
Abstract
Introduction
Historically, some of the worst abuses of human research participants have involved populations which are vulnerable to coercion, harm, or exploitation, such as prisoners, children, people with impaired decision-making capacity (DMC), gravely ill people, and minoritized and socioeconomically disadvantaged individuals (Resnik, 2018). The Belmont Report, an influential document that provided a conceptual foundation for revisions of federal human research policies in 1981 and 1991, states that: One special instance of injustice results from the involvement of vulnerable subjects. Certain groups, such as racial minorities, the economically disadvantaged, the very sick, and the institutionalized may continually be sought as research subjects, owing to their ready availability in settings where research is conducted. Given their dependent status and their frequently compromised capacity for free consent, they should be protected against the danger of being involved in research solely for administrative convenience, or because they are easy to manipulate as a result of their illness or socioeconomic condition (National Commission, 1979, p. 7).
The Report clearly indicates that the principal of justice requires additional protections for vulnerable research participants. The 1991 revisions of the Common Rule (45 CFR 46) reflect this protectionistic philosophy and include additional protections for vulnerable groups, including protections pregnant women, fetuses, neonates (subpart B); prisoners (subpart C); and children (subpart D) (Department of Health and Human Services, 2017). The Common Rule also state that “When some or all of the subjects are likely to be vulnerable to coercion or undue influence, such as children, prisoners, individuals with impaired decision-making capacity, or economically or educationally disadvantaged persons, additional safeguards have been included in the study to protect the rights and welfare of these subjects (45 CFR 46.111b).” 1
Since the 1990s, the categories of “vulnerable” populations discussed in the bioethics and health policy literature have expanded beyond those with special protections under the Common Rule to include people with impaired DMC (Council for the International Organizations of Medical Sciences, 2016; National Bioethics Advisory Commission, 1998), people who are seriously ill (Menikoff, 2009), people with limited English proficiency (Resnik & Jones, 2006), employees (Resnik, 2016), military personnel (Moskop, 1998), students (Resnik, 2024), socioeconomically disadvantaged people (Macklin, 2003), victims of natural disasters (Council for the International Organizations of Medical Sciences, 2016; Ferreira et al., 2015), elderly people (Sanchini et al., 2022), members of racial and ethnic minority groups (Rogers & Lange, 2013), and Native American and indigenous peoples (Minaya & Roque, 2015).
While policies that provide additional safeguards for vulnerable research participants appear to be well-intended, commentators have argued that, in some respects, they have harmed the very groups they were designed to protect (Friesen et al., 2023; Lyerly et al., 2008; Mastroianni & Henry, 2024; Ross, 2008). Physicians, scientists, and bioethicists have argued that policies that protect fetuses have discouraged enrollment of pregnant and non-pregnant women in clinical trials, which has substantially impeded research on these populations (Dresser, 1992; Little et al., 2024; Lyerly et al., 2008). For example, about 75% of drugs administered in pregnancy are prescribed on an off-label basis (Herring et al., 2010; Mastroianni & Henry, 2024). Likewise, pediatricians and bioethicists have raised similar concerns about the lack of inclusion of children in clinical research (Ross, 2008), which has resulted in off-label prescribing rate for children of about 35% (Allen et al., 2018). Beginning with the protests by AIDS activists for access to clinical trials and experimental therapies in the mid-1980s, the policy debate about vulnerable populations in research has shifted from exclusion/protection to inclusion/access (DeCormier Plosky et al., 2022; Dresser, 2001; Friesen et al., 2023; Mastroianni & Henry, 2024; Mastroianni & Kahn, 2001; Ouelette, 2024; Rios et al., 2016).
Additionally, some commentators have criticized the notion of a “vulnerable” population as inherently stigmatizing and vague and argued that it should be replaced with a different term (or several different terms) or eliminated entirely (Garrett & Altman, 2024; Levine et al., 2004; Little et al., 2024; Solomon, 2013; ten Have, 2015).
