
Abstract
Human biological samples are a valuable source of information that may aid in the generation of new knowledge. However, the use of human biological samples for research poses various ethical, legal and social issues (ELSI). We performed a scoping review to identify the ethical issues surrounding the use of human biological samples for research. We developed a search string strategy to identify literature in PubMed, Scopus, Web of Science, and Google Scholar. Out of 4067 identified articles, 61 articles were included for final analysis. The findings of this study revealed multiple ethical issues stemming from the knowledge and awareness of different stakeholders involved in research, the factors affecting donors’ study participation, the consent process, and the governance and structures of these human biological samples. This study will provide guidance for researchers, IRB members, and other stakeholders involved in the ethical consideration of using human biological samples for secondary research.
Keywords
Introduction
When patients visit their physicians for consultation or treatment, it is common for the physicians to collect patients’ information and medical history, and to request laboratory tests either for diagnostic or therapeutic interventions. (Vaught & Henderson, 2011). To perform a laboratory test, human biological samples, such as blood, urine, stool, and biopsies, are commonly obtained from patients. A laboratory test can be conducted locally, provided the institution has the necessary capacity (for example, certain machines and experts). If this capacity is lacking, the samples may be shipped to other institutions or countries. This was evident during public health emergencies when a large number of biological samples that were obtained from patients were sent to the chosen laboratory, which can do the test for confirmation following the guidelines issued by WHO (WHO, 2000). But what would happen to the leftover human biological samples, especially the remnants of human specimens collected for routine clinical care or analysis that would otherwise have been discarded (FDA, 2006), after the diagnostic purposes have been fulfilled? Some hospitals, especially teaching and academic institutions, store these biological samples (Chen et al., 2020), allowing other researchers to have access to them for secondary research.
Eikemo and colleagues defined secondary research as research using already collected data and biological samples (Eikemo et al., 2022). While human biological samples can be a valuable source of information for generating new knowledge, their use raises ethical concerns regarding respecting patients’ rights, particularly when samples were not originally collected for research purposes or obtained with explicit consent. Several empirical cases illustrate these ethical tensions. For example, the Michigan BioTrust for Health collected approximately 4 million samples from 1984 to 2009 without explicit consent for their biobank (Thiel et al., 2014). These samples could potentially have been exploited had the institution not subsequently established a governance mechanism to protect these samples. Similarly, a study in Hong Kong, examining the views and concerns about the long-term storage and secondary use of residual dried blood spots (rDBS) collected from newborn screening programs, found that although their use in medical research was generally accepted, most parents were unaware that these samples could be reused for research purposes (Hui et al., 2022). Such a lack of awareness may increase vulnerability among donors.
These examples emphasized the importance of a robust consent process. Healthcare professionals responsible for obtaining consent for the donation of biological samples should ensure that patients receive sufficient information regarding the potential secondary use of their samples, particularly for research purposes, and assess their understanding to ensure voluntariness. In the United States (US), a study examining patients’ attitudes and preferences towards the use of anonymous and identifiable human biological samples showed that patients want to be informed about the research, especially when the samples are identifiable (Hull et al., 2008). The study also found that donors were concerned about their privacy. Similar concerns have also been reported in low and middle-income settings. For example, a study conducted in Ghana and Kenya examined stakeholders’ perspectives on the ethical issues arising from the use of human biological samples and emphasized the need to address the ethical concerns surrounding their use (Tindana et al., 2014).
A number of studies have examined the use of biological samples for research. However, most of this literature focuses on the perspectives of a single stakeholder group, such as participants, researchers, or IRB members – rather than comparing perspectives across these groups on the same topic or issue. As science and medicine continue to evolve, so does the use of samples and associated data in generating new information. Empirical research examining the ethical dilemmas related to the secondary use of human biological samples from various contexts and stakeholder perspectives is therefore needed to identify emerging trends and ethical challenges. In this context, this paper aims to describe the ethical issues related to the secondary use of human biological samples.
Methods
This study employed a scoping review methodology to identify the ethical issues with the use of human biological samples. Scoping reviews are particularly useful for investigating broad literature, identifying knowledge gaps, setting research agendas, clarifying concepts, and identifying implications for decision-making, proving effective in identifying the ethical issues in the use of human biological samples (Munn et al., 2018; Tricco et al., 2016).
To conduct the scoping review, we followed the framework developed by Arksey and O’Malley which consists of five (5) stages, which are: 1) identifying the research question, 2) identifying relevant studies, 3) selecting studies, 4) charting the data, and 5) collating, summarizing, and reporting the results (Arksey & O'Malley, 2005). The procedures for each stage are outlined below:
Identifying Research Questions and Relevant Studies
The study was guided by the research question “What are the ethical issues regarding the secondary use of clinical samples for research?”. To identify the relevant studies on this topic, we developed a search string combining keywords (focusing on title and abstract) and subject headings (such as MeSH in PubMed). These keywords were combined by using Boolean operators like ‘AND’, ‘OR’, and ‘NOT’. All authors pilot-tested the developed search strategy and ran it in PubMed and Web of Science to identify any remaining potential issues or if any keywords were missed and subsequently finalized the search strings (see Table 1).
Search Strategies Used to Identify Relevant Articles.
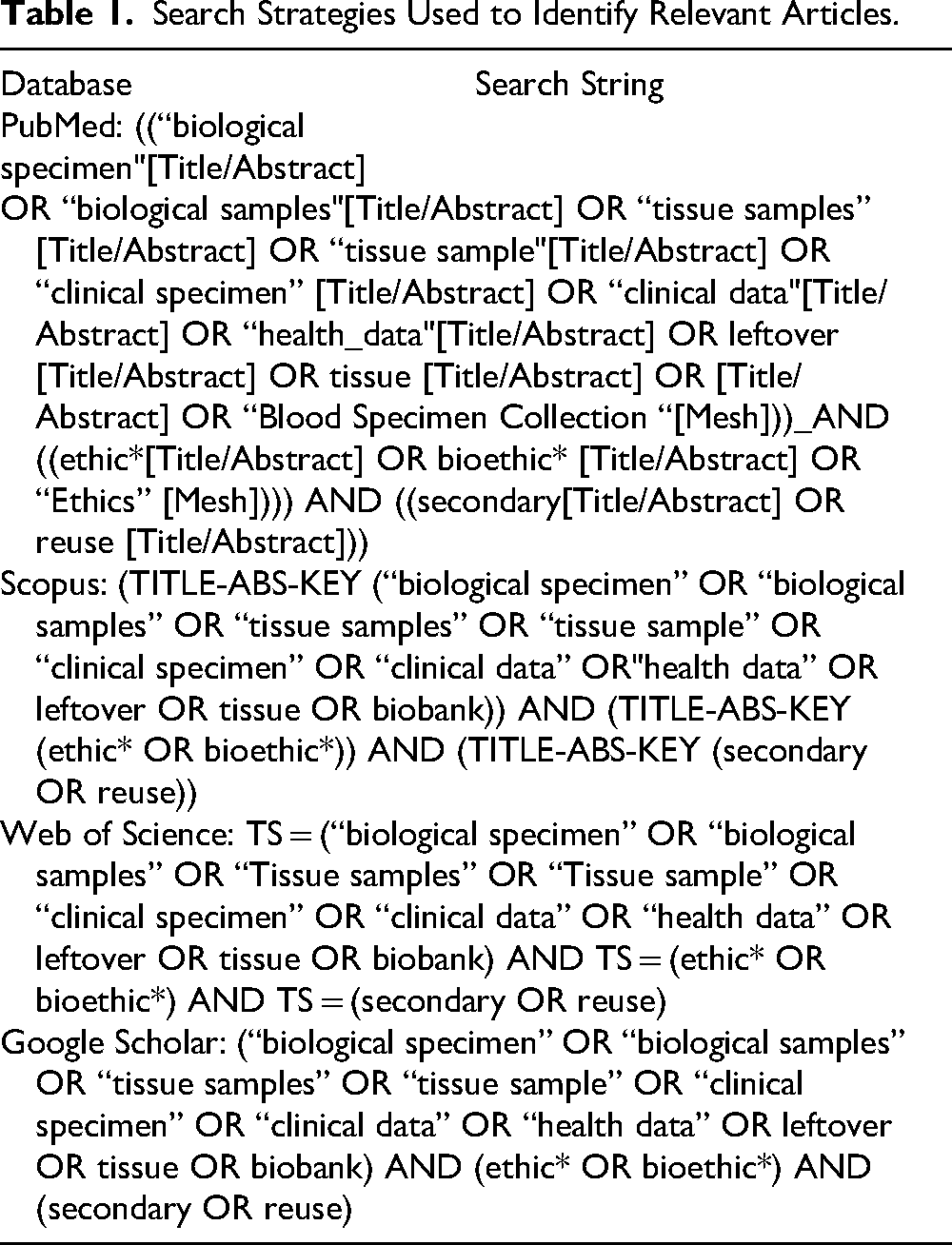
The final search strategy was conducted between March 28 and March 31, 2023, across three databases: PubMed, Web of Science, and Scopus. A secondary search was also conducted using Google Scholar to supplement and capture potential publications in grey literature. The result was exported and saved in a reference manager, i.e., EndNote 20. Duplicates were identified, counted, and removed following the PRISMA guidelines for reporting in systematic reviews and meta-analyses (Page et al., 2021).
