
Abstract
Background: Coccygodynia has been described as a disabling pain in the coccyx usually associated with sitting or with changing position from a sitting to a standing position. Pain may radiate to the sacrum, to the lumbar spine, or laterally to the buttocks. Treatment has rarely been studied in the adolescent population. Purposes/Questions: This study aimed to assess pain relief and satisfaction after partial or total coccygectomy in pediatric and adolescent patients suffering from coccygodynia that was resistant to conservative treatment. Methods: A retrospective, consecutive case series was performed to review the data from the hospital records of 29 patients who underwent partial or total coccygectomy from January 2016 to January 2020 in a university hospital setting. Patients suffered from coccygodynia resistant to conservative treatment. The study included 16 female (55%) and 13 male (45%) patients who ranged in age from 3 to 15 years. Patient records were assessed for postoperative complications, period of hospital stay, time to regain normal activity, postoperative pain improvement (using a 4-point Likert scale), and patients’ or parents’ satisfaction (using a 5-point questionnaire). Results: Total coccygectomy was performed in 19 patients and partial coccygectomy in 10 patients. Only 1 patient had a superficial infection after surgery. The length of hospital stay was 1.44 ± 0.97 days. Time to regain normal activity was 24.68 ± 4.32 days. Pain relief was excellent (complete pain relief) in 23 cases (79.3%) and good (relief of most pain but mild discomfort after prolonged sitting) in 6 cases (20.7%). There were no reports of fair (minimal or no pain relief) or poor (pain worse than before surgery) pain relief. In terms of patient or parent satisfaction, no one reported being “absolutely dissatisfied,” 1 person was “dissatisfied” (3.4%), 3 people were “neither dissatisfied nor satisfied” (10.4%), 9 were “satisfied” (31%), and 16 were “absolutely satisfied” (55.2%). Conclusion: This case series suggests that coccygectomy may be a feasible management option for pediatric and adolescent patients, with favorable outcomes including pain relief, patient or parent satisfaction, and early return to activity.
Introduction
Any problem with the coccyx can produce pain and tenderness and cause radiating complaints [1-4]. In 1859, Simpson described coccygodynia as an incapacitating pain in the coccyx stimulated by sitting or changing position from a sitting to a standing position. Pain may radiate to the sacrum, to the lumbar spine, or laterally to the buttocks. Rectal pain or radicular symptoms present rarely; however, one-third of patients with coccygodynia have associated back pain [2-18]. Coccygodynia is categorized as either posttraumatic or idiopathic; true coccygodynia must be distinguished from pseudo-coccygodynia, in which pain is referred to the coccygeal region from visceral organs, dural irritation, or a radiculopathy. It can be classified as acute or chronic, the latter defined as pain lasting more than 2 months [16].
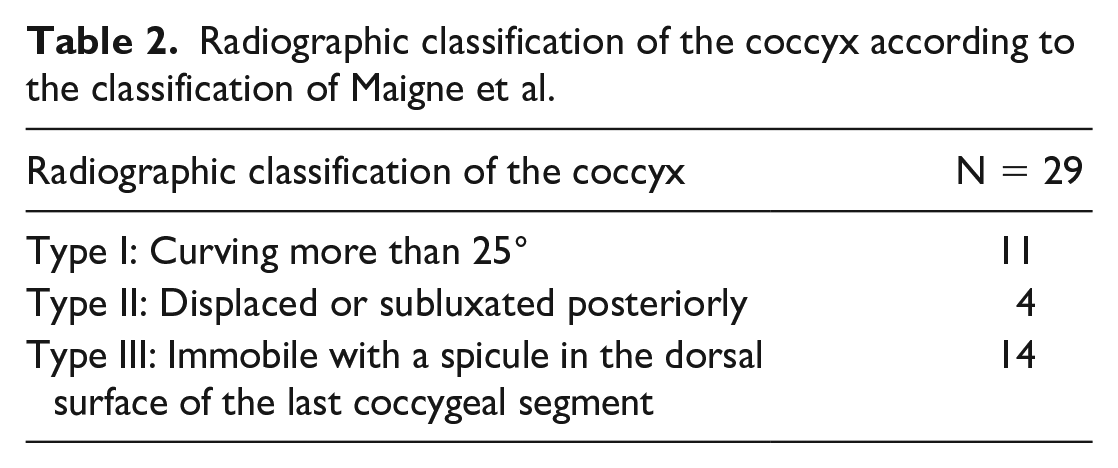
Maigne et al described 3 types of coccyx abnormality. The first is an anterior curvature of more than 25°. The second is a hypermobile or dislocated coccyx [12,15], and the third is a coccygeal spicule, a minor bony projection on the dorsal aspect of the tip of the coccyx that is evident on radiologic evaluation [5]. The second and third types are often best treated surgically [11].
