
Abstract
Self-experimentation is a research practice that might advance scientific progress and benefit populations worldwide. However, it also carries risks, both in terms of potential harm to researchers and the possibility of undermining research. This study seeks to explore expert perspectives on self-experimentation, examining its potential benefits and risks, identifying areas of consensus and divergence, and highlighting key themes to inform debates on its role in medical research.
We conducted a three-round online Delphi study with a multi-regional panel of 16 experts with varying views on self-experimentation. The panel assessed, commented on, and proposed revisions to statements drafted by both the authors and panellists.
Consensus was reached on several key points. Experts agreed that self-experimentation can serve as a means of gathering preliminary evidence, accelerating research, and assessing the technical feasibility of an intervention. However, there was also agreement that self-experimentation can harm scientists, has limited scientific value, and may produce unreliable data.
Background
In the quest to advance medical research, it is worth exploring the potential of research practices that may be useful in achieving scientific progress and benefiting populations worldwide (Benatar, 2000). One such practice is self-experimentation, a research practice that gained remarkable prominence during the COVID-19 pandemic, when scientists in the Americas, Europe and Asia began conducting self-experiments to develop a vaccine against the virus (Manríquez Roa & Biller-Andorno, 2024; H. Murphy, 2020; Regalado, 2020).
Before the institutionalisation of research on human subjects and the establishment of research ethics regulations in the mid-twentieth century, self-experimentation was a generally accepted scientific practice in medical research (Manríquez Roa & Biller-Andorno, 2020). The Nuremberg Code, however, reflects a shift in this context, laying the foundation for modern research ethics and establishing voluntary, informed consent and the protection of research participants. Its only reference to self-experimentation concerns high-risk research, pointing to the idea that it should not be subject to the same risk limits that govern standard forms of research (Pugh et al., 2025):
‘No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects.’ (World Medical Association, 1947).
Today, self-experimentation is often undertaken without public or institutional oversight (Hanley et al., 2019). It is not addressed in key research ethics regulations, such as the Declaration of Helsinki; its legal status is unclear, and its potential benefits and risks are a matter of debate (Manríquez Roa & Biller-Andorno, 2020; Manríquez Roa & Biller-Andorno, 2024). While it is difficult to establish how much self-experimentation is being carried out in the present, literature and online platforms that connect self-experimenters point out that this research practice is used in most regions of the world (Hanley et al., 2019; Open Humans, 2023; RADVaC, 2022; ScienceDirect, 2023).
We understand self-experimentation in a narrow sense: as a research practice in which trained scientists design a study and conduct experiments on themselves voluntarily with the goal of generating knowledge. 1 Self-experimentation has generated valuable knowledge in the last decades (Weisse, 2012) and scientists have been awarded Nobel prizes because of findings obtained through self-experiments (Hanley et al., 2019). Self-experimentation has been used to test research ideas that initially found resistance amongst scientific communities (e.g., the link between Helicobacter pylori and peptic ulcers described by Barry Marshall) (Nobel Prize Outreach AB, 2023), to test the technical feasibility of research interventions (Ackerman et al., 1988), to promote agility in the research process (Estep & Church, 2020), to enable the formulation of new hypotheses (Rammensee et al., 2021), and for educational purposes (Dresser, 2013). However, self-experimentation carries significant risks, including scientific inadequacy due to the lack of proper controls, the potential for investigator bias when assessing the effects on oneself (Davis, 2003), and the possibility that the risks may outweigh potential benefits (Caplan & Bateman-House, 2020; Guerrini et al., 2020).
This study is a pioneer in gathering an international panel of experts with heterogeneous views on self-experimentation. Considering the secrecy that surrounds self-experimentation and the lack of systematic evidence on this research practice in the last decades, we conducted an online Delphi study to generate new data while offering panellists the option of permanent anonymity – though ultimately, this provision proved unnecessary. The empirical findings obtained are expert opinions and do not necessarily represent normative views that are predominant or with which the authors agree. To our knowledge, this study is the first attempt to discuss with experts whether and why self-experimentation is a valuable research practice, and to identify the key considerations for conducting self-experiments if they are to be regarded as standard research in humans.
The findings of this study allowed the research team to analyse consensus ideas of the panel on the benefits and risks of self-experimentation and propose six cross-cutting themes to advance in normative analyses and policy debates on self-experimentation in medical research. This Delphi study is the exploratory part of a larger research project on self-experimentation.
Methods
First, we conducted a literature search in English and Spanish to map arguments concerning self-experimentation, focusing on media reports in newspapers and blogs, online forums, grey literature, public statements, and academic articles in electronic databases (PubMed, Google Scholar and specialised journals). Second, we organised the webinar ‘Self-Experimentation in Times of Covid-19’ (Forum for Global Health Ethics, 2020) and used it as an exploratory tool to understand competing arguments on self-experimentation. Third, we convened a panel of 16 experts and conducted an online Delphi study between September and December 2022 to seek convergence of views, identify divergence, and understand the benefits and downsides of the practice of self-experimentation.
