
Abstract
Computer-assisted navigation and robotic surgery have gained popularity in the treatment of pelvic bone malignancies, given the complexity of the bony pelvis, the proximity of numerous vital structures, and the historical challenges of pelvic bone tumor surgery. Initial interest was on enhancing the accuracy in sarcoma resection by improving the quality of surgical margins and decreasing the incidence of local recurrences. Several studies have shown an association between intraoperative navigation and increased incidence of negative margin bone resection, but long-term outcomes of navigation in pelvic bone tumor resection have yet to be established. Historically, mechanical stabilization of pelvic bone metastases has been limited to Harrington-type total hip arthroplasty for disabling periacetabular disease, but more recently, computer-assisted surgery has been employed for minimally invasive percutaneous fixation and stabilization; although still in its incipient stages, this procedure is potentially appealing for treating patients with bone metastases to the pelvis. The authors review the literature on navigation for the treatment of primary and metastatic tumors of the pelvic bone and discuss the best practices and limitations of these techniques.
Introduction
Given the challenging 3-dimensional (3D) anatomy of the pelvis, the use of navigation and robotic technologies for primary pelvic bone tumor resection sparked interest over 2 decades ago, as early studies demonstrated its ability to consistently achieve negative margins. Cho et al [9] used fused computed tomography (CT) and magnetic resonance imaging (MRI) to navigate 18 tumor resections, 10 in the pelvis, between 2005 and 2008; they achieved negative margins at the site of bone resection in all 18 cases and 80% 3-year survival for the pelvic malignancies. Wong and Kumta [50] had similar results in 21 patients (11 pelvic cases) treated from 2006 to 2009 using a CT-based navigation system with fused MRI (CT spine, Version 1.6; Stryker Navigation, Freiburg, Germany); they also achieved negative bony margins in all cases, with postoperative analysis demonstrating a difference between achieved bone resection and preoperative planned resection level of ≤ 2 mm. Similarly, a study of 28 patients (8 pelvic cases) treated with CT-guided navigation in Buenos Aires demonstrated minimal differences in planned and achieved bony resection using postoperative CT scans of the resection specimen compared to the preoperative plan [39]. Finally, the Birmingham group examined 31 consecutive patients with pelvic tumors treated with navigated resection between 2010 and 2012 using an oncology-specific navigation system (Stryker OrthoMap 3D Navigation System II; Kalamazoo, MI) with fused MRI and CT [26]. In 23 patients with primary bone tumors, all 23 showed negative bone margins and 21 showed negative soft tissue margins, leading to a 13% local recurrence rate. The authors noted that this was significantly decreased from 27% negative margins and 29% local recurrence from their center’s previously published series of 539 primary pelvic bone tumors treated with conventional techniques.
Shortly after, several in vitro studies demonstrated the improved accuracy of navigated resection technologies compared to conventional techniques. A pilot study using haptic robotic-assisted resection on 12 sawbones resulted in a mean improvement in linear deviation and angular deviation for target planes compared to manual techniques [28]. Cartiaux et al [6] simulated a periacetabular tumor resection using a pelvic bone model and compared manual versus navigated cuts performed by 10 senior and 14 junior surgeons and found no cases of intralesional cuts with the navigation system and a significantly narrower zone of error compared to the desired cut—6.5 mm average deviation with navigation versus 13 mm freehand. The Toronto group, using a cone-beam CT-based C-arm and real-time optical tracking (Polaris; NDI, Waterloo, Ontario, Canada) to compare 90 navigated sawbones cuts to 54 non-navigated cuts, found the navigation system to be accurate and feasible and the navigated cuts to be significantly more accurate than the manual cuts [43]. They determined that with a 5-mm planned margin between the tumor and the cut, they could achieve a negative margin in 95% of cases.
