
Abstract
Background:
The use of telemedicine increased greatly following the onset of the COVID-19 pandemic. It is unclear whether and how sociodemographic factors have affected orthopedics patients’ use of this technology in the pandemic.
Purpose:
The aim of this study was to determine how patient demographic variability in telemedicine use is influenced by the Area Deprivation Index (ADI) and distance to clinical site among patients seeking care for hip and knee arthritis from orthopedic surgeons.
Methods:
Demographic data and visit type were collected from the electronic medical record for patients seen in our academic medical center either before or during the COVID-19 pandemic by orthopedic surgeons who specialize in hip and knee arthroplasty. Univariate and multivariate analyses were performed regarding age, race, insurance status, ADI, and distance to a clinical site.
Results:
In the COVID era, among 4901 visits with 3124 unique patients, those using telemedicine were younger and more likely to be White compared to those who did not use telemedicine. There was no significant difference in telemedicine use based on ADI, distance to a clinical site, or insurance status.
Conclusions:
This retrospective analysis suggests that orthopedic patients who were White and of younger age were more likely to use telemedicine in the first year of the COVID-19 pandemic. There was no statistically significant relationship between distance from a clinical site or ADI and telemedicine use, suggesting that factors other than these are greater contributors to telemedicine utilization in our cohort. Further information is needed to determine how telemedicine may disproportionately limit access to orthopedic care according to these and other patient factors.
Introduction
Disparities in the provision of orthopedic care have been well described [1,2,5,16,19]. Previous studies have shown race or ethnicity, socioeconomic status, and type of insurance coverage to influence these disparities. Minority patients, those living in areas with lower mean incomes, and those with noncommercial insurance are all less likely to receive orthopedic care [4,6,14,15]. Similar factors have affected access to care since the onset of the COVID-19 pandemic [16].
The use of telemedicine significantly increased following the onset of the COVID-19 pandemic, with the primary aim of ensuring safety during visits [3], and telemedicine has been viewed as a potential tool to improve access to care [12]. To evaluate the use of telemedicine during the COVID-19 pandemic and in the future, it is important for researchers to understand how it affects preexisting disparities in orthopedic care.
Telemedicine has the potential to decrease disparities by improving care access through shorter wait times, decreased travel cost, and increased safety. Studies have shown that telemedicine has improved access for those in remote areas [13] and is also more likely to be used in postoperative or follow-up visits [3]. However, limitations in the use of telemedicine include lack of Internet access and technological literacy [12]. Disparities exist in the use of telemedicine according to race, insurance status, sex, patient’s primary language, and age at the time of visit [13,17,20,21].
We therefore sought to (1) evaluate the influence of socioeconomic status, as measured by Area Deprivation Index (ADI), on the demographic variability in telemedicine usage, (2) determine whether living farther from a large metropolitan area is an independent predictor of telemedicine use, and (3) compare the effect of demographic factors on the use of telemedicine within our cohort with the effects reported by previous studies. We focused on patients seeking care from hip and knee arthroplasty surgeons, hypothesizing that patients from socioeconomically disadvantaged communities were less likely to utilize telemedicine.
Methods
Following approval from our institutional review board, we obtained data on all ambulatory orthopedic visits with hip and knee specialists from April 1, 2019 to December 31, 2019 and from April 1, 2020 to December 31, 2020, from electronic health records. Visit information, including date of service, visit type, provider, and Current Procedural Terminology codes, and patient information, including race, address, age, and insurance status, were also collected. Race was self-reported as 1 of 6 categories: White, Black or African American, Asian, American Indian or Alaska Native, Other Pacific Islander, or Other. For statistical analysis, groups other than White and Black or African American were grouped into “other” due to insufficient responses for analysis. Patients who declined to select a race, were of unknown race, or were unable to answer were excluded from analyses of race. Age was grouped into 5 categories (18–25, 26–34, 35–50, 51–65, and older than 65 years) for both univariate and multivariate analysis. The ADI, which is publicly available at Neighborhood Atlas by the University of Wisconsin School of Medicine and Public Health, was used as a measure of socioeconomic deprivation, with higher scores representing increased disadvantage [18]. The ADI ranks neighborhoods at the Census Block Group level according to socioeconomic disadvantage by incorporating income, education, employment, and housing quality. Area Deprivation Index scores are determined based on the patient’s 9-digit zip code. Distance to the hospital was calculated between the geographical center of the patient’s 5-digit zip code and the nearest of 5 institutional ambulatory orthopedic centers. Distance was grouped into 1 of 8 categories (less than 2, 2–4.9, 5–9.9, 10–24.9, 25–49.9, 50–99.9, 100–199.9, and more than 200 miles) for both univariate and multivariate analysis. Visits were categorized according to time cohort (pre-COVID, defined as April 1, 2019–December 31, 2019, or COVID, defined as April 1, 2020–December 31, 2020) and visit type (telemedicine or in person). Telemedicine visit type was defined as any visit type listed as “phone/video” or “Zoom.”