Although there has been considerable philosophical and ethical debate about vulnerable populations, there have been only a handful of empirical studies on vulnerable population policies. Some noteworthy studies include:
Wolf et al. (2005) analyzed the guidance for pediatric research available on websites from institutional review boards (IRBs) at 39 of the top-funded U.S. biomedical research institutions. Resnik and Jones (2006) analyzed policies pertaining to research subjects with limited English-proficiency at 30 of the top-funded U.S. biomedical institutions research institutions. Gong et al. (2010) surveyed 104 randomly selected U.S. IRBs concerning their practices concerning the use surrogate decision-makers for adults with impaired decision-making. Bracken-Roche et al. (2017) examined the concept of vulnerability in five national and six international policies and guidelines, including a discussion of the definition of vulnerability, its application to specific cases, and its moral justification. McMillan (2020) analyzed policies pertaining to research subjects with limited English-proficiency at 30 of the top-funded U.S. biomedical institutions research institutions.
The goal of our study was to fill in gaps in the literature on IRB policies pertaining to vulnerable (or complex) populations. Our specific aims were to 1) obtain cross-sectional data on the types of vulnerable populations at top-funded U.S. research institutions; and 2) determine whether having a policy on a specific type of population (e.g., children, employees, etc.) is associated with institutional characteristics, including Association for Accreditation of Human Research Protection Programs (AAHRPP) accreditation, research and development (R &D) expenditures, U.S. geographic region, and public vs. private status.
Methods
We attempted to access IRB policies on websites from the 100 top academic institutions ranked by R & D expenditures for 2022, the most recent year available for which data were available (National Science Foundation, 2024). We did not include an institution if we could not access its policies. We located policies on institutional websites by 1) searching for sections specifically dedicated to IRB policies on “vulnerable populations,” “special populations,” or related terms; 2) searching for general IRB policies (including policies on informed consent) or standard operating procedures and looking for policies mentioning “vulnerable populations,” or specific populations, such as “children,” “pregnant people,” and so on; 3) using internet search engines to locate policies when we could not readily find them by manually searching for them on institutional websites. We obtained public vs. private status information from common knowledge and internet searches. We selected R & D expenditure rank, public vs. private status, and U.S. census geographic region as variables of interest for institutional characteristics because research has shown that these variables have been associated with policy development (Resnik et al., 2014; Terlizzi & Cohen, 2023). We chose AAHRPP (2024) accreditation as a variable of interests because we hypothesized that accreditation is likely to influence policy development, since AAHRPP reviews and evaluates human research protections policies and standard operating procedures as part of its accreditation process.
We used deductive and inductive methods to develop our framework for coding the policies (Bradley et al., 2007). The framework based on 1) reading the background literature on vulnerable populations and 2) an initial examination of the policies. We refined the coding framework during the coding process to account for groups not initially included in the framework. We coded the policies according to whether they had policies [yes or no] pertaining to 14 different types of populations. Two members of the research team, EA and IJ, independently accessed, read, and coded the policies and then resolved disagreements. Data collection and coding took place from April to June 2024.
We used logistic regression analysis to assess the association between the institutional criteria (AAHRPP Accreditation, public vs. private status, geographic region and R&D expenditure rank) and each coding category for policies in turn. Linear regression was used to evaluate the association between the institutional criteria and total number of policies. P-values <0.05 were considered as statistically significant.
