
Abstract
Background: Grit, defined as perseverance and passion for long-term goals, and self-control, defined as the capacity to regulate impulses in the presence of momentarily gratifying temptations or diversion, have shown to be predictors of professional achievement. Their role in health care outcomes is less well understood. Purpose: We sought to determine whether grit and self-control are associated with patient-reported outcome measures (PROMs) following spine surgery. Methods: We conducted a retrospective review of adult patients who underwent cervical or lumbar procedures by a single fellowship-trained spine surgeon between March 2017 and October 2020. We included patients who underwent anterior cervical discectomy and fusion, cervical disk replacement, minimally invasive laminectomy/laminoplasty (MI-D), or minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) with minimum 1-year follow-up. Grit and self-control scores were collected 1 year after the surgery. PROMs were collected preoperatively and at 6 postoperative timepoints. Grit and self-control were compared between patients who achieved substantial clinical benefit (SCB) in either physical or mental health versus those who did not. The association between grit/self-control and change in PROMs was also assessed. Results: In the 129 patients included in the analysis, we found that patients who achieved SCB in mental health had significantly higher grit scores than those who did not. In bivariate analysis, self-control was associated with greater improvement in leg pain scores at 1-year and 2-year follow-up following an MI-D. For the MI-TLIF cohort, grit was associated with a smaller change in Short Form 12 mental component score at 6 weeks, and self-control was associated with a smaller change in Patient-Reported Outcome Measurement Information System Physical Function at the 6-month timepoint. Grit and self-control were not associated with PROMs at other timepoints. Conclusion: This retrospective review found that grit and self-control were not significantly associated with PROMs at most postoperative timepoints in patients who underwent spine surgery.
Keywords
Introduction
Over the past few decades, there has been an increase in the number of patients whose outcomes following spine surgery did not meet the patient’s and surgeon’s presurgical expectations, and this trend is expected to continue [2,16]. Many of these reports are based on analyses of patient-reported outcome measures (PROMs), which are a widely accepted tool for the measurement of outcomes in spine surgery [2,6]. Moreover, there is often disagreement between the patient and the surgeon on surgical outcomes; 1 study found that 24% of patients disagreed with their surgeon’s postoperative assessment [13]. Why some patients fail to achieve significant clinical improvement in pain and disability following spine surgery remains 1 of the field’s most studied and discussed topics.
According to psychological research, 2 highly correlated characteristics, grit and self-control, are significant determinants of success in a number of domains [4]. Grit is a noncognitive trait defined as perseverance and passion for long-term goals [4], and it has been studied as a factor in outcomes in patients with substance use disorder and type 2 diabetes [7,11]. Self-control is defined as the capacity to regulate attention, emotion, and behavior in the presence of temptation [3]. Given that grit and self-control have been associated with success in various areas, we decided to study whether this construct can help to elucidate why certain patients experience better or poorer clinical outcomes after spine surgery.
The purpose of this study was to determine whether patients’ grit and self-control scores would be predictors of outcomes following spine surgery. We hypothesized that patients with higher grit and self-control scores would have greater improvement in their PROMs following spine surgery. To our knowledge, this is the first study assessing grit and self-control in patients undergoing spine surgery.
Methods
A retrospective review was performed involving adult patients (aged 18 to 80 years) who underwent cervical or lumbar procedures by a single fellowship-trained spine surgeon between March 2017 and October 2020. Patients included in the study underwent anterior cervical discectomy and fusion (ACDF), cervical disk replacement (CDR), minimally invasive laminectomy/laminoplasty (MI-D), or minimally invasive transforaminal lumbar interbody fusion (MI-TLIF). Patients who had a minimum of 1-year follow-up were included.
Following institutional review board approval, patient demographic information and PROMs were reviewed retrospectively from a single-institution, single-surgeon, prospectively maintained database. PROMs are collected from the database by trained research assistants either during a clinic appointment or via an emailed survey. PROMs collected include the visual analog score for back pain (VAS Back), visual analog score for leg pain (VAS Leg), Short Form 12 mental component score (SF-12 MCS), and Patient-Reported Outcome Measurement Information System Physical Function (PROMIS PF). Additionally, grit was assessed using the previously validated 8-question Short Grit Scale [5]; self-control was assessed using the 10-item Self-Scoring Self-Control Scale, which was adapted from the previously validated 13-item survey [15] (Supplemental Table 1). The maximum score for both scales is 5 (extremely gritty/most self-control), and the lowest score on this scale is 1 (not at all gritty/least self-control) [5,15]. In addition, VAS Back, VAS Leg, SF-12 MCS, and PROMIS PF scores were collected preoperatively and postoperatively at 2 weeks, 6 weeks, 12 weeks, 6 months, 1 year, and 2 years. Grit and self-control scores were only collected at the 1-year timepoint.