Selecting Studies
In secondary review, it is recommended to have two independent reviewers who would independently assess the literature to ensure that relevant studies are included and minimize selection bias. However, due to practical constraints in this study, it was not feasible for two reviewers to independently screen all identified records. To reduce the potential for selection bias in the identification of relevant literature, we adopted the approach suggested by Mak and Tomas (Mak & Thomas, 2022) when dual independent reviewers are not feasible. Specifically, we randomly selected ten percent (10%) of the total number of publications for independent title and abstract screening and assessment. Then, the primary researcher (JL) and the junior supervisor (CT), independently assessed and compared the results of the screening of the randomly selected articles, which resulted in 91.8% reliability. Discrepant cases were discussed between the two reviewers until consensus was reached. When a consensus could not be achieved, the third researcher (NG) was consulted to resolve the disagreement. Following this calibration process, the primary author independently screened the remaining articles’ titles and abstracts. When uncertainty arose regarding the inclusion of an article, the decision was discussed with all research team during a regular weekly meeting to reach a collective judgement.
Inclusion and Exclusion Criteria
Following the title and abstract screening, a full-text screening was conducted. The articles were included if they were original studies (qualitative, quantitative, or mixed method), focused on the reuse of human biological samples, and discussed ethical issues. Studies were excluded if they involved autopsy samples, as these which raise distinct ethical, legal, cultural, and regulatory concerns. Additionally, case studies, review articles, commentaries, editorials, books reviews, theses, and conference papers were excluded. Only articles written in English languages were included. After screening and assessing the eligibility of the identified articles, our study yielded 44 articles for data analysis (see Figure 1).
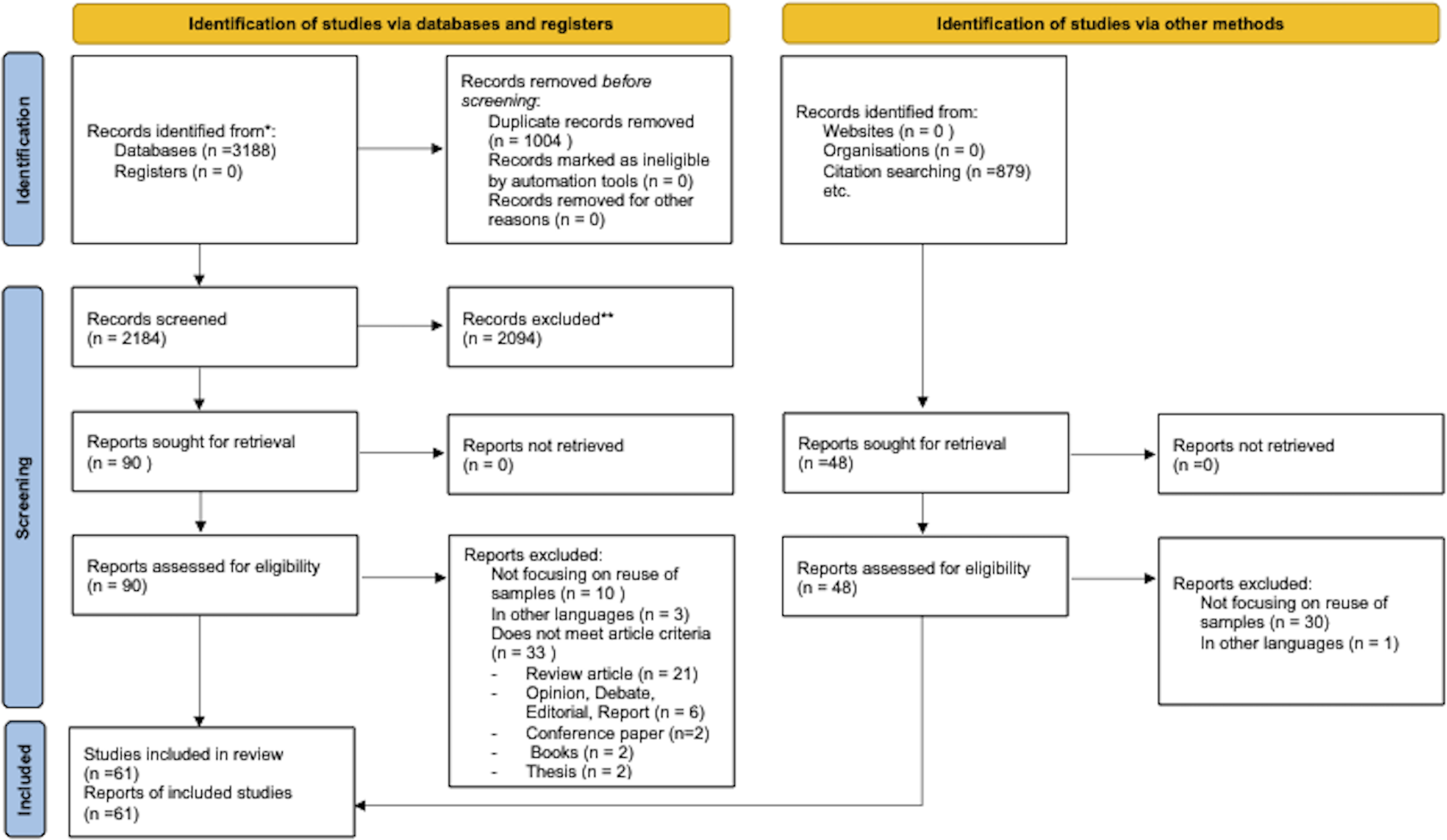
Literature Screening Process and Result following PRISMA 2020 Flow Diagram.
We conducted reference listings in the 44 included articles and found 879 relevant articles. After screening the abstracts, we excluded 831 records. We reviewed the full text of the remaining 48 articles and selected 17, resulting in a total of 61 studies that were included in the data analysis and final report (see Figure 1).
Charting the Data
The primary author reviewed the final included papers to identify the ethical issues. During this stage, a codebook was developed using data reduction. The research team developed a framework for data analysis (see Figure 2). The research team conducted pilot testing, revised, and expanded the framework based on a few articles. Using a spreadsheet, issues were tabulated and categorized according to the themes using the developed framework.
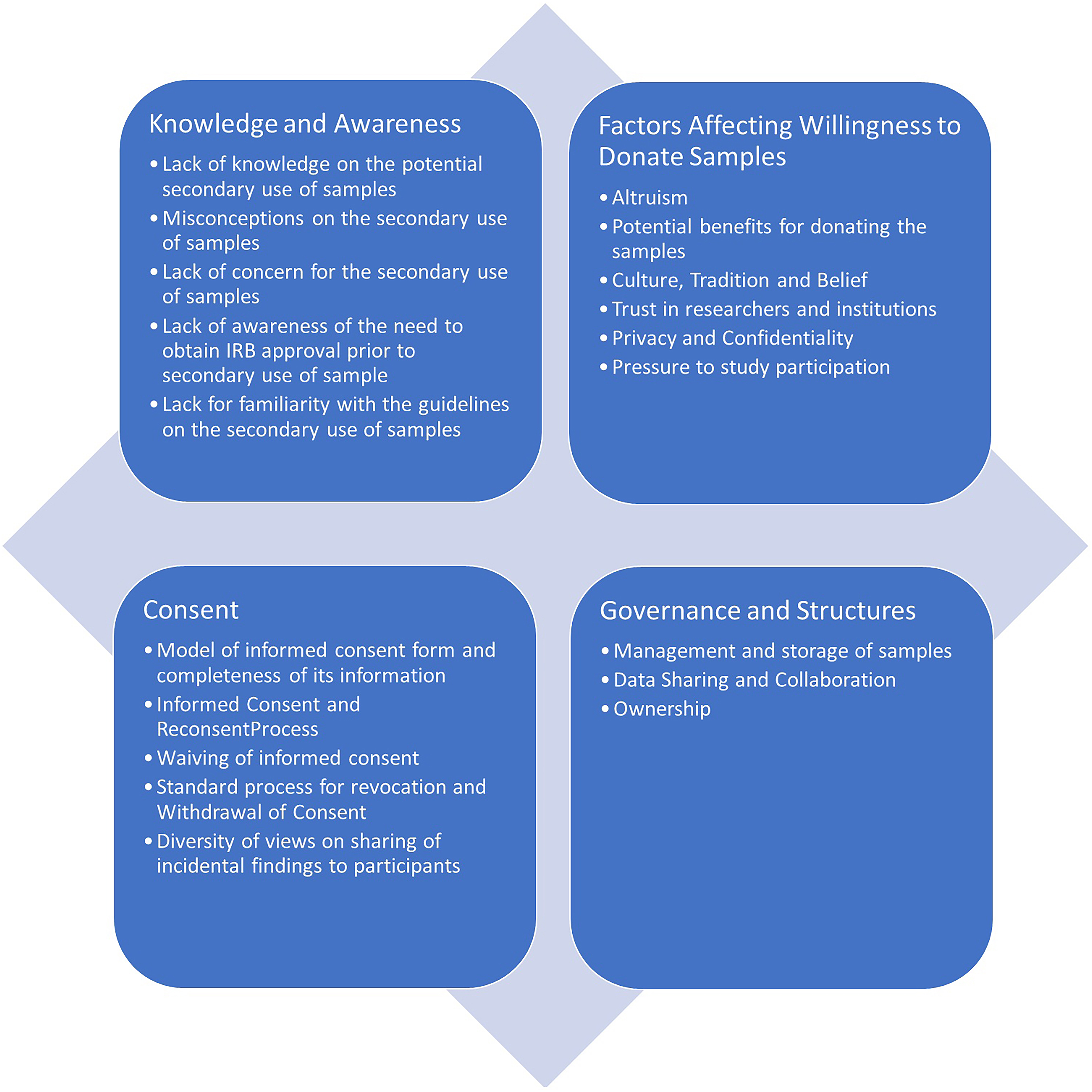
Four Themes on the Issues Related to the Secondary Use of Human Biological Samples for Research.
