
Abstract
Background:
Although hip bracing after hip arthroscopy is relatively common, it is not an evidence-based practice; no comparative studies or clinical trials exploring its effectiveness exist.
Purpose:
We sought to summarize the rates of and indications for hip bracing after hip arthroscopy, surgeons’ preferences on braces, and the types of braces used.
Methods:
A systematic review was conducted using the PubMed, Embase, and Medline databases to identify studies that examined hip bracing following hip arthroscopy. Two independent reviewers identified relevant studies with final inclusion determined by the senior author. Full-length, original research articles regarding relevant subject matter that were published prior to January 2022 were included in the analysis.
Results:
Of the 52 articles that underwent full-text review, 14 were included (10 clinical case series, comparative studies, or case-control studies and 4 cross-sectional studies of surgeon-specific postoperative rehabilitation protocols). These studies revealed that the practice of hip bracing after hip arthroscopy is relatively common among orthopedic surgeons, with up to 40% of surgeons using them. Surgical indications for postoperative brace use varied widely. Recommendations on the length of brace use varied, but range of motion restrictions were consistent.
Conclusions:
Although up to 40% of surgeons use post-hip arthroscopy bracing, there is insufficient evidence to determine whether it improves patient outcomes. Research producing higher levels of evidence regarding the efficacy of bracing following hip arthroscopy is necessary to understand the physical, mental, and economic costs and benefits to patients.
Introduction
Hip arthroscopy is a minimally invasive procedure used to treat and diagnose intra-articular hip pathologies. The procedure has increased in popularity since the early 1930s [3], but only in the last several decades has it become particularly mainstream [4,7,9,20,28,32]. In the United States, there was a 350% rise in the number of hip arthroscopies performed between 2004 and 2009 and a 600% rise between 2005 and 2010 [3,32].
Hip arthroscopy is most commonly performed to treat femoracetabular impingement syndrome (FAIS), with osteoplasty to reshape osseous sources of impingement and to repair impingement-associated labral tears [3,4,7,9,28,32]. Additional indications for hip arthroscopy include septic arthritis, osteoarthritis, idiopathic hip pain, loose body removal, and iliopsoas impingement [3,20]. It is theorized that the minimally invasive nature of hip arthroscopy inflicts less trauma on the bony and soft-tissue structures within the hip than open procedures and thus involves less pain, improved outcomes, and expedited recovery [3,4,21].
Postoperative rehabilitation protocols after hip arthroscopy vary widely among surgeons due to a lack of evidence on issues such as weight-bearing status, range of motion, and heterotopic ossification prophylaxis [9,10,21]. The use of hip braces following hip arthroscopy is controversial. Proponents of postoperative hip braces believe that offloading the hip musculature may decrease postoperative pain and may reduce the overuse of hip flexors during ambulation [22,26]. However, a hip brace costs as much as $800 in the United States, which makes its broad use cost prohibitive [13].
We therefore sought to conduct a systematic review to assess the efficacy of hip bracing following hip arthroscopy and to inform recommendations on this common practice. Upon discovering the dearth of high-quality literature assessing this question, this systematic review rather describes the current landscape of postoperative hip bracing in the growing practice of hip arthroscopy. This review synopsizes the rates of bracing, indications, surgeon preferences and justifications, and the types of braces used in the context of hip arthroscopy. A better understanding of these practices will frame modern practice patterns and identify areas for further research on this important topic in the field of arthroscopic hip surgery.
Methods
The systematic review protocol was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations [23]. To minimize selection bias, literature search criteria and processes were established and agreed upon a priori by 3 authors (SM, AGF, MMH).
To identify all studies examining the use of hip bracing following arthroscopic hip procedures, a search was conducted on the following databases: PubMed, Embase, and Medline. These databases were queried on January 29, 2022, using the terms “brace,” “bracing,” “hip,” and “arthroscopy.”
Titles and abstracts were screened by 2 independent reviewers (SM, AGF) to identify relevant studies. Any discordance between reviewers was resolved with the more liberal selection for further review. These studies subsequently underwent full-text review by the 2 independent reviewers, with final inclusion determined by the senior author (MMH). Reference lists of included studies were manually examined for additional eligible studies.