Data were collected and managed using Research Electronic Data Capture (REDCap) [8,9] and supported by the following grant: CTSC GRANT UL1 TR002384. REDCap is a secure, Health Insurance Portability and Accountability Act–compliant Web-based software platform designed to support data capture for research studies.
Statistical Analysis
Patients were first sorted into 2 cohorts, regardless of the type of surgery, based on whether a substantial clinical benefit (SCB) was achieved, using the SF-12’s anchor question: “How does your mental/physical health compare to that 1 year ago?” For both physical and mental health, SCB was achieved if the patient answered “much better” out of the 5 possible responses (much worse, slightly worse, about the same, slightly better, or much better), in accordance with a previously published methodology [14]. Using independent samples student’s t tests, grit and self-control scores were compared between physical health SCB achieved vs physical health SCB not achieved as well as mental health SCB achieved vs mental health SCB not achieved.
A bivariate analysis was then performed for MI-D and MI-TLIF subgroups to assess for the association between grit/self-control and change in PROMs at various postoperative timepoints. Pearson’s correlation coefficients were generated for each analysis, and a significance threshold of P < .05 was used. Descriptive statistics for demographic characteristics and PROMs were reported either as the mean ± standard deviation for continuous variables and as frequency (percentage) for categorical variables. A type I error rate of P < .05 was considered significant. Statistical analyses were performed using SPSS version 28 (IBM, Armonk, New York).