Result
Study Characteristics
Out of 61 articles included in the analysis, 36% came from North American countries (n = 22), 18% were from European countries (n = 11), 21% were from Asian countries (n = 13), 16% were from African Countries (n = 10), and 7% were from Oceania (n = 4). The remaining 2% of the articles were conducted globally (n = 1). None of the included studies originated from South America. Of the total number of articles, 20% were published between 2000 and 2010 (n = 12); 30% were from 2011 to 2015 (n = 18); 38% were articles from 2016 to 2020 (n = 23), and 13% of the articles were from 2021 to 2023 (n = 8). In terms of study design, 44% employed a quantitative (n = 27), 43% were a qualitative (n = 26), and 13% used a mixed method (n = 8). The most common types of data collection were surveys, interviews, and focus group discussions. A majority of the participants in the articles included were donors or research participants (57%). Studies examining the perspective of researchers and REC members accounted for 10% each, while a combination of different research stakeholders, such as community group representatives, REC, researchers, directors of institutions, and policymakers was included in 16% of the articles. Finally, biobank managers and laboratory personnel made up a small percentage of 7%.
Ethical Issues on the Secondary use of Human Biological Samples
Based on the thematic analysis of the included literature, four key themes emerged regarding the ethical issues of the secondary use of human biological samples. These include knowledge and awareness; factors affecting the willingness to donate samples; consent; and governance and structures (see Figure 2).
Knowledge and Awareness on the Secondary use of Human Biological Samples
Based on the result of the study, some donors lacked sufficient knowledge and awareness regarding the potential secondary uses of human biological samples, leading to confusion about the role of biospecimens in clinical and research settings (Ahram et al., 2022; Barchi et al., 2015; Hui et al., 2022; Jansen et al., 2019; Rothwell et al., 2010; Rothwell et al., 2012; Thiel et al., 2014). These misunderstandings sometimes resulted in misconceptions about secondary use, such as believing that their samples might be reused for cloning a person or producing biological weapons (Abdelhafiz et al., 2022; Ahram et al., 2022; Lee et al., 2019; Murad et al., 2017). Some participants were unconcerned about the secondary use of their samples for research and allowed researchers to “just use it” as long as it was for altruistic purposes (Ballantyne & Moore, 2018; Mathews et al., 2019). In a study conducted in the USA, some participants did not view their blood as uniquely identifying and ignored the potential risk of exposure. Additionally, they lacked a clear understanding of the storage and usage of their samples (Braun et al., 2014; Kasperbauer et al., 2022). Similarly, in a Canadian study, participants were surprised to learn that newborn screening (NBS) samples are already stored and available for research (Bombard et al., 2012).
The literature suggests that some researchers lack awareness regarding the need to obtain ethics approval before they can reuse human biological samples for research (Asai et al., 2002; Ballantyne et al., 2020) and view the application process as time-consuming (Whitley et al., 2012). Researchers in South Africa emphasized that Research Ethics Committees (RECs) must understand the difference between biobanks and tailor their reviews according to the risk associated with biological samples. (Moodley & Singh, 2016).
Research Ethics Committees (RECs) encounter their own set of challenges in the evaluation and approval of ethics for the secondary use of human biological l samples. A study in Botswana revealed that some REC members lacked familiarity with the guidelines related to the secondary use of samples for research (Barchi et al., 2015). This finding was supported by the study conducted in New Zealand, which reported a lack of guidance to assist REC members in evaluating the ethical issues related to the secondary use of samples (Ballantyne & Moore, 2018).
Factors Affecting the Willingness of Participants to Donate Human Biological Samples
Several factors motivate individuals’ willingness to donate their biological samples for research. These include altruism, potential benefits to participants, cultural tradition and belief, trust in researchers and institutions, privacy and confidentiality issues, doctor's instruction, timing of obtaining consent, and the type of consent model used to obtain the sample.
The literature suggests that some individuals are willing to donate their samples for research (Hui et al., 2022; Makhlouf et al., 2019; Sexton-Oates et al., 2016; van Teeffelen et al., 2016). Factors motivating participation include the perceived value and importance of research, altruistic intention, advancement of research, and contribution to clinical care (Braun et al., 2014; Dixon-Woods et al., 2017; Jansen et al., 2019; Makhlouf et al., 2019; Mathews et al., 2019; Merdad et al., 2017; Moodley & Singh, 2016; Page et al., 2016; Pentz et al., 2006; Rothwell et al., 2012; Vermeulen et al., 2009). Other participants were motivated by direct benefits such as free diagnostic or laboratory tests or the opportunity to receive personalized health insights (Al-Ebbini et al., 2021; Dixon-Woods et al., 2017; Merdad et al., 2017).
Our study also noted that the acceptability of donating human biological samples for research was influenced by culture and tradition. For example, during a focus group discussion in the United States (US) to understand diverse patient perspectives on donating biological samples for precision medicine research, an Asian participant mentioned, “I was raised Muslim, and there are very clear guidelines on how to conduct yourself medically.” To emphasize his point, he used the kidney as an example: “You're allowed to give a kidney because that benefits someone else… and you can't have something done out of vanity.” (Lee et al., 2019; Makhlouf et al., 2019).
Several studies also showed that individuals in some regions, particularly in parts of the Middle East, may be hesitant to donate their samples due to fear that their samples might be used in religiously prohibited research or misused for other purposes that are not congruent with their values (Ahram et al., 2022; Makhlouf et al., 2019; Whitley et al., 2012). Within certain African communities, concerns about loss of bodily integrity after death have also been reported, particularly if parts of their body went missing. These apprehensions stem from the belief that the removal of body parts could result in permanent loss, used for sorcery or witchcraft (Barchi et al., 2015; Braun et al., 2014). Furthermore, researchers were also rumored to be ‘selling blood’ and ‘devil-worshipping’ (Tindana et al., 2014). These cultural belief norms and traditions were confirmed as a real concern by researchers, which has fueled the community's apprehensions about the use of blood samples in research (Tindana et al., 2014).
Trust in the researchers and research institutions also plays an important role in shaping individuals’ willingness to donate samples (Asai et al., 2002; Quinn et al., 2014). However, a lack of trust among participants towards the researchers, biobanks, and institutions conducting biospecimen research, including the government, negatively affected the sample donation (Abdelhafiz et al., 2022; Ahram et al., 2022; Hui et al., 2022; Quinn et al., 2014). Participants expressed concerns about scientific exploitations and doubts about the lack of transparency in research processes, which may further discourage participation (Lee et al., 2019; Mathews et al., 2019; Murad et al., 2017; Pentz et al., 2006). Some expressed concerns that the researchers might profit from the use of donated samples (Gao et al., 2018; Jansen et al., 2019; Merdad et al., 2017). Additionally, there is also a lack of trust in the intentions of researchers from other countries (Alrabadi et al., 2019). For example, in a study conducted in Africa, some participants expressed that they did not want their blood to be shared with the United States (US), European countries, or the United Kingdom (UK), likely due to a history of research exploitation (Moodley et al., 2014). Similarly, participants in Scotland emphasized the importance of ensuring that the research activities reflect appropriate ethical values and incorporate adequate precautionary safeguards (Dixon-Woods et al., 2017).