Symptoms of coccygeal spicule occur most frequently in patients with a rigid coccyx. The spicule irritates the subcutaneous soft tissue while sitting down, especially on hard seats. In the initial description, a pit of greater or lesser depth in the skin overlying the spicule (or a little higher in the natal cleft) is present in 60% of cases. Although this pit is usually discreet, it can be a frank retro-coccygeal pilonidal sinus. The pit is considered to be evidence of the embryonic origin of malformation [11]. Maigne et al [13] reported that spicules are the most common cause of coccygodynia in adolescents. In adults, they appear to represent 15% of cases of common coccygodynia [11]. A fourth type of coccyx abnormality is characterized by a subluxation in the sacrococcygeal or intercoccygeal joint.
Preliminary management consists of ergonomic adjustments such as a specialized pillow for sitting, application of local heat, and oral analgesics. Favorable results are reported after using local injections of steroids and/or local sodium channel–blocking anesthetic agents [19-23]. Additional measures include repetitive hyperflexion and hyperextension of the coccyx under general anesthesia. A gloved finger placed transrectally with gentle massage in the direction of the fibers may relax and release the soft tissue, ligaments, and muscles attached to the coccyx; the finger may then be placed on the coccyx, which may then be gently pushed posteriorly into its normal position. The most aggressive management for this condition involves surgically removing the coccyx [1,2,18,17,19].
The aim of this study was to evaluate the ability of coccygectomy to relieve the pain of persistent coccygodynia in adolescent and pediatric patients. Secondary outcomes assessed included postoperative complications, length of hospital stay, time to regain normal activity, and patient or parent satisfaction.
Methods
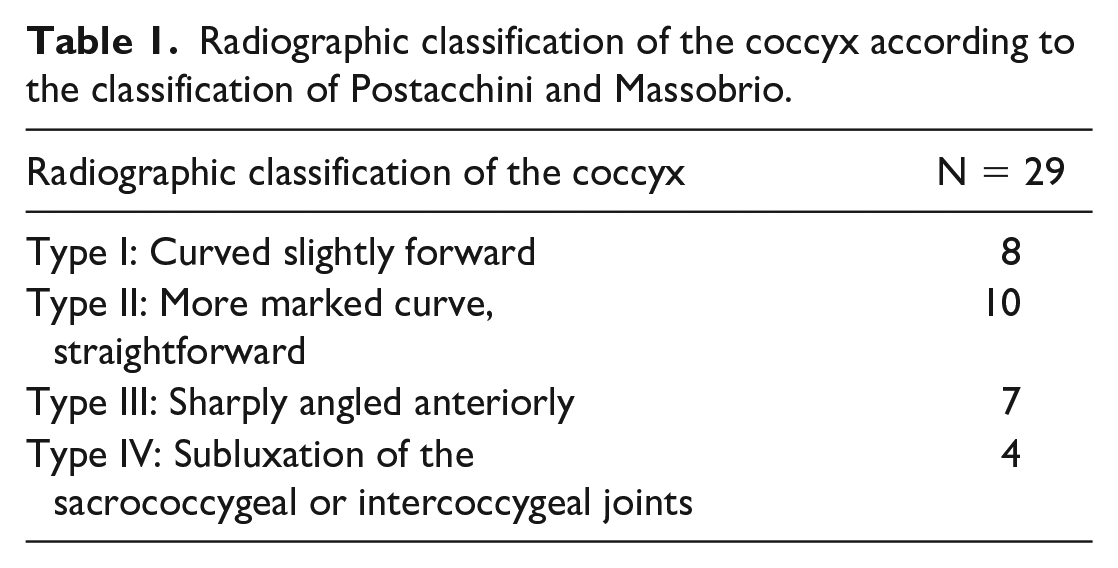
A retrospective consecutive case series of 29 pediatric patients who underwent partial or total coccygectomy was conducted. They were suffering from pain while sitting or changing positions from a sitting to a standing position; the pain radiated to the sacrum, to the lumbar spine, or laterally to the buttocks. The diagnosis was established through history and physical examination, based on the presence of pain at the tip of the coccyx and palpation of a painful bony projection beneath the skin. Anteroposterior and lateral radiographs of the sacrum and coccyx before surgery determined the anatomical configuration and the type of coccyx according to the classifications of Postacchini and Massobrio [19] and Maigne et al [12,15] (Tables 1 and 2).