Statistical analysis was conducted using SPSS Version 28. Univariate analysis was completed using Pearson’s χ2 tests. Multivariate logistic regression analysis (with telemedicine use as the dependent variable) was performed only using independent/predictor variables that were statistically significant in the univariate logistic regression analysis. Given the a priori interest in variables such as insurance status and distance, we conducted a sensitivity analysis with an additional regression model that included all variables (Supplemental Table 1). P values less than .05 were considered statistically significant.
Results
During the pre-COVID time period, there were 5423 visits with 3594 different patients (Fig. 1), all of which occurred in person. During the COVID time period, there were 4901 visits with 3124 patients, 3945 (80.5%) visits in person and 956 (19.5%) via telemedicine (Fig. 1). Univariate analyses of all visits in the COVID time period demonstrated that telemedicine was more likely to be used by younger patients (P = .002) and patients of White race (P = .046; Table 1). No significant difference was seen regarding ADI, distance to the clinical site, or insurance status (Table 1).
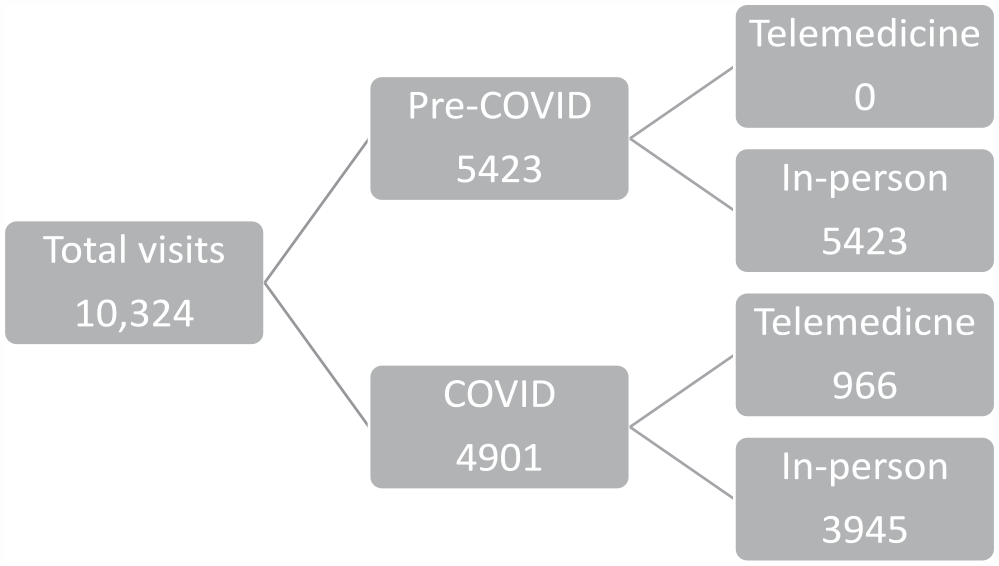
Distribution of included visits by time period and method of visit.
Univariate analysis of all visits during the COVID time period.