Included studies were those published before January 29, 2022, and involved patients who underwent hip bracing after hip arthroscopy. Only full-length, original research articles written in English were considered. Abstracts, editorials, review papers, technique papers, commentaries, and case reports were excluded, along with studies that did not pertain to the role of bracing in hip arthroscopy.
For included studies, all relevant validated patient-reported pain scores and hip-specific pain scores were recorded. These measures include the modified Harris Hip Score (mHHS), Hip Outcome Score-Activities of Daily Living (HOS-ADL), Hip Outcome Score-Sport-Specific Subscale (HOS-SSS), Non-Arthritic Hip Score (NAHS), and visual analog score (VAS), International Hip Outcome Tool (iHOT-12), and the Vail Hip Score (VHS).
The Methodological Index for Non-Randomized Studies (MINORS) criteria [29] and Agency for Healthcare Research and Quality (AHRQ) checklist [1] were used to appraise the methodological quality of the included comparative studies and cross-sectional studies, respectively. No relevant randomized studies had been published at the time of the literature search, but 1 randomized clinical trial was registered under ClinicalTrials.gov [19]. Quality appraisal of the included studies was rated by 2 independent reviewers (SM, AGF). Minimum scores of 10 (out of 16) and 14 (out of 22) on the MINORS and AHRQ checklists, respectively, were deemed sufficient a priori for inclusion.
Statistical Analysis
Agreement on the quality appraisal scores between the reviewers was calculated using an interclass correlation coefficient (ICC). Descriptive statistics, such as mean, standard deviation (SD), and ranges are presented.
Results
The initial electronic database search identified 134 papers for evaluation (Supplemental Figure 1). Following the removal of duplicate articles (n = 38), 96 articles underwent screening at the abstract and title level, and 52 subsequently underwent full-text review. Fourteen studies fulfilled all inclusion criteria and met critical appraisal standards; of these, 10 were clinical case series, comparative studies, or case-control studies (Table 1) and 4 were cross-sectional studies of surgeon-specific postoperative rehabilitation protocols.
Included study characteristics.