Several authors have examined the learning curve of using navigation for pelvic bone resections, with mixed results. In a 2011 retrospective review, Cheong and Letson [8] found computer-assisted navigation in the resection of bone sarcoma to be helpful in a small, heterogeneous group of patients at their institution, but noted that the surgeries took longer to perform than those not using navigation. Similarly, in evaluating the learning curve in 124 pelvic resections (63% of which were navigated), Farfalli et al [18] found that the earlier navigation surgeries took longer to perform. However, the Birmingham group found navigation to decrease operative time and blood loss in a cohort of 21 patients undergoing posterior ilium and sacrum resections [29]. Finally, Staatz et al [42] reviewed their first 24 cases of navigation-assisted resection and found the mean registration error to be 0.9 mm, indicating the facile use of the technology despite the lack of experience. Also, no navigation-related complication occurred in any of these series, indicating an acceptable learning curve and quick adaptation with experienced oncologic surgeons.
Larger contemporary retrospective series have demonstrated the safety and efficacy of navigation-aided resection of primary pelvic neoplasms. In a retrospective comparative study, Bosma et al [5] demonstrated the significant advantage in the use of CT-based navigation in achieving negative resection margins for pelvic and sacral primary bone sarcoma resections when compared to conventional techniques (81% vs 50%, respectively). In a series of 33 patients with type 2 resections of primary periacetabular tumors, Fujiwara et al [20] demonstrated 91% negative margins with navigated resection versus 82% with non-navigated resection and a 12% local recurrence rate, all in the non-navigated group. In a larger group of 50 periacetabular resections for chondrosarcoma (13 navigated, 37 non-navigated), the same researchers found significant differences in intralesional resection (8% navigated vs 19% conventional), local recurrence (23% navigated vs 56% conventional), and disease-specific survival at 5 years (76% navigated vs 53% conventional) [19]. In the largest series published, Albergo et al [3] reviewed 203 navigated resections, 57% of which were in the pelvis, and reported that all bone margins were negative for tumor but 2 showed positive soft tissue margins. Abraham et al [2] reviewed a series of 24 patients who underwent navigated pelvic resection from 2009 to 2015 and found all bone margins negative but 2 with positive soft tissue margins. Nandra et al [35] studied a series of 23 patients who underwent navigated resection of a primary bone sarcoma of the pelvis from 2010 to 2012 and found that all bone margins were negative but at 59 months of follow-up, the local recurrence rate was 35%, all in soft tissues.
The value of intraoperative navigation in this setting should be ultimately assessed in terms of negative versus positive margins, perioperative complications, local recurrence rate, and survival. Since no randomized clinical trial has been conducted, the clinical benefit of navigation in this setting is judged by comparing retrospective series to pre-navigation data. However, comparing navigation data to earlier non-navigated series introduces an additional confounding factor, as surgeon experience and superior imaging quality are relevant factors affecting the quality of resection. Therefore, recent cohorts are likely biased in favor of improved results regardless of surgical navigation. The small sample sizes of these studies, heterogeneous tumor grades and stages, and short follow-up, as well as the aforementioned limitations, lead to inconclusive evidence regarding long-term disease-specific survival. These studies not only highlight the improved accuracy of bone resection using computer-assisted navigation for pelvic tumors, but also consistently demonstrate its limitations with regard to the soft tissues. While negative bone resection margin is an essential component for successful sarcoma surgery, soft tissue tumor extension and dissection appear to be an even more critical factor in predicting the quality of surgical margin and local recurrence. Technologic advances and integration of CT and MR imaging in the navigation systems will likely improve the accuracy and current shortcomings regarding soft tissues. Meanwhile, surgeons may still use different navigation technologies and manufacturers to accurately plan and execute bone resections throughout the pelvis, but need to pay close attention to the soft tissue extension and margin of resection (Fig. 1).
