
Abstract
Background:
There is no consensus on whether adductor canal block (ACB) combined with infiltration between the popliteal artery and capsule of the posterior knee (IPACK) block can further increase analgesia and reduce opioid consumption after total knee arthroplasty (TKA) compared with ACB and periarticular infiltration analgesia (PIA).
Purpose:
This study aimed to evaluate the effectiveness of combining ACB and PACK block on analgesia and functional recovery following TKA.
Methods:
A retrospective cohort study was conducted involving 386 patients who underwent primary unilateral TKA at our institution from January 2020 to October 2022. Patients were divided into 3 groups and treated with PIA, ACB, or ACB combined with IPACK block, respectively. Primary outcomes were postoperative morphine consumption and visual analogue scale (VAS) pain scores. Secondary outcomes included functional recovery, evaluated by knee range of motion, quadriceps strength, daily mobilization distance, and postoperative length of stay. Other outcomes included incidence of complications.
Results:
Patients in the ACB + IPACK group had significantly less morphine consumption on postoperative day 1 and during hospitalization than patients in the PIA and ACB groups. Furthermore, the ACB + IPACK group had significantly lower VAS scores at rest and during motion at 6, 12, and 24 hours postoperatively (but not at other time points), better knee range of motion on postoperative days 1 and 2 (but not day 3), and a greater daily mobilization distance on postoperative day 1 (but not days 2 and 3). The ACB + IPACK group had significantly lower incidences of postoperative nausea and vomiting than the PIA and ACB groups.
Conclusion:
This retrospective cohort study suggests that a combination of ACB and IPACK block may have a greater effect than PIA or ACB alone on analgesia following TKA, while providing better functional recovery. Further study is warranted.
Introduction
Total knee arthroplasty (TKA) is considered one of the most effective treatments for relieving knee pain and improving knee function in patients with end-stage degenerative knee disease [23]. While the demand for TKA is expected to increase dramatically in an aging population [9,20], previous investigations have shown that over 60% of patients experience moderate-to-severe postoperative pain after TKA [7,11]. Severe pain often hinders patient participation in early postoperative rehabilitation training and causes negative impacts on eating, sleeping, and mood, which can delay recovery. Poor functional exercise due to postoperative pain can also lead to associated complications such as venous thromboembolism (VTE), myocardial infarction, pneumonia, and arthrofibrosis [27]. Therefore, it’s essential to adopt effective pain management strategies to accelerate patient recovery and improve satisfaction.
Multimodal analgesia, which includes systemic medications, periarticular infiltration analgesia (PIA), peripheral nerve block, and patient-controlled analgesia, has become the standard of care for TKA [11]. Femoral nerve block is one of the commonly used peripheral nerve block methods in the perioperative period of TKA. It usually provides good analgesia, but can also weaken postoperative quadriceps strength and increase the risk of postoperative falls [15]. Adductor canal block (ACB) has been shown to provide similar analgesic effect as femoral nerve block by blocking distal branches of vastus medialis and the saphenous nerve, the sensory branch of the femoral nerve, without affecting the quadriceps strength [14,30,33]. However, the analgesic effect of ACB is still controversial, because it blocks only the anteromedial sensory nerve of the knee joint and not the posterolateral sensory nerve, which may reduce its overall analgesic effect [5,24,28].
During TKA, the release of the posterior joint capsule, cleaning of the popliteal fossa soft tissue, and removal of the popliteal cyst may damage the posterior joint capsule of the knee, leading to severe posterior knee pain. The deficiency in ACB can be addressed by an infiltration between the popliteal artery and capsule of the posterior knee (IPACK) block. Previous studies have shown that IPACK block can provide significant analgesic effect behind the knee while preserving the strength of the lower limb muscles [3,21].
Despite the growing popularity of IPACK block, there is no consensus on whether ACB combined with IPACK block can further increase analgesia and reduce opioid consumption [13,19]. In this retrospective cohort study, we aimed to investigate the analgesic effect of ACB combined with IPACK block after TKA, its influence on functional recovery, and its safety.
Methods
This retrospective cohort study adhered to the principles of the Declaration of Helsinki and was approved by the Clinical Trials and Biomedical Ethics Committee of our hospital. Given the retrospective design of the study, the absence of any potential harm to the participants, and the use of anonymized patient data, the requirement for informed consent was waived. This study was registered in the Chinese Clinical Trial Registry on December 7, 2022 (registration number: ChiCTR2200066505) and reported according to the STROBE statement [29].
Patients who underwent primary unilateral TKA in our department from January 2020 to October 2022 were eligible for recruitment. The inclusion criteria were patients who (1) had body mass index (BMI) of 18 to 30 kg/m2; (2) received only PIA, ACB, or ACB combined with IPACK block; and (3) had American Society of Anesthesiologists (ASA) functional status of I to III. The exclusion criteria were (1) diagnosis of nonosteoarthritis (including rheumatoid arthritis, traumatic arthritis, and septic arthritis); (2) previous knee surgery; (3) knee flexion deformity ≥ 30° or varus-valgus deformity ≥ 30°; (4) history of cognitive impairment, opioid dependence, or psychiatric disease; or (5) allergy to the medications used in this study.