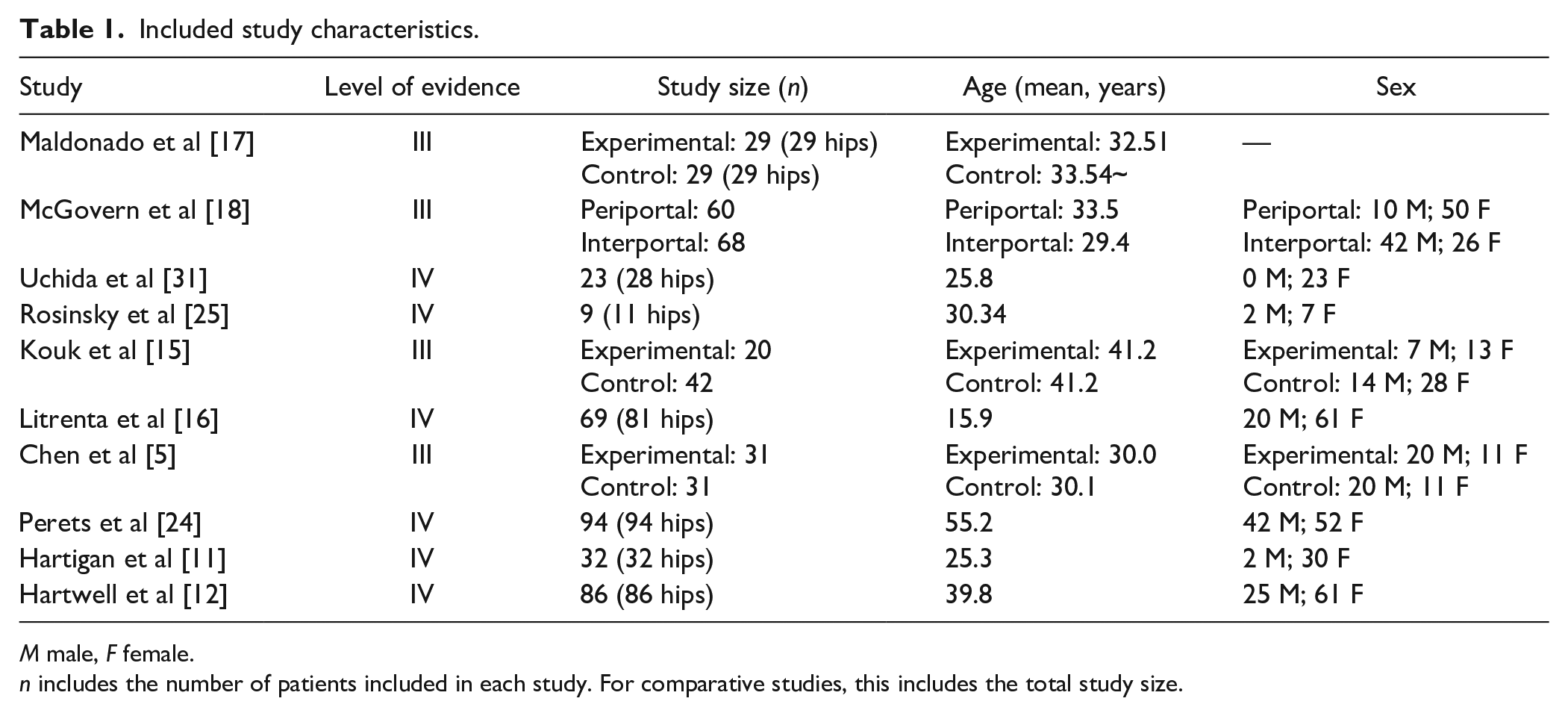
M male, F female.
n includes the number of patients included in each study. For comparative studies, this includes the total study size.
The assessment of study quality revealed good agreement (defined by ICC between 0.75 and 0.90) among quality assessment scores of included studies, with ICC = 0.80 [14]. All 14 of the included studies exceeded the minimum scores required for final inclusion, with an overall mean (±SD) MINORS score of 12.5 ± 1.79 (range, 10 to 16 out of 16) and mean (±SD) AHQR score of 16.9 ± 1.13 (range, 15 to 18 out of 22).
In 4 studies, a DonJoy hip brace was postoperatively prescribed for 2 weeks [11,16,17,24] (Supplemental Table 2). In 2 studies, a hip abduction brace was used; 1 study recommended bracing for 1 week [15], while the other recommended bracing for 6 weeks [25]. In 1 study, a Philippon/Bledsoe hip brace was prescribed for 2 to 3 weeks following hip arthroscopy [31]. In 1 study, a T-Scope Hip brace was prescribed for a minimum of 2 weeks; in patients who underwent microfracture and/or labral reconstruction procedures, an additional 4 weeks of bracing was prescribed at the surgeon’s discretion [18]. In 2 studies, patients wore an unspecified hip brace for 2 to 6 weeks following their arthroscopic procedure [5,12].
Range of motion restrictions within bracing protocols were also evaluated. In 5 of the 10 studies, braces were initially set to limit hip flexion to 90° [5,11,18,24,25]. One study allowed for hip flexion up to 120°, with abduction and external rotation limited to 45° and 0°, respectively [31]. Another study allowed for flexion as tolerated and restricted range of motion to prevent extremes of motion (the scale of “extremes” was undefined) [15]. Range of motion parameters were set to limit hyperflexion and abduction in 1 study [12], while 2 studies omitted their brace range of motion constraints all together [16,17]. Range of motion restrictions using the hip brace were implemented to protect the repair and ensure optimal healing.
The patient outcome measures most frequently reported in the reviewed articles included, but are not limited to, the mHHS, HOS-ADL, HOS-SSS, NAHS, VAS, iHOT-12, and VHS (Supplemental Table 2). In all studies in which hip bracing was employed, there was a trend toward improvement in patient-reported outcomes.