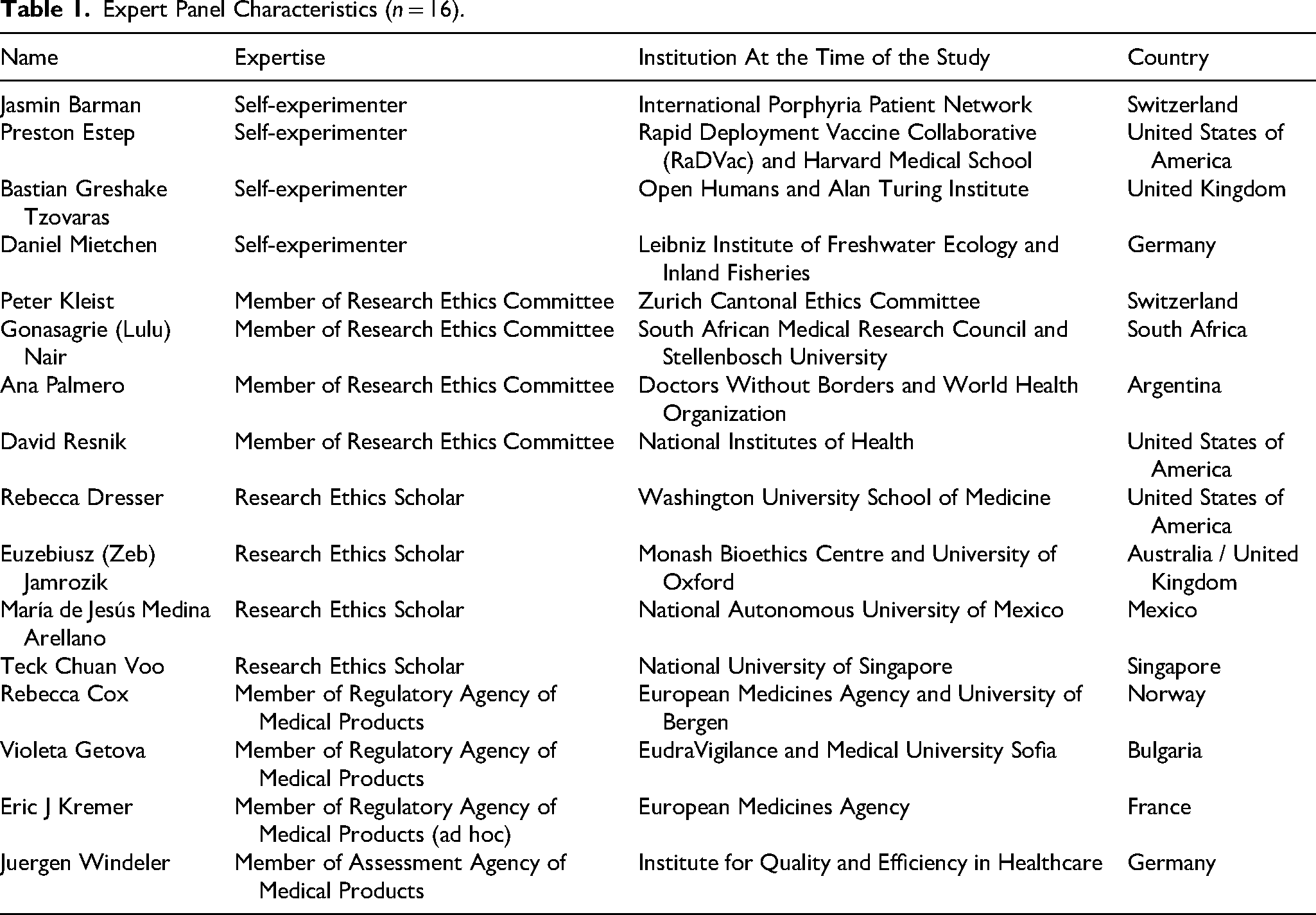
Table 1 shows the expert panel. All experts participated in their professional capacity and not representing their institutions. The panel was formed using purposive sampling to gather the experts: four self-experimenters, four scholars with expertise in research ethics, four members of research ethics committees, and four members of regulatory and assessment agencies of medical products. The experts, from 12 different countries, hold diverse views on self-experimentation – some are firmly in favour, others resolutely opposed, while many occupy more nuanced positions. The panel included five experts who had either publicly expressed support or conducted scientific self-experiments, four experts whom the authors believed to be opposed to the practice (some of whom had publicly spoken against it), and seven experts whose positions were unknown to us. The panel members were identified during the literature search. The composition of the panel was not disclosed to the experts until the end of the last round to ensure anonymity during the fieldwork of the Delphi study and prevent that a few participants monopolised the discussion. Experts from the following countries were invited but declined to participate or did not reply: Austria, Brazil, China, Ghana, Denmark, Japan, Kazakhstan, Peru, Portugal, Russia and Spain.
Expert Panel Characteristics (n = 16).
Data Collection Process – Rounds
This Delphi study comprised three rounds in which participants were asked to reflect and comment on pre-defined statements written by the authors of this study based on our literature search and webinar discussions (Round 1), on pre-defined statements modified following suggestions of the panel (Rounds 2 and 3), and on statements suggested by the panel (Round 3). Please note that some of the statements are descriptive, reflecting current views and practices surrounding self-experimentation, while others are normative, seeking to establish a common understanding of how self-experimentation should be approached.
