
Abstract
Femoroacetabular impingement (FAI) is considered the mechanical cause of hip osteoarthritis (OA). Surgical intervention involves labrum repair and osteochondroplasty to remove the impingement, alleviating symptoms. Nevertheless, some patients progress to hip OA after surgery, indicating that factors other than mechanical abnormality are contributing to hip OA progression. This review article discusses our laboratory’s studies on hip FAI and OA, undertaken to identify key molecular players in the progression of hip OA. Transcriptome analysis identified peroxisome proliferator activated receptor gamma (PPARγ) as a crucial molecule in early hip OA. PPARγ, widely expressed in chondrocytes, has a protective role in preventing OA, but its true mechanism remains unknown. We observed a dysregulation of DNA methyltransferase (DNMT) in the progression of hip OA, with high expression of DNMT1 and 3A and downregulation of DNMT3B. Moreover, we established that DNMT3A is the main molecule that is binding to PPARγ promoter CpG area, and hypermethylation of this area occurs during disease progression. This suggests that epigenetic changes are a main mechanism that regulates PPARγ expression. Finally, we developed a novel rabbit model of hip FAI and OA and are currently performing studies to validate our small-animal model to human FAI.
Introduction
Osteoarthritis (OA) is a chronic joint disease that causes pain, disability, and limitations on daily activity [18,24]. The hip is the second most common OA location after the knee [3]. Currently, total hip replacement (THR) is the treatment of choice for advanced hip OA. Given that we live longer and have not found a cure for OA, it is predicted that THR procedures in the United States will increase to more than 1.4 million per year by 2040 [35].
Early studies pioneered by Ganz, Harris, Murray, and Solomon suggested that primary hip OA was a rare condition and that hip OA was mostly secondary to an abnormal femoral or acetabular bone deformity [17,28,36]. Ganz et al [13] proposed the mechanical concept of femoroacetabular impingement (FAI) and suggested that there are 2 types. The first is Pincer-type FAI, in which over coverage of the acetabulum causes impingement between the acetabular rim and the head-neck junction of the proximal femur. The second is cam-type FAI, in which the nonspherical extension of the femoral head impinges into the acetabular rim, causing cartilage wear and detachment of the labrum [12,13]. Although these 2 types of FAI often co-exist (mixed FAI), they exhibit different damage patterns due to their differing impingement mechanisms. Pincer-type FAI initially causes labral damage, resulting most commonly in hypotrophic and calcified labrums [6,25,26]. In contrast, cam-type FAI initially causes chondrolabral damage, resulting in delamination of the cartilage from the labrum [6]. Progression to OA is most often seen in cam-type FAI. Moderate and severe cam deformities are reported to be 3.7 to 10 times more likely to develop hip OA over 5-year time span when compared to controls, respectively [2]. Therefore, primary hip OA is rarely observed in young adults.
Our group previously reported on 802 patients undergoing hip arthroscopy for symptomatic FAI and showed a significant association between acetabular cartilage wear patterns and FAI hip deformity [30]. We assessed the frequency of presence of cartilage wear and its severity using the Beck classification. In a separate study, significantly more frequent and severe debonding of acetabular cartilage was observed in patients with symptomatic cam type FAI and mixed type compared with Pincer-type FAI hip (Figure 1) [5]. Cam-type and mixed FAI hips showed significantly more frequent and severe superolateral peripheral cartilage lesions when compared with Pincer-type FAI hips (Figure 1).