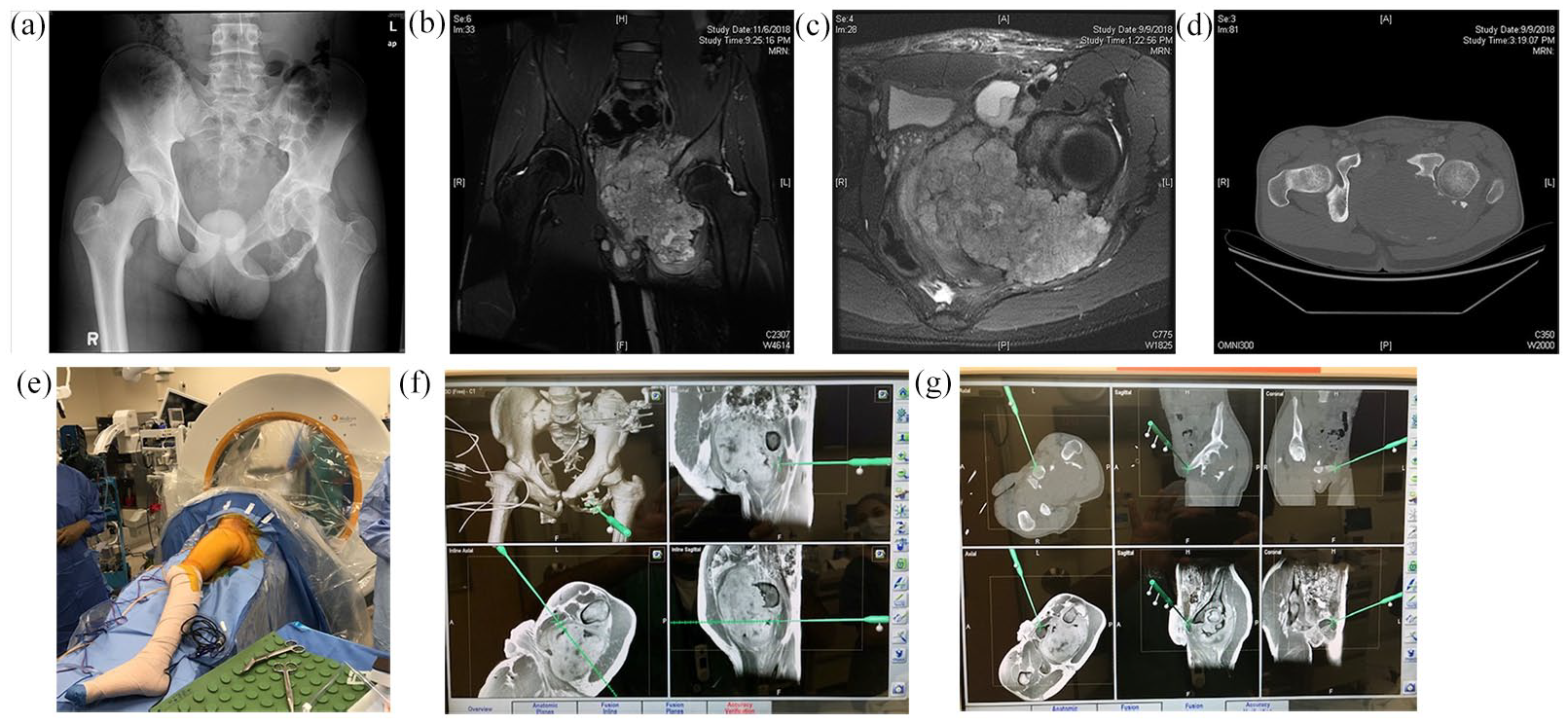
Plain radiograph (a), sagittal (b) and coronal (c) MRI images, and axial (d) CT scan of a 16-year-old male with histologically proven low-grade chondrosarcoma of the left acetabular and ischial region. The tumor presented with marked intrapelvic extension, compression/displacement of the prostate and rectum, and abutted the base of the left corpus cavernosum. The patient underwent preoperative MRI and image fusion was obtained after intraoperative CT scan. (e) The patient was positioned loose lateral on a Brainlab Airo Mobile CT Scanner Navigation System and different fusion windows were used based on anatomic tumor extension (f, g). The tumor was resected with negative bone and soft tissue margins. The patient remains disease free at 2.5 years from surgery. MRI magnetic resonance imaging; CT computed tomography.