Results
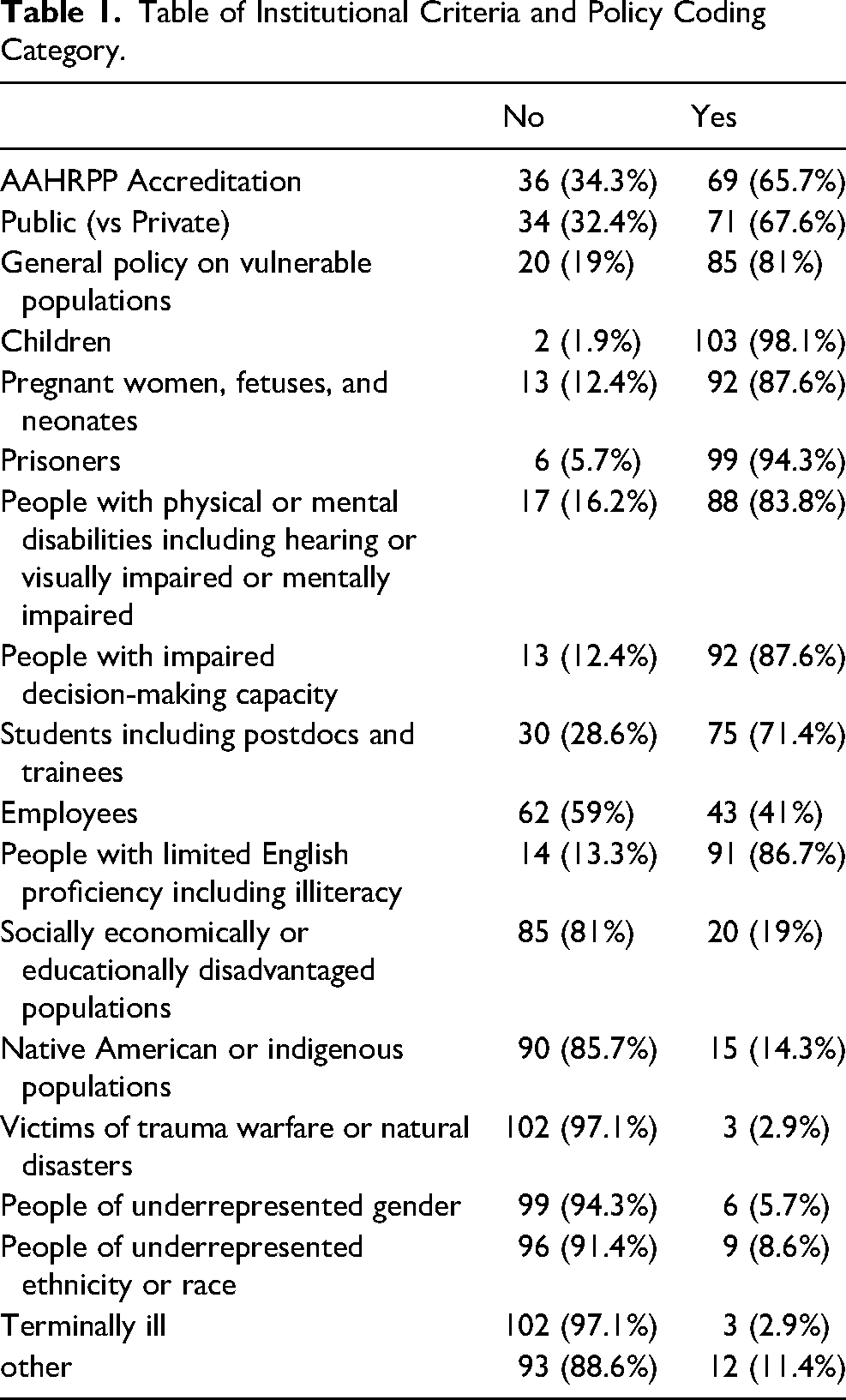
We excluded 24 institutions due to inability to access their IRB policies. We coded policies from 105 institutions instead of the targeted 100 because we coded 5 additional institutions by mistake. 65.7% of the institutions had AAHRPP accreditation and 34.3% did not. 67.6% were public and 32.4% were private. The geographic breakdown was South (39%), Northeast (23%), West (19%), and Midwest (19%). 81% had a general policy on vulnerable populations Policies concerning specific populations including children (98.1%); pregnant women fetuses and neonates (87.6%); prisoners (94.3%); people with physical or mental disabilities including hearing or visually impaired or mentally impaired (83.8%); people with impaired DMC (87.6%); students including postdocs and trainees (71.4%); employees (41%); people with limited English proficiency including illiteracy (86.7%); socially economically or educationally disadvantaged populations (19%); Native American or indigenous populations (14.3%); people of underrepresented ethnicity or race (8.6%); people of underrepresented gender (5.7%); victims of trauma warfare or natural disasters (2.9%); terminally ill people (2.9%); other (11.4%), including subjects with HIV, subjects in severe pain, subjects in long-term care facilities, the elderly, and researchers as subjects (i.e., self-experimentation). See Table 1. The average number of policies was 7.91 (range 2–13).
Table of Institutional Criteria and Policy Coding Category.