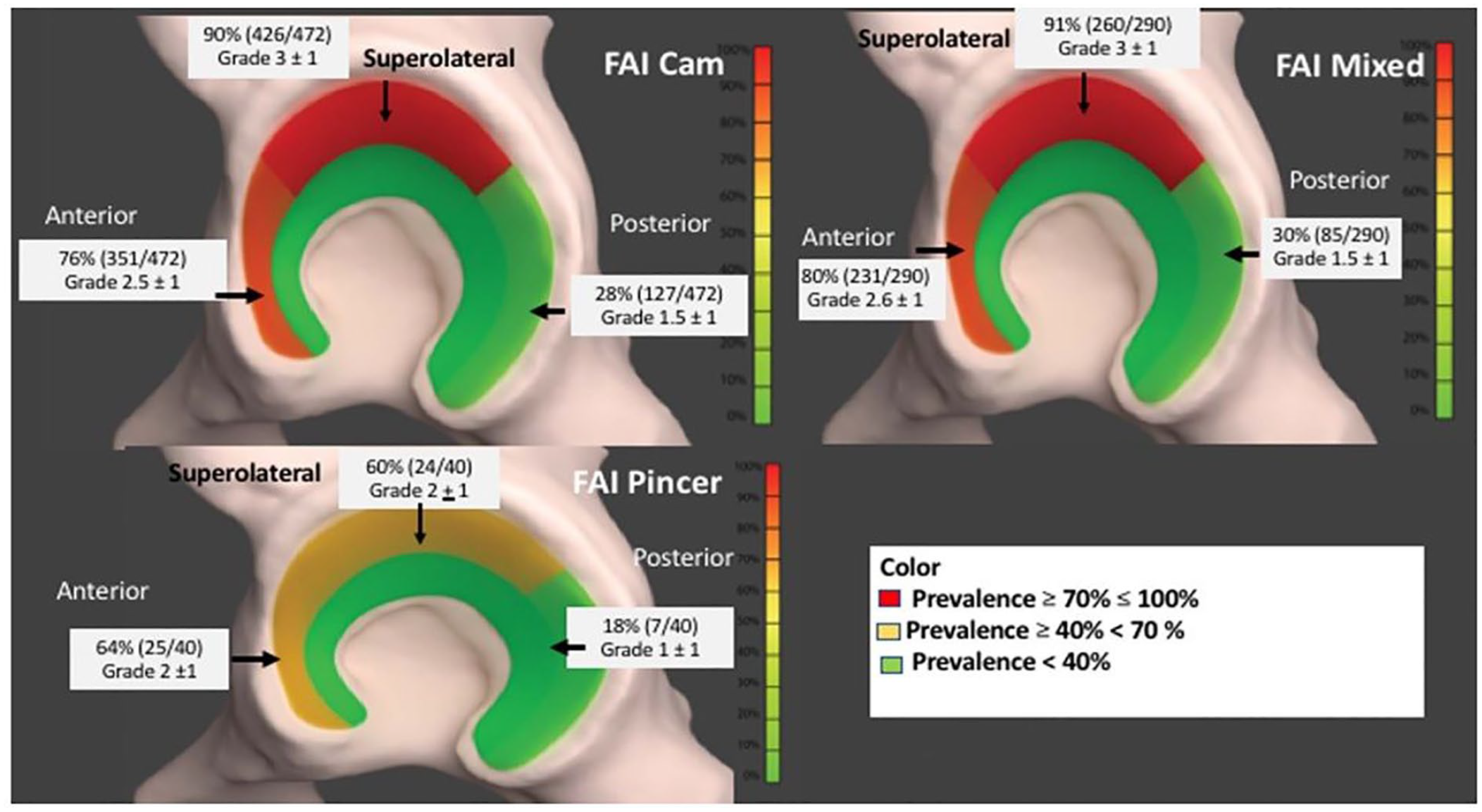
A heat map demonstrates the prevalence of cartilage damage. Percent represents frequency of presence of the cartilage wear. The severity of the cartilage wear was assessed using Beck classification and the average grades observed in each location for each pathology were shown in the figure. Red: 70% to 100%, yellow: ≥40 < 70, and green: <40. Acetabular articular cartilage damage topographies across FAI diagnoses. Graphic design courtesy of Udayabhanu Jammalamadaka PhD. Reprinted from Pascual-Garrido et al. [30].
Surgical interventions for treating FAI are focused on labrum repair and osteochondroplasty to remove the impingement and alleviate symptoms. Femoroacetabular impingement surgery is reported to provide lasting improvements in function and a joint preservation rate of 90.4% at 10 years [14]. Nevertheless, some patients progress to hip OA after surgery. It has been reported that 15% of patients will progress to hip OA within 2 years, and 1.7% to 10% will undergo THR secondary to progression to hip OA [4,7,8,21,32]. It therefore seems appropriate to consider factors other than mechanical abnormality of the FAI hip are involved in hip OA progression.
Initial Experiments: In Search of Inflammation
To understand the mechanism of hip OA, our laboratory is working to identify molecular players in hip OA progression. Initially, we investigated cartilage samples at the impingement zone in patients who underwent hip surgery for the treatment of FAI cam (early stage) or hip OA (late stage) [16]. Groups were established based on clinical findings, intraoperative findings, Tönnis classification, alpha angle, and lateral center-edge (LCEA) angle using radiographs as previously reported [10,16,37]. Femoral head fresh allografts from young adult donors were used as control. Histologically, cartilage samples were assessed with the Osteoarthritis Research Society International (OARSI) grading system and Mankin scoring system [27,31]. Immunohistochemical analysis was also performed to assess inflammation and catabolic markers. Cartilage samples from both early- and late-stage disease confirmed an osteoarthritic phenotype, suggesting that cartilage is already severely degenerated at the zone of impingement in early OA, similar to that observed in advanced OA. Moreover, the expression of inflammatory-related molecules such as interleukin 1β (IL-1β) and matrix metalloproteinase 13 (MMP13) and a disintegrin and metalloproteinase with thrombospondin motif 4 (ADAMTS4) were similar in both stages of disease, concluding that the impingement zone is a local area of chronic inflammation and degeneration.