Patients were divided into three groups based on their admission time method and treated with PIA, ACB, or ACB combined with IPACK block, respectively. The only variation among the groups was the method of intraoperative analgesia employed.
Basic demographic data were recorded, including age, BMI, sex, side of surgery, preoperative visual analogue scale (VAS) pain score for daily activities, knee range of motion (ROM), quadriceps strength, and ASA functional status. Patients were administered loxoprofen (60 mg) orally 3 times a day for preemptive analgesia starting on the day of admission.
All patients underwent TKA performed by the same senior surgeon using the medial parapatellar approach under general anesthesia carried out by the anesthesiologist. After pure oxygen inhalation, the following anesthetics were administered intravenously: midazolam, 2.0 mg/kg; propofol, 2.0 mg/kg; sufentanil, 0.3 μg/kg; and cis-atracurium, 0.2 mg/kg. Mechanical ventilation was performed with a laryngeal mask or endotracheal intubation. Sevoflurane was inhaled, and remifentanil was pumped for analgesia during surgery according to the patients’ anesthesia needs. Cemented prostheses (DePuy Synthes) were implanted, and no tourniquets or drainage tubes were utilized. Flurbiprofen (50 mg) was administered 20 minutes before the end of the surgery to prevent postoperative pain, along with tropisetron (5 mg) to prevent postoperative nausea and vomiting. To reduce blood loss, all patients received tranexamic acid 1 g IV 30 minutes prior to skin incision:
PIA: Before prosthesis implantation, 20 mL of the anesthetic cocktail (0.2% ropivacaine and 2.0 μg/mL epinephrine) was injected into the posterior aspect of the capsule. Subsequently, 20 mL of the cocktail was used to infiltrate the medial and lateral collateral ligaments. After implantation, the quadricep and retinacular tissues were infiltrated with 20 mL of the cocktail, while the subcutaneous tissues and fat were infiltrated with another 40 mL of the cocktail.
ACB: A single, experienced anesthesiologist performed the ACB procedure 30 minutes before general anesthesia. Under ultrasound guidance at the mid-thigh level, the structures of the vastus medialis, superficial femoral artery, sartorius muscle, and adductor canal were identified. The anterolateral hyperechoic structures of the artery (included the saphenous nerve and medial femoral nerve) were then infiltrated with 20 mL analgesic cocktail.
IPACK: Using ultrasound guidance, the gap between the popliteal artery and femur was identified at the interface of the medial and lateral femoral condyles, with the needle migrating toward the femoral stem. An in-plane technique with a medial thigh approach was used to inject 20 mL of the analgesic cocktail.
All patients received ice compressions upon their return to the ward, but no patient-controlled analgesia pump was used. Oral loxoprofen (60 mg, 3 times daily) and oxycodone hydrochloride prolonged-release tablets (10 mg, twice daily) were administered to manage postoperative pain. If patients were unable to tolerate the pain (VAS pain score at rest was ≥ 4 or during motion was ≥ 6), 10 mg of subcutaneous morphine hydrochloride was administered. To prevent VTE, enoxaparin (0.2 mL) was administered subcutaneously 12 hours after surgery, followed by 0.4 mL every 24 hours until discharge. After discharge, rivaroxaban 10 mg was taken orally once a day for 2 weeks. Lower extremity strength training was initiated when patients could move their lower limbs. During postoperative hospitalization, patients walked with walking aids.
Primary outcomes were postoperative morphine hydrochloride consumption and VAS pain scores [8] at rest and during motion (45° knee flexion). The VAS scale ranged from 0 to 10, where 0 indicated no pain, 10 indicated the worst pain, and scores above 3 indicated moderate pain. Pain at rest was assessed at 2, 6, 12, 24, 48, and 72 hours after surgery, and pain during motion was assessed at 6, 12, 24, 48, and 72 hours after surgery.
Secondary outcomes included recovery of knee function as assessed by knee ROM, quadriceps strength, daily mobilization distance, and postoperative length of stay. Knee ROM was measured using a protractor 3 times per day, at 6-hour intervals, and the optimal value was recorded for each day. Quadriceps strength was evaluated on a scale of 0 to 5, with 0 representing the worst strength and 5 representing optimal strength, by asking patients to flex their knees and hips. For daily mobilization distance, patients needed to walk as far as possible in a single attempt, and the distance was recorded. In addition, the postoperative length of stay was also documented.
Other outcomes included incidence of complications such as nausea, vomiting, wound complications, VTE, neurovascular injury, postoperative infection, fall after surgery, and 3-month readmission.