Participants also expressed concerns related to privacy and confidentiality. These include fears about potential negative consequences of research on participants, (Alrabadi et al., 2019; Ballantyne & Moore, 2018; Makhlouf et al., 2019; Rothwell et al., 2010) stigmatization (Ballantyne et al., 2020; Joly et al., 2015; Makhlouf et al., 2019; Merdad et al., 2017; Moodley & Singh, 2016; Pentz et al., 2006; Quinn et al., 2014) leaking of data or breach of confidentiality, (Ballantyne & Moore, 2018; Braun et al., 2014; Hens et al., 2010); Hui et al., 2022; Jansen et al., 2019; Joly et al., 2015; Lee et al., 2019; Merdad et al., 2017; Murad et al., 2017; Nagaraj et al., 2014; Pentz et al., 2006) and identity theft (Joly et al., 2015; Murad et al., 2017). Some participants also raised concerns about a lack of understanding regarding the use of their samples and who can access them. (Hens & Dierickx, 2010; Kasperbauer et al., 2022). Some were concerned that their samples might be used by external parties such as insurance agents, governments, or legal authorities (Hens & Dierickx, 2010; Jansen et al., 2019; Lee et al., 2019; Murad et al., 2017; Page et al., 2016; Pentz et al., 2006; Rothwell et al., 2012). As a result, many studies recommended the importance of establishing a mechanism to protect participants’ privacy and confidentiality during storage and data sharing (Joly et al., 2015; Kasperbauer et al., 2022; Makhlouf et al., 2019; Matandika et al., 2020). Most biobanks linked donors’ samples to a health record database, posing risks if donor identities are compromised from coded data (Clark et al., 2006; Ibrahim et al., 2023). However, some researchers neglected to implement precautionary mechanisms, with one study reporting that a few researchers were storing samples using the participant's identifying information (Alkaraki et al., 2022).
Research Ethics Committees (RECs) also expressed concern about the potential for stigmatization and stereotyping of certain populations (Ballantyne & Moore, 2018). At the same time, RECs have varying approaches and requirements when reviewing and approving research protocols involving the secondary use of biological samples. According to our study, RECs have varying opinions about the level of risk involved in using identified samples. They categorize them as either less than minimal risk or greater than minimal risk. For example, in the United States (US), most RECs consider research using anonymized biological samples to involve minimal risk, whereas in Switzerland, a request for tissue samples for research, even without associated data, must require review by the full committee. This indicates that they consider the use of human biological samples to pose greater than minimal risk (Colledge et al., 2018).
Our study also showed that some individuals felt pressured to participate in studies as they were instructed by doctors to donate samples, feeling they had no choice due to the unequal relationships. (Al-Ebbini et al., 2021; Asai et al., 2002; Bombard et al., 2012; Frunză & Sandu, 2017; Moodley et al., 2014). The timing of obtaining the consent and the consent model were also identified as factors that pressured participation (Jansen et al., 2019; Rothwell et al., 2010; Rothwell et al., 2012). In some cases, consent was often obtained during hospital admission through a bundle consent form, that combines permission for medical treatment with consent for research participation (Bombard et al., 2012; Frunză & Sandu, 2017; Thiel et al., 2014). One participant described signing informed consent forms during the admission process, which made them feel vulnerable and made it difficult to refuse research participation (Frunză & Sandu, 2017).
Finally, some participants expressed concern that their contribution to research was not adequately recognized (Barchi et al., 2015). Others feared that their samples might be reused in the future without their explicit consent (Angell et al., 2009; Barchi et al., 2015; Hui et al., 2022; Merdad et al., 2017). As one participant noted, “I would not want to be another Henrietta Lacks” (Joly et al., 2015)
Consent
Several ethical concerns were also identified involving consent. These concerns were related to the model of informed consent documents used to obtain the samples from the participants, the consenting and reconsenting process, granting of waiver of consent, revocation of consent, and withdrawal from research participation, and the sharing of results or incidental findings with participants.
Informed Consent Documents
Different researchers and institutions used various models of informed consent to obtain the participants’ consent for the secondary use of their samples, including blanket consent, broad consent or general consent, open consent, and specific consent (Al-Qadire et al., 2010; Alrabadi et al., 2019; Bombard et al., 2012; Braun et al., 2014; Brown et al., 2016; Caulfield et al., 2012; Dissanayake et al., 2015; Eikemo et al., 2022; Joly et al., 2015; Master et al., 2013; Mathews et al., 2019; Rothwell et al., 2010; Vermeulen et al., 2009). Some participants expressed concern with blanket and open consent, because these models do not provide sufficient information and offered little control over the future use of samples (Al-Qadire et al., 2010; Alrabadi et al., 2019). A study examining the views of Non-Hispanic Black and Non-Hispanic White women on different informed consent models found that both groups preferred broad consent, as it provided sufficient information and allowed them to control the use of their sample and be asked for permission. However, the study showed that Non-Hispanic Black participants wanted to be asked for their consent before researchers could use their samples in future studies while Non-Hispanic White participants preferred to give one-time permission rather than being asked for each study (Brown et al., 2016).
Biobank managers and researchers acknowledge that different biobanks employ various types of consent forms for the procurement of samples (Abdelhafiz et al., 2022; Clark et al., 2006; Colledge et al., 2014; Edwards et al., 2014). They recognize that designing general consent forms that explain all the possible future uses of the sample at the time of donation is nearly impossible (Colledge et al., 2014; Whitley et al., 2012). Consequently, many researchers favored the broad consent model (Ibrahim et al., 2023; Moodley & Singh, 2016; Mwaka & Horn, 2019).
RECs also recognized the difficulty of explaining future uses of samples when these are uncertain at the time of collection (Tindana et al., 2014). Yet support for broad consent was not universal. While it was often preferred model by both participants and researchers, REC members in Africa believed that broad consent has limitations as it undermines participants’ autonomy since the requirements of full disclosure are not guaranteed (Matandika et al., 2020; Tindana et al., 2014).
Across studies, a recurring concern the adequacy of information contained in informed consent documents. Some individuals viewed consent documents as a kind of contracts between researchers and participants and therefore expected them to contain sufficient information to support meaningful decision-making. Several studies found that the information provided was incomplete or required improvement (Alkaraki et al., 2022; Clark et al., 2006; Frunză & Sandu, 2017; Goisauf et al., 2019). At the same time, some researchers noted that potential “abuse” may still occur even when the relevant information is formally included in the consent form (Tindana et al., 2014).
Informed Consent and Reconsenting Process
There were instances when the donors had difficulty making a decision based solely on the informed consent documents and preferred to have a discussion with the research team to better understand the research before making their decision whether to participate or not. (Bombard et al., 2012; Colledge et al., 2014; Dixon-Woods et al., 2017).
Participants in Scotland expressed that they wanted a proper consent process in place, otherwise they would not participate in the study (Dixon-Woods et al., 2017). In the US, parents raised the issue of the timing of the informed consent process for the storage of new dried blood spots, suggesting they should be informed before childbirth (Thiel et al., 2014). Participants in Canada echoed the concerns of participants in Romania, expressing the inappropriateness of including consent for screening in a “package” with consent for the storage of samples for research (Brown et al., 2016; Frunză & Sandu, 2017).
RECs have also raised the issue of the validity of consent that was obtained during the standard clinical consent process (Ballantyne et al., 2020). Obtaining consent during the standard clinical consent process at the point of collection posed an ethical issue, as patients are quite distressed and vulnerable during this period (Ballantyne et al., 2020; Goisauf et al., 2019; Hens et al., 2010). REC members in the UK emphasized the need to ensure the adequacy of the proposed consent process and clarity in the information to avoid confusion about whether the samples were collected as a part of standard care or for research purposes (Angell et al., 2009).
Participants have different views and preferences on the re-consenting process. Most of the research participants from Jordan, South Africa, and the Native Hawaiian communities wanted to limit the re-use of their samples and preferred to be contacted and provided with information each time their sample would be re-used (Al-Ebbini et al., 2021; Brown et al., 2016; Moodley et al., 2014). However, participants from Norway, Scotland, Australia, and Canada did not think it was unnecessary to be contacted and consented to every single use of their stored samples as it might create anxiety (Dixon-Woods et al., 2017; Eikemo et al., 2022; Page et al., 2016; Sexton-Oates et al., 2016).
Researchers likewise held divergent views regarding the need to re-consent participants for the secondary use of samples. Researchers in Egypt, Sudan, Morocco, and Jordan agreed that re-consent is necessary for any additional research on samples initially collected for medical purposes or when conducting additional analyses that fall outside the original scope of the study (Ibrahim et al., 2023). This contrasts with a study conducted in New Zealand and Canada (Whitley et al., 2012) where many researchers believed that obtaining re-consent was unnecessary and expensive, or could cause harm and anxiety to patients (Ballantyne et al., 2020). There were instances when researchers requested a waiver but were aware that informed consent might be required by local RECs or, in some cases, by journals during publications (Whitley et al., 2012).