We consequently performed transcriptome analysis on a similar cohort. Although several pathological pathways had been investigated in hip OA using transcriptome analysis, none focused on early hip OA [41]. Therefore, to reveal early molecular mechanisms of hip OA, we compared cartilage samples from patients with FAI and advanced hip OA and found 50 gene transcripts differentially expressed between the early-FAI and late-FAI groups; the heatmap revealed 2 distinct clusters, indicating for the first time that early and late stage of hip OA are different molecular entities [29]. In addition, we performed a protein interaction analysis to identify hub genes in the process of hip OA degeneration. Protein interaction analysis suggested hub genes that could be critical in the progression of hip OA (Figure 2). Among these, PPARγ was assigned as a hub with 7 connections with other differentially expressed genes, suggesting that PPARγ is a key molecular player in OA.
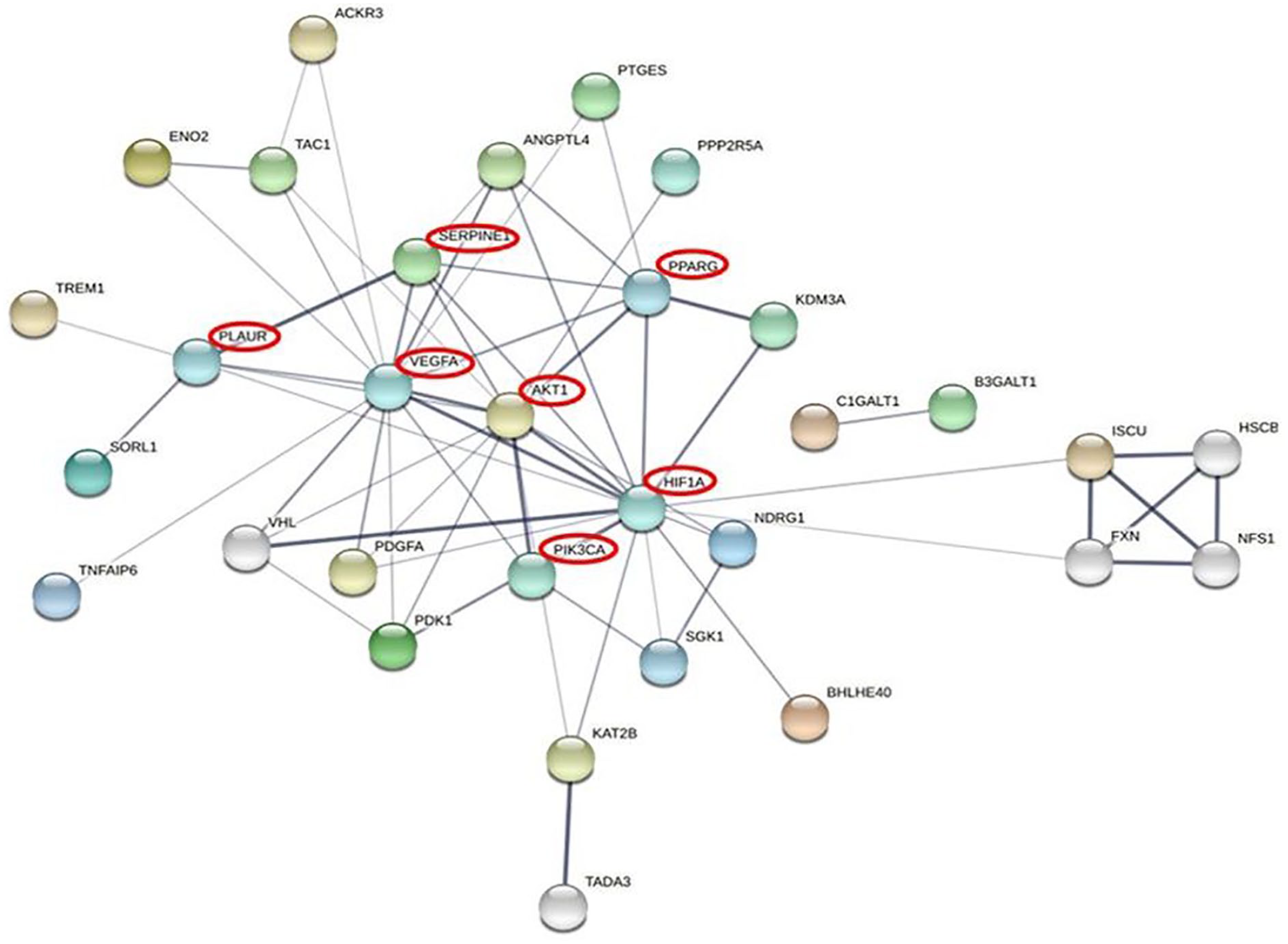
Protein interaction network of genes. Network analysis was performed on all genes, either upregulated or downregulated in the gene expression analysis and pathway analysis in early femoroacetabular impingement. Reprinted from Pascual-Garrido et al. [29]. Copyright 2022, with permission from Elsevier.