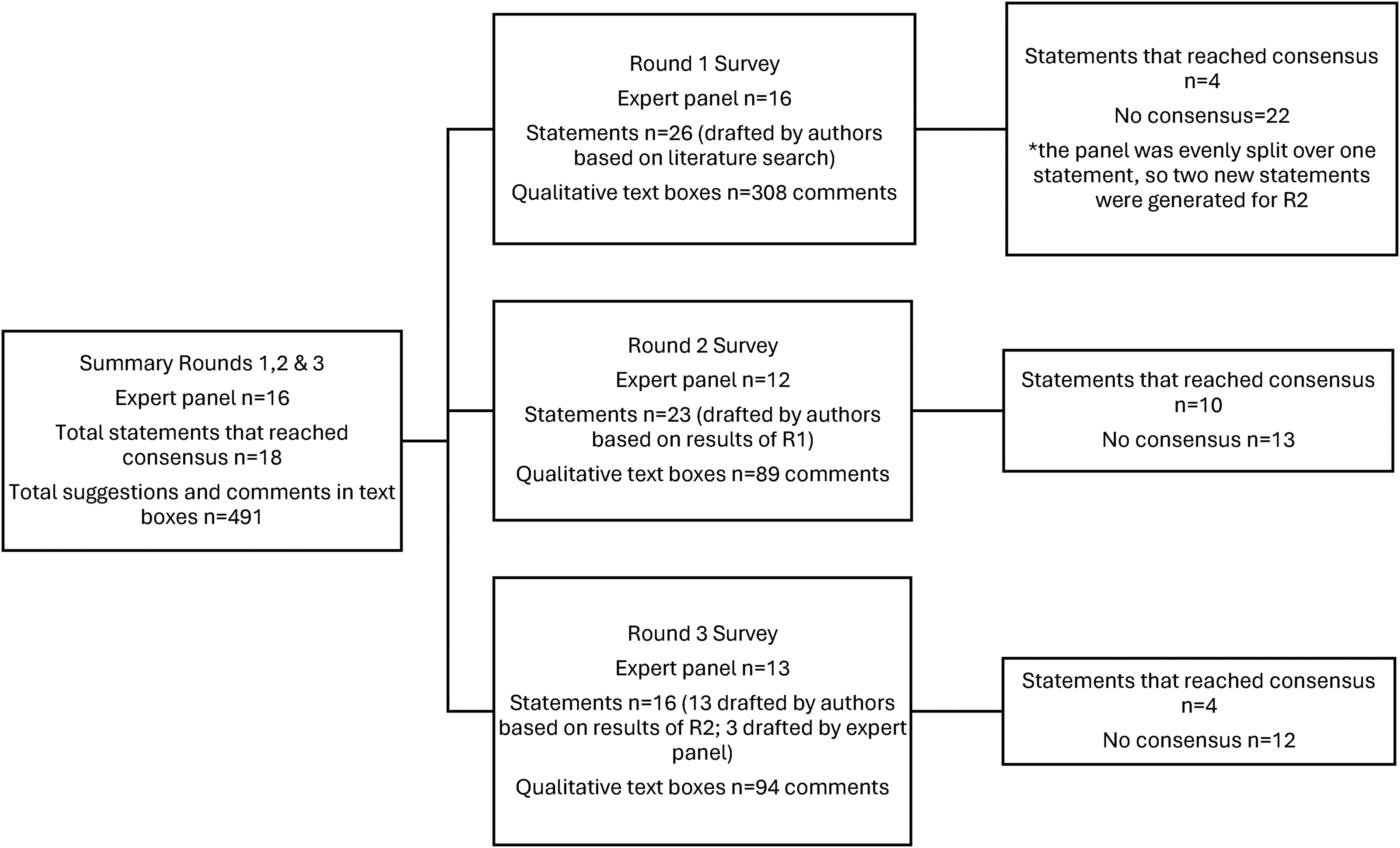
Figure 1 presents a summary of the data collection process.
Delphi digital data collection.
The statements presented in the rounds were organised in four sections: the delimitation of self-experimentation; arguments in favour of self-experimentation; arguments against self-experimentation; and the role of ethics committees and regulatory agencies. In each round we asked participants to express their level of agreement or disagreement with each statement using a 5-point Likert-scale, and to comment on the statements. Additionally, in Round 1 (R1) and Round 2 (R2) we asked participants to make suggestions to modify the statements. At the end of each round, we sent experts a document with the results, including the levels of agreement and disagreement of the panel with each statement (highlighting the statements that reached consensus), and the comments and suggestions of all experts. After R1 and R2, we asked experts to reflect on the results and reconsider their views for the next round, emphasising that they did not need to conform.
Moreover, in Round 1 we asked experts to suggest new statements if they thought there was a relevant topic concerning self-experimentation that was missing. In Round 2 we included a list with the new statements suggested by the experts (n = 4) and asked them to vote if they wanted to include them to be discussed in the last round. The three statements that reached a simple majority were added for discussion in Round 3 in a separate section.
Results
This international consensus study produced a total of 65 statements (26 in Round 1, 23 in Round 2, and 16 in Round 3), along with 491 comments and suggestions relating to self-experimentation. The complete set of statements is presented in Table 2, while the comments and suggestions are provided in the annex for reference. In the following, we highlight the principal findings, focusing on the statements that reached consensus and those that generated broad disagreement amongst panellists. It should be noted that some expert views diverge from current general ethical standards for human research.
