry, medical field, and health food industry. We obtained informed consent from all respondents prior to their participation and provided them with information about the study objectives, potential risks, and right to choose whether to participate in the first page of the online questionnaire or not. The respondents voluntarily clicked on the “Start” button if they wished to participate. The study protocol was approved by the research ethics committee of the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo (2019029NI).
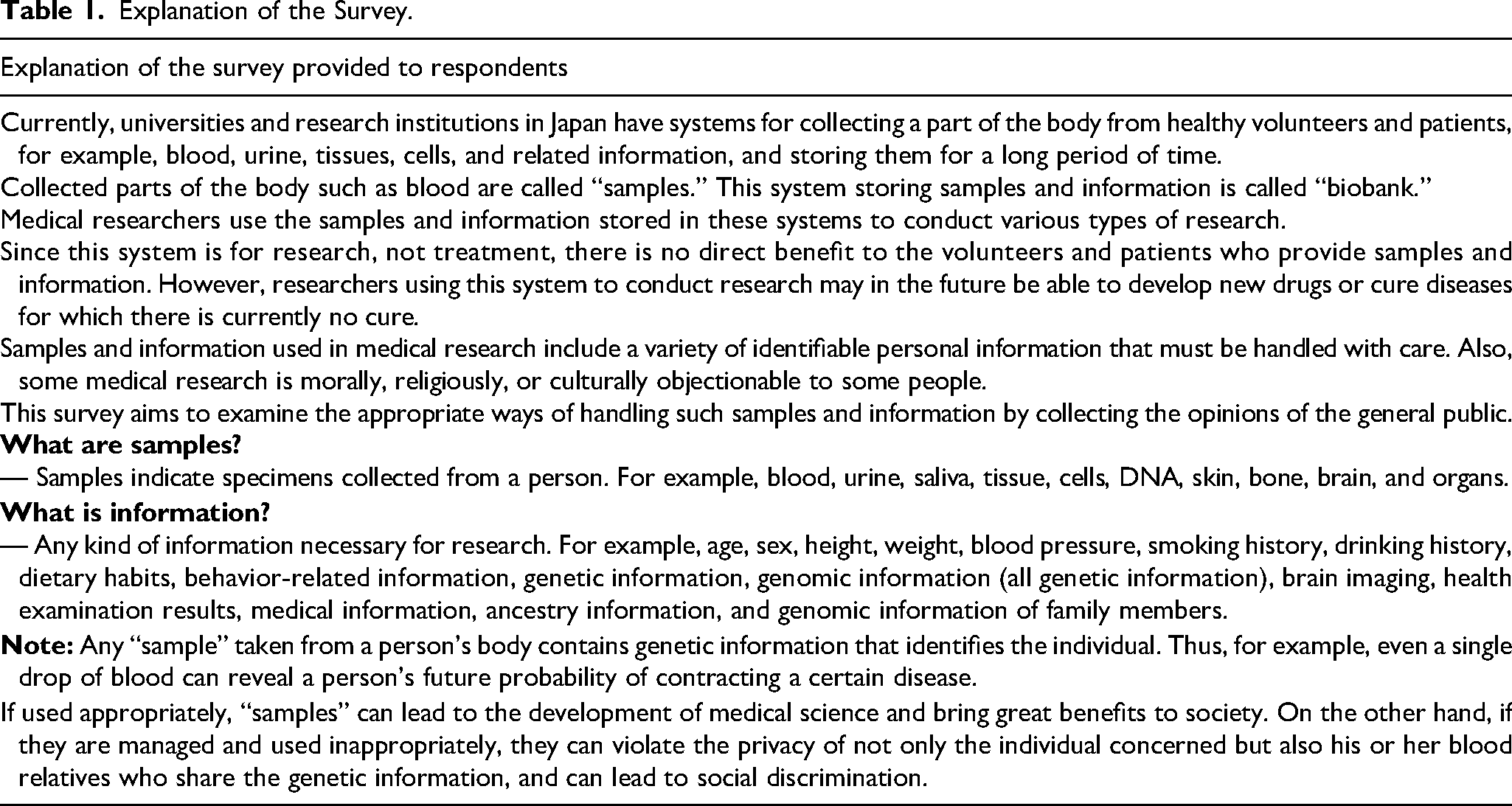
Biobank research was explained at the beginning of the survey using examples of “samples” and “information” (Table 1). We made multiple inquiries to evaluate engagement in biobank research across various sample types and studies (Table 2) and used a 5-point Likert scale for the responses.
Explanation of the Survey.
Questions Assessing Participation in Biobank Research.