Key Molecular Player in Hip OA: The Role of PPARγ
Widely expressed in chondrocytes and essential for cartilage homeostasis [43], PPARγ inhibits several inflammatory and catabolic events in OA pathogenesis, suggesting its role in preventing OA [1]. Indeed, some animal studies revealed that PPARγ receptor agonists have a protective role against OA progression [9,11,23]. Pioglitazone (PPARγ agonist) is reported to attenuate the severity of experimental knee OA induced by partial medial meniscectomy in a large animal model [23]. In addition, up-regulation of PPARγ expression was reported to alleviate experimentally induced knee OA in mice [9], but the true mechanism in which PPARγ protects articular cartilage and why there is loss of expression during hip OA remains unknown. To investigate this, we explored the role of epigenetics on the regulation of PPARγ, specifically if hypermethylation of the PPARγ CpG could result in the suppression of this gene.
Epigenetic Regulation of PPARγ
Epigenetic changes, specifically DNA methylation, play an important role in maintaining genome stability and regulating gene expression [19]. DNA methyltransferase (DNMT) family members, including DNMT1, DNMT3A, DNMT3B, and DNMT3L are enzymes in charge of methylating DNA and regulating gene expression. Dysregulation of DNMTs might result in silenced or overexpression of genes. Previously, Shen et al [34]. have reported that DNMT3B is critical in maintaining cartilage homeostasis and that DNMT3B loss of function (LOF) results in cartilage catabolism [34]. Dysregulation of DNMTs might be triggered by inflammation. Since FAI results in chronic inflammation, we thought to investigate the expression of DNMTs in hip cartilage at the zone of impingement during progression of hip OA. We confirmed that there is a dysregulation of DNMTs in the progression of hip OA, with high expression of DNMT1 and 3A and downregulation of DNMT3B [29]. Moreover, we established that DNMT3A is the main molecule that binds to the PPARγ promoter CpG area. In addition, we confirmed a hypermethylation of PPARγ promoter CpG area as OA progressed, suggesting that epigenetic change is one of the main mechanisms regulating expression of PPARγ. (unpublished data).
Why Is PPARγ Critical in the Progression of Hip OA?
We found that the phosphoinositide 3-kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) pathway is also up-regulated in the early-FAI group [29]. Proliferator activated receptor gamma has been reported to be critical in cartilage homeostasis via mTOR signaling and critical in chondrocyte autophagy [15,22,29,38–40]. Previous analysis has revealed that the PI3K/AKT/mTOR pathway is downregulated in human cartilage tissues with OA, compared to normal cartilage. The PI3K/AKT/mTOR signaling also plays an important role in mediating synovial inflammation. It has been reported that mTOR activation enhances the pro-inflammatory macrophage in OA synovium [42]. Accordingly, we proposed a mechanism by which alteration of the PPARγ and mTOR pathways might induce cartilage autophagy dysregulation and synovitis in hip OA progression (Figure 3). Therefore, we are characterizing the transcriptome profile in synovial tissues in hip OA progression and investigating the effect of PPARγ pathway on synovial macrophage polarization.