Radiographic classification of the coccyx according to the classification of Postacchini and Massobrio.
Radiographic classification of the coccyx according to the classification of Maigne et al.
Before coccygectomy, all patients underwent nonoperative conservative treatment modalities for 6 months. These included application of local heat, oral analgesics including nonsteroidal anti-inflammatory drugs (NSAIDs), ergonomic adjustments such as specialized pillows for sitting, and at least 1 sacrococcygeal local injection of lidocaine mixed with triamcinolone 40 mg. All cases were resistant to treatment.
The study was approved by the hospital’s institutional review board. The parents or legal guardians of each patient were informed about every step of the operation, and informed consent was obtained. The privacy of the participants and the confidentiality of the data were maintained.
Data were collected from medical records of 29 patients who underwent 29 coccygectomies performed in the pediatric surgery unit and affiliated hospitals within a single university hospital system, from January 2016 to January 2020. Data included patient demographics (age, sex, race, and nationality), duration of symptoms and clinical findings, preoperative radiographic imaging of the sacrum, period of hospital stay, time to regain normal activity, and occurrence of postoperative complications. Postoperative pain improvement was assessed by a 4-point Likert scale, and patients’ or parents’ satisfaction was determined with a 5-point questionnaire. The study included 16 female (55%) and 13 male (45%) patients, ranging in age from 3 to 15 years (mean: 9 ± 2.3 years). The results of the pathologic types of coccyx according to the classification of Postacchini and Massobrio [19] and Maigne et al [12,15] were tabulated (Tables 1 and 2) (Figs 1 and 2).
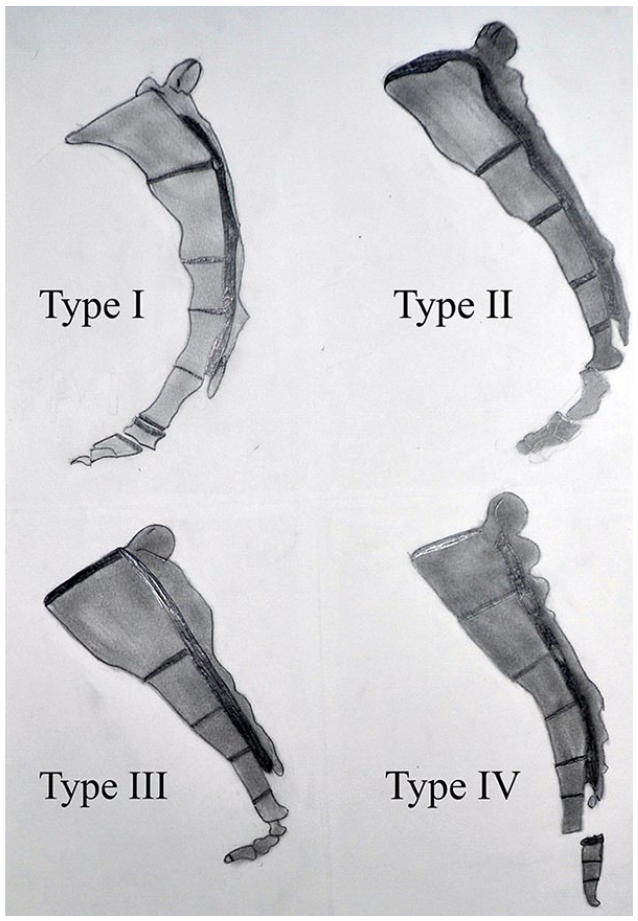
The classification of coccyx according to Postacchini and Massobrio.[19]
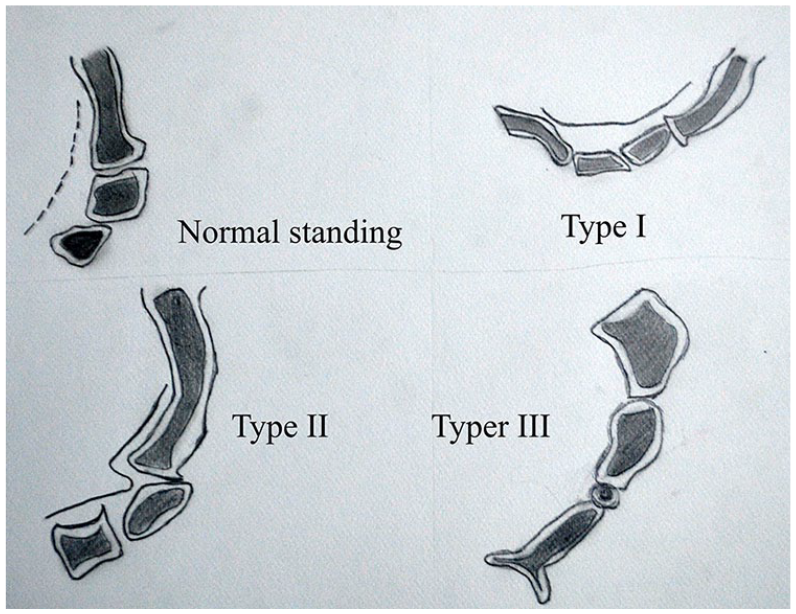
The types of coccyx according to the classification of Maigne.[12,15]