Statistical Analysis
All statistical analyses were conducted using SPSS version 25 (IBM Corp, Armonk, NY, USA). Data normality was assessed using the Shapiro-Wilk test. For normally distributed data, 1-way analysis of variance (ANOVA) was performed, followed by post hoc testing using the least significant difference (LSD) test to evaluate differences among groups. Kruskal-Wallis rank sum test and post hoc tests were utilized for skewed and ordinal distribution data. The Bonferroni test was employed to P value correct for multiple comparisons among groups. Categorical data was analyzed using the Pearson χ2 test or Fisher exact probability test. Continuous data was reported as mean ± standard deviation (SD), while categorical data were expressed as numbers or percentages, unless otherwise indicated. Differences were considered significant if P < .05.
Results
The final patient cohort included 386 primary unilateral TKA patients, 158 patients in the PIA group, 121 patients in the ACB group, and 107 patients in the ACB + IPACK group. There were no significant differences in preoperative baseline characteristics or surgery time among the 3 groups (P > .05, Table 1).
Patients’ clinical and demographic characteristics.
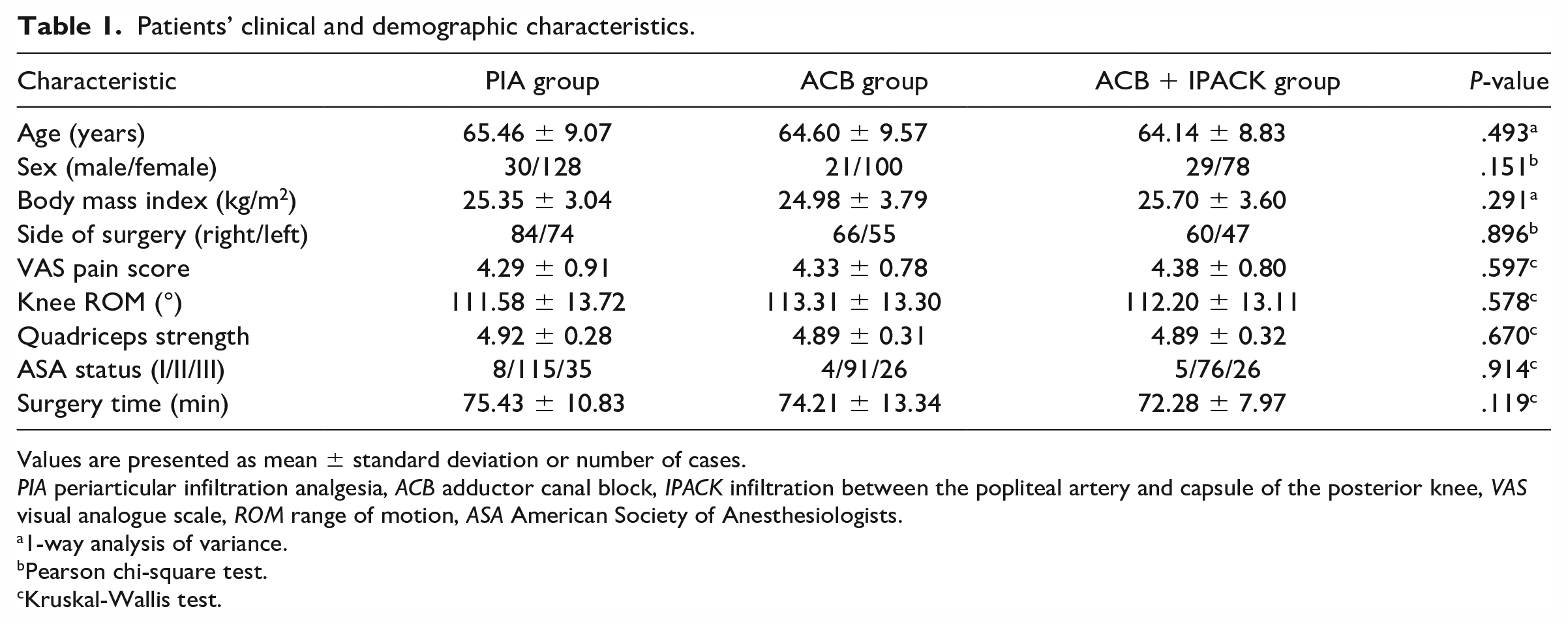
Values are presented as mean ± standard deviation or number of cases.
PIA periarticular infiltration analgesia, ACB adductor canal block, IPACK infiltration between the popliteal artery and capsule of the posterior knee, VAS visual analogue scale, ROM range of motion, ASA American Society of Anesthesiologists.
1-way analysis of variance.
Pearson chi-square test.
Kruskal-Wallis test.
Compared with the PIA and ACB groups, patients in the ACB + IPACK group exhibited statistically significantly lower VAS scores at rest and during motion at 6-, 12-, and 24-hour points postoperatively (Fig. 1). However, there were no significant differences in VAS scores among the 3 groups at other time points (P > .05). Besides, the ACB + IPACK group had less morphine consumption on postoperative day 1 and less total morphine consumption during hospitalization than the PIA and ACB groups (P < .001, Table 2). The differences in morphine consumption among the 3 groups on postoperative days 2 and 3 were not statistically significant (P > .05). There were no statistically significant differences in the postoperative primary outcomes between the PIA and ACB groups (Fig. 1, Table 2).