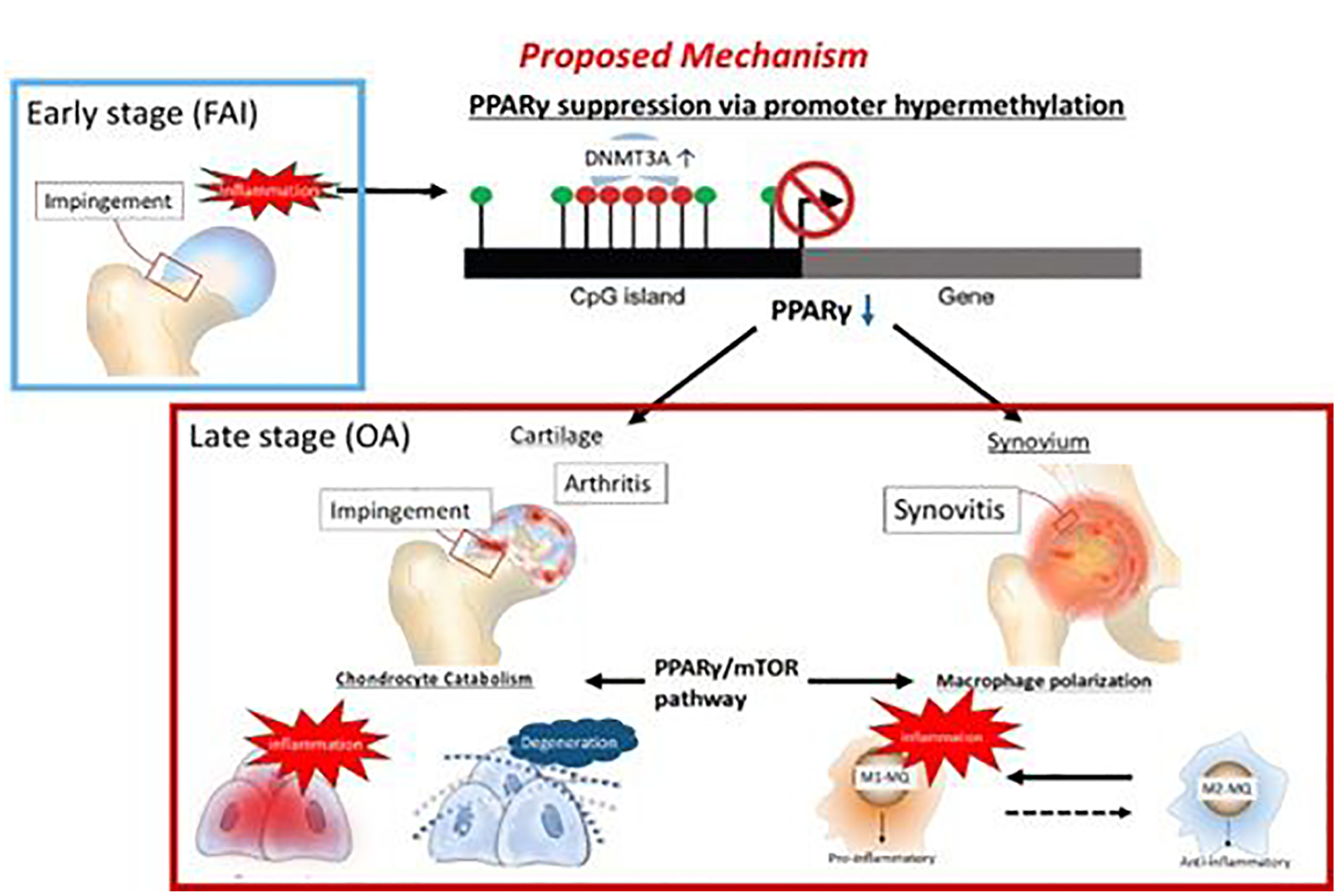
Proposed mechanism of progression of early stage FAI to late-stage OA. Inflammation at the impingement zone of the FAI hip induces the overexpression of DNMT3A and subsequent hypermethylation of the CpG island of the PPARγ promoter, resulting in PPARγ suppression. Suppression of PPARγ causes chondrocyte catabolism and M1 polarization of macrophages in the synovium via PI3K/AKT/mTOR pathway. FAI femoroacetabular impingement; OA osteoarthritis; PPARγ peroxisome proliferator activated receptor gamma; PI3K phosphoinositide 3-kinase; AKT alpha serine/threonine-protein kinase; mTOR mammalian target of rapamycin.