Overall Results Delphi Study on Self-Experimentation.

SA, strongly agree; A, agree; NAD, neither agree nor disagree; D, disagree; SD, strongly disagree; Comb A, combined agreement (strongly agree + agree); Comb D, combined disagreement (strongly disagree + disagree); N, total number of responses.
Views of Consensus
A total of 18 statements reached consensus understood as combined agreement, this is, ≥75% of the panellists agreed or strongly agreed with them (4 statements in R1; 10 statements in R2; 4 statements in R3). The consensus threshold of ≥75%, together with the composition of our panel (12–16 members per round, with at least two representatives from each group), meant that any statement reaching consensus was endorsed by experts from at least three of the four constituent groups, with members of at least three stakeholder groups expressing agreement or strong agreement in every instance. Table 3 presents all consensus statements on self-experimentation.
Statements that Reached Consensus.
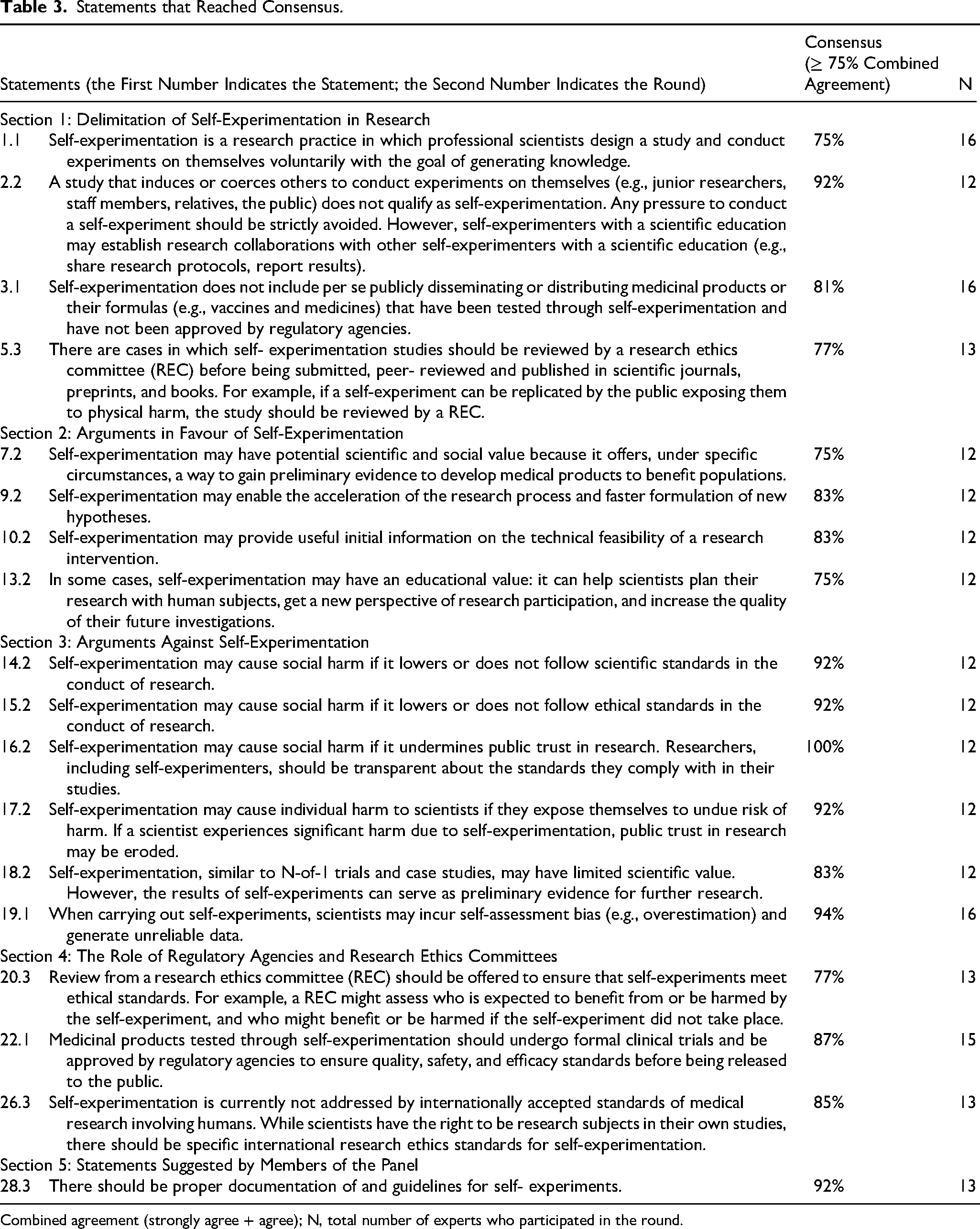
Combined agreement (strongly agree + agree); N, total number of experts who participated in the round.
According to experts, the main points regarding the delimitation of self-experimentation include the following key criteria: the voluntariness of the scientists who conduct self-experiments, the goal of knowledge generation, and the possibility of collaboration amongst self-experimenters with a scientific education. In a more nuanced understanding of self-experimentation, the panel reached consensus on two points: self-experimentation must comply with the provision of not pressuring, inducing or coercing others to conduct experiments on themselves, and it does not include publicly disseminating products or formulas that have not been approved by regulatory agencies. Notably, consensus was reached on the point that in some cases, self-experiments should be reviewed by a REC before submission for publication.