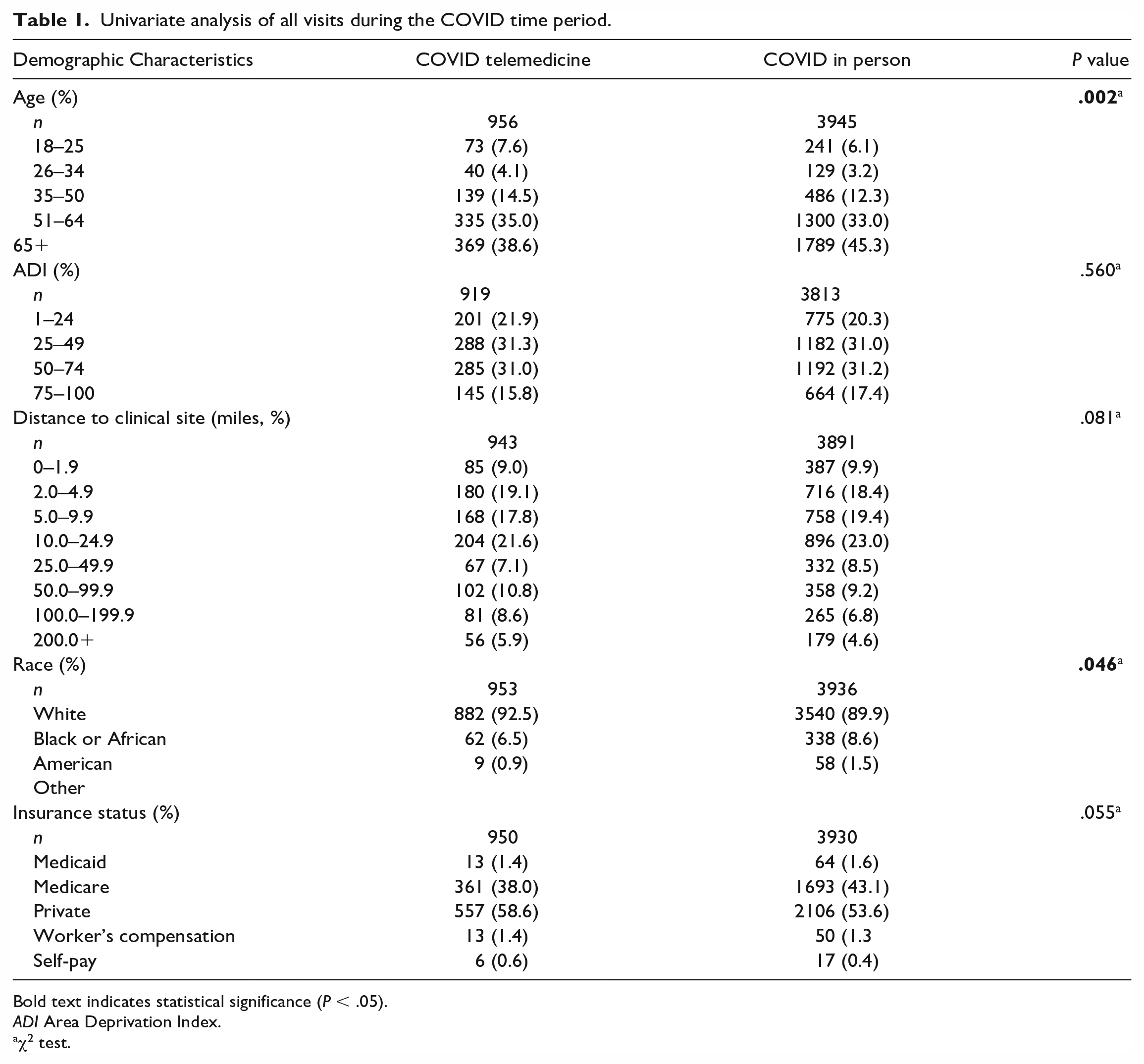
Bold text indicates statistical significance (P < .05).
ADI Area Deprivation Index.
χ2 test.
Multivariate analysis of independently statistically significant variables during COVID visits demonstrated that age (P = .002) and race (P = .040) remained independent predictors of telemedicine usage (Table 2). Patients aged 65 years or older were less likely than younger patients to utilize telemedicine during the COVID-19 pandemic (odds ratio [OR] = 0.686, 95% confidence interval [CI] = 0.516–0.912). Black or African American race (OR = 0.728, 95% CI = 0.549–0.965) was also associated with decreased telemedicine usage (Table 2).