Preclinical Animal Model of Hip FAI and Hip OA
Animal models can serve as pre-clinical platforms to study the mechanism of disease and the efficacy of potential interventions. To date, there has only been 1 published study of large animal hip impingement [33], an FAI sheep model that was induced via extraarticular proximal varus osteotomy. This model has limitations, including that it is costly and there is limited availability of large animals compared with small animals and that it does not reproduce the natural cause of hip FAI. To overcome this limitation, we developed an induced proximal femoral deformity by creating a physeal injury to the medial third of the proximal femoral epiphysis of immature hips of New Zealand white rabbits (Figure 4) [20]. This model led to growth arrest at the proximal femoral physis, resulting in head-neck deformity at the anterosuperior part, as in human cam FAI deformity (Figure 5). Moreover, 3 months following the injury, the joint progressed with intraarticular cartilage damage and OA, as seen in humans (unpublished data), suggesting that this could be the first small-animal model of hip FAI and OA. To validate our model to human FAI, we are performing finite element analysis (FEA) of the hip joint. Our goal is to examine the effects of experiment-induced femoral head deformity on hip joint mechanical loading and to develop a computational–experimental framework to perform mechanical characterization of the superficial zone of articular cartilage at the zone of impingement.
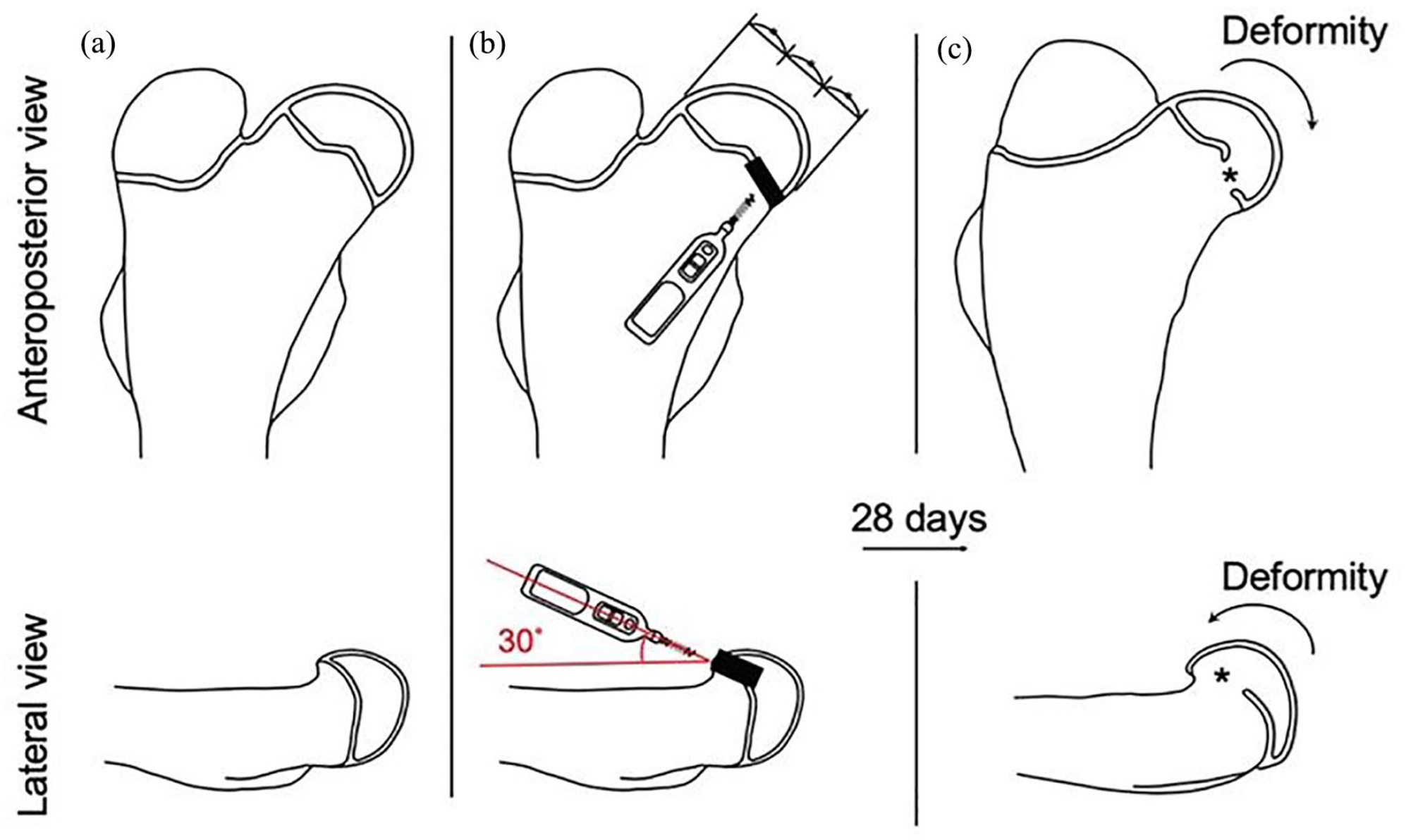
Injury model. (a) The right hip before an epiphyseal injury. (b) An epiphyseal injury is created using a 1.6-mm drill bit through the anteromedial aspect of the medial third of the femoral head at an angle of 30° with respect to the femoral diaphysis. (c) Damage to the femoral epiphysis results in a deformity of the femoral head at 4 weeks after surgery. Reprinted courtesy of Kamenaga et al. [20].