The panel acknowledged four points of consensus on the potential value of self-experimentation: (1) it can offer under specific circumstances (yet to be discussed), a way to gain preliminary evidence to develop medical products to benefit populations; (2) it may enable the acceleration of research and faster formulation of new hypotheses; (3) it can provide information on the technical feasibility of a research intervention; (4) and it may have an educational value for scientists. Two topics were highly controversial: whether self-experimentation may be useful in the context of a public health emergency, or to improve access to medical products. Moreover, the panel reached consensus on six statements against self-experimentation: it may cause social harm (1) if it lowers or does not follow scientific standards 2 ; (2) if it lowers or does not follow ethical standards; and (3) if it undermines public trust in research. Self-experiments may also (4) harm scientists if they expose themselves to undue risks; (5) have limited scientific value; and (6) lead scientists to incur self-assessment bias and generate unreliable data. Because we examined the potential benefits and risks of self-experimentation separately, this study does not capture expert views on the overall balance between benefits and risks, or on whether the risks outweigh the benefits.
Although there was disagreement regarding the roles of RAs and RECs, consensus was reached on two points: review from a REC should be offered to ensure that self-experiments meet ethical standards; and medical products tested through self-experimentation should undergo clinical trials and be approved by RAs. Additionally, the panel agreed on two other matters: there should be specific international research ethics standards for self-experimentation, and there should be documentation of and guidelines for self-experiments. 3
Views of Broad Disagreement
Throughout the study, three statements generated broad disagreement amongst the panel, this is ≥50% of the panellists disagreed or strongly disagreed (2 statements in R1; 1 statement in R2). Although our study shows relatively few points of disagreement, they may be valuable aspects to consider as controversial areas in future policymaking concerning self-experimentation. These statements are presented in Table 4.
Statements that Generated Broad Disagreement.
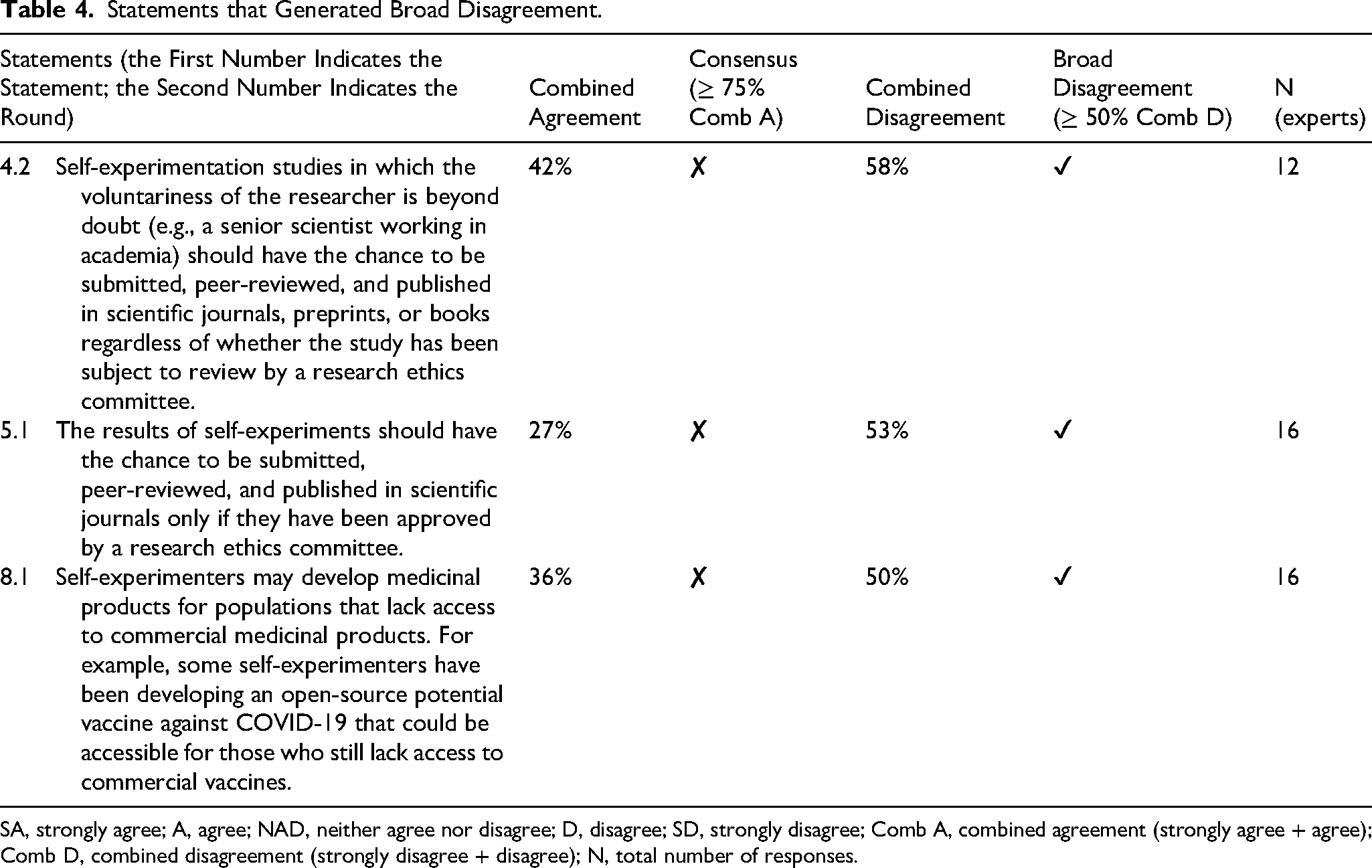
SA, strongly agree; A, agree; NAD, neither agree nor disagree; D, disagree; SD, strongly disagree; Comb A, combined agreement (strongly agree + agree); Comb D, combined disagreement (strongly disagree + disagree); N, total number of responses.