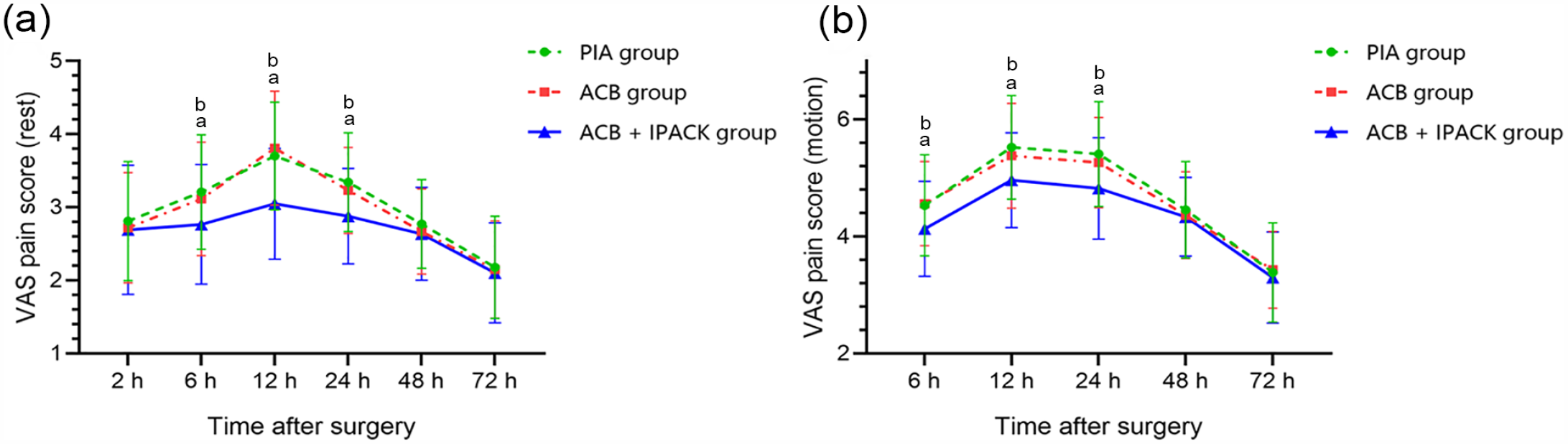
Postoperative VAS pain scores of patients in all groups presented as mean and standard deviation. (a) Pain scores at rest. (b) Pain scores during motion. VAS visual analogue scale, PIA periarticular infiltration analgesia, ACB adductor canal block, IPACK infiltration between the popliteal artery and capsule of the posterior knee. a Significant difference between PIA group and ACB + IPACK group (P < .05). b Significant difference between ACB group and ACB + IPACK group (P < .05).
Primary outcomes.
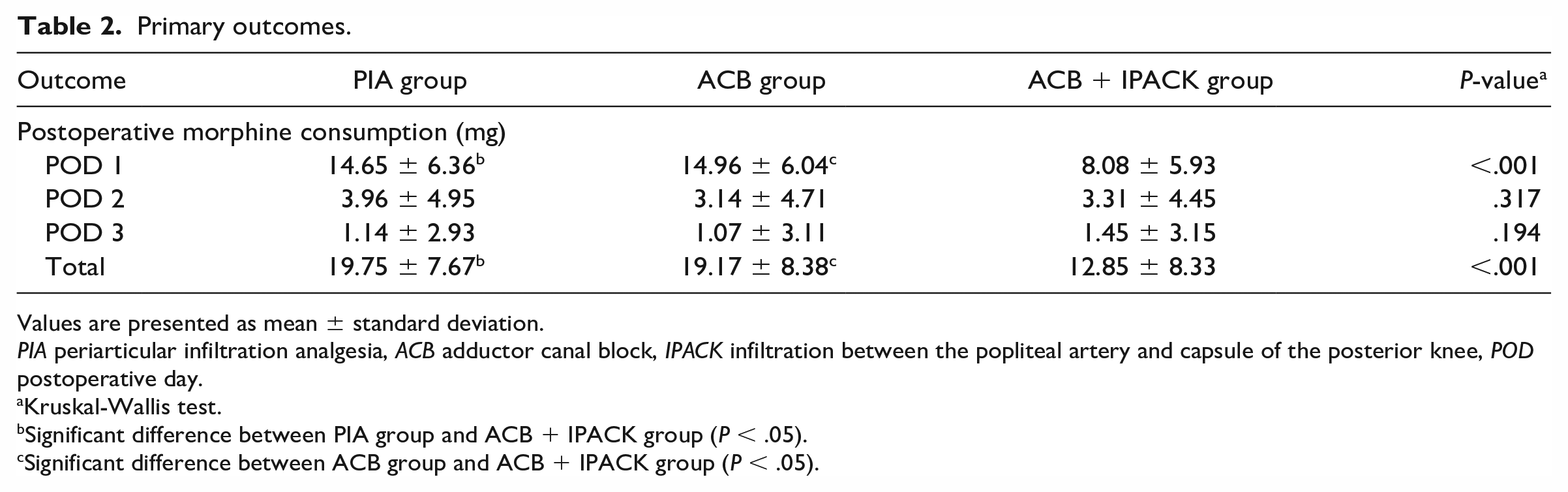
Values are presented as mean ± standard deviation.