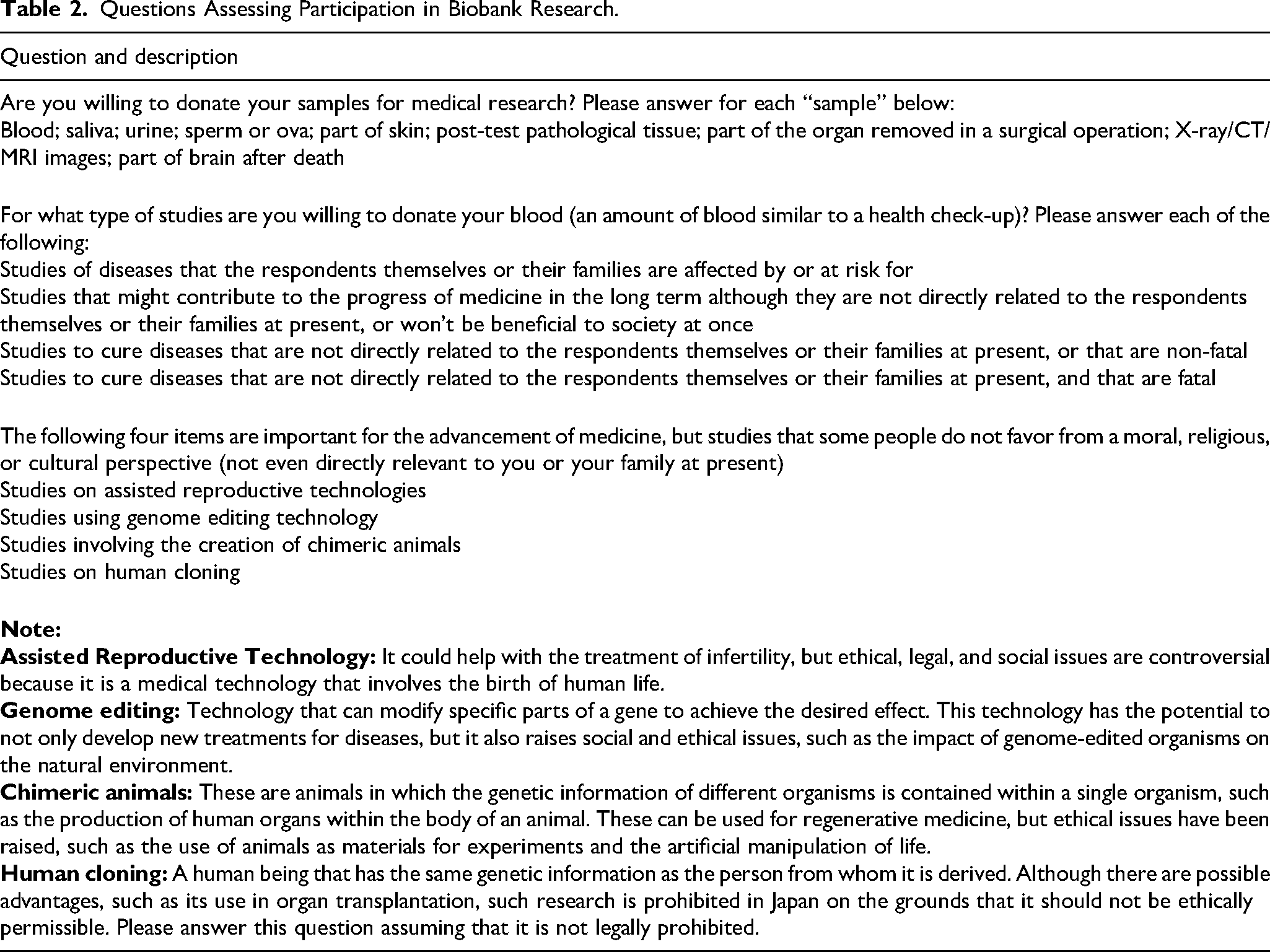
This survey adopted the framework and definition of broad consent used in the 2014 U.S. national survey by De Vries et al. (2016) with the authors’ permission, which presented five types of consent: (1) broad consent, (2) broad consent combined with caution, (3) broad consent combined with an option to withdraw, (4) broad consent combined with limits, and (5) real-time specific (study-by-study) consent for the use of the donated samples. In this definition, broad consent means that the “donors have control over whether to donate but not over how the samples are used in any future research.” “Caution” is defined as an advance alert to donors: “Some people may have moral, religious, or cultural concerns about some kinds of research.”
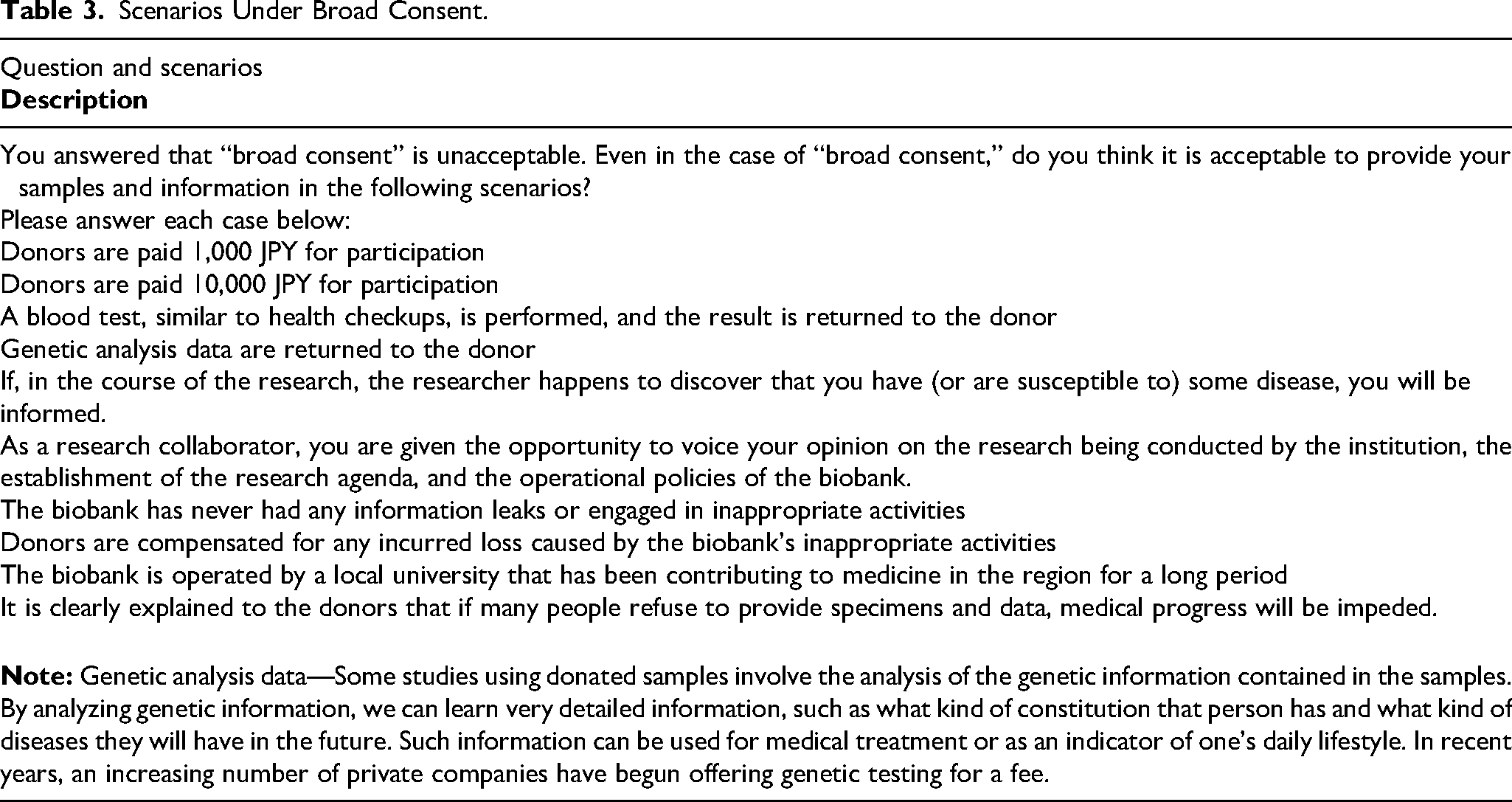