Waiver of Consent
The responsibility of providing approval for waivers of consent caused anxiety and stress for IRB members (Angell et al., 2009; Ballantyne & Moore, 2018). One study reported RECs’ lack of clarity and uncertainty on whether they should demand researchers to obtain separate informed consent for the secondary use of leftover samples or when these human biological samples were already stored (Angell et al., 2009). Sometimes RECs were willing to consider allowing the use of human biological samples without consent after obtaining justification from the researchers, to balance the potential benefit of the study and the impracticability of obtaining consent (Angell et al., 2009; Ballantyne & Moore, 2018; Ballantyne et al., 2020; Goisauf et al., 2019). However, not all justifications were considered sufficient; for some RECs, the financial cost of reconsent alone did not satisfy the condition of impracticability (Ballantyne et al., 2020).
Revocation of Consent and Withdrawal of Research Participation
The majority of the participants believed they had a right to withdraw their consent and sample at any time, and they would appreciate it if the researchers would allow them to opt in for the research (Caulfield et al., 2012; Dixon-Woods et al., 2017; Hui et al., 2022; Ibrahim et al., 2023; Master et al., 2013; Thiel et al., 2014). Researchers recognized participants’ right to withdraw from a study but were unsure about the appropriate process following a request for revocation of consent (Whitley et al., 2012). One study even reported receiving a request for withdrawal of a sample but decided to keep it, arguing that if it were destroyed, the diagnostic tests conducted using that sample could no longer be validated (Hens et al., 2010).
Sharing of Incidental Findings
There is a lack of a clear policy on whether the results should be returned to the participants. Participants themselves have different preferences on whether they would want to be notified of the findings from studies conducted using their samples. Some participants hope that researchers would remember the “face behind the sample” and notify them of the findings, especially those related to their health (Caulfield et al., 2012; Fong et al., 2004; Gao et al., 2018; Gordon et al., 2019; Quinn et al., 2014; Sexton-Oates et al., 2016; Thiel et al., 2014; Vermeulen et al., 2009). These participants believed they would benefit from the result due to early warning that could enable earlier diagnosis or prevention (Gordon et al., 2019), but some participants wanted information even if the illness could not be treated or prevented (Eikemo et al., 2022). When the information was made available, some participants wanted to personally receive relevant health information and research findings (Fong et al., 2004; Thiel et al., 2014). Other participants preferred to be contacted by a researcher affiliated with the study, a specialist physician, or a genetic counsellor who could provide information about the health implications of such findings (Quinn et al., 2014). When the donor is deceased, some believe the findings should be offered to families and shared only after obtaining their permission (Gordon et al., 2019).
Other participants were less interested in knowing the research result unless the findings directly affected their own or their family's health (Ahram et al., 2022; Quinn et al., 2014), especially results “from a new test that was not well understood” (Gordon et al., 2019). Participants expressed that receiving such information could only cause negative emotional impact, leading to unnecessary fear and anxiety (Gordon et al., 2019).
Researchers generally believed donors should be notified if there's an incidental finding from the participants’ samples that would impact their health (Quinn et al., 2014). However, they were divided on whether to notify and return the results, only if the findings were clinically actionable or regardless of whether a medical intervention could be provided (Ibrahim et al., 2023; Quinn et al., 2014). Researchers also faced difficulty in balancing the privacy of the individual and the need to communicate the results, as well as deciding how and who should deliver the information to the donor (Quinn et al., 2014). In India, researchers recognized the importance of having a physician as part of the team to convey the results to the participants (Vaz & Vaz, 2018).
REC members also have different opinions regarding the return of incidental findings to the participants. While the majority of RECs in Switzerland thought incidental findings should be shared with the donor (Colledge et al., 2014), lay members in India were concerned about the usefulness of the results to donors with limited access to healthcare. Meanwhile, legal members of the IRB in India worried that providing such findings to participants might be misinterpreted as medical negligence by the doctors (Vaz & Vaz, 2018).
Governance and Structures
Several ethical concerns were also identified in relation to the governance of human biological samples, particularly in the areas of sample management and storage, data sharing and collaboration, ownership, and benefit sharing.
Management and Storage of Samples
Research participants were amenable to the sample storage if they were informed about it and given permission (Moodley et al., 2014; Thiel et al., 2014). In the Netherlands, mothers generally supported the storage of neonatal dried blood spots indefinitely for research purposes. (Jansen et al., 2019; van Teeffelen et al., 2016). Similarly, the majority of individuals with familial risk agreed that researchers should have unlimited access to samples provided that RECs were monitoring the research (Quinn et al., 2014). However, most adult individuals from Jordan and the United States (US) believed that a time limit for sample storage should be implemented (Abou-Zeid et al., 2010; Alrabadi et al., 2019).
Researchers were also divided on whether time limits should be imposed on the use of donated human biological samples. One group of researchers believed that like any other REC-approved research, time limits should be implemented in biobanking consents. The other group argued that a time limit should not be specified in every study, but should be reviewed on a case-by-case basis (Abou-Zeid et al., 2010; Quinn et al., 2014; Rothwell et al., 2012). Researchers also suggested it's the research participants who have the right to establish limits on the use of their samples (Mwaka & Horn, 2019).
Regarding the disposal of samples, the researcher employed different approaches for the disposal and return of samples. Some samples were discarded or destroyed following the completion of research; some were retained in long-term storage; some were returned to diagnostic pathology services; and some had no specified management plan for the return or disposal of samples (Clark et al., 2006). In Belgium, there was uncertainty about the legal allowance for sample disposal, though destruction upon donors’ request was permitted (Hens et al., 2010). A study conducted in the United States (US) found that only 33% of the biobanks surveyed had a formal business plan, and only 27% had a written plan for biological sample termination (Edwards et al., 2014). Researchers in Malawi expressed the lack of ethical governance guiding the retention and destruction of samples.
REC members expressed concerns about destroying the samples after a single use, fearing it might hinder scientific progress and prevent validation of tests performed using the samples ( Hens et al., 2010); Mathews et al., 2019). They also have different views about duration and the manner of storing samples in an identified vs de-identified form. Some researchers emphasized the importance of de-identification to ensure the donor's privacy, while others stressed the need to link data back to participants in case of incidental findings (Barchi et al., 2015).
Data Sharing and Collaboration
Some participants strongly disapprove of sharing and exporting samples outside their countries, preferring to maintain control over their samples by providing consent for any potential transfer to another country (Abou-Zeid et al., 2010; Ahram et al., 2022; Al-Ebbini et al., 2021; Alrabadi et al., 2019; Brown et al., 2016; Moodley et al., 2014; Pentz et al., 2006). Factors affecting the participants’ willingness to share data and collaborate include cultural beliefs, fear of cross-border collaboration, concern of sample exploitation by governmental and commercial bodies, mistrust of researchers and research institutions, and skepticism towards government institutions that hold the samples (Ahram et al., 2022; Alrabadi et al., 2019; Hui et al., 2022; Kasperbauer et al., 2022; Makhlouf et al., 2019; Matandika et al., 2020).
Some were more lenient and believed it was unnecessary to obtain their consent or receive any information if their samples were exported to other countries (Eikemo et al., 2022; Moodley et al., 2014) or shared with an investigator from another institution (Ibrahim et al., 2023). The majority of the participants in Norway also agreed to research collaboration with the health industry if the aim of the collaboration is for treatment improvement and not for profit (Eikemo et al., 2022).
Researchers have highlighted the need for proper guidance on sharing and accessing samples (Matandika et al., 2020). Based on the study results, researchers exhibit varying attitudes and perspectives about data sharing and collaboration. Some have shown positive attitudes toward data sharing with researchers within institutions in their countries, but have low acceptance of sharing the samples with institutions outside of their countries (Ibrahim et al., 2023; Zhang et al., 2010). Factors affecting the willingness of the researcher to share their data with other countries include a lack of recognition for local researchers’ contributions to research collaborations (Abdelhafiz et al., 2022; Dissanayake et al., 2015; Ibrahim et al., 2023; Tindana et al., 2014; Zhang et al., 2010), inability to control the fate of the exported samples (Tindana et al., 2014; van Teeffelen et al., 2016) and fear of exploitation of research (Matandika et al., 2020), and the possibility of unauthorized, reidentification of donors (Whitley et al., 2012). Thus, an appropriate mechanism is needed to protect the identities of the individuals sharing samples in international collaboration (Ibrahim et al., 2023). Researchers believe that in international collaboration, local partners should be capacitated through training and opportunities to strengthen their scientific capacity and contribute to the conduct of the study, analysis, and publication of the research (Tindana et al., 2014). Collaborators should also ensure that all countries involved benefit fairly (Ibrahim et al., 2023).
The lack of common standards for data sharing can create problems both for the export of samples and the use of samples from overseas biobanks (Whitley et al., 2012). IRB members echoed the sentiment of the researchers on the need for clear institutional and national policies and guidelines governing these practices (Tindana et al., 2014). Currently, there no mechanisms in place to determine the fate of exported samples but they were hoping that the host institutions would take responsibility for the action of their local researchers and will keep them updated on the outcome of the overseas analysis (Tindana et al., 2014).