PIA periarticular infiltration analgesia, ACB adductor canal block, IPACK infiltration between the popliteal artery and capsule of the posterior knee, POD postoperative day.
Kruskal-Wallis test.
Significant difference between PIA group and ACB + IPACK group (P < .05).
Significant difference between ACB group and ACB + IPACK group (P < .05).
Compared with the PIA and ACB groups, patients in the ACB + IPACK group had better knee ROM on postoperative days 1 and 2, and the differences were statistically significant (P < .001, Table 3). There were no significant differences in knee ROM on postoperative day 3 among the 3 groups (P = .649). Patients in the ACB + IPACK group had further mobilization distance than patients in the PIA and ACB groups on postoperative day 1 (P < .001). Differences in daily mobilization distance among the 3 groups on postoperative days 2 and 3 were not significant (P > .05). There were no significant differences in quadriceps strength among the 3 groups on the first 3 days after surgery (P > .05). Postoperative length of stay was similar among the 3 groups without significant difference (P = .121, Table 3).
Secondary outcomes.
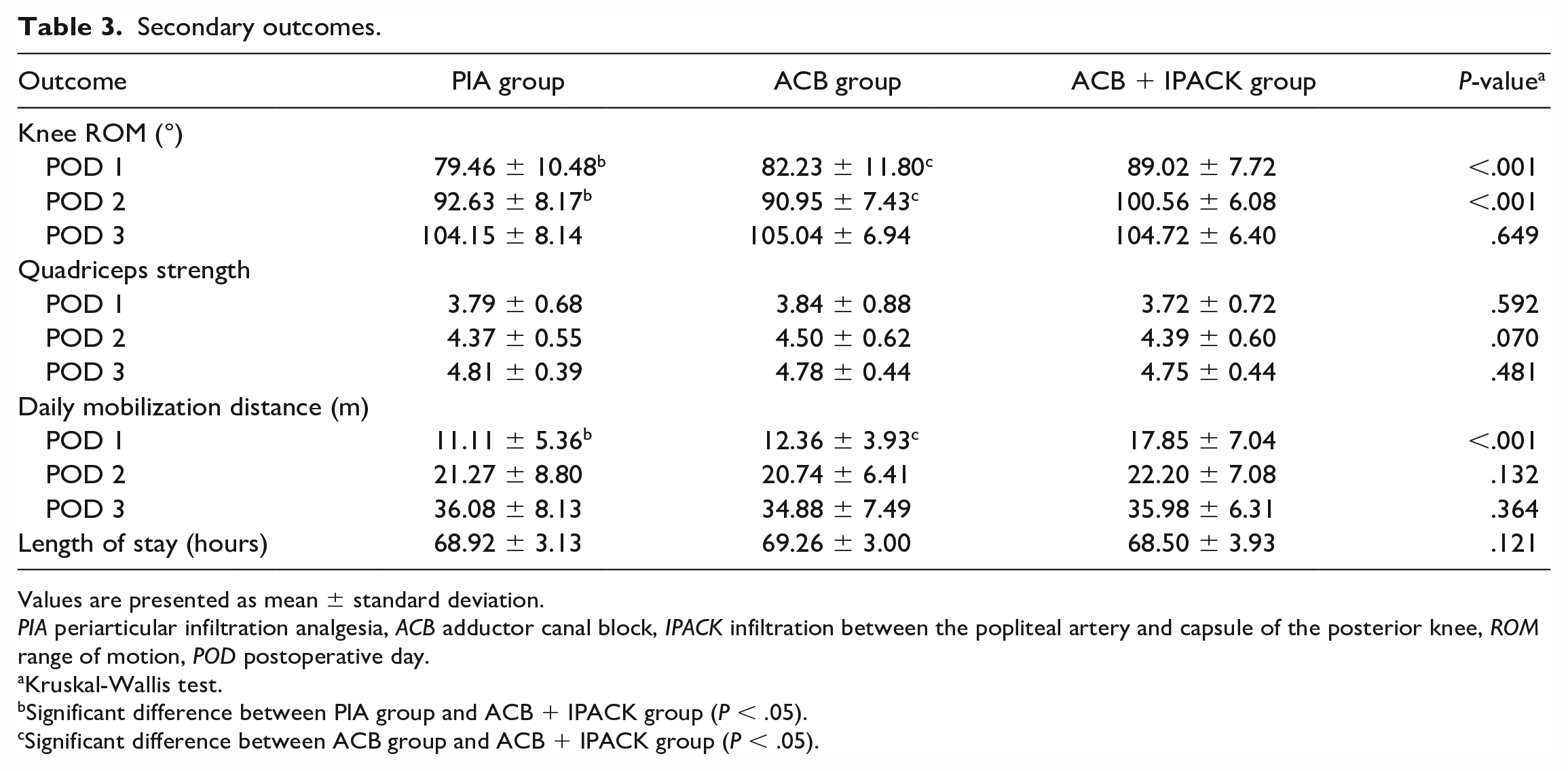
Values are presented as mean ± standard deviation.