In broad consent with limits, donors “are given a short list of types of research projects that might worry some people. The donors then decide which types of research can’t use their donation” (De Vries et al., 2016, p. 4). It should be noted that, for consistency in terminology, in this paper, we use the term “broad” in the categorization of consents instead of “blanket,” which was used by De Vries et al. (2016) (also see the Limitation section for the comparison between the two studies). After explaining these consent models, we asked the participants to examine which types of consent models were acceptable or unacceptable and best and worst. Additionally, those who responded that broad consent was “unacceptable” were presented with scenarios to check whether they would change their minds in certain situations (Table 3).
Scenarios Under Broad Consent.
To analyze data distribution and characteristics, we computed descriptive statistics, including frequencies and percentages of responses for each item, using the IBM SPSS for Mac version 27.0 (IBM Corp., Armonk, NY).
Results
Demographics
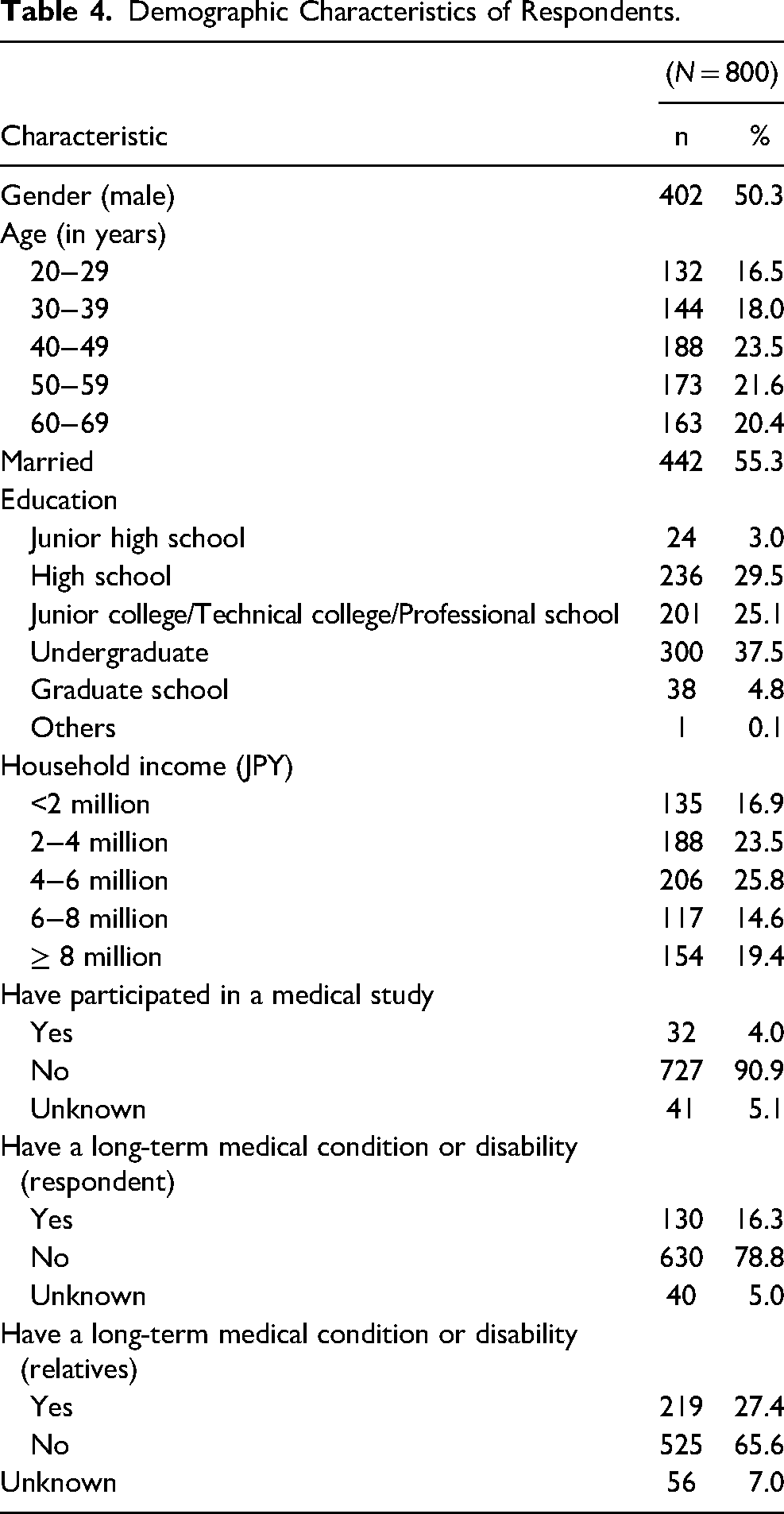
Table 4 presents the respondents’ demographics.
Demographic Characteristics of Respondents.
Participation in Biobank Research
This survey demonstrated that more than 50% of respondents were willing to provide blood and saliva as specimens. Between 40%–50% were willing to provide urine, post-test pathological tissue, a part of the organ removed in a surgical operation, and X-ray/CT/MRI images. Fewer respondents (30%–40%) were willing to provide part of their skin or brain after death, and only 21.5% indicated a willingness to provide their sperm or ova (Figure 1).
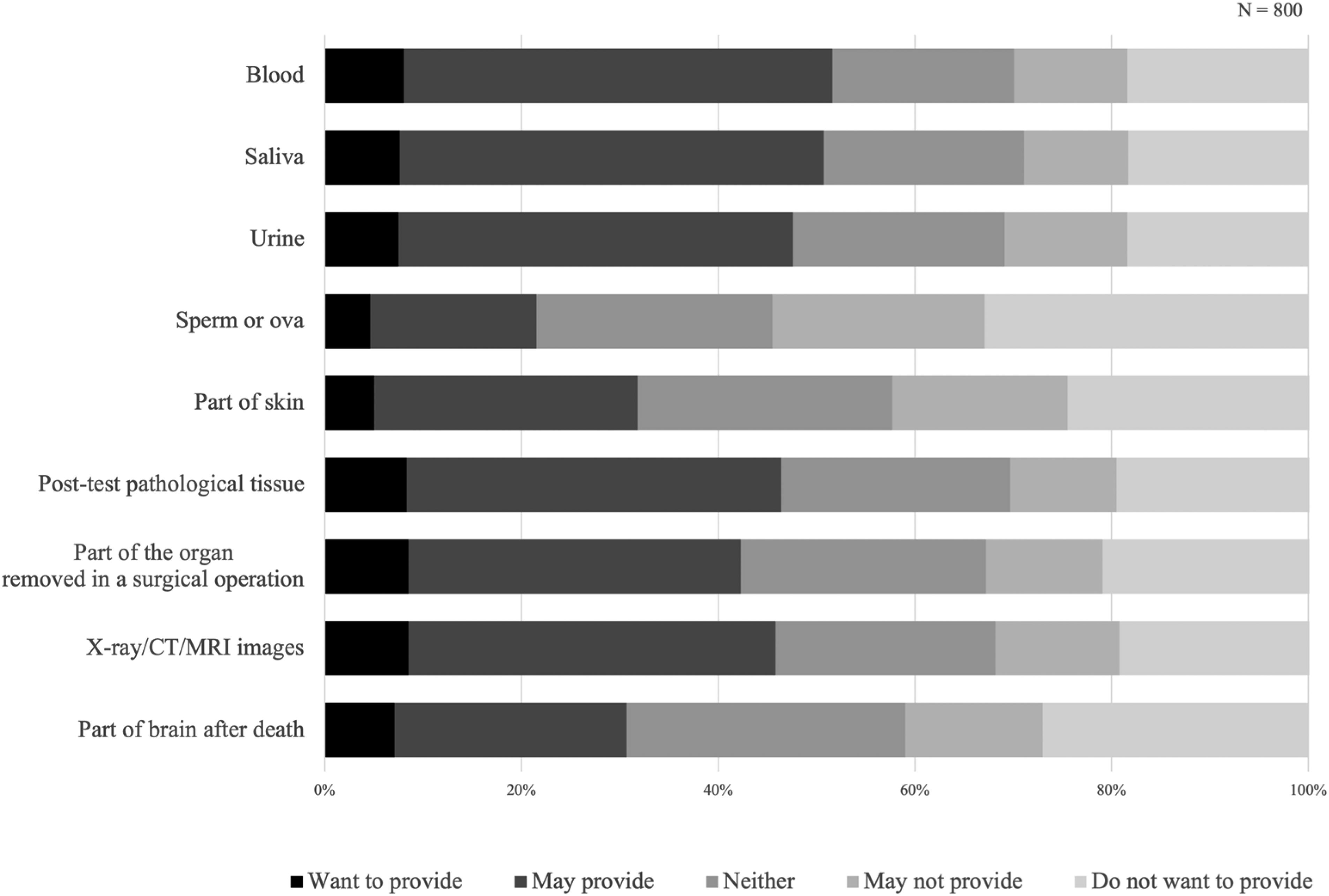
Specimen that may be provided.