Ownership
Participants, researchers, and IRBs have varied perceptions of who owns the samples (Master et al., 2013). The majority of the participants thought they and their families owned the sample (Barchi et al., 2015; Caulfield et al., 2012; Gordon et al., 2019; Rothwell et al., 2010; Rothwell et al., 2012). However, some participants hold different opinions. In a study conducted in Canada, the majority of respondents indicated that they thought the institution where the research was being conducted owned the samples, while some thought they belonged to the researcher or funder (Caulfield et al., 2012) but despite this varied perception of ownership, participants maintain that they have the right to decide with regards to their sample (Caulfield et al., 2012; Gordon et al., 2019). In a study conducted in India, ethics committee members and medical researchers viewed the patient as the true owner, which emerged as a ‘moral’ construct (Vaz & Vaz, 2018).
Most researchers do not inform the donor who owns the sample after it was donated (Clark et al., 2006). Researchers also have varied perceptions of ownership; the majority believed that the institution or the hospital owned the sample, while a few think the donor owns them. (Clark et al., 2006). Some researchers also felt that they had a stake in the ownership because they were instrumental in the process of obtaining the sample, and the ownership was handed over to them through the consent form (Vaz & Vaz, 2018).
Researchers cautioned that while it is their responsibility to safeguard the samples and ensure that informed consent has been obtained, some of them believe that the RECs should serve as custodians of samples collected or research (Matandika et al., 2020). However, most of the REC members viewed the storage facility as the virtual owner or “Custodian” (Vaz & Vaz, 2018). In a study conducted in USA, it was found that a few biobanks have no policy on specimen ownership. Those with written policies have different provisions regarding ownership (Edwards et al., 2014). Because of the diversity of views on ownership, the REC recommended that there must be guidelines and a framework for ownership (Matandika et al., 2020).
Benefit Sharing
Arising from the issue of ownership is the issue of benefit sharing following the commercialization of research results (Vaz & Vaz, 2018; Zhang et al., 2010). The majority of the participants believed that they should have a share because it's their blood, they provided the sample (Abou-Zeid et al., 2010; Al-Ebbini et al., 2021; Barchi et al., 2015; Joly et al., 2015). Others believed that “everybody” should benefit financially. Some researchers believed that appropriate benefit sharing with participants and the larger community should be agreed upon. However, the majority of the REC believed that the participants should not receive payment for samples or any monetary gain for sample contributors and that altruism should drive sample donation, not personal gain (Joly et al., 2015).
Discussion
The secondary use of human biological samples for research presents complex and persistent ethical challenges related to research stakeholders’ knowledge and awareness, factors influencing participation, consent practices, and the governance of the human biological samples and the four analytical axes identified in this review can be mapped directly onto the classical bioethical principles of autonomy, beneficence, non-maleficence, and justice, and are governed by international documents.
The knowledge axis concerns whether participants, researchers, and the REC possess adequate, comprehensible information about the secondary use of human biological samples. Our findings showed that participants often lack knowledge and awareness regarding the potential secondary use of their biological samples. Even among those who are aware, there are often misconceptions about how and where their sample will be used. Many participants also have a limited understanding of privacy-related issues, which necessitates informing them about the potential risks involved in using samples for research, how their samples will be protected from unauthorized use, and who will have access to them and due to this lack of knowledge, participants may be vulnerable to exploitation. Therefore, it is the duty of the physicians and the researchers to assess participants’ understanding and provide them with sufficient information regarding the use of the sample, the research being conducted, and their rights as participants. Emphasis should be placed on distinguishing between sample collection for medical treatment and research purposes. Ensuring such understanding is a precondition for autonomy and a safeguard for non-maleficence as emphasized in paragraphs 25 and 26 provisions of the WMA Declaration of Helsinki (WMA, 2013), Council for International Organizations of Medical Sciences (CIOMS) Guidelines 9 −1 1, the General Data Protection Regulation (GDPR) provisions on transparent, informed processing of personal data and biological materials (EU, 2016) and Article 3 of the Universal Declaration on Bioethics and Human Rights which mandates that “The interests and welfare of the individual should have priority over the sole interest of science or society” (UNESCO, 2005). Therefore, it is the moral obligation of the researchers to uphold participants’ human rights, and respect and protect them from mistreatment due to their lack of knowledge and awareness.
The findings also showed that some researchers are unaware of the need to obtain approval before accessing the sample for research. The CIOMS Guideline 11 states that, “The protocol for every study using stored human biological materials and related data must be submitted to a research ethics committee” (CIOMS, 2016). Researchers should make an effort to familiarize themselves with the ethical, legal, and standards for research as mandated by the Declaration of Helsinki (WMA, 2013) and the Declaration of Taipei (WMA, 2016). Here, the central issue is not a novel ethical dilemma about what ought to be done, but a regulatory and professional compliance problem; existing ethical requirements are clear, yet knowledge of and adherence to them is incomplete. Becoming an investigator requires more than just education; they should also receive proper training in research ethics and applicable guidelines. Investigators who work directly with participants, especially in clinical studies, must seek ethical approval. RECs then play an organizational and regulatory role in evaluating the study's social value, potential risks, and benefits, and in providing recommendations on how to protect participants and minimize harm during the research study. This speaks to both beneficence by promoting social value and potential benefits, and non-maleficence by minimizing risks. By ensuring fair review processes, the REC contributes to justice by ensuring equal distribution of the burdens and benefits of research.
Another finding in the study is that some REC members, like the researchers, are not familiar with the guidelines. This is more of an administrative and capacity problem rather than an ethical dilemma; the ethical guidelines are in place, but the organizational structures do not yet ensure that the REC members are trained and supported, to apply them consistently. REC members must receive training related to bioethical concerns on biobanking. Without proper training, RECs would have difficulty in detecting ethical concerns related to the use of the samples, leading to failure to safeguard the interests of the study participants. Strengthening the knowledge of the RECs through training, standardized procedures, and alignment with international guidelines such as CIOMS, Declaration of Helsinki, Declaration of Taipei, and UNESCO's Universal Declaration on Bioethics and Human Rights, is essential for implementing justice, beneficence, and non-maleficence in practice.
The willingness axis captures participants’ readiness to donate samples in contexts shaped by culture, history, and trust. In several African settings, fears related to loss of bodily integrity, sorcery, and rumors of “selling blood” or devil worshipping shape community responses to sample donation and reuse (Barchi et al., 2015; Braun et al., 2014; Tindana et al., 2014). In parts of the Middle East, concerns that samples might be used for religiously impermissible research or exported to foreign institutions without adequate oversight heighten scrutiny of consent processes (Ahram et al., 2022; Makhlouf et al., 2019; Whitley et al., 2012). These raise genuine ethical questions about respect for cultural values, fairness, and global justice, but they also point out to organizational challenges around communication, engagement, and community consultation. Researchers must be sensitive and respectful of the prevailing cultural beliefs of individuals. Respect for research participants is operationalized by obtaining informed consent, which requires providing sufficient information for individuals to make informed decisions. For instance, the parental surprise in the Asian context at the long-term storage and secondary use of newborn screening samples and worries about future misuse illustrate how limited transparency can undermine trust (Hui et al., 2022). Thus, to bridge the gap of misunderstanding and obtain their consent, researchers should establish effective communication and build trust with participants.
The study findings also indicate that a lack of trust in researchers, institutions, and government serves as a significant barrier to sample donation. Trust deficits are not only a procedural problem. These are rooted in past injustices and fears of exploitation, and thus represent substantive ethical concerns, i.e., justice, non-maleficence, and respect. At the same time, addressing these concerns requires institutional and regulatory responses such as transparent governance, clear accountability, and community engagement, which are organizational in nature. Without the willingness of individuals to donate human samples, the advancement of science and medicine will be hampered. Therefore, fostering trust and understanding are crucial both for facilitating the donation process and to ensure that research proceeds in an ethically legitimate manner, ensuring the progress of medical research. Supporting willingness through respectful communication and community engagement advances autonomy through voluntariness, beneficence by enabling socially valuable research, non-maleficence by addressing fears of exploitation and justice by responding to historical inequities, which are in line with the UNESCO's Universal Declaration on Bioethics and Human Rights call for respect for cultural diversity and pluralism and CIOMS guidance on community engagement (UNESCO, 2005; CIOMS, 2016).
The consent axis focuses on when and how permission for storage and secondary use is obtained. Human biological samples are often obtained from patients in the healthcare settings, where decisions to donate samples or participate in a study may be influenced by perceived expectations or pressures from their physicians, nurses, or even family members due to the timing of obtaining consent and the unequal power relationship. This finding suggests a potential misuse or at least problematic use of the doctor's authority and the medical institution, which raises significant ethical concerns about voluntariness and respect for autonomy. In particular, the timing of obtaining consent merits substantial ethical and organizational discussion. In many settings, consent for the secondary use of human biological samples is often obtained during the standard of delivery of care at the point of sample collection, a stage where patients are vulnerable and dependent on their physician. Ethically, obtaining consent in these circumstances risks undermining voluntariness; organizationally, it reflects how hospital workflows and documentation practices bundle clinical and research decisions together (e.g., “package” consent form). These structural features of recruitment and the consent process may compromise the validity of consent and shape the human biological samples that are later used in secondary research. Article 8 of the Universal Declaration on Bioethics and Human Rights mandates respect for human vulnerability and personal integrity (UNESCO, 2005). Institutions should therefore reconsider consent pathways and documentation practices to ensure that patients are fully informed and able to make independent decisions without undue pressure.