PIA periarticular infiltration analgesia, ACB adductor canal block, IPACK infiltration between the popliteal artery and capsule of the posterior knee, ROM range of motion, POD postoperative day.
Kruskal-Wallis test.
Significant difference between PIA group and ACB + IPACK group (P < .05).
Significant difference between ACB group and ACB + IPACK group (P < .05).
The incidences of postoperative nausea and vomiting in the ACB + IPACK group were significantly lower than the PIA and ACB groups (P < .05, Table 4). The incidences of wound complications (P = .760) and VTE (P = .828) were similar among the 3 groups. There was no fall after surgery, neurovascular injury, postoperative infection, or 3-month readmission in the 3 groups (Table 4).
Postoperative complications.
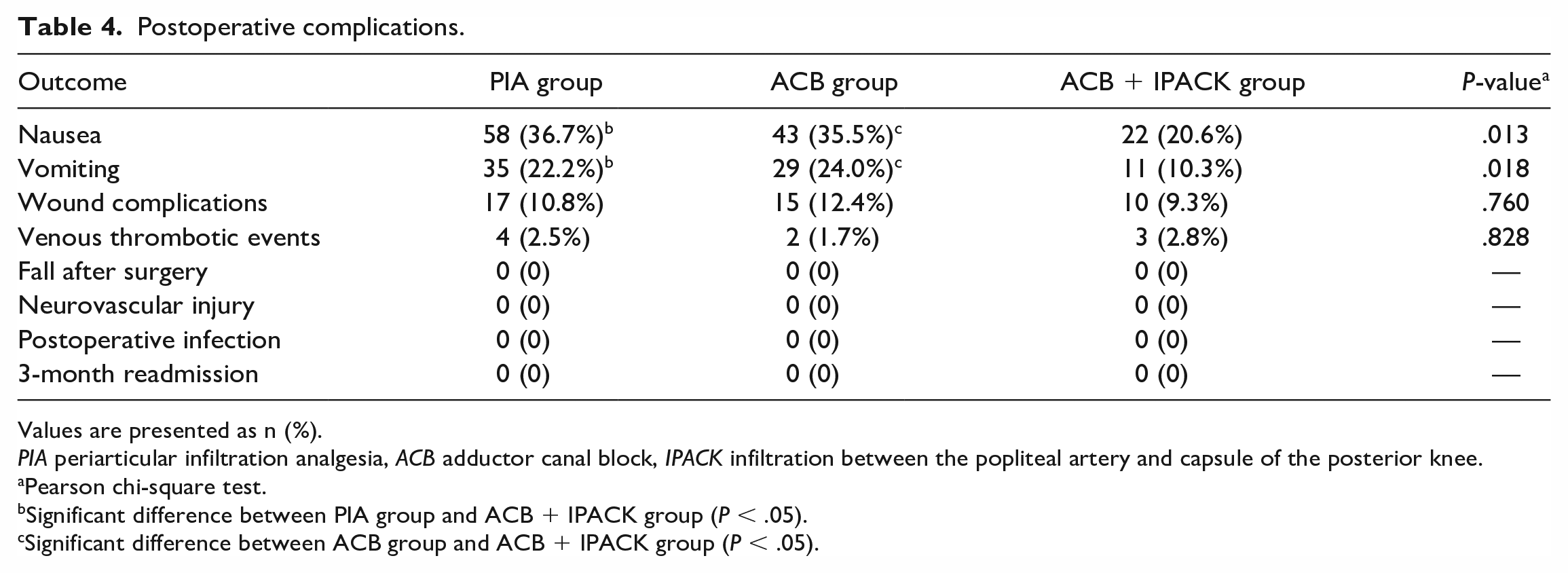
Values are presented as n (%).
PIA periarticular infiltration analgesia, ACB adductor canal block, IPACK infiltration between the popliteal artery and capsule of the posterior knee.
Pearson chi-square test.
Significant difference between PIA group and ACB + IPACK group (P < .05).
Significant difference between ACB group and ACB + IPACK group (P < .05).
Discussion
This retrospective study found associations between combined ACB and IPACK block and better pain relief, reduced opioid use, improved postoperative motor function, and reduced incidence of postoperative nausea and vomiting, when compared with PIA and ACB alone.