Technical concerns in the use of computer navigation include software and hardware crashes, registration failure, increased operating room footprint of imaging and navigation machines, increased time for intraoperative set-up, and tracker-associated nerve injury. While initial studies demonstrated increased operative time, others have demonstrated decreased operative time, as well as good registration reliability. This will likely continue to improve as orthopedic surgeons become more confident with these technologies. Similarly, reports of tracker-related injury are rare. Systems such as the Airo Mobile CT Scanner Navigation System (Brainlab AG, Munich, Germany) are decreasing the operating room footprint compared to previous technologies and allowing for more efficient set-up and scanning, as well as integration of MRI data. Lastly, computer navigation can be compared to patient-specific instrumentation (PSI), another technology gaining popularity in orthopedic surgery. While a full discussion is outside the scope of this article, PSI in musculoskeletal oncology usually involves 3D cutting guides placed against the bone to perform planned resections. PSI is relatively simple and efficient, with minimal additional footprint in the operating room. However, it can require additional dissection to place the guides on uninvolved bone, cannot accommodate intraoperative adjustments, and does not assist with soft-tissue resection. While both technologies are increasingly used, the optimal setting for each is yet to be established.
Navigation for Fixation of Pelvic Metastases
The skeleton is the third most common site of metastases after the lung and the liver, and the pelvis is the third most common site in bone after the thoracic spine and the femur, comprising 19% of all skeletal metastases [10,37]. Primary cancers of the prostate (32%) and the breast (22%) are the most common metastasizing to bone, along with kidney, lung, and thyroid cancers accounting for more than 80% of metastatic bone disease [1]. In 2008, it was estimated that over 280,000 adults in the United States were living with metastatic cancer to bone, and it is now estimated to be over 350,000 [25,31]. These patients will have a skeletally related event every 3 to 6 months [10]; cancer survival has increased over the past 4 decades, and patients require a tailored approach to relieve pain and maintain function [41].
The mainstay of nonsurgical management for symptomatic bone metastases remains radiation therapy [23,27]. However, nearly 50% of patients have residual pain not amenable to reradiation, implying the need for mechanical stabilization [49]. Antiresorptive agents, including primarily bisphosphonates and denosumab, play an important role in decreasing pain and preventing skeletal events but do not obviate the need for mechanical stabilization [11,36]. Scoring systems have been established and validated to predict completion of impending pathologic fractures in long bones, but a clinical algorithm does not exist for the pelvis, where the decision to pursue surgical treatment is based on the surgeon’s clinical assessment, training, and experience [13,17,33,47].
To date, the majority of surgical management of metastatic disease of the pelvis has focused on periacetabular disease and complex hip reconstruction [22,32,46]. Until recently, little attention has been paid to either extra-acetabular disease or diffuse involvement of the entire hemipelvis, due to the morbidity of open surgery in patients with limited life expectancy and lack of reliable alternatives. Over the past 2 decades, minimally invasive local strategies have been developed, including thermal ablation, cementoplasty, and a combination of these methods [30,40,48]. Several authors have combined these techniques with additional screw augmentation to enhance skeletal stability [4,24,38]. Despite clinical success, evidence on the role of these local strategies is not established. They do not address mechanical symptoms associated with significant structural deficiency of impending or current pathologic fractures and should still be considered as a short-term strategy for low-demand patients with limited life expectancy.
Surgical navigation for minimally invasive screw placement has been shown to be accurate for percutaneous fixation of pelvic fractures [12,14,34,45]. Furthermore, it has been demonstrated to be more accurate than standard fluoroscopic guidance for iliosacral screw placement and helpful for less-experienced surgeons [44,52,53,54]. This improved accuracy is especially important for unusual locations and trajectories of fixation, as pathologic fractures may not always occur in locations amenable to screw placement under standard fluoroscopy, such as the anterior column, posterior column, anterior to posterior supra-acetabular region, and ilio-sacral corridors.