This survey showed people's willingness to provide blood for certain fields of study. In total, 60.4% of respondents were willing to donate an amount of blood “similar to a health check-up” for “studies of diseases that the respondents themselves or their family are affected by or at risk for,” and 40%–50% were willing to do so for “studies that might contribute to the progress of medicine in the long term although they won’t be beneficial to society at once,” “studies of fatal diseases,” and “studies of non-fatal diseases.” A total of 30.3% expressed their willingness to donate blood for studies on assisted reproductive technologies; however, only 10%–20% would do so for studies using genome editing technologies, those involving the creation of chimeric animals, and those related to human cloning (Figure 2).
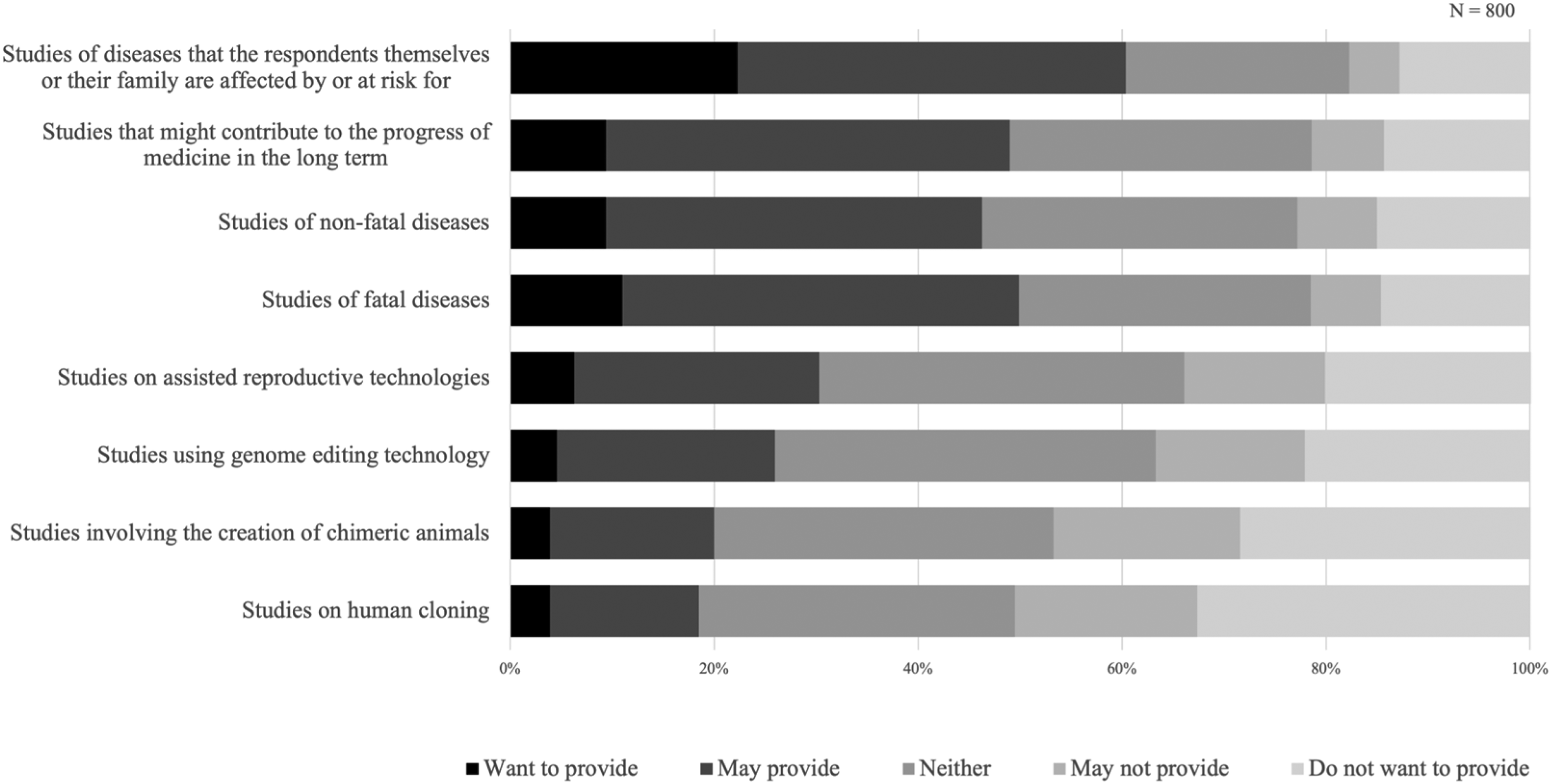
Type of studies that may be provided.
Attitudes Toward Consent Models
Table 5 shows the attitudes toward various types of broad consent. The most acceptable consent type was specific consent, followed by broad consent with limits, broad consent with an option to withdraw, broad consent with caution, and broad consent. Nearly half of the respondents (46.3%) selected specific consent as the best model, whilst more than half (52.1%) considered broad consent the worst option.
Attitudes Toward various Types of Broad Consent.
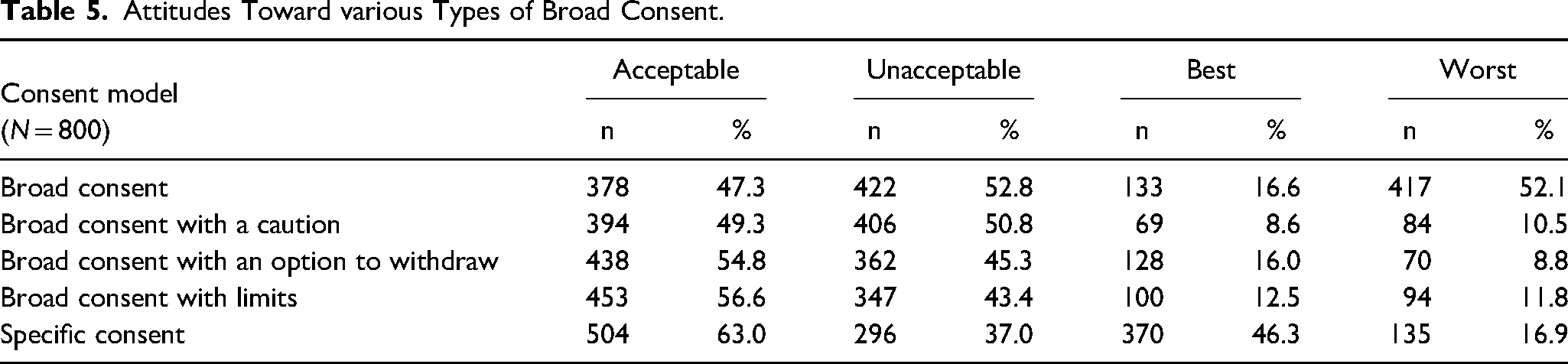
Table 6 presents scenarios that increased the acceptability of broad consent. For those who found broad consent to be “unacceptable” (n = 422), if donors were informed about incidental findings, approximately one in three respondents (27.7%) would provide specimens and data to the biobank under broad consent. A similar percentage (26.3%) would participate in the biobank if donors were compensated for any incurred loss; 22.5% would participate if genetic analysis data were returned to the donor; 21.8% would participate if the biobank had never suffered any information leaks or inappropriate activities, and 21.6% would donate if the results of a blood test were returned to the donor. Additionally, other scenarios were found to be effective in changing the minds of 10%–20% of respondents to accept broad consent.
Scenarios Increasing the Acceptability of Broad Consent.
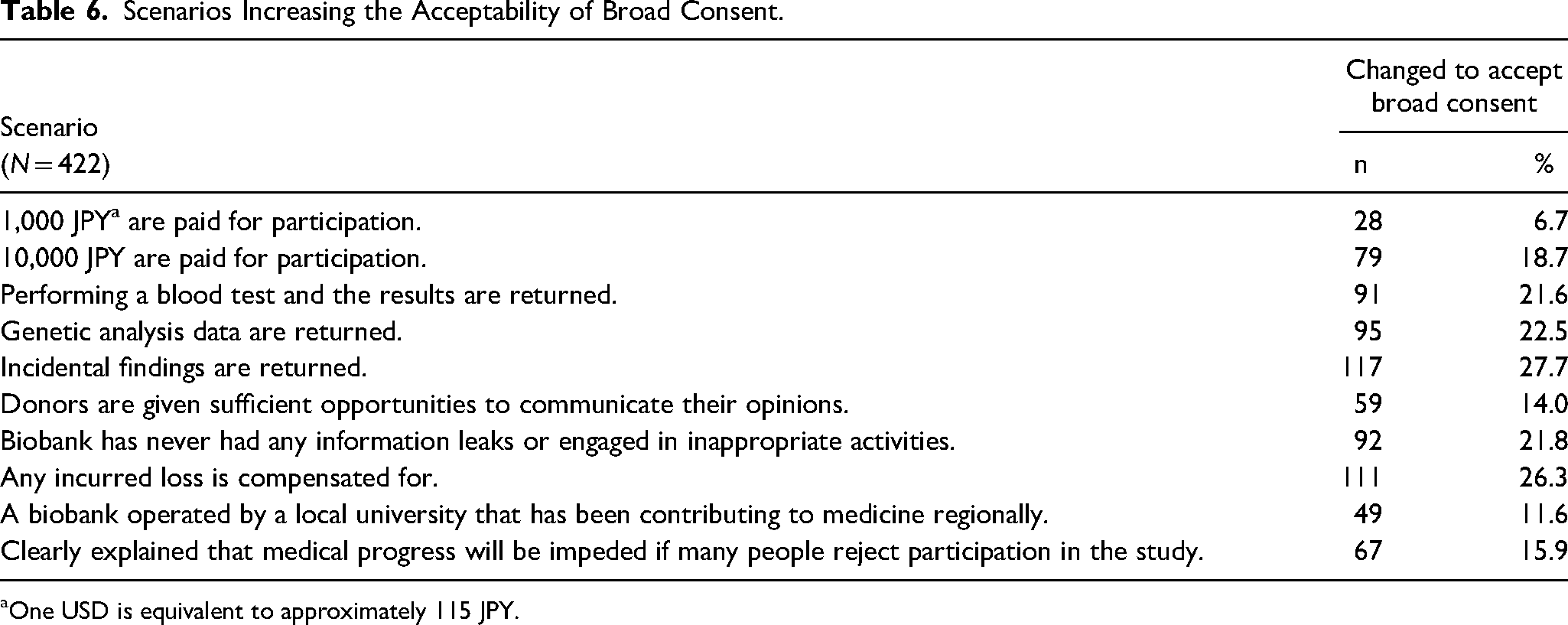
One USD is equivalent to approximately 115 JPY.
Discussion
Acceptability for Broad Consent
In this study, we conducted an online quantitative survey to investigate the Japanese public's attitudes regarding biobanking research. The results indicated that nearly 60% of respondents were willing to provide samples for biobanking; however, the rate was lower for specific samples. The participation rates were low for controversial studies; these results were consistent with previous surveys (Domaradzki & Pawlikowski, 2019).
Even when options were available for broad consent (caution, withdrawal, or limits), specific consent was considered the best model. Compared with the results of De Vries et al. (2016), whose broad consent framework we adopted in this survey, the present study indicated that, compared to US citizens, more Japanese people preferred specific consent (Japan vs. the US for specific consent: acceptable: 63% vs. 57%; best: 46.3% vs. 19.4%; worst: 16.9% vs. 45%). Overall, approximately half of the respondents agreed to some type of broad consent. Furthermore, limited broad consent was more acceptable than other types of broad consent. Although this result supported the first hypothesis, it contradicted the results of the US study (Japan vs. the US for the acceptability of broad consent with caution: 49.3% vs. 71.9%, broad consent with an option to withdraw: 54.8% vs. 70.8%, and broad consent with limits: 56.6% vs. 65.1%). Limited broad consent was preferred in Japan as specific consent was perceived as the best model by nearly half of the respondents; however, this could not be ascertained due to lack of data.
Trust, Reciprocity, and Solidarity
The present survey demonstrated how scenarios that would promote trust in biobanks and reciprocity or solidarity between biobanks and donors increased the rates of acceptability of broad consent. This result supports the second hypothesis. As mentioned in the Introduction, the issues surrounding the ethical and social aspects of biobank research imply the importance of trust in the relationship between biobanks and the public for the sustainability of biobank research. This is because broad consent, in the context of biobank and genomic research, has limitations concerning options and flexibility for the donors. Therefore, biobank governance promoting trust, reciprocity, and solidarity has been emphasized (Cargill, 2016; Chadwick & Berg, 2001; Hansson, 2005; Knoppers & Chadwick, 2005; O’Doherty et al., 2011).
As long as biobank activity depends on the donors’ voluntariness, goodwill, or altruism, public trust plays an important role in biobank research. While trust is multifaceted and context-dependent, and definitions vary considerably (Sheikh & Hoeyer, 2018), they share certain common themes (Hall et al., 2001; Samuel et al., 2022). Such definitions stress “the optimistic acceptance of a vulnerable situation in which the truster believes the trustee will care for the truster's interests.” Here, “vulnerability” is inseparable from trust; therefore, “[t]he greater the risk, the greater the potential for either trust or distrust” (Hall et al., 2001, p. 615). When uncertainty arises in a particular situation or system, trust can be a way of providing people with the means to deal with those uncertainties. This understanding of trust is closely related to Luhmann (2017), who discusses it as a mechanism of complexity reduction. Trust aims to reduce social complexity or uncertainty during decision-making (Samuel et al., 2022).
As, under broad consent, donors must decide whether to participate in future research with limited information and do so based on a current situation and the factors therein, broad consent involves a high degree of confidence. Donors decide to participate in biobank research as they trust that the biobank will appropriately treat their donated materials based on the different “trust mechanisms,” such as rational decision-making, knowledge-based trust rooted in previous experience, and identification-based trust related to emotional ties, shared values, or altruism (Nielsen & Kongsholm, 2022; Samuel et al., 2022). In broad consent, “the informational component is replaced by trust; instead of knowing that nothing untoward will happen with the sample, the consenter trusts that the consentee will not misuse the sample” (Nielsen & Kongsholm, 2022, p. 7).
Concepts of reciprocity and solidarity in biobanking and genomic research are elusive. These have recently been examined as more relational and less individualistic concepts, particularly in the field of public health ethics (Baylis et al., 2008). Reciprocity is being discussed as a model of exchange relationships to replace the traditional gift and altruistic models in research participation, and systems providing individual returns and benefits to the participants are being considered in biobank research (Hobbs et al., 2012; Kanellopoulou, 2011). Jennings and Dawson (2015, p. 32) define solidarity as “a moral practice that is fundamental to a social and cultural structure of right relationship,” where the right relationship is “a condition of mutuality—the mutuality of interdependence, care, and concern for others and their relational human flourishing.” More specifically, solidarity is defined as “common interests, purposes or sympathies between discrete individuals or among members of a group” (Baylis et al., 2008, p. 204) and “manifestations of people's willingness to carry costs (financial, social, emotional, or otherwise) to assist others” (Prainsack & Buyx, 2013, p. 75). The UK Biobank has been successful in recruiting by emphasizing solidarity and appealing to the citizens’ moral principles for a better society in the future (Hobbs et al., 2012; Lenk, 2011).
Empirical studies have demonstrated the practical significance of these concepts in creating a robust and durable research infrastructure. Trust is often associated with a preference for broad consent (Caulfield et al., 2012; De Vries et al., 2016; Gaskell & Gottweis, 2011). Modest payments or the return of individual research results could outweigh the privacy concerns of some people when deciding whether to participate in biobank research (Hobbs et al., 2012; Kaufman et al., 2009). A recent survey in Africa also demonstrated that many potential donors preferred to receive feedback on results of any relevance to their health (Nansumba et al., 2022).
The present survey confirmed that the degree to which some potential donors would accept broad consent could be increased by implementing various measures related to biobank governance. Specifically, efforts intended to promote trust, reciprocity, and solidarity in biobank research would change donors’ attitudes toward the consent model. The return of incidental findings, genetic analysis data, blood test results, and payments for donations are factors that foster reciprocity. People find biobanks trustworthy if they provide compensation for any incurred loss, never have information leaks or engage in inappropriate activities, and are operated by a reputable local university. If biobanks respect people's opinions and emphasize the common good, people will lend their support in solidarity. Overall, approximately 10%–30% of potential donors who initially found broad consent unacceptable changed their minds as a result of appropriate governance-related efforts. The survey results have considerable practical implications, especially on the recruitment of donors for biobank research implemented with broad-type consent.
Prior studies have developed philosophical arguments regarding broad consent, focusing on donor autonomy. However, this study suggests that other moral, psychological, societal, and relational perspectives, such as trust, reciprocity, and solidarity, are equally or even more crucial for donors and sustainable biobank operations. Donor autonomy is an importance principle in research ethics. This empirical study proved that if the concerned research body implemented certain governance measures, a substantial number of prospective donors would be convinced to accept broad consent or abandon opportunities for decision-making at their discretion based on the information of individual research protocols. However, this study does not suggest that autonomy can be replaced ethically and epistemologically by these concepts, which, however, appear to be factors that supplement autonomy in some ways. A theoretical and philosophical discussion of this topic about the implications of autonomy and the normativity and legitimacy of trust, reciprocity, and solidarity in biobank research, together with the relationship between philosophical perspectives and empirical data, will be a topic for future research.
Limitations
The initial explanations of the survey given to the respondents might have resulted in biased outcomes, although we had carefully chosen the wording and expressions to improve the respondents’ understanding. Furthermore, in terms of data comparison with the US, it should be noted that this is not an exact comparison owing to the differences between the US study and this survey in the initial explanation given to the respondents, the overall questionnaire structure, and the sample recruitment method.
As this study was limited to the Japanese population, its generalizability in a global context remains unknown. The attitudes of the public regarding the handling of human biospecimen and data are influenced by cultural and religious factors (Fleming et al., 2021; Jenkins & Sugarman, 2005; Mello & Wolf, 2010); therefore, the present findings cannot directly represent the attitudes of the public in other countries.
Best Practices
In this study, Japanese people preferred specific consent, while broad consent was acceptable when it was the limited type. Given the practical significance of appropriate governance for broad consent, this study suggests two possible future courses of action for biobanks as best practices. One is to pursue specific or flexible consent, including dynamic consent and meta consent, to emphasize donors’ decision-making at their discretion. The other is to accept broad consent with appropriate limitations, understand the donor's possible demand for specific consent, and consider implementing carefully designed governance policies aimed at mitigating donors’ concerns. The suitability of either approach will be defined by the type of biobank based on objective, size, prospective donors, specimens and data, range of data sharing, period of storage, financial circumstances, and whether it is public or private.
Educational Implications
Although many biobanks currently adopt broad consent, this study suggests that it is necessary to reconsider what kind of “broad” consent is ethically and socially appropriate. Furthermore, this study reveals the practical importance of concepts, such as trust, reciprocity, and solidarity, for donors, which have received little attention to date. Those involved in the management of biobanks need to understand these points and consider how these concepts can be incorporated into specific governance measures.
Research Agenda
This study found that specific social concepts were practically relevant as a basis for the biobank's governance and sustainability. In the future, research must clarify the specific governance policies that should be implemented following our study results. In addition to theoretical studies, an empirical approach will be beneficial. Several studies have addressed this matter based on the theory of deliberative democracy, which seeks appropriate governance models and its principles through exchanges of opinions among different social groups in some countries (Garrett et al., 2015; McWhirter et al., 2014; O’Doherty et al., 2011). The authors’ future work will include this empirical approach to sufficiently consider Japanese perspectives.
Conclusion
This quantitative study examined two hypotheses: (1) narrower and limited broad consent are more accepted by the public and (2) acceptance rates for broad consent increase in the presence of established measures related to biobank governance. The data and analyses supported both hypotheses, which implies that the limited type of broad consent must be considered an important option, as well as the relevance of the governance in promoting trust, reciprocity, and solidarity.
Footnotes
Acknowledgements
We would like to thank De Vries et al. for permitting us to use their framework of categorization of broad consent in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the grant from the Japan Agency for Medical Research and Development (AMED) under Grant Number 15653106 and JP20dm0107567.
Ethics Approval
The study protocol was approved by the ethics committee of the Graduate School of Medicine and Faculty of Medicine, the University of Tokyo (2019029NI).