Our study presents several limitations. First, it was conducted retrospectively, employing a historical controlled design and stratifying participants based on their admission time, consequently diminishing its rigor and dependability when compared with a randomized controlled trial. A prospective design would have reduced the biases inherent in a retrospective design. Second, only a single injection of ACB was included; further investigations are required to confirm whether continuous ACB would yield the same outcomes. Third, we did not include patients receiving IPACK block alone, and the postoperative efficacy of IPACK block alone could not be determined. Finally, the majority of patients in the study were female, which may limit the generalizability of the findings. The predominance of women in our study is based on the predominance of women in the population of knee osteoarthritis patients that present to our hospital. Nonetheless, our study provides valuable insights into the safety and efficacy of combining ACB with IPACK block for TKA. Future studies should focus on larger, prospective trials with more diverse patient populations to confirm the findings of our study and evaluate the long-term outcomes and cost-effectiveness associated with this analgesic technique.
TKA is a major orthopedic surgical procedure that can cause the exposure of sensory nerve fibers around the patella with insufficient protection of the soft tissues, leading to severe postoperative pain [14,23]. Currently, several multimodal pain management techniques are available following TKA, such as patient-controlled analgesia, epidural analgesia, oral analgesics, PIA, and peripheral nerve block [11,16]. Opioids and epidural analgesia are established analgesic techniques, but they are frequently linked with an increased incidence of adverse effects [10,16]. Oral analgesics are commonly used for perioperative pain management in TKA, but they may not offer adequate pain relief when used alone [34]. Therefore, PIA and peripheral nerve block are increasingly used for perioperative analgesia [11,34]. PIA reduces postoperative pain by preventing central nervous system sensitization through the prophylactic application of analgesics directly at the surgical site. Therefore, a group of patients in this study received PIA as it provides satisfactory postoperative analgesia without reducing postoperative muscle strength or causing opioid-related complications [22,32].
Enhanced recovery after surgery (ERAS), first proposed by Henrik Kehlet in the 1990s, aims to minimize the physiological and psychological stress caused by surgery using specific interventions throughout the treatment pathway [23,25]. As per the ERAS guidelines, crucial goals for joint surgeons were to reduce postoperative pain, reduce opioid consumption, and accelerate functional rehabilitation of patients [16,27]. The results of this study suggest that PIA was not inferior to ACB in terms of providing analgesic effects since there were no significant differences in postoperative clinical outcomes between the 2 groups. One of the primary outcomes of this study was postoperative morphine consumption. The findings suggest that morphine consumption on postoperative day 1 and total morphine consumption during hospitalization were significantly lower in the ACB + IPACK group. Furthermore, the incidence of postoperative opioid-related side effects, such as nausea and vomiting, was significantly reduced in this group.
The combination of ACB and IPACK block appeared to alleviate early postoperative pain, although there was no significant difference in resting pain scores at 2 hours postoperatively. This could be due to the residual effects of general anesthesia during surgery. From the second day after surgery, pain scores were not significantly different among the 3 groups, indicating that the current analgesic cocktail (0.2% ropivacaine and 2.0 μg/mL epinephrine) did not provide prolonged analgesia. Different formulations of the anesthetic cocktail may lead to different analgesic effects [11,22]. Improved analgesia may contribute to early postoperative functional recovery. The study suggests that the combination of ACB and IPACK block allowed patients to achieve better knee ROM and further mobilization distance in the early postoperative period than PIA and ACB. Moreover, the combination was not associated with reduced postoperative muscle strength or delayed recovery, which was consistent with previous findings [1,13–15]. In terms of ERAS, ACB combined with IPACK block had advantages and could accelerate early recovery after TKA.
Recent studies on ACB and IPACK block have suggested that the combination of ACB and IPACK block can lead to reduced opioid consumption [6,26,31], improved early postoperative analgesia [6,18], and enhanced functional recovery [26] (Table 5). Our findings align with these results. Conversely, other studies have demonstrated that the addition of IPACK block does not yield analgesic benefits [4,12] or alter opioid consumption [2,4] or a majority of functional outcomes [2]. This disparity from our findings may be attributed to variances in population selection and the implementation of multimodal analgesia protocols. Further research is necessary to elucidate this topic. In this study, there were no complications associated with ACB and IPACK block, such as nerve paralysis or damage and vascular injury [17]. Furthermore, ACB combined with IPACK block reduced opioid-related side effects, such as nausea and vomiting. However, the cost-effectiveness of ACB combined with IPACK block may be a concern since it requires ultrasound-guided anesthesia in addition to general anesthesia, which may increase the economic costs and risks associated with anesthesia. Although this study preliminarily suggested that ACB combined with IPACK block is safe for TKA, further verification is necessary in larger, preferably prospective studies.
Related papers on literature about ACB and IPACK block.