Two of the statements that generated broad disagreement refer to the role of RECs regarding the submission, peer-review process and publication of self-experimentation studies and their results. On the one hand, the panel of experts strongly disagreed with the idea of the results of self-experiments having the chance to be submitted, peer-reviewed and published in scientific journals
Discussion
Based on the statements that reached expert consensus, we synthesised the main findings of this study into six cross-cutting themes that frame the discussion and explore current challenges of self-experimentation for medical research. The comments and suggestions of the experts – on statements that reached consensus, the ones that show broad disagreement, and the ones that did not reach consensus nor broad disagreement – inform these themes. Box 1 presents the themes.
Cross-Cutting Themes Based on Consensus Statements.
(1) Delimiting Self-Experimentation
A contentious subject for the panel was the definition of self-experimentation, with experts advocating for understanding self-experimentation either in a narrow or broad sense. In our view, one relevant distinction to advance in the standardisation of this research practice is to clarify whether the self-experimenter is a trained scientist. Literature shows that in a broad sense, self-experimentation may be understood as carried out by non-scientists – sometimes although not necessarily in collaboration with scientists – in projects involving citizen scientists (Guerrini et al., 2019), groups of patients (Kempner & Bailey, 2019; Vayena et al., 2016), members of the quantified-self movement (Swan, 2012), self-trackers, and others (Bains, 2008). In a narrow sense (the one that we refer to in this study), self-experimentation is conducted by scientists who aim to generate knowledge. However, the definition of scientist is not necessarily straightforward – it remains to be discussed whether people trained outside the natural sciences count as self-experimenters in a narrow sense. Another key point is to determine the extent to which reproducibility and systematicity are required to move from simply experimenting on oneself out of curiosity to formulating a hypothesis and testing its validity in an N-of-1 study.
(2) Deciding on Results
The findings of this study show that experts hold very different positions on how to treat and share the results of self-experiments, particularly regarding the status of those results in relation to the general conception of scientific data. Some experts argue that as long as self-experimentation studies follow research ethics standards (yet to be defined for self-experiments), the results should have the chance to be submitted, peer-reviewed and published in academic publications. Other experts consider this insufficient, primarily because self-experiments may produce unreliable data. Moreover, while some experts believe the results of self-experiments should be submitted, peer-reviewed and published in academic publications, regardless of whether the study has been approved by a REC, others strongly disagree. It is noteworthy that the panel reached consensus on the idea that scientists may report the results of their self-experiments with other scientists. The openness to exchange the results of self-experiments with peers but avoid the formal publication of them is an interesting point that needs to be further explored. Relatedly, the publication in the internet of the results of self-experiments and how to conduct them (e.g., open-source, citizen science, do-it-yourself initiatives) has strong supporters and detractors amongst experts and has raised regulatory and ethical questions in the literature (Guerrini et al., 2020; Ienca & Vayena, 2020; Wexler, 2015). The way in which the results of self-experiments are treated has important implications for minimising the risk of social harm, safeguarding public trust, rethinking the role of research ethics committees (RECs) and regulatory authorities (RAs), and shaping ethical standards for self-experimentation. On the one hand, publishing online instructions on how to self-manufacture and self-administer a DIY vaccine during a pandemic, based on findings from self-experiments, could endanger public health and signal a lowering of standards, thereby potentially undermining public trust in vaccines (Guerrini et al., 2020). On the other hand, the publication of a case report in which a virologist successfully used an experimental form of oncolytic virotherapy to treat her own recurrent breast cancer may be morally justified (Pugh et al., 2025).
(3) Minimising the Risk of Social Harm While Safeguarding Public Trust
The literature on self-experimentation highlights that this practice may cause social harm in several ways (Caplan & Bateman-House, 2020; Guerrini et al., 2020; London & London, 1997). For example, a self-experiment that can be replicated by the public may expose individuals to physical harm, a scientist who catches an infectious disease through a self-experiment might spread it to others and harm them, or a scientist who bio hacks his genes through a self-experiment might pass potentially harmful mutations to their offspring (Zettler et al., 2019). Relatedly, our panel reached consensus on identifying three scenarios in which self-experimentation may cause social harm in other ways: if it lowers ethical standards, if it lowers scientific standards, or if it undermines public trust in research. The current lack of guidance to conduct self-experiments, and the fact that self-experimentation is often not regulated, may increase the risk of social harm.