Ebraheim and Biyani first reported on percutaneous screw fixation for pathologic fractures of the sacroiliac region using CT guidance [16]. In 6 patients, they demonstrated an average improvement of visual analog scale (VAS) pain scores from 9 to 2.8 at 1 week postoperatively; at 18 months, the 4 surviving patients reported persistent benefit. Cazzato et al [7] reviewed percutaneous, image-guided fixation in an interventional radiology setting of 36 lesions, 25% of them in the pelvis, and noted clinical improvement in 87% of patients at 1 month. An interventional radiology study of 64 patients treated for oncologic disease of the pelvis with CT-guided, percutaneous screw fixation found, in 33 patients with completed pathologic fractures, VAS scores decreased from 80/100 to 20/100; in 10 patients with impending fractures of the ilium, no fractures occurred after percutaneous screw placement and cementoplasty [15]. Finally, an orthopedic group evaluated 20 patients treated with a novel, fluoroscopy-guided percutaneous technique of cannulated screw insertion described as a tripod formation for painful pelvic metastases [51]. The authors demonstrated significant improvements in VAS and Eastern Cooperative Oncology Group scores; 15 of 16 living patients remained ambulatory at final follow-up, and 4 patients were later converted to cemented total hip arthroplasty for incomplete pain relief. However, the authors felt that the reinforcement provided by this technique was helpful for the stability of the acetabular component during hip arthroplasty. While these cases were not navigated, they illustrate the benefits of percutaneous screw fixation for metastatic disease of the pelvis. Finally, the current authors have reviewed their initial experience and described the preferred technique using the Medtronic O-arm/Stealth Navigation System or the Brainlab Airo Mobile CT Scanner Navigation System [21]. We demonstrated the ability to place cannulated screws safely across a variety of trajectories and the durability of these constructs, which can be augmented with bone cement. Fenestrated screws from different manufacturers are now available for this purpose and may be selectively used to enhance cement extrusion and maximize fixation. We anticipate the use of navigation only to grow in this clinical setting, as surgeons are tasked with providing safe, less invasive and durable options to stabilize and palliate complex metastatic lesions of the pelvis in a patient population with increasing life expectancy (Fig. 2). In summary, navigation-assisted percutaneous fixation offers the advantages of decreased radiation and likely more accurate screw placement than fluoroscopic guidance, especially in unconventional trajectories that may be required in the oncologic setting. The learning curve for this technology appears to be minimal, and differences in operative time compared to fluoroscopy have yet to be studied. However, initial reports, including ours, are promising, and should generate increased interest in and scholarship regarding this technique.
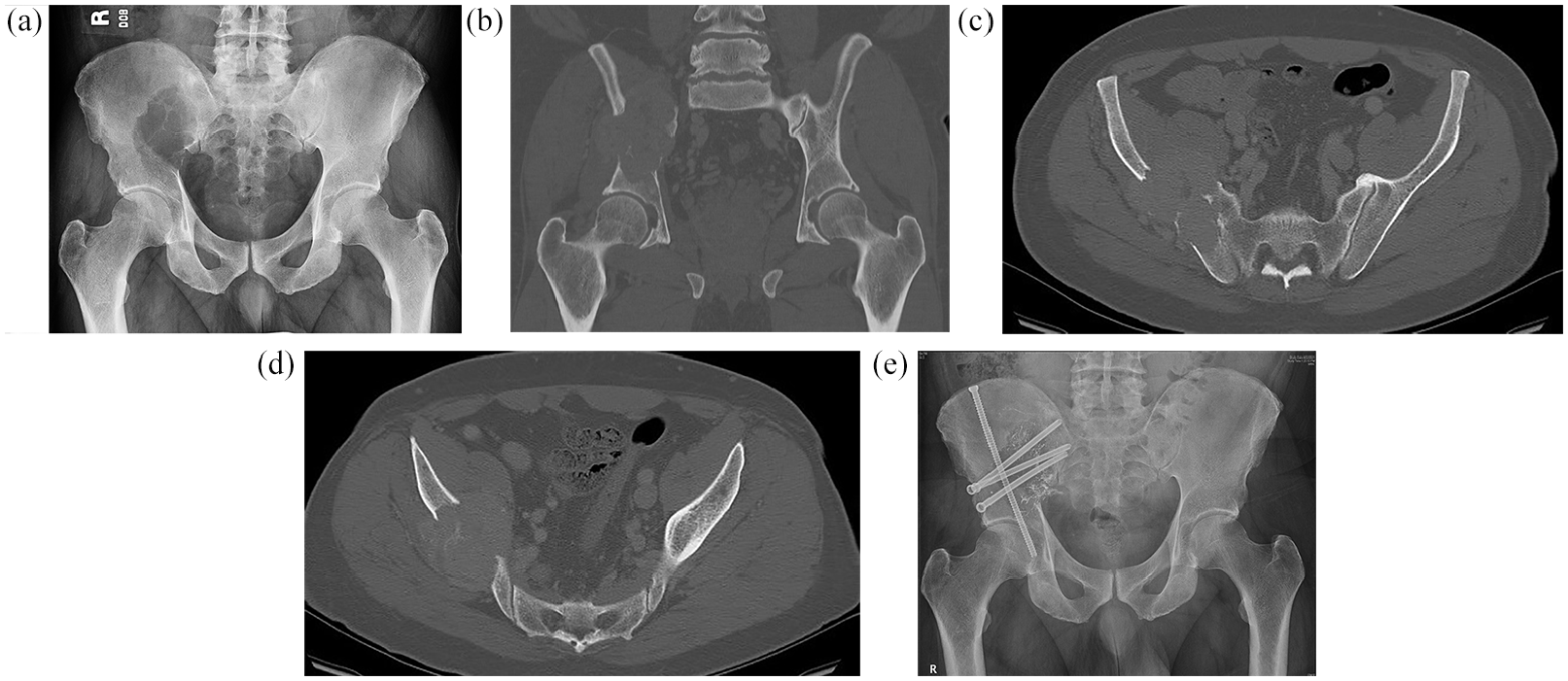