Beyond the timing of consent, the model of consent used in obtaining permission must also be reconsidered. Several models of consent were used to procure the sample for storage, each with limitations in providing sufficient information about the study. Blanket consent is convenient for researchers, as it allows unlimited future use of samples for other studies; however, it conflicts with the ethical requirement to respect participants′autonomy by enabling specific, informed decisions about future uses of the samples (Quinn et al., 2014). This poses a substantive ethical concern: the tension between maximizing scientific utility (beneficence) and preserving meaningful control for participants (respect for persons/autonomy).
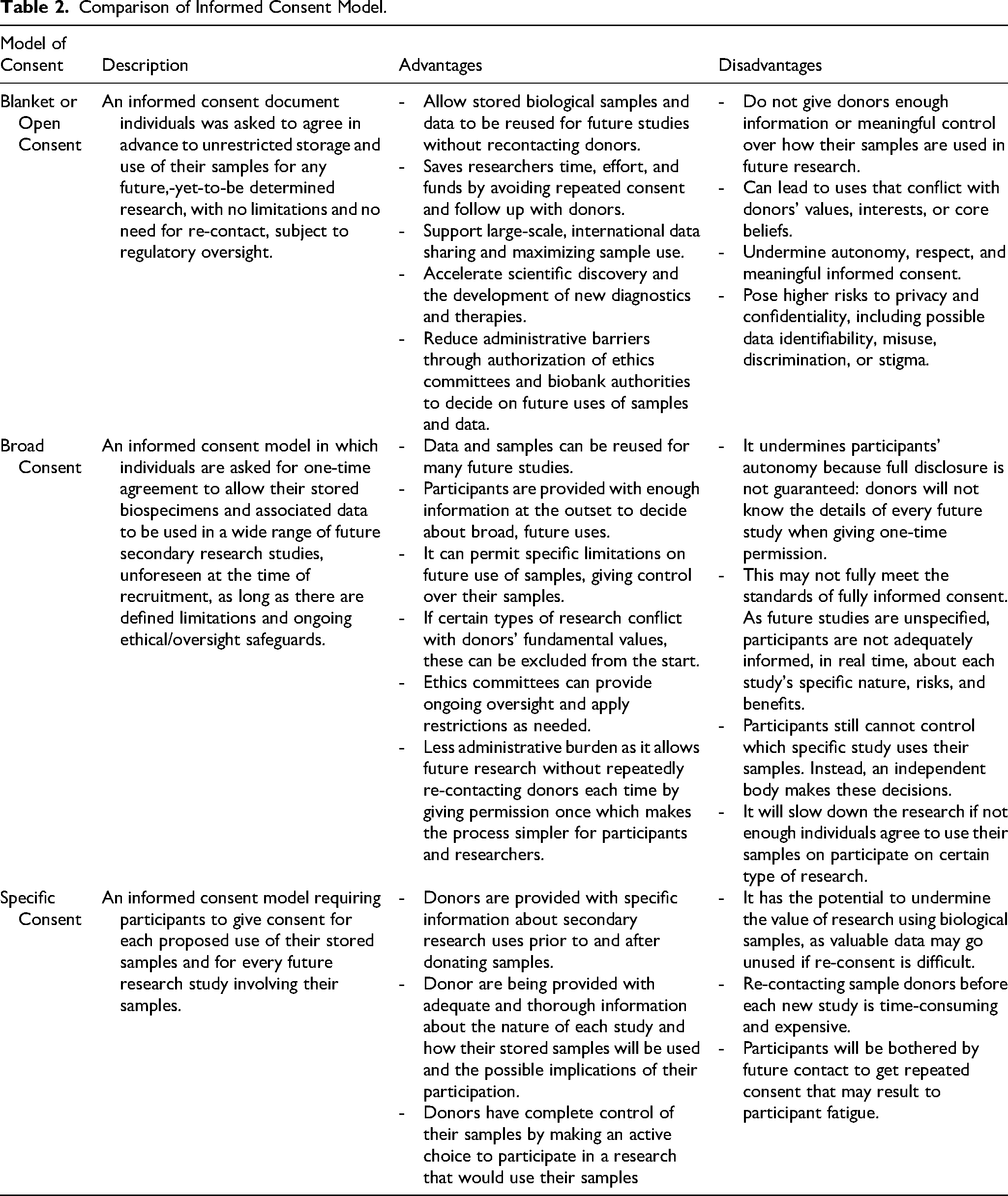
Most researchers prefer the broad consent model, which allows for a wider scope of future research without needing to re-consent participants for each study. However, some participants prefer to be informed and be asked for permission for every test conducted on their sample. One of the pillars of the ethical principles for research is Respect for Persons, which acknowledges that the individual is an autonomous agent. According to Belmont Report, “an autonomous person is an individual capable of making decisions about personal goals and of acting under the direction of such deliberation and to respect autonomy is to give weight to autonomous person's considered opinions and choices”. When participants explicitly wish to approve each new use, the ethical issue is how to respect this preference without rendering research impracticable. This is a genuine ethical dilemma between respect for autonomy and individual control, and feasibility, efficiency, and the social value of research (beneficence). If broad consent is used, without mechanisms for ongoing information or choice, researchers may fail to honor the preference of these participants, which can be interpreted as a lack of respect. At the same time, implementing fully specific consent for every secondary use maybe organizationally infeasible for large biobanks. Thus, the ethical dilemma (autonomy vs feasibility/beneficence) manifests as a regulatory and organizational design problem. Therefore, researchers should work with the institutions and RECs to develop an informed consent model that allows active engagement so that participants who wish greater control can exercise it, while permitting socially valuable research. We have included a comparative model of consent to guide the researchers and institutions when developing the appropriate consent for secondary use of human biological samples (Table 2).
Comparison of Informed Consent Model.
There were also instances in which researchers request for a waiver of consent. According to CIOMS, RECs “may waive the requirement of individual informed consent if: 1) the research would not be feasible or practicable to carry out without the waiver; 2) the research has important social value; and 3) the research poses no more than minimal risks to participants or to the group to which the participant belongs” (CIOMS, 2016). Additionally, the Declaration of Taipei has stated that “reasonable efforts should be made to seek the consent of those persons for continued storage and research use of their data and biological materials” (WMA, 2016). Here, the ethical dilemma is explicit: balancing respect for individual autonomy against the public interest in generating socially valuable knowledge from existing data (beneficence and justice). The regulatory and organizational challenge is to define what constitutes “reasonable efforts” and “impracticability” of obtaining consent and to ensure that RECs apply these criteria consistently rather than an ad hoc judgement. Clarifying these thresholds in national and institutional guidelines would transform an area of recurring case-to-case uncertainty into a more stable regulatory framework, while keeping the underlying balance transparent and consistent with international standards.
Another interesting finding is the varying opinions of different research stakeholders regarding the return of results of unsolicited findings. Some patients wanted results regardless of clinical actionability, others, only if results would affect their family's health, and some wished to avoid information that might cause anxiety. According to CIOMS, the result of the incidental discoveries must be returned to the individual donor if they wish to receive them (CIOMS, 2016). However, this recommendation highlights a substantive ethical tension between beneficence and respect for person/autonomy versus non-maleficence and justice. Returning clinically significant findings that may enable prevention or early treatment, especially when participants express a desire to know, but concerns about potential psychological harm, limited access to follow-up care, and resource constraints, justifies not returning certain findings, or limiting return to “actionable” results.
Researchers and RECs members were likewise divided on whether to return all pertinent findings, only actionable ones, or none at all. These are genuine ethical dilemmas about beneficence, non-maleficence, and respect for autonomy. It also translates into regulatory and organizational as to who is responsible for validating findings, re-identifying donors, and communicating results, and how consent forms should record participants’ preferences. Including clear options about the results in consent processes, as suggested by participants (Gordon et al., 2019), is an organizational response to this ethical tension. International instruments, including the Declaration of Helsinki, CIOMS, the Declaration of Taipei, the UNESCO Universal Declaration on Bioethics and Human Rights, and GDPR articles 7,9, and 13–21, converge on the importance of informed, voluntary, and appropriately scoped consent, as well as careful justification of broad consent models and waivers.