For all patients, the surgical procedure began with receiving a bowel preparation preoperatively to prevent fecal contamination of the wound and to minimize complications in the unlikely event of rectal perforation. A third-generation antibiotic (ceftriaxone) was administered prophylactically before skin incision. Surgery was performed with the patient in the prone position under general anesthesia. The buttocks were retracted laterally with adhesive tape to expose the gluteal cleft. The operative technique used consisted of approaching the terminal coccygeal segment directly via a small vertical incision in the natal cleft, followed by exposure from a proximal to distal direction. The coccyx was elevated and separated from the surrounding tissues circumferentially in a subperiosteal plane using monopolar electrocautery, proceeding with an en bloc resection and removing the terminal coccygeal segment completely or partially according to the affected length of the coccyx (Figs 3 and 4).
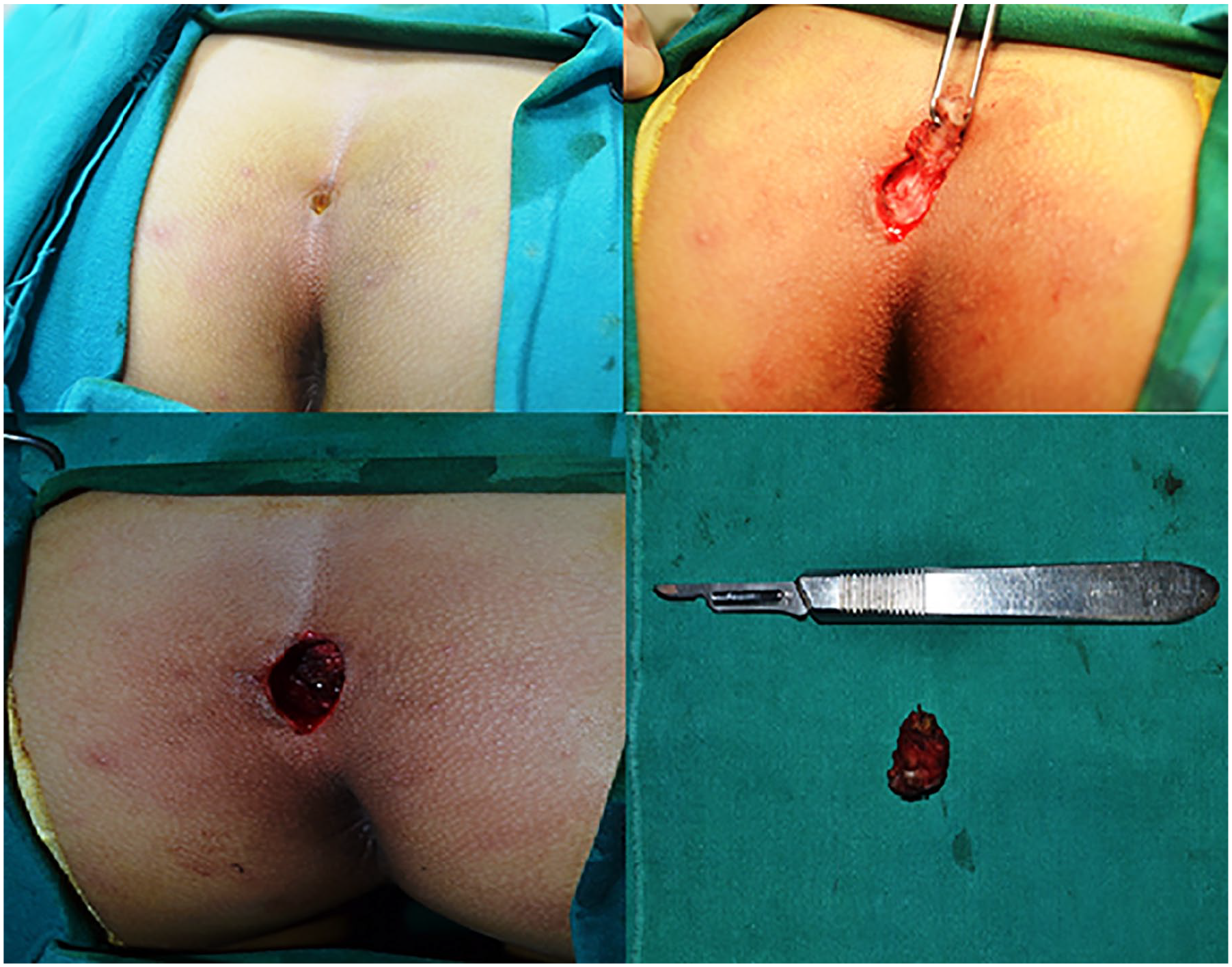
Sacral pit and complete coccygectomy.
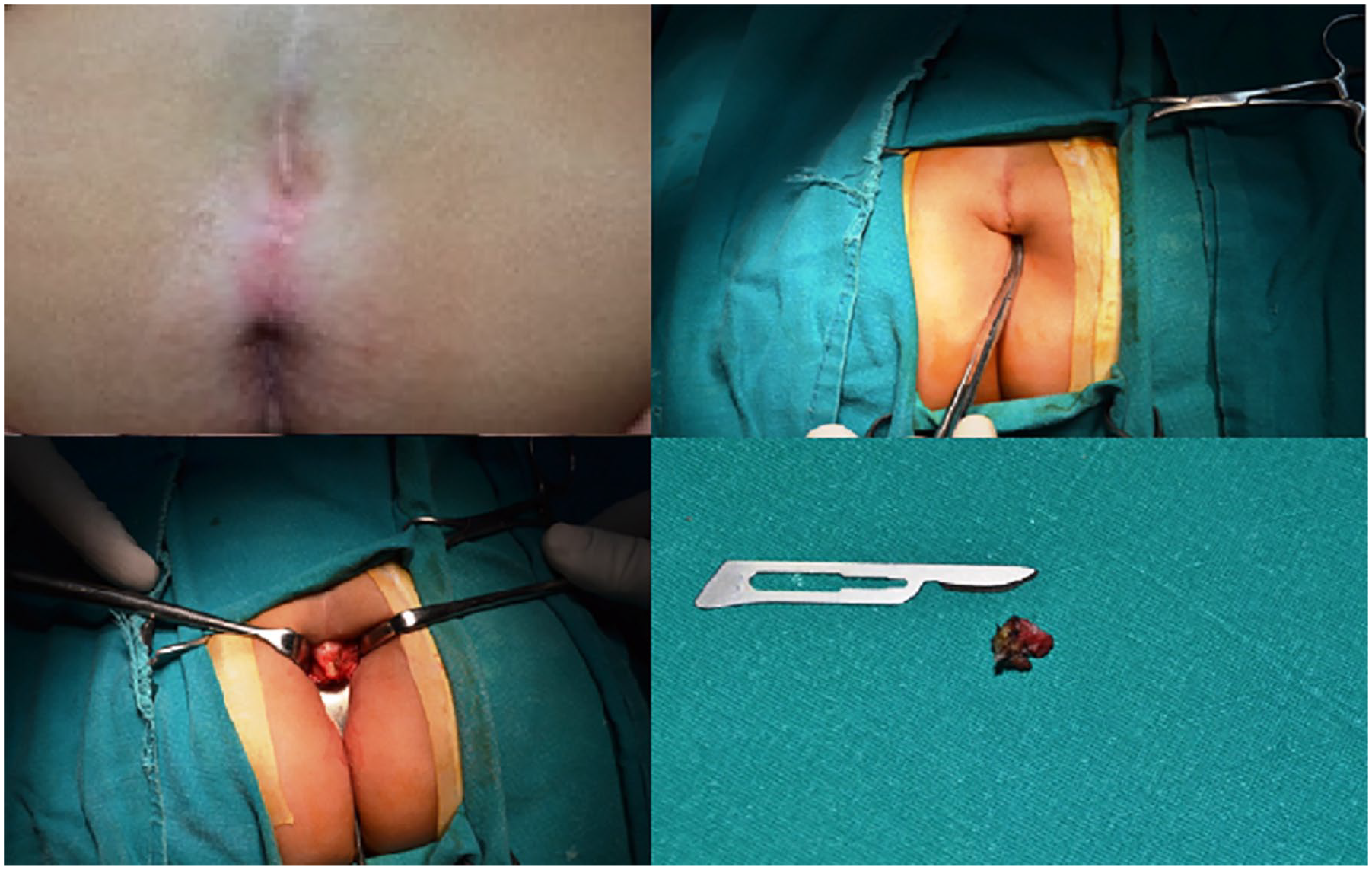
Partial coccygectomy for coccygeal spicule.