Public trust appeared as a prominent topic connected to self-experimentation in the experts’ comments and suggestions. To unpack the risk of undermining public trust in research, we believe it is relevant to distinguish between the practice of self-experimentation in itself and sharing the results and procedures of self-experiments with the public. There is extensive literature that tackles cases in which sharing the results and procedures of self-experiments and DIY initiatives might undermine trust and presents arguments against sharing them with the public (Caplan & Bateman-House, 2020; Guerrini et al., 2020). It is worth noting that what these arguments show is that non-evidence-based claims sow mistrust of science and public health (Caplan & Bateman-House, 2020), regardless of the research practice used to back those results. However, the need to safeguard public trust remains an open issue, particularly in the context of self-experimentation. In this regard, proponents of self-experimentation argue that this research practice can help to build public trust, as it demonstrates researchers’ genuine commitment to the pursuit of knowledge (Dresser, 2014).
(4) Discussing Reasonable Risks
Our findings suggest that self-experimentation adds a new dimension to discussions on (un)reasonable risk of harm in research (Resnik, 2011). On the one hand, some scholars oppose self-experimentation in cases where there is an undue risk of harm to individual self-experimenters (Davis, 2003). Additionally, training scientists is costly and often subsidised by public resources, so if they were to fall seriously ill, this could also result in harm to society. On the other hand, arguments that emphasise individual freedom assert that it is not justifiable to prohibit self-experimentation (Pugh et al., 2021). These arguments rest on the premise that as long as self-experiments are conducted voluntarily and do not pose a risk of harm to others, they should be permitted – regardless of whether the expected harms outweigh the expected benefits, this is, irrespective of whether self-experimenters expose themselves to ‘reasonable risks’ (Pugh et al., 2021). However, a fundamental principle of medical research involving human subjects is that it may only proceed if the importance of the objective outweighs the risks to participants (World Medical Association, 2022). If self-experimentation is to comply with this requirement, then liberal arguments alone are insufficient (Pugh et al., 2021).
Interestingly, our expert panel reached consensus on the following: ‘Self-experimentation may cause individual harm to scientists if they expose themselves to undue risk of harm. If a scientist experiences significant harm due to self-experimentation, public trust in research may be eroded’ (Statement 17, Round 2). This statement suggests that opposition to unreasonable risks in self-experimentation comes not only from those who uphold the fundamental principle that research should only be conducted when its objectives outweigh the risks to participants, but also from those who believe that self-experimenters taking unreasonable risks may cause wider social harm by undermining public trust in research.
(5) Rethinking the Role of Research Ethics Committees (RECs) and Regulatory Agencies of Medical Products (RAs)
Although our panel reached consensus on the idea that review from a REC should be offered to ensure that self-experiments meet ethical standards, it is unclear whether RECs are prepared to actually offer an ethical review of self-experiments – assuming this takes place in jurisdictions in which self-experimentation is not illegal. Interestingly, the panel showed mixed views on whether a review from a REC should be required, and on whether RECs or self-experimenters are well positioned to determine when, how and who should participate in a self-experiment. Experts reached consensus on the idea that self-experimentation studies should, in certain cases, be subject to review by a Research Ethics Committee (REC). Specifically, consensus was achieved on the notion that studies warrant REC review when a self-experiment could, if replicated by members of the public, expose them to physical harm (see Statement 5.3).
Some contentious points regarding the role of RAs amongst the experts in our study were whether such institutions should recognise or support self-experimentation, if they should provide guidance to self-experimenters, whether they should determine what kinds of self-experimentation studies require review from a REC, or if an adapted or specific regulatory mechanism should be developed to mitigate the risks of harm associated to self-experimentation studies, maximise their potential benefits, and ensure the scientific quality and ethical acceptability of research. In fact, some self-experiments would be illegal in certain jurisdictions if they violate required risk-mitigation plans (e.g., genetically modified organisms, class 2 + pathogens, radiation). Although our expert panel reached consensus on the idea that medical products tested through self-experimentation should undergo clinical trials and be approved by RAs, it remains to be discussed whether these processes can be the same as they are for other kinds of research, or if adapted, new or hybrid models could be best suited. A key point to reflect on is whether self-experimenters should follow current principles in research ethics or if such principles should be different or understood in a different way. A related open question is what the procedure should be if scientists do not register their self-experiments.
(6) Setting Ethical Standards
Experts reached consensus on three points relevant to the discussion on the development of ethical standards for self-experimentation: • ‘(…) Researchers, including self-experimenters, should be transparent about the standards they comply with in their studies’ (Statement 16, Round 2). • ‘(…) While scientists have the right to be research subjects in their own studies, there should be specific international research ethics standards for self-experimentation’ (Statement 26, Round 3) • ‘There should be proper documentation of and guidelines for self-experiments’ (Statement 28, Round 3).
Limitations
Although reporting guidelines for Delphi studies in health research vary widely and there are no common applicable criteria (Spranger et al., 2022; The Equator Network, 2023), we followed the reporting recommendations of CREDES (Conducting and Reporting of Delphi Studies) (Jünger et al., 2017). One limitation of this study is that although the sample number is higher than the minimum threshold of 12 experts recommended for consensus studies (M. K. Murphy et al., 1998), it relies on the views of 16 experts whose views are not necessarily typical and who may not fully represent the wider expert community on self-experimentation. To minimise potential key informant bias, we employed a purposive sampling approach to recruit experts representing the broadest possible range of views on self-experimentation.