Results
A total of 129 patients reached at least 1-year follow-up and were included in the analysis. The mean age was 58.1 ± 13.5 years, the mean body mass index was 26.8 ± 4.6, and 67 (52%) patients were male. Of the total cohort, 24 (19%) underwent ACDF/CDR, 66 (51%) underwent MI-D, and 39 (30%) underwent MI-TLIF. The average grit and self-control scores were 3.98 ± 0.54 and 3.97 ± 0.54, respectively. The demographic information of the total cohort is listed in Table 1.
Demographics/summary statistics.
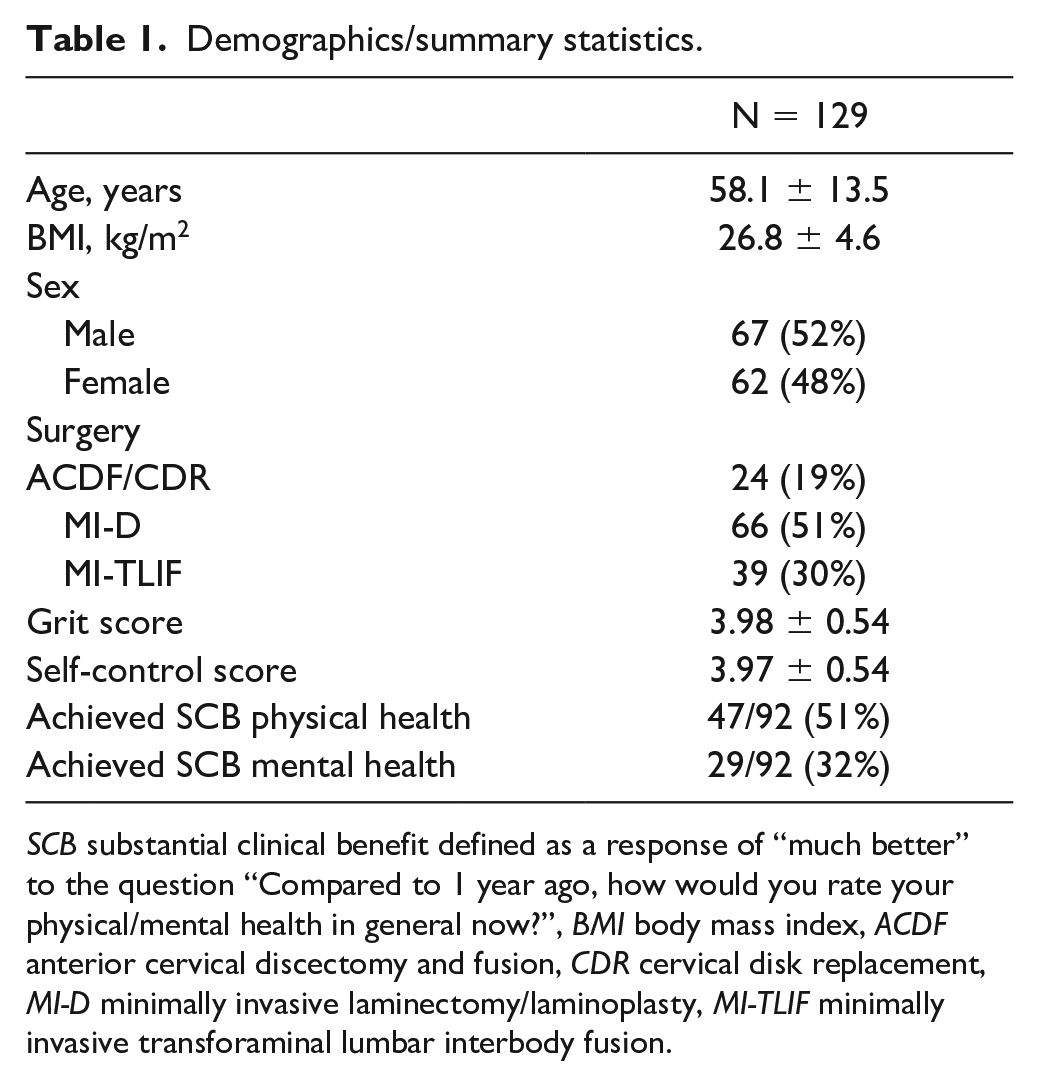
SCB substantial clinical benefit defined as a response of “much better” to the question “Compared to 1 year ago, how would you rate your physical/mental health in general now?”, BMI body mass index, ACDF anterior cervical discectomy and fusion, CDR cervical disk replacement, MI-D minimally invasive laminectomy/laminoplasty, MI-TLIF minimally invasive transforaminal lumbar interbody fusion.
A total of 92 patients (71%) responded to the anchor question, of which 47 (51%) achieved SCB for physical health, and 29 (32%) achieved SCB for mental health (Table 1). There was no statistically significant difference in grit and self-control scores between patients who achieved SCB for physical health and those who did not achieve SCB for physical health. However, patients who achieved SCB for mental health had a mean grit score of 4.14 ± 0.49, which was significantly higher than the mean grit score of 3.90 ± 0.49 for those who did not achieve SCB (P = .035; Table 2).