The governance axis encompasses the institutional, legal, and procedural framework for managing samples and data in terms of ethical review, policies on storage, sharing and export, data protection, ownership, and benefit-sharing. Many of the problems identified in this axis are primarily regulatory and organizational, such as the absence of guidelines for sample storage, disposal, or destruction, as well as for sharing and access of samples, exporting, and using samples from overseas biobanks. These governance gaps create environments in which ethical violations – such as unauthorized use, privacy breaches, or exploitative collaborations – are more likely. For example, conflict can arise between the Principle of Beneficence and the Principle of Respect for a Person/Autonomy if these samples are used without permission, or if the researcher fails to consider individuals’ preferences for being actively involved in decision-making about their samples. Similarly, tensions between the Principle of Beneficence and the Principle of Justice arise when products or profitable innovations are developed from the biospecimens, as in the widely cited case of Henrietta Lacks (Joly et al., 2015). With these, ethical questions as to who should benefit from these developments and how the benefits should be distributed arose. In addition, organizational questions such as “Does the institution have a business plan or is there a written institutional policy for specimen termination?” should also be assessed, as the absence of such a policy may lead to ethical problems. This governance domain thus operated at the intersection of ethical principles and institutional design. CIOMS and the Declaration of Taipei both recommend that governance structures for biobank materials should be established, including oversight committees, clear access policies, and monitoring mechanisms. Institutions should therefore develop detailed policies on access, storage, data sharing, and collaboration agreements for the use of human biological samples, including provisions for monitoring, auditing, and accountability. Strengthening this domain of governance is crucial for realizing justice, non-maleficence, beneficence, and autonomy.
Additionally, there is a lack of provision regarding ownership in the guidelines and framework. Participants, researchers, and RECs hold diverse views about who owns the samples. Some stakeholders invoke ownership in a moral sense, i.e., the patients as “true owners” because the samples were derived from their bodies, while others treat ownership as a legal and custodial concept (Vaz & Vaz, 2018). These conceptual ambiguities generate ethical dilemmas about control, benefit sharing, and respect for persons, but the practical problems they create, such as inconsistent consent language, unclear custodianship, or disputes over commercialization, are fundamentally regulatory and organizational. RECs’ call for guidelines and framework on ownership (Matandika et al., 2020) is an attempt to resolve those operational uncertainties. CIOMS and the Declaration of Taipei recommended that governance structures related to biobank materials must be in place. In keeping with the principles of autonomy, justice, and beneficence, institutions should develop detailed policies concerning the governance of research using biobank materials, including access to stored samples, data sharing, and a collaboration agreement for the use of biological samples. These guidelines should also include a clear definition of ownership and benefit sharing to address ethical concerns effectively.
Benefit sharing is another area where ethical and organizational dimensions are intertwined. The ethical concerns center on justice and fairness: whether and how donors and communities should share in benefits arising from commercialization or other uses of their samples. Many participants believed they should receive some form of benefit – sometimes conceived as personal financial gain, sometimes as benefits to everybody, including communities or health systems (Abou-Zeid et al., 2010; Al-Ebbini et al., 2021; Barchi et al., 2015; Joly et al., 2015). Many IRB members, by contrast, argued that sample donation should be driven by altruism and that individual payment risks commodifying the body, undermining voluntariness, or exacerbating inequities (Joly et al., 2015). These are substantive ethical debates about justice, exploitation, and the moral meaning of bodily materials. Translating them into practice requires regulatory or organizational solutions, such as explicit policies on whether and how financial benefits, capacity building, or infrastructural investments will be shared with source communities and countries, consistent with CIOMS guidance on benefit sharing and UNESCO′s Universal Declaration on Bioethics and Human Rights’ emphasis on social responsibility and health.
This review complements the importance of secondary use of human biological samples in generating new knowledge, but its ethical acceptability depends on how well four axes – knowledge, willingness, consent, and governance – are addressed in practice. Autonomy can be realized through adequate knowledge, genuine willingness, and valid consent. Beneficence and non-maleficence can be promoted by ensuring that participants understand potential outcomes (knowledge) and are not pressured (willingness), and are included in an ethically reviewed protocol under proper governance that promotes fair selection of participants, transparency, and equitable sharing of risks and benefits, including consent processes that are accessible to all groups. The challenges identified are not related to the absence of the ethical principles but more on gaps on the implementations, regulations and oversights. Addressing these challenges requires deliberate action to translate ethical practices into enforceable policies and routine research practices.
Limitations
Methodologically, this study has several limitations. First, the exclusion of non-English articles may have resulted in the omission of relevant studies and language bias. Second, publication bias may have arisen from the independent selection and screening process, as relevant studies may have been unintentionally excluded. Third, the absence of studies from Latin America limits the geographical representativeness and generalizability of the findings. Fourth, the exclusion of autopsy samples would limit its applicability to pathology archives and research programs that rely heavily on post-mortem samples. Finally, no formal critical appraisal of included studies was conducted to ensure that the most significant and high-quality studies were included.
Conclusion
The use of human biological samples for research is widely recognized as important for advancing science and medicine; it thereby generates strong beneficence-based reasons to facilitate secondary uses. However, this must be balanced with robust protection of autonomy, non-maleficence, and justice across four axes of knowledge, willingness, consent, and governance. Many of the most pressing challenges identified are not gaps in ethical theory but short falls on the implementation, regulation, and oversight. Aligning local practices with the international guidelines discussed – Declaration of Helsinki, CIOMS, UDBHR, the Declaration of Taipei, and GDPPR – can enhance the global applicability and ethical robustness of the use of human biological samples for research, particularly in low-and middle-income settings where histories of exploitation and infrastructural constraints heighten the need for trustworthy, participant-centered governance.
Our findings outline a roadmap for strengthening ethical and regulatory governance for the secondary use of human biological samples for research. First, national and institutional policies should explicitly address secondary use of human biological samples, including clear guidance on the model of consent, timing of consent, and management of clinician-patient power imbalances in hospital settings, ownership, and benefit sharing. Second, institutions should implement standardized governance frameworks for human biological samples to ensure transparent oversight mechanisms, documentation of consent conditions, and clear accountability for secondary use decisions. Third, mandatory, role-specific ethics training should be developed, focusing on the secondary use of human biological samples, consent models, and emerging ethical risks to strengthen ethical decision-making and oversight in practice. Finally, mechanisms for ongoing stakeholders’ engagement, particularly with patients and communities, should be integrated into policy development and review to ensure that ethical guidelines remain contextually relevant and socially responsive.
Best Practices
Many ethical issues concerning the secondary use of human biological samples can be mitigated if the principle of respect for persons is upheld. The autonomy of the individual should be respected, and they should be provided with sufficient information regarding the study. The availability of comprehensive national and institutional policies and guidelines for the harmonization of research involving human biological samples. These guidelines will also be instrumental in ensuring the responsible conduct of research involving these samples. Researchers and REC members are encouraged to undergo training related to research ethics, particularly on the use of clinical samples.
Research Agenda
Many ethical issues were rooted in the governance and structures. There is a need to examine if countries have available guidelines governing the secondary use of human biological samples and evaluate their content
Educational Implication
We synthesized all knowledge from the available literature from different contexts and areas to determine what are the ethical issues and their sources to use as a guide in conducting research using the secondary use of clinical samples ethically. Research participants, researchers, REC members, and other stakeholders involved in the secondary use of clinical samples must be aware of these different issues. Training related to the ethical concerns of the secondary use of samples and applicable guidelines will be useful for the researchers, REC members, and other research stakeholders. Additionally, we also synthesized and tabulated the information that different research stakeholders identified as important in the informed consent process. We also provide a comparative table of the advantages and limitations of the different models of consent in the context of the secondary use of human biological samples.
Supplemental Material
sj-docx-1-jre-10.1177_15562646261452718 - Supplemental material for Ethical Issues on the Secondary Use of Human Biological Samples: A Scoping Review
Supplemental material, sj-docx-1-jre-10.1177_15562646261452718 for Ethical Issues on the Secondary Use of Human Biological Samples: A Scoping Review by Jeniffer Landicho, Chin Hai Teo, and Nishakanthi Gopalan in Journal of Empirical Research on Human Research Ethics
Supplemental Material
sj-docx-2-jre-10.1177_15562646261452718 - Supplemental material for Ethical Issues on the Secondary Use of Human Biological Samples: A Scoping Review
Supplemental material, sj-docx-2-jre-10.1177_15562646261452718 for Ethical Issues on the Secondary Use of Human Biological Samples: A Scoping Review by Jeniffer Landicho, Chin Hai Teo, and Nishakanthi Gopalan in Journal of Empirical Research on Human Research Ethics
Footnotes
Acknowledgment
The authors would like to express their gratitude for the valuable support of the Faculty Members of the Master of Health Research Ethics (MOHRE) programme at Universiti Malaya and Berman Institute of Bioethics, Johns Hopkins University.
Ethical Approval
The study does not involve human or animal participation; thus, informed consent is not required. It was granted an exemption from review by the RITM Institutional Review Board.
Funding
This work was supported by the Fogarty International Center of the United States, National Institutes of Health (Grant R25TW010891) in collaboration with the Berman Institute of Bioethics, Johns Hopkins University, and the Faculty of Medicine, Universiti Malaya, Malaysia.
Declaration of Conflict of Interest
The authors declared no conflict of interests for the research, authorship, and/or publication of this article.
Data Availability Statement
The data used for this review are available upon request by sending an email to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.