The composition of the Delphi panel varied across the three rounds of data collection. In Round 1, the panel comprised 16 experts. In Round 2, participation decreased to 12 experts, as two scholars, one representative from a regulatory agency for medical products, and one self-experimenter did not complete the exercise. In Round 3, 13 experts contributed responses, with one scholar, one member of a Research Ethics Committee (REC), and one self-experimenter not participating in that round. Such variations in the number of participants across Delphi rounds are frequently observed, and the overall consistency of participation across the three rounds suggests that the panel retained sufficient expertise and diversity to support the credibility of the findings. From a methodological perspective, the study accounted for these changes transparently and maintained the same criteria for consensus thresholds across all rounds, regardless of panel size.
One limitation of consensus-based methods, such as Delphi studies, is that disagreement with a given statement cannot be readily interpreted. Panellists may reject a statement in its entirety or only specific elements, such as its wording, underlying assumptions, or on conceptual or ethical grounds, and the method does not systematically capture these distinctions. Although some insight may be gained from optional comments and suggestions provided by participants, the interpretability of dissenting responses remains limited.
Another limitation is that we may have restricted views concerning two expert profiles because: (1) several self-experimenters declined to participate, possibly because this research practice is in grey legal zones, and (2) although we invited experts from regulatory and assessment agencies of medical products from four continents, we could only recruit experts based in Europe. Moreover, participation in this study was limited to English speakers, although the inclusion of experts from five continents gives our study a multiregional character.
Conclusions
This consensus study advances a multi-stakeholder perspective on self-experimentation, addressing its current challenges and outlining key considerations for how such experiments should be conducted if they are to be regarded as standard research in humans. These considerations are twofold: first, to harness the potential scientific and social value of self-experimentation by generating preliminary evidence that can inform the development of medical products benefiting populations; and second, to mitigate potential social harms, including undermining public trust in research and lowering ethical and scientific standards.
While expert stakeholders currently disagree on the roles that RAs and RECs should play in overseeing self-experimentation, they have reached consensus on two key points: first, that RECs should offer review to ensure self-experiments meet ethical standards; and second, that medical products tested through self-experimentation should undergo clinical trials and be approved by RAs. Notably, some expert views diverge from current general ethical standards for human research. Although specific standards for self-experimentation remain to be developed, research that fails to adequately protect the public and maintain trust in research poses serious risks.
We believe the results and discussion presented in this paper contribute to academic and policy debates on self-experimentation, particularly regarding two areas where expert consensus was reached: the establishment of international research ethics standards, and the development of documentation and guidelines for its responsible practice.
Educational Implications, Best Practices, and Research Agenda
Self-experimentation presents a number of valuable educational implications, particularly as a pedagogical tool for scientists. It has the potential to foster critical thinking and to enhance researchers’ understanding of the experiences of human participants in their studies. As a contribution to discussions on best practice, this study underscores the capacity of self-experimentation to generate novel insights and to refine research hypotheses. The findings also identify several key points of contention in self-experimentation, particularly concerning its ethical dimensions and its epistemological role within scientific research, and thereby delineate important directions for further inquiry.
Footnotes
Acknowledgments
TMR thanks the Digital Society Initiative at the University of Zurich for funding her doctoral research. The authors thank the 16 experts who formed the Delphi panel: Jasmin Barman, Rebecca Cox, Rebecca Dresser, Preston Estep, Violeta Getova, Bastian Greshake Tzovaras, Euzebiusz (Zeb) Jamrozik, Peter Kleist, Eric J Kremer, María de Jesús Medina Arellano, Daniel Mietchen, Gonasagrie (Lulu) Nair, Ana Palmero, David Resnik, Teck Chuan Voo, and Juergen Windeler. We are also grateful to the speakers of the webinar ‘Self-Experimentation in Times of Covid-19’: Rebecca Dresser, Preston Estep, Peter Kleist, and Samia Hurst-Majno. Some of the ideas expressed in this event were used in the development of statements for Round 1 of the Delphi study. This webinar took place on Dec 16, 2020 and was organised by the Forum for Global Health Ethics, an outreach project hosted by the Institute of Biomedical Ethics and History of Medicine at the University of Zurich (![]() ).
).
Ethical Approval and Informed Consent Statements
This research was approved by the Research Ethics Committee of the University of Zurich (CEBES Review Board) on 8 August 2022 (Reviewer: Markus Christen). No reference number. All panelists signed written consent forms to participate in this research and for the study to be published.
Author Contributions
TMR, FH, JM and NBA contributed to the design, conduct, and analysis of the findings of the research project. NBA was the PI of the study. TMR led the three rounds of the Delphi study, oversaw the analysis, and wrote the manuscript with inputs from all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors have no financial or non-financial conflicts of interest to disclose.
Data Availability Statement
The data that support the findings of this study are available as supplemental files.
Notes
Author Biographies
Research Interests
Research Interests
Julian's main research interests lie in the areas of biomedical innovation law, research ethics, and pharmaceutical pricing, with a particular focus on gene and cell therapies, AI in pharmaceutical R&D, and innovative therapies for rare diseases.
Research interests