Association between grit/self-control and physical/mental health.
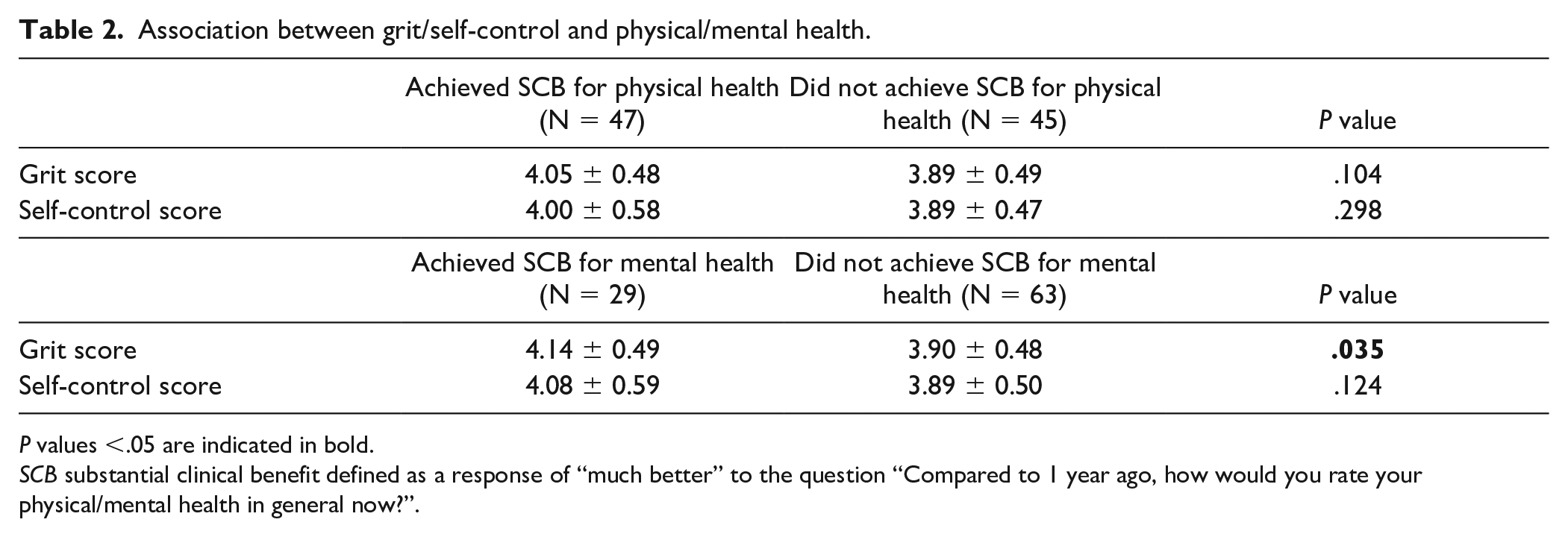
P values <.05 are indicated in bold.
SCB substantial clinical benefit defined as a response of “much better” to the question “Compared to 1 year ago, how would you rate your physical/mental health in general now?”.
Simple correlation analyses were performed for the MI-D and MI-TLIF cohorts, but not for ACDF/CDR due to its smaller cohort size. For the MI-D patients, higher self-control scores were associated with greater improvement in VAS Leg scores at the 1-year (r = −0.28, P = .03) and 2-year (r = −0.40, P = .02) timepoints (Table 3). However, grit and self-control were not associated with PROMs at any of the other timepoints.
Bivariate analysis in MI-D (n = 66).
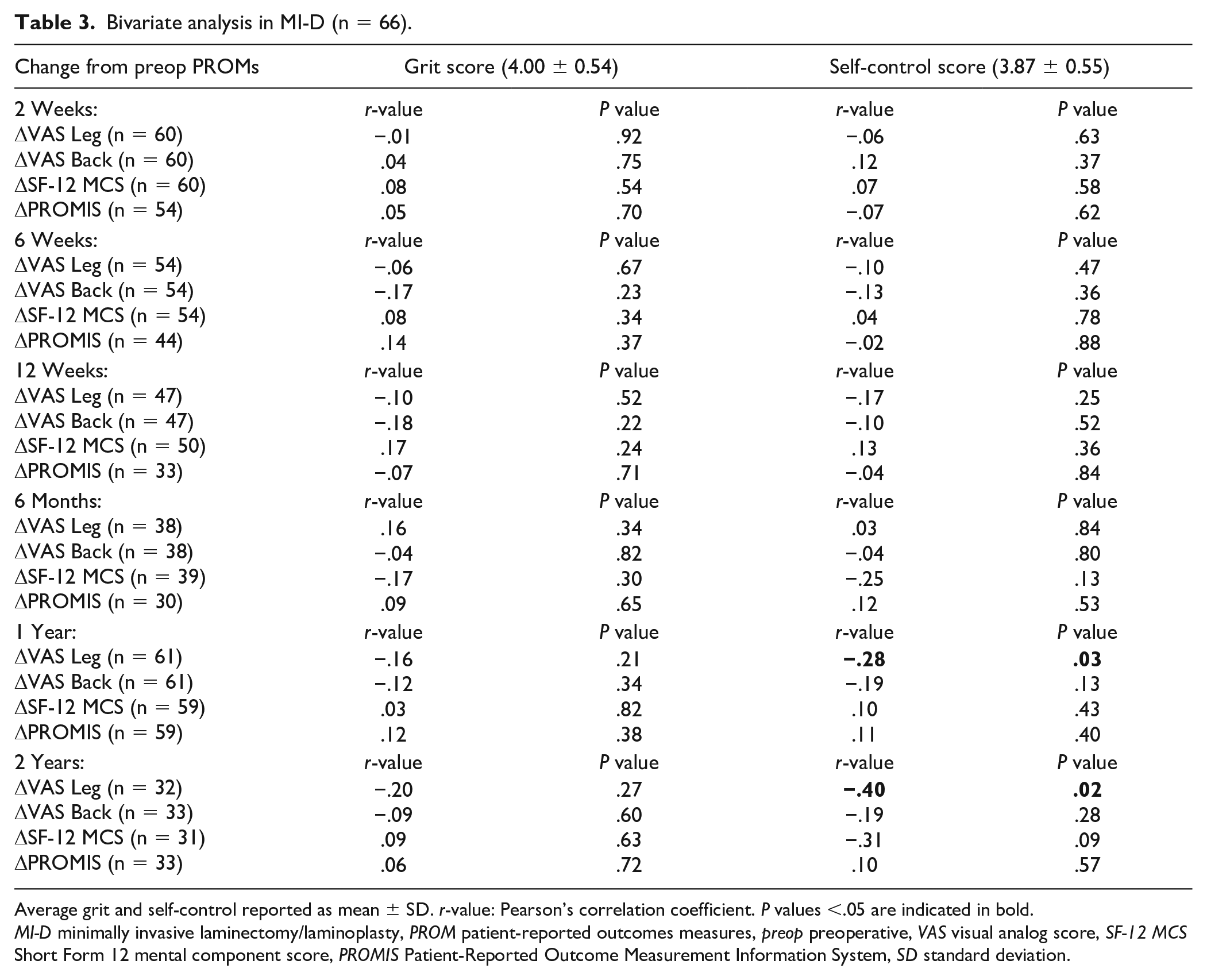
Average grit and self-control reported as mean ± SD. r-value: Pearson’s correlation coefficient.
P values <.05 are indicated in bold.
MI-D minimally invasive laminectomy/laminoplasty, PROM patient-reported outcomes measures, preop preoperative, VAS visual analog score, SF-12 MCS Short Form 12 mental component score, PROMIS Patient-Reported Outcome Measurement Information System, SD standard deviation.
For the MI-TLIF patients, a higher grit score was associated with a smaller change in SF-12 MCS at the 6-week timepoint (r = −0.38, P = .03), and a higher self-control score correlated with a smaller change in PROMIS PF at the 6-month timepoint (r = −0.46, P < .01; Table 4). Grit and self-control were not found to be significantly associated with other PROMs at any of the other timepoints included for the MI-TLIF patients.