A summary of the results of the 3 survey studies can be found in Table 2. Bolia et al [2] stratified orthopedic surgeons into hip arthroscopy experts and non-experts, with experts having performed over 500 hip arthroscopies over the course of their career and non-experts having performed less than that number. Results from a survey were used to compare the clinical practices between the 2 cohorts [2]. Forty percent of expert hip arthroscopists recommended postoperative hip bracing, whereas only 28% of the non-expert surgeons did [2]. No significant difference existed between the rates of expert and non-expert surgeons who recommended bracing postoperatively. An international survey study of 75 orthopedic surgeons found that the majority of surgeons never (52%) or rarely (17%) used a hip orthosis or hip bracing postoperatively, while the remaining did some of the time (6.1%), most of the time (14%), or always (12%) [30]. Gupta et al [10] surveyed 27 high-volume orthopedic surgeons to assess their practices during hip arthroscopy. This study defined an orthopedic surgeon as high volume if they performed more than 50 hip arthroscopies annually [10]. Results from this survey similarly found that the majority of orthopedic surgeons (41%) never prescribed a hip brace postoperatively, while 22% did so less than 50% of the time [10]. The survey found that 30% of orthopedic surgeons used a hip brace following all procedures and 7% recommended the postoperative use of a hip brace more than half of the time [10]. All surgeons who used a hip brace postoperatively set the brace to limit hip flexion to 90° and to control abduction [10].
Summary of bracing results from surveys on surgeons’ use of hip bracing post hip arthroscopy.
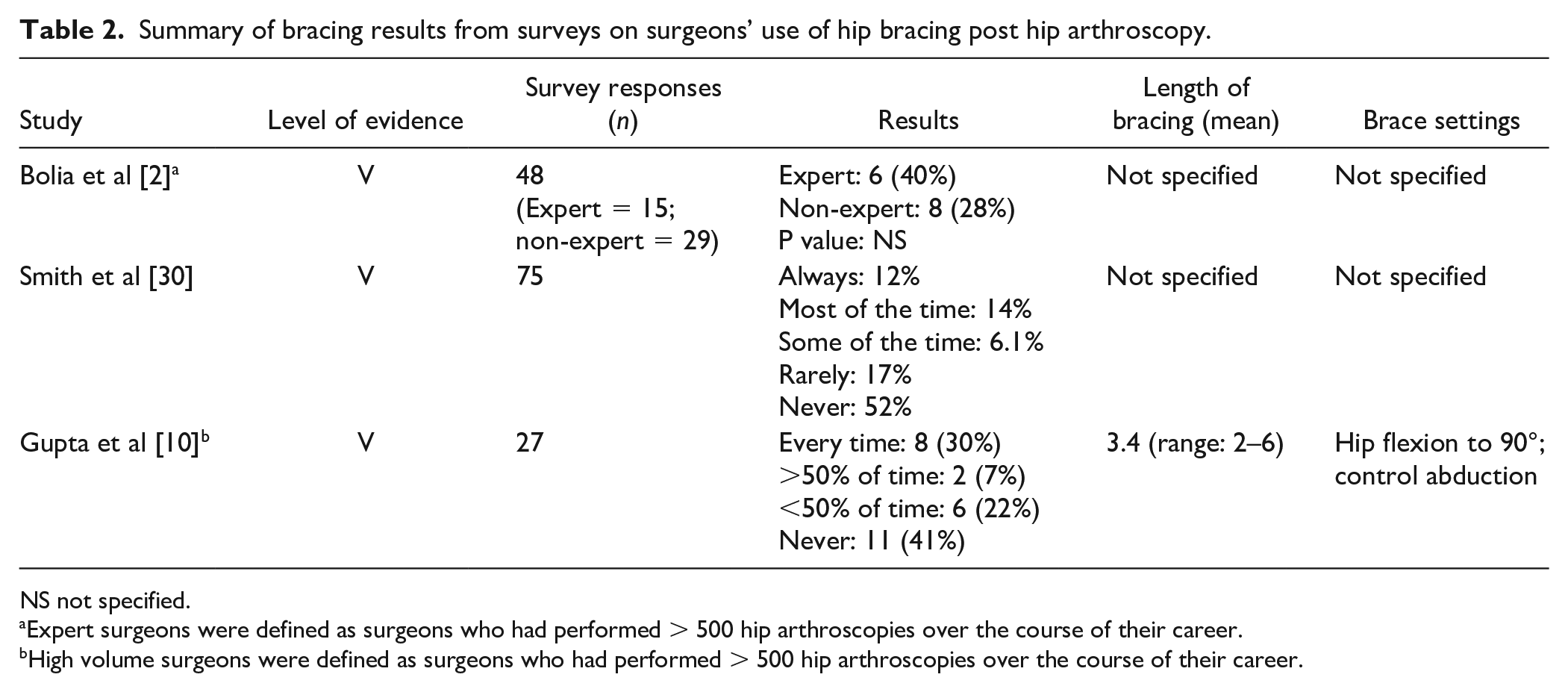
NS not specified.