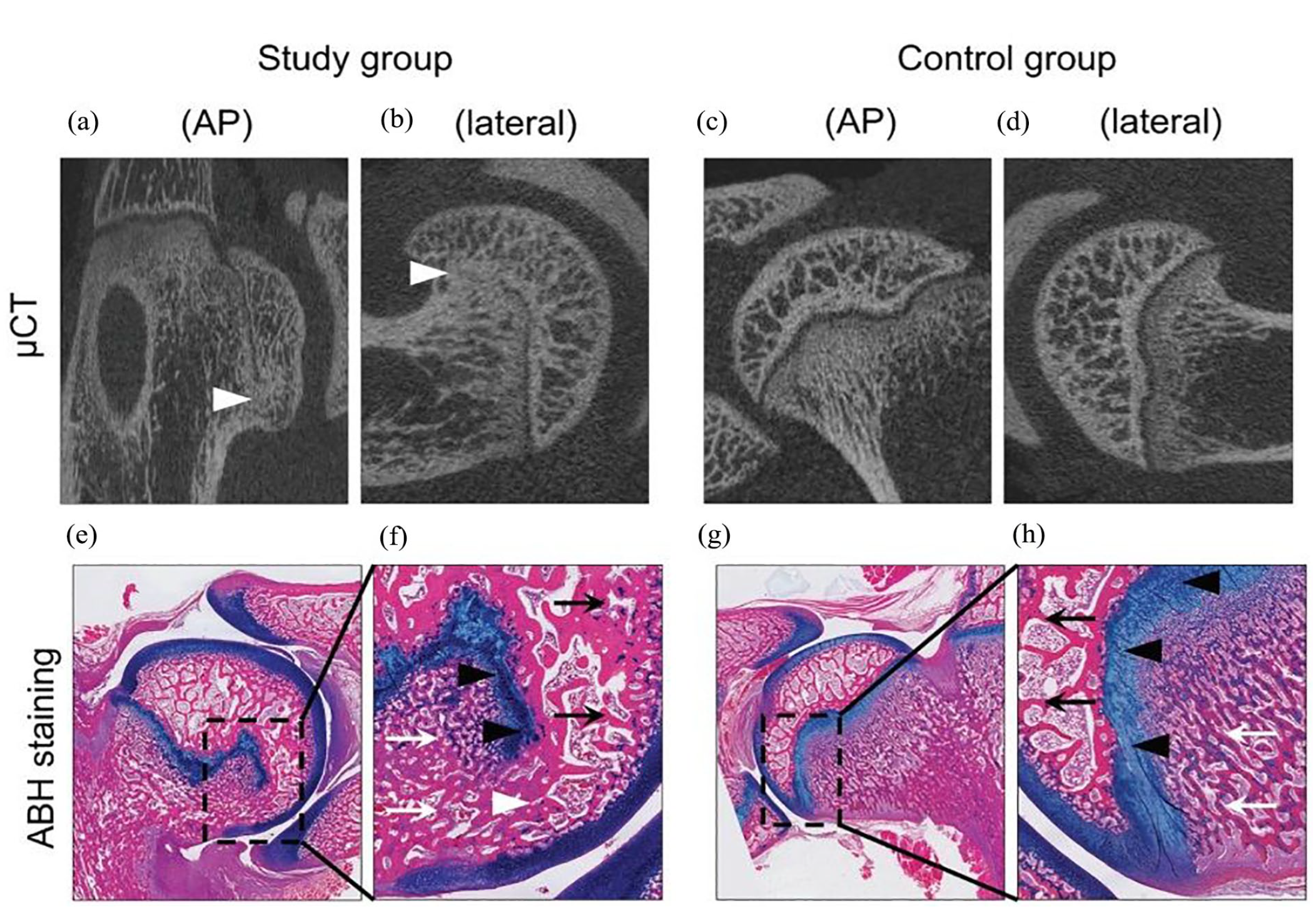
(a-d) Micro-computed tomography images and (e-h) ABH staining of the femoral head in the (a, b, e, f) study group and (c, d, g, h) control group. A bone bridge (white arrowhead) extending from the epiphyseal bone (black arrow) through the physeal line (black arrowhead) and into the metaphyseal bone (white arrow) is seen. AP anteroposterior; ABH Alcian blue hematoxylin. Reprinted courtesy of Kamenaga et al. [20].