Bivariate analysis in MI-TLIF (n = 39).
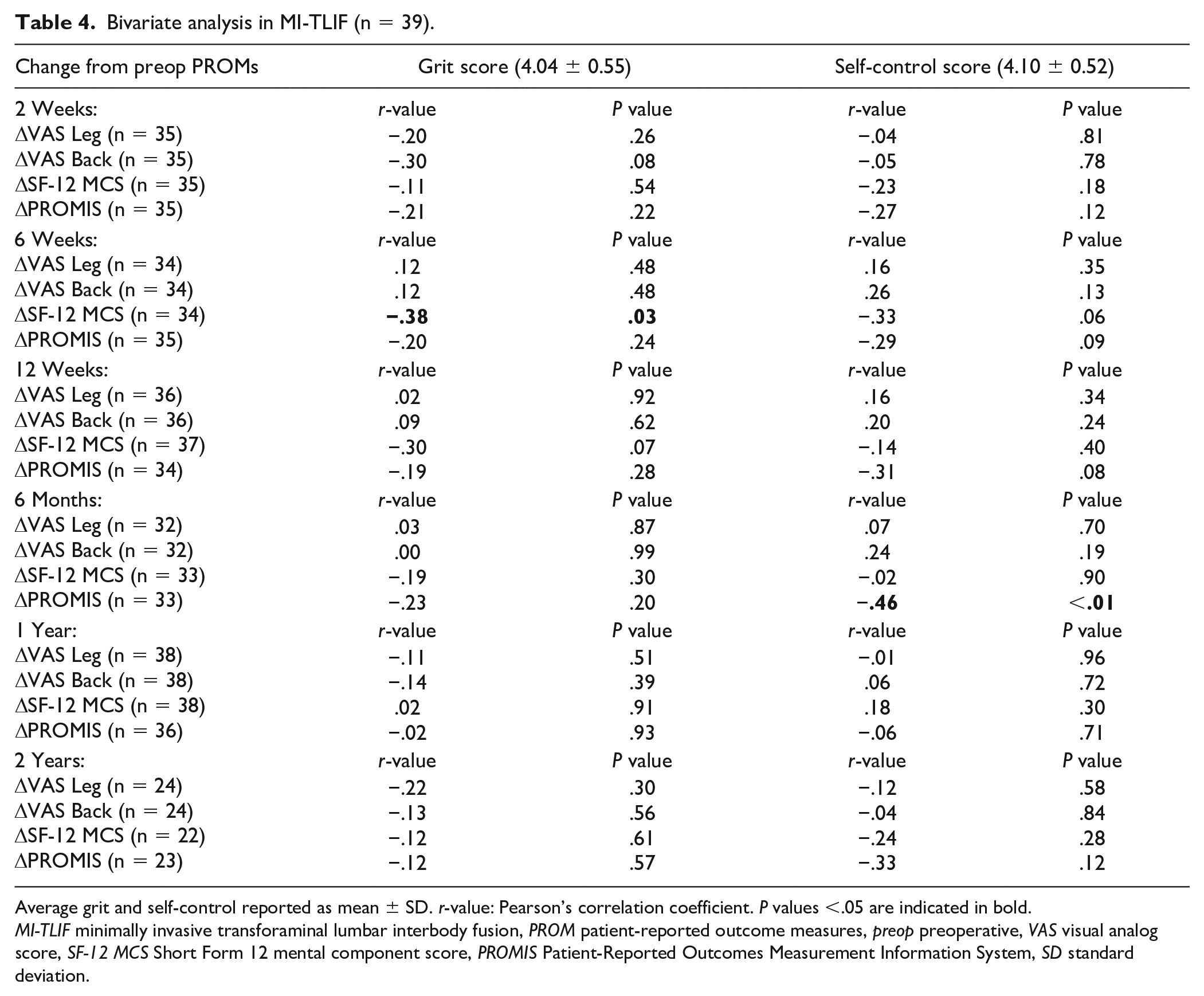
Average grit and self-control reported as mean ± SD. r-value: Pearson’s correlation coefficient.
P values <.05 are indicated in bold.
MI-TLIF minimally invasive transforaminal lumbar interbody fusion, PROM patient-reported outcome measures, preop preoperative, VAS visual analog score, SF-12 MCS Short Form 12 mental component score, PROMIS Patient-Reported Outcomes Measurement Information System, SD standard deviation.
Discussion
Grit and self-control have been shown to be important predictors of achievement, especially in professional domains. Our study assessed a cohort of patients who underwent spine surgery between March 2017 and October 2020. Overall, our findings suggest that grit and self-control scores are not as strongly associated with PROMs following spine surgery as we initially hypothesized. Our analyses identified an association between the grit score and the ability to attain SCB for mental health 1 year after spine surgery. An association between the self-control score and the ability to achieve improvement in leg pain at 1-year and 2-year timepoints was also identified. However, due to multiple testing, the potential of type 1 error must be considered. We hope these findings may help guide physicians when counseling patients and managing treatment expectations.
There were multiple limitations in this study that must be acknowledged. Given the retrospective nature of this study, there is a possibility for selection and recall bias, especially as patients were asked to fill out the grit and self-control questionnaires up to 1 year after their surgery. Another limitation is the low sample size, especially for the ACDF/CDR cohort. The significance of any positive finding is also limited due to the large number of statistical tests run, which may increase the likelihood of type I error.
To our knowledge, this is the first study assessing grit and self-control in patients undergoing spine surgery. Previous studies have looked at the role of grit and self-control for predicting success in orthopedic surgeries for attending physicians, residents, and residency applicants. Samuelsen et al found that residency applicants had higher grit than attending orthopedic surgeons and that attending orthopedic surgeons with more publications had higher grit and self-control scores [12]. Another study by Camp et al found that orthopedic surgery residency applicants who were former college athletes had higher grit and self-control scores and that female applicants also had increased grit [1]. Finally, Kurian et al found that higher self-control was associated with being inducted into the Alpha Omega Alpha honor society and increased publications for orthopedic surgery residents [10]. The results of these previous studies suggest that grit and self-control may be associated with attaining professional success for orthopedic surgeons. However, whether patients experience “success” following spine surgery in relation to grit and self-control has not previously been assessed, and our study sought to answer this question.