The wound was irrigated with normal saline and closed in 2 layers without a drain. A water-resistant adhesive covering was then applied to the wound.
All patients received postoperative analgesia for 2 days and were discharged home on the day of surgery if they were tolerating oral feeding, had pain well controlled, and the wound was clean and dry. Patients received nursing care in a lateral position to avoid direct pressure on the surgical wound. They were instructed not to sit for at least 3 weeks following surgery pending suture removal and to avoid straining for 3 months. Clinical results including improvement in pain were assessed by a 4-part Likert scale. Pain relief was qualified as “excellent” (complete pain relief), “good” (relief of most pain but mild discomfort after prolonged sitting), “fair” (minimal or no pain relief), or “poor” (pain worse than before surgery). Patients and parents were also queried about their satisfaction with the procedure; satisfaction was assessed with a 5-point scale: “absolutely dissatisfied” = 1 point, “dissatisfied” = 2 points, “neither dissatisfied nor satisfied” = 3 points, “satisfied” = 4 points, and “absolutely satisfied” = 5 points.
Surgeons followed up with their patients in 3-month intervals for the first year. All patients completed 12 months of follow-up.
Results
In all, 19 patients underwent total coccygectomy and 10 patients had partial coccygectomy. There was 1 case of superficial infection treated with oral antibiotics, but no significant surgical complications. The length of hospital stay ranged from 1 to 3 days (mean: 1.44 ± 0.97 days). Time to regain normal activity ranged from 21 to 29 days (mean: 24.68 ± 4.32 days).
In assessing postoperative pain improvement, 23 patients (79.3%) considered the results “excellent” (complete pain relief), and 6 patients (20.7%) considered them “good” (relief of most pain but mild discomfort after prolonged sitting). No one reported results that were “fair” (minimal or no pain relief) or “poor” (pain worse than before surgery) (Table 3).
The 4-scale score for pain improvement postoperatively.

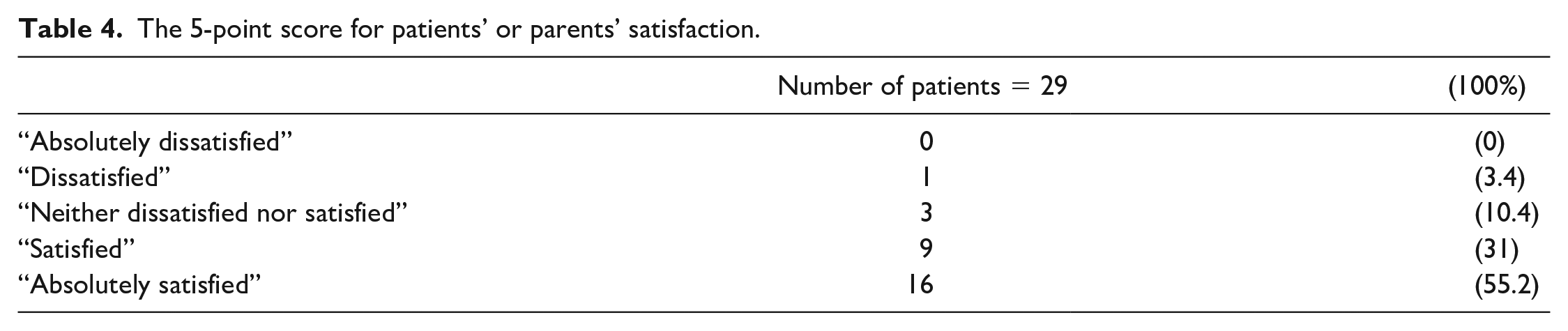
When assessing patients’ or parents’ satisfaction with the 5-point score, no one was “absolutely dissatisfied” and 1 person (3.4%) was “dissatisfied” due to wound infection and frequent outpatient clinic visits. Three people (10.4%) were “neither dissatisfied nor satisfied” due to unexpected mild discomfort after prolonged sitting. Finally, 9 people (31%) were “satisfied” and 16 (55.2%) were “absolutely satisfied” (Table 4).