Multivariate analysis of age and race on telemedicine usage during the COVID time period (April 1, 2020–December 31, 2020).
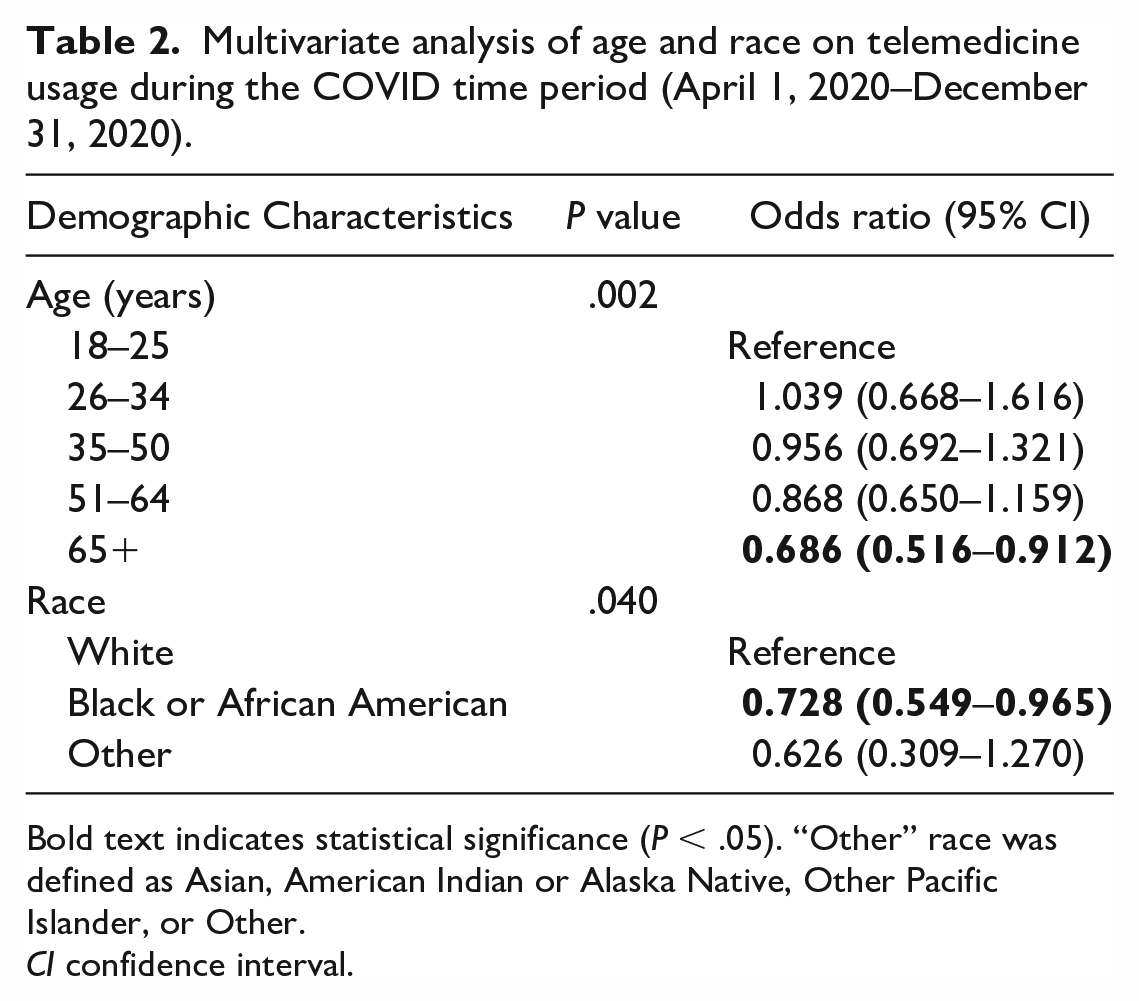
Bold text indicates statistical significance (P < .05). “Other” race was defined as Asian, American Indian or Alaska Native, Other Pacific Islander, or Other.
CI confidence interval.