AAHRPP accreditation was significantly positively associated with having a general policy on vulnerable population (p = 0.004); policy on pregnant women fetuses and neonates (p = 0.015); prisoners (p = 0.015); people with physical or mental disabilities including hearing or visually impaired or mentally impaired (p = 0.0033); people with impaired DMC (p = 4.2 × 10−46); employees (p = 0.011); people with limited English proficiency including illiteracy (p = 0.005); and socially economically or educationally disadvantaged populations (p = 0.018). Public status was positively associated with having a policy for people with limited English proficiency including illiteracy (p = 0.05) and negatively associated with have a policy for employees (p = 0.056). See Table 2. Funding ranking was slightly negatively associated with having a policy pregnant women fetuses and neonates and people with limited English proficiency including illiteracy, but odds ratios were close to 1. Geographic Region was significantly associated with having a policy for Native American or indigenous populations (p = 0.013), with institutions in the South less likely to have such a policy compared to institutions in the West. See Table 2.
Results of Regression Analysis of Association Between Institutional Criteria and Each Coding Category in Turn. Only Significant Associations (P < 0.05) are Shown.
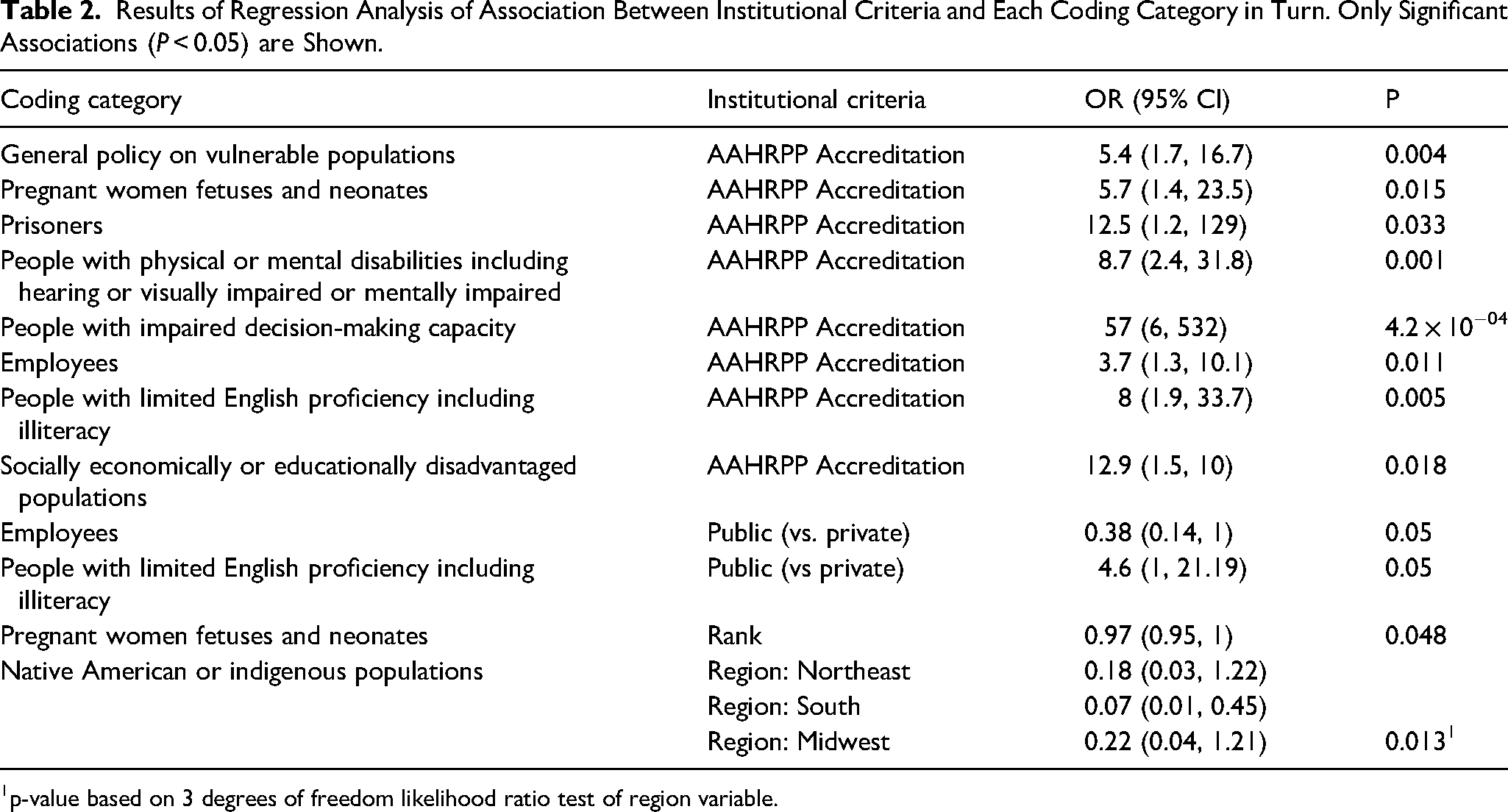
p-value based on 3 degrees of freedom likelihood ratio test of region variable.