The 5-point score for patients’ or parents’ satisfaction.
Discussion
The aim of this study was to report on a series of pediatric patients treated for persistent coccygodynia with coccygectomy. Pain relief and patient satisfaction with the procedure were good to excellent.
This study has several limitations. First was a limited follow-up period. Second, this was a retrospective study subject to selection bias, and as a single institutional case series the results may not be generalizable. All patients were treated after failed conservative care, and therefore coccygectomy cannot be evaluated as a primary approach.
In this study, the average duration of pain before surgery was 6 months. It included 29 patients, 13 male and 16 female; this contrasts with the gender distribution reported by Karadimas et al [10], who reported that the preponderance of the patients (including both adults and children) were female, with a ratio of 4.4/1. The ages in this study ranged from 3 to 15 years, in contrast to most studies that include primarily adults. All cases had undergone nonoperative treatment modalities for 6 months, in agreement with other reported studies [8,9].
Using the radiographic configurations established by Postacchini and Massobrio, this study found that 27% of the patients were type 1 classification, 34% were type II, 24% were type III, and 13% were type IV (Table 1). In comparison, Karadimas et al [10], in a review of the literature, analyzed 153 adult and pediatric radiographs and found that 37% were type I classification, 31% were type II, 19% were type III, and 12% were type IV. Grosso and van Dam reported that 4 out of 5 of their patient population were in group II, III, or IV [7]. Postacchini et al [19] found that in a study of 120 asymptomatic patients, 68% had a type I configuration.
Wound infection is the most frequently reported complication. To reduce the infection rate after coccygectomy, other studies have proposed various strategies, such as antibiotic prophylaxis before or after surgery, longitudinal incision [8], use of a drain, periosteal preservation, and meticulous closure [3]. In this study, a low-residue diet and enema were used before surgery to prevent contamination of the wound during the operation, while intravenous administration of third-generation cephalosporin (ceftriaxone) was used to prevent infection after surgery. In a review of the literature, Karadimas et al found that perioperative use of antibiotics was recorded in all studies except 1 [2,10]. Pennekamp et al [17] observed wound infection in 19% of the patients in their study, whereas Sehirlioglu et al [20] reported that 7% of the patients in their study developed a complication directly associated with the surgical procedure. This study had only 1 case of superficial infection and it was treated with oral antibiotics. Other studies have reported rates of infection ranging from 7% to 19% [17,20]. No other significant surgical complications were encountered in this study.
Scores for pain improvement postoperatively were excellent in 80% of patients and good in the remaining 20% of cases, and the parents were quite satisfied in almost all cases. Improvement in pain is also reported in other reports, with excellent or good outcomes in 84.6%, fair outcomes in 7.7%, and poor outcomes in 7.7% [2,3,19,22,23].
In conclusion, coccygodynia can be a disabling problem in pediatric and adolescent patients. Although the number of cases in this study is small, the findings suggest that coccygectomy may be a feasible and successful solution for pediatric and adolescent patients. Further study is warranted.
Supplemental Material
sj-pdf-1-hss-10.1177_1556331621991498 – Supplemental material for The Surgical Role in the Management of Persistent Coccygodynia in Adolescent and Pediatric Patients: A Retrospective Case Series
Supplemental material, sj-pdf-1-hss-10.1177_1556331621991498 for The Surgical Role in the Management of Persistent Coccygodynia in Adolescent and Pediatric Patients: A Retrospective Case Series by Mohamed M. Shalaby in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV: Therapeutic Study
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.