Discussion
Disparities in access to orthopedic care based on race, socioeconomic status, and insurance have been widely noted prior to the COVID-19 pandemic. There had been concern that the pandemic would exacerbate these disparities. Our analysis suggests that Black or African American patients are less likely to utilize telemedicine than White patients and that older patients are less likely to utilize telemedicine than younger patients (a finding widely supported by previous literature, possibly due to lower use of computers or the Internet among older adults). The 2018 National Health Interview Survey reported that 29.7% of adults aged 61 to 80 years and 66.3% of adults older than 80 years reported “never or almost never” using a computer. Internet use was reported by just 68.7% of adults aged 61 to 80 years and 32.0% of adults older than 80 years. Racial differences in general health care utilization may be a product of lower trust in the health care system or increased reliance on alternative or self-care among Black or African American patients [8,10], but this study and previous studies demonstrate this disparity with specific regard to telemedicine [9,16]. This suggests that while the use of telemedicine may be necessary in some circumstances, its use in the long term may worsen preexisting racial disparities. Similar points are true for older patients. Although older patients are believed to be at higher risk of COVID-19–related morbidity and mortality, we found a decreased use of telemedicine in this population. While this is possibly due to decreased technological literacy or a similar factor, it hints that telemedicine has the potential to limit care for older patients.
There are limitations to our study. We were unable to discern whether patients were fully aware of the option for telemedicine visits, whether they had the perceived capability and/or willingness to conduct telemedicine visits, and whether the health care providers encouraged use of telemedicine during the pandemic. The ongoing pandemic may have also skewed which patients felt the need to be seen at all. Additional limitations arise from our collection of patient information through the electronic medical record. For instance, racial data and residence location are self-reported. Distances were calculated using less precise 5-digit zip codes, because no coordinates of 9-digit zip codes are freely available. Finally, this study used retrospective data from a single subspecialty in the field of orthopedics at a single institution in the Midwestern United States and may not be generalizable to all of orthopedics or other areas of the country.
We did not demonstrate a relationship between community-level social deprivation (as measured by the ADI) and telemedicine use. We are unaware of other studies evaluating the use of telemedicine using ADI as a measure of socioeconomic disadvantage, but previous studies have associated higher socioeconomic status with increased telemedicine use [7,9,11]. It is likely that the effects of socioeconomic status on telemedicine use are complex and multifaceted and thus not easily elicited in a single study. More research should be done to determine the relationship of socioeconomic factors and telemedicine use.
We also did not demonstrate a relationship between insurance status and telemedicine use. Upon univariate analysis, patients with Medicare insurance were less likely to utilize telemedicine than those with private insurance, but after controlling for other variables, this relationship was not maintained. The confounding variable in this finding was likely age, suggesting age remains an important predictor of telemedicine use but insurance status alone does not.
We did not demonstrate a clear association between the use of telemedicine and increasing distance from our medical center. This finding seems counterintuitive but may be explained by a few factors. One is state policy, which prohibits our institution’s providers from completing telemedicine visits with patients not physically located in either our home state or one neighboring state. Of the 235 patients in this study whose address is 200 miles or more from the nearest clinical site, 197 (83.8%) did not live in 1 of these 2 states. This raises concern that these policies may disproportionately limit access to care for patients in other states, especially those requiring complex care or those receiving longitudinal care from the same provider.
Overall, this study suggests that variability in telemedicine use exists for demographic factors such as race and age, as previous studies have shown. Community-level social deprivation was not associated with variation in telemedicine use, suggesting that demographic differences are not broadly attributable to socioeconomic status. A potential explanation for this finding is a difference in a more specific variable, like computer ownership or Internet use. While these were not measurable in our cohort, future studies should aim to more narrowly define demographic variability in telemedicine use as we aim to reduce disparities in access to care across orthopedics.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231207632 – Supplemental material for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients
Supplemental material, sj-docx-1-hss-10.1177_15563316231207632 for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients by Brendan J. Navarro, Ling Chen and Christopher J. Dy in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231207632 – Supplemental material for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients
Supplemental material, sj-docx-2-hss-10.1177_15563316231207632 for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients by Brendan J. Navarro, Ling Chen and