Conclusion
Hip FAI plays a critical role in the cause of hip OA. Today, we know that primary arthritis of the hip is a rare condition, with most of the cases being secondary to abnormal mechanics including FAI, dysplasia, and sequelae of childhood hip disease. Although FAI has been morphologically and clinically well characterized, there is still a scientific gap in the understanding of the mechanism of this disease. We believe that surgeries have outpaced the true understanding of the disease, and as a result some patients progress to OA after surgery. Today, the best method for identification of FAI patients at risk of progressing to hip OA with or without surgery is unknown. Our research is focused on identifying key molecular players and pathways that could be used to diagnose cartilage disease, identify patients at risk and responders to therapies, and alter the natural history of disease or slow its progression. We believe critical epigenetic changes occur in pre-OA, secondary to the chronic inflammation that results from chronic impingement. Although several pathways result in loss of joint homeostasis, we have focused on the PPARγ and its potential effect on macrophage polarization and dysregulation of cartilage autophagy. The development of a preclinical animal model of FAI and hip OA is critical and an excellent tool to translate our findings. Understanding the mechanism of disease may result in a breakthrough in the diagnosis, treatment, and prevention of hip OA.
Supplemental Material
sj-pdf-1-hss-10.1177_15563316231190084 – Supplemental material for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement
Supplemental material, sj-pdf-1-hss-10.1177_15563316231190084 for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement by Cecilia Pascual-Garrido, Kenichi Kikuchi, John C. Clohisy, Regis J. O’Keefe and Tomoyuki Kamenaga in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-pdf-2-hss-10.1177_15563316231190084 – Supplemental material for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement
Supplemental material, sj-pdf-2-hss-10.1177_15563316231190084 for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement by Cecilia Pascual-Garrido, Kenichi Kikuchi, John C. Clohisy, Regis J. O’Keefe and Tomoyuki Kamenaga in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-pdf-3-hss-10.1177_15563316231190084 – Supplemental material for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement
Supplemental material, sj-pdf-3-hss-10.1177_15563316231190084 for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement by Cecilia Pascual-Garrido, Kenichi Kikuchi, John C. Clohisy, Regis J. O’Keefe and Tomoyuki Kamenaga in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-pdf-4-hss-10.1177_15563316231190084 – Supplemental material for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement
Supplemental material, sj-pdf-4-hss-10.1177_15563316231190084 for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement by Cecilia Pascual-Garrido, Kenichi Kikuchi, John C. Clohisy, Regis J. O’Keefe and Tomoyuki Kamenaga in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-pdf-5-hss-10.1177_15563316231190084 – Supplemental material for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement
Supplemental material, sj-pdf-5-hss-10.1177_15563316231190084 for Revealing a Natural Model of Pre-Osteoarthritis of the Hip Through Study of Femoroacetabular Impingement by Cecilia Pascual-Garrido, Kenichi Kikuchi, John C. Clohisy, Regis J. O’Keefe and Tomoyuki Kamenaga in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cecilia Pascual-Garrido, MD, PhD, reports relationships with the National Institutes of Health, Orthopedic Research and Education Foundation, ARVIS, Zed View Lexi 3D Developing Software, and the National Football League Musculoskeletal Committee. John C. Clohisy, MD, reports relationships with the Department of Defense–USAMRAA, Zimmer Biomet, Wolters Kluwer Health, Microport Orthopedics, Hip Society, International Society for Hip Arthroscopy, International Hip Society, ANCHOR Fund, and Curing Hip Disease Fund. Regis J. O’Keefe, MD, PhD, reports relationships with the National Institutes of Health, Fate Therapeutics, Loma Linda University, University of Vermont, MiMedx Group, University Health Network of the University of Toronto Advisory Board, and Indiana Center for Musculoskeletal Health, and he holds a patent (DNA methyltransferases for the treatment and prevention of arthritis, #US-10123983-B2). The other authors declare no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH KO8 Clinical Investigator Award, 1K08AR077740-01, NIH R01 award, R01AR069605, 0REF/Goldberg Research Grant in Arthritis and the OREF Mentored Clinician Scientist Grant. Curing Hip Disease Fund and Jackie and Randy Baker Research Funds provided partial support for the research personnel. The Arthritis Foundation and Hospital for Special Surgery funded the 2023 Hip Osteoarthritis Clinical Studies Conference, with support from Stryker, Alexion, and Smith+Nephew.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this review article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.