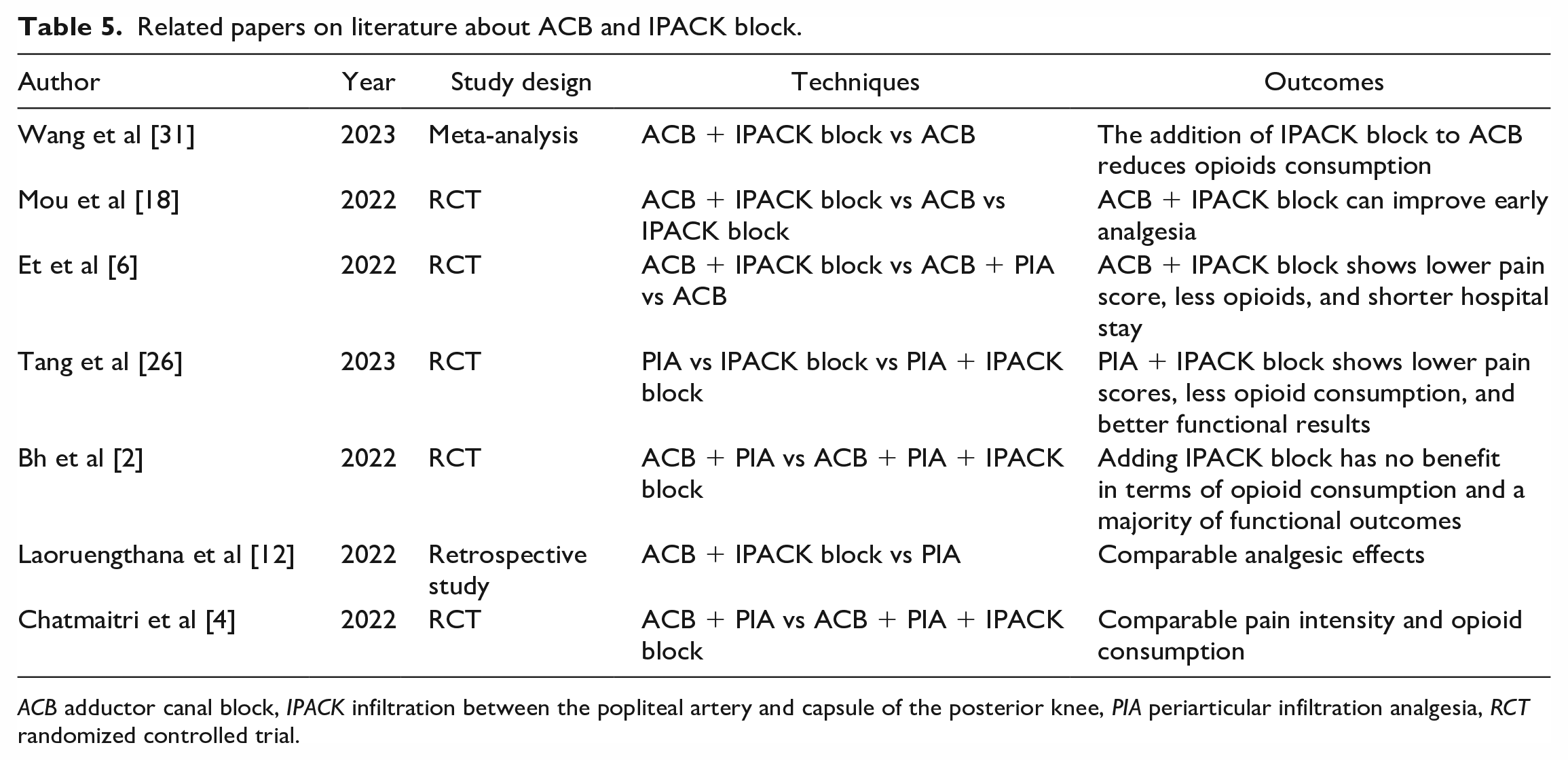
ACB adductor canal block, IPACK infiltration between the popliteal artery and capsule of the posterior knee, PIA periarticular infiltration analgesia, RCT randomized controlled trial.
In conclusion, our retrospective study suggests that compared with PIA and ACB, ACB combined with IPACK block may be more effective as analgesia after TKA, which may alleviate early postoperative pain, decrease opioid consumption, and accelerate functional recovery with lower incidence of opioid side effects. Further study is needed on the optimal multimodal analgesic protocol during the perioperative period for TKA.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231201126 – Supplemental material for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-1-hss-10.1177_15563316231201126 for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study by Chengcheng Zhao, Qiuru Wang, Lijun Cai, Liyile Chen and Pengde Kang in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231201126 – Supplemental material for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-2-hss-10.1177_15563316231201126 for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study by Chengcheng Zhao, Qiuru Wang, Lijun Cai, Liyile Chen and Pengde Kang in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231201126 – Supplemental material for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-3-hss-10.1177_15563316231201126 for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study by Chengcheng Zhao, Qiuru Wang, Lijun Cai, Liyile Chen and Pengde Kang in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231201126 – Supplemental material for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-4-hss-10.1177_15563316231201126 for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study by Chengcheng Zhao, Qiuru Wang, Lijun Cai, Liyile Chen and Pengde Kang in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231201126 – Supplemental material for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-5-hss-10.1177_15563316231201126 for Adductor Canal Block Combined With IPACK Block for Postoperative Analgesia After Total Knee Arthroplasty: A Retrospective Cohort Study by Chengcheng Zhao, Qiuru Wang, Lijun Cai, Liyile Chen and Pengde Kang in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University, grant no. ZYJC18040.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level III, therapeutic study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.