Expert surgeons were defined as surgeons who had performed > 500 hip arthroscopies over the course of their career.
High volume surgeons were defined as surgeons who had performed > 500 hip arthroscopies over the course of their career.
The remaining article by Cvetanovich et al [6] examined orthopedic surgeons’ departmental or personal websites for their recommended physical therapy protocols following treatment of FAIS and labral repair (Table 2). They found extensive variability in postoperative restrictions and rehabilitation recommendations, including bracing [6]. Their analysis showed that 55% of protocols (17/31) recommended the postoperative use of a hip brace for a median of 2 weeks [6]. They also found that approximately 20% of these online physical therapy protocols endorsed the use of a nighttime hip brace for a median of 2 weeks following arthroscopic surgery for FAI and labral repair [6]. The results of this study again highlight the inconsistent recommendations for bracing following hip arthroscopy.
Discussion
The results of this systematic review show there are no high-level studies to support the efficacy of hip bracing following hip arthroscopy. Therefore, this review summarizes current practice patterns in postoperative hip bracing, including rates of bracing, indications, surgeon preferences, and types of braces used. To our knowledge, this systematic review is the first to summarize the current use of post-arthroscopy hip bracing and to outline the circumstances in which providers use them.
Our review has limitations. For instance, this review is limited by the dearth of literature that exists regarding the efficacy of hip bracing following hip arthroscopy. Furthermore, the original studies included in this study may contain bias; in a systematic review, the presence of bias in multiple included studies may confound and contribute to inaccurate estimations regarding the efficacy of a treatment [27]. However, given the lack of evidence to either support or argue against the effectiveness of hip bracing, the issue of bias in the studies included is unlikely to have strong clinical implications.
Practice patterns surrounding bracing following hip arthroscopy vary considerably by surgeon. This is evidenced by 3 survey studies demonstrating no consensus on post-hip arthroscopy bracing practices among orthopedic surgeons [2,10,30]. In each study, orthopedic surgeons who did not use bracing postoperatively comprised the largest percentage of responses [2,10,30]. However, survey results indicate that a sizable proportion of orthopedic surgeons—ranging from 26% to 40% in Bolia et al’s [2] expert cohort—do in fact recommend the use of a brace following hip arthroscopy all or most of the time [10,30]. Hip braces used included DonJoy [11,16,17,24], Philippon/Bledsoe [31], and T-Scope Hip Brace [18].
Indications for hip arthroscopy in which bracing was included in the postoperative rehabilitation protocol varied. In several studies, surgery and subsequent hip bracing were indicated in patients with symptomatic hip pain who had failed conservative management [5,18,24]. Borderline dysplastic females with painful internal snapping were treated arthroscopically and wore a hip brace postoperatively as well [17]. Arthroscopic hip surgery with postoperative bracing was also indicated in patients with systemic inflammatory diseases who had labral tears, cartilage wear, and/or loose bodies [15]. Additional indications for this treatment regimen included FAIS with and without associated pathologies [12,16]. Finally, patients with symptomatic torn or dysfunctional ligamentum teres [25], symptomatic acetabular dysplasia [31], or iliopsoas snapping and radiographic acetabular dysplasia [11] were all arthroscopically treated and were prescribed postoperative hip braces.
The patient outcome measures were generally positive in the studies in which postoperative hip bracing was prescribed; however, without higher-level investigations, these outcomes cannot be attributed to the bracing specifically. Despite evidence of a causal relationship, these favorable postoperative patient outcomes may still motivate surgeons to continue to prescribe postoperative hip bracing. Further research through observational studies and randomized clinical trials are necessary to determine the utility and subsequent cost-effectiveness of hip bracing.