Plain radiograph (a), and coronal (b) and axial (c, d) computed tomography images of a 67-year-old man who presented with disabling pain of the right hip and hemipelvis and a history of clear cell renal cancer status-postnephrectomy 7 years prior. Imaging demonstrated extensive bone destruction and soft tissue involvement due to a large metastatic lesion of the peri-/supra-acetabular and sacroiliac region. After preoperative selective arterial embolization, the patient underwent computed tomography-guided percutaneous fixation with multiple 6.5 mm cannulated screws (Asnis III Cannulated Screw System, Stryker) with a nearly orthogonal trajectory to maximize mechanical stability (e). Postoperative radiation (30 Gy in 3 fractions) was given at 2 weeks from surgery. The patient remains fully ambulatory, functions independently, and does not require narcotics at 7 months from surgery.
In conclusion, computer-assisted surgical navigation in the treatment of pelvic primary malignancy and metastatic cancer continues to increase in both popularity and utility. The ability of navigation to predictably increase resection accuracy and obtain negative bone margins in bone sarcomas has been clearly established, with variable benefits based on comparative and ideally contemporary non-navigated data. However, long-term data regarding disease-specific survival is lacking, and the majority of the data available is from small, level IV retrospective series. Prospective data collection and rigorous comparison with contemporary non-navigated data are critical for full appreciation of the clinical benefit and cost/analysis assessment. Further work in terms of technological advances and further experience is needed to improve the effectiveness of soft tissue navigation and resection.
There is increasing interest in the use of the anatomic accuracy of surgical navigation to facilitate minimally invasive percutaneous fixation of impending and actual pathologic fractures of the pelvis due to metastatic cancer, with emphasis on pain palliation, reduced morbidity, and improved quality of life. This indication for navigation is very appealing, as these patients have limited physiologic reserve and life expectancy and stand to benefit from less morbid procedures, increased mobility, and reduced opioid use. However, indications for these procedures are not well-established and represent work in progress where further prospective research is needed to define ideal clinical applications in the setting of metastatic cancer to bone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John H. Healey, MD, reports relationships with Stryker; Daiichi-Sanyo; AAOS; Association of Bone and Joint Surgeons; Musculoskeletal Transplant Foundation; Musculoskeletal Tumor Society; Orthopaedic Research and Education Foundation; Orthopaedic Research Society; Lumicell; IlluminOss; and Clinical Orthopaedics and Related Research. Nicola Fabbri, MD, reports relationships with Memorial Sloan Kettering Cancer Center Device Design and Development Fund; Springer; IlluminOss; Onkos Surgical; Smith & Nephew, Inc.; National Comprehensive Cancer Network; Musculoskeletal Tumor Society; Association of Bone and Joint Surgeons; and European Journal of Surgical Oncology. The other authors report no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not necessary for this review article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.