Overall, our study found that grit and self-control were not as strongly associated with PROMs as we had expected. For both the MI-D and MI-TLIF cohorts, PROMs were not correlated with grit or self-control scores at several timepoints after a surgery. We expected that patients with more grit and self-control would have more successful recovery and, therefore, a greater improvement in PROMs. However, our findings suggest that a patient’s grit or self-control is not associated with postoperative recovery, as reflected by their PROMs, and that other factors are likely involved.
Interestingly, for the MI-D and MI-TLIF cohorts, higher grit was not associated with greater improvement in SF-12 MCS at the 1-year timepoint; however, grit was associated with the ability to achieve SCB in mental health. This discrepancy may be explained by the way SCB was defined: Patients achieved SCB in mental health if they answered “much better” to the question “Compared to 1 year ago, how would you rate your mental health in general now?” The anchor question requires patients to reflect and assess their own personal improvement, which suggests that grit may be more related to how a patient perceives their current health compared to that in the past, rather than the actual change itself.
Our study also identified an association between self-control and degree of leg pain improvement at 1-year and 2-year timepoints, suggesting that self-control may be related to long-term improvement since correlation was seen only at the later postoperative timepoints. Lastly, a negative association was observed between grit and change in SF-12 MCS at 6 weeks. Patients with more grit had less improvement in their mental health scores, which was not what we had expected to see. One potential explanation is that patients with higher grit have higher MCS scores to begin with and, therefore, have less room for improvement. Upon closer inspection, we found that higher grit was already associated with a higher preoperative baseline SF-12 MCS (r = 0.41, P = .01), which leaves less room for improvement. Similarly, higher self-control was associated with a higher preoperative PROMIS PF score (r = 0.36, P = .03), which may explain why these patients had less improvement in PROMIS PF score at 6 months.
In conclusion, our retrospective study suggests that grit and self-control are not strongly associated with PROMs following spine surgery. There may be some association between the degree of leg pain improvement and self-control. However, these findings are limited by the sample size, multiple testing, and the retrospective nature of the study. Nonetheless, we hope that the results of this study may be helpful to spine surgeons when counseling patients on the postoperative recovery process and managing postoperative expectations.
Supplemental Material
sj-docx-1-hss-10.1177_15563316221147193 – Supplemental material for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery?
Supplemental material, sj-docx-1-hss-10.1177_15563316221147193 for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery? by Marcel Dupont, Kasra Araghi, Daniel Shinn, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-2-hss-10.1177_15563316221147193 – Supplemental material for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery?
Supplemental material, sj-docx-2-hss-10.1177_15563316221147193 for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery? by Marcel Dupont, Kasra Araghi, Daniel Shinn, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-3-hss-10.1177_15563316221147193 – Supplemental material for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery?
Supplemental material, sj-docx-3-hss-10.1177_15563316221147193 for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery? by Marcel Dupont, Kasra Araghi, Daniel Shinn, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-4-hss-10.1177_15563316221147193 – Supplemental material for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery?
Supplemental material, sj-docx-4-hss-10.1177_15563316221147193 for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery? by Marcel Dupont, Kasra Araghi, Daniel Shinn, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-5-hss-10.1177_15563316221147193 – Supplemental material for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery?
Supplemental material, sj-docx-5-hss-10.1177_15563316221147193 for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery? by Marcel Dupont, Kasra Araghi, Daniel Shinn, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-6-hss-10.1177_15563316221147193 – Supplemental material for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery?
Supplemental material, sj-docx-6-hss-10.1177_15563316221147193 for Are Grit and Self-Control Associated With Patient-Reported Outcomes Following Spine Surgery? by Marcel Dupont, Kasra Araghi, Daniel Shinn, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.Q. reports relationships with AMOpportunities, Globus Medical, HS2 LLC, K2M, Lifelink, Minimally Invasive Spine Study Group, Simplify Medical, Spinal Simplicity, SpineGuard, Stryker, Surgalign, Viseon Inc., and Tissue Differentiation Intelligence. S.I. reports relationships with Globus Medical, Healthgrades, HS2 LLC, Innovasis, and Stryker. The other authors declare no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data gathering was supported by the CTSC grant # UL1-TR-002384.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was obtained for all patients included in this study.
Level of Evidence
Level III, retrospective prognostic study
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.