While the value of bracing following hip arthroscopy has not been formally evaluated, the efficacy of hip bracing as a conservative management for hip pain has been studied. An abstract from Safran et al [26] found that hip bracing in 8 individuals with FAIS led to reductions in motions that exacerbated FAIS-related pain, thus suggesting bracing as a viable non-operative option. Newcomb et al [22] aimed to assess the effects of 4 weeks of hip bracing using a strap brace on individuals with symptomatic FAIS and found that bracing helped to reduce hip movements associated with impingement; they concluded that bracing did not lead to improvements in pain or in patient-reported outcome measures. Notably, a recent exploratory randomized trial explored the impacts of bracing as conservative management in people with FAIS and labral tears [8]. This study found improved hip-related quality of life (iHOT-33), reduced pain levels, and improved symptoms and function in the bracing group; however, the confidence intervals for these measures were large in the setting of a small sample size [8]. The results of these studies are inconsistent and raise questions on the effectiveness of bracing as conservative management for hip pathologies, such as FAIS, that may otherwise be treated arthroscopically.
Further research on the efficacy of bracing following hip arthroscopy is imperative, as this practice may impact patients’ quality of life. In their exploratory randomized trial, Eyles et al [8] measured participants’ satisfaction with hip bracing as conservative management using the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) survey. They found that while patients generally tolerated hip bracing, comfort, and effectiveness were deleteriously impacted by brace use. For instance, patients said that the brace was restrictive, bulky, and/or impacted their ability to perform certain daily activities. Overall, the dissatisfaction with brace comfort and effectiveness led to poor adherence, with more than half participants wearing the brace for only 1 to 2 hours per day [8]. As hip bracing can be cumbersome to the patient, it is necessary to determine whether bracing translates to improved outcomes following hip arthroscopy. Until then, the continued use of hip bracing without evidence supporting its efficacy may be unnecessarily subjecting patients to discomfort and financial burden.
In conclusion, although our systematic review was limited by the paucity of literature available on the topic of hip bracing following hip arthroscopy, it does provide some insight into how and why braces are used. Until further research exploring the efficacy of this practice is conducted, the use of hip bracing following hip arthroscopy may be unnecessary, cumbersome, and cost ineffective.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231190603 – Supplemental material for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review
Supplemental material, sj-docx-1-hss-10.1177_15563316231190603 for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review by Sophia Mavrommatis, Aliya G. Feroe, Ryan R. Fader and Mahad M. Hassan in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231190603 – Supplemental material for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review
Supplemental material, sj-docx-2-hss-10.1177_15563316231190603 for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review by Sophia Mavrommatis, Aliya G. Feroe, Ryan R. Fader and Mahad M. Hassan in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231190603 – Supplemental material for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review
Supplemental material, sj-docx-3-hss-10.1177_15563316231190603 for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review by Sophia Mavrommatis, Aliya G. Feroe, Ryan R. Fader and Mahad M. Hassan in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231190603 – Supplemental material for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review
Supplemental material, sj-docx-4-hss-10.1177_15563316231190603 for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review by Sophia Mavrommatis, Aliya G. Feroe, Ryan R. Fader and Mahad M. Hassan in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231190603 – Supplemental material for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review
Supplemental material, sj-docx-5-hss-10.1177_15563316231190603 for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review by Sophia Mavrommatis, Aliya G. Feroe, Ryan R. Fader and Mahad M. Hassan in HSS Journal®
Supplemental Material
sj-pdf-6-hss-10.1177_15563316231190603 – Supplemental material for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review
Supplemental material, sj-pdf-6-hss-10.1177_15563316231190603 for Postoperative Brace Use After Hip Arthroscopy: A Systematic Review by Sophia Mavrommatis, Aliya G. Feroe, Ryan R. Fader and Mahad M. Hassan in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ryan R. Fader, MD, reports relationships with Stryker and NewClip Technics. The other authors declared no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this review article.
Level of Evidence
Level IV, systematic review of level III and level IV studies.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.