Discussion
Our research indicates that academic institutions have a variety of policies for research with vulnerable populations. We collected data on policies for 14 different types of populations. Every institution in our sample had at least 2 policies for research with vulnerable populations (including a general policy) and most had 8 or more. As expected, the most highly prevalent policies pertained to populations covered in subparts B, C, and D of the Common Rule (pregnant women, fetuses, neonates, prisoners, and children) but other groups were well-represented, including people with disabilities; people with impaired DMC; students/trainees; and people with limited English proficiency.
As expected, AAHRPP accreditation predicted having a general policy on vulnerable population, and policies pertaining to pregnant women fetuses and neonates; prisoners; people with physical or mental disabilities including hearing or visually impaired or mentally impaired; people with impaired decision-making capacity; employees; people with limited English proficiency including illiteracy; and socially economically or educationally disadvantaged populations. The positive association between accreditation and human research policy development suggests that accreditation can play an important role in protecting vulnerable (and non-vulnerable) populations involved in research (Hurley, 2024). We make this statement not as an endorsement of AAHRPP but as an observation concerning the result of our data analysis.
Geographic region was a significant predictor of having policy that addresses research with Native American or indigenous populations, with institutions in the South less likely to have such policies as compared to those in the West. A plausible explanation for this association is that institutions located in areas close to Native American reservations are more likely to develop policies to address ethical concerns related to research with these populations than institutions which are not near Native American reservations. 8/15 (53.3%) of the institutions with such policies were from the West. These institutions included Arizona State University, University of University of Arizona, University of California at Santa Barbara, University of New Mexico, University of Southern California, University of Utah, University of Washington, and Washington State University.
Limitations
Our study has several limitations. First, our sample was drawn from U.S. research institutions, so it is not generalizable to other countries. Second, we did not interview human research protection officials about their IRB policies, so we did not obtain information about the institutional, social, or cultural factors that may have influenced policy development. Third, we did not analyze policies related to specific vulnerable populations. As noted above, some researchers have done this kind of analysis for children (Wolf et al., 2005) and people with limited English proficiency (Resnik & Jones, 2006). We are planning to do some of this analysis in two future sub-studies that are part of a larger project, including a sub-study on policies for enrolling people with impaired or questionable decision-making capacity, and a sub-study on enrolling pregnant women. We encourage other researchers to address topics and the questions not covered answered by our study.
Research Agenda
Future research on vulnerable populations should address the questions not answered by our study, such as the kind of protections extended to different types of populations and the factors that influence policy development.
Educational Implications
Education in human research ethics should include discussion not only of the ethical issues related to research with vulnerable populations (such as protection vs. access) but also the variety of policies adopted by research institutions.
Best Practices
Academic institutions should consider developing policies for vulnerable populations to address specific issues arising research undertaken by faculty.
Conclusion
U.S. academic institutions have a variety of policies for research with vulnerable populations. Additional research is needed to better understand the types of safeguards that institutions have adopted to protect vulnerable populations and the factors that influence policy development.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Environmental Health Sciences (grant number ZIAES-102646-10). The research was funded by the National Institute of Environmental Health Sciences, National Institutes of Health. It does not represent the views of the NIEHS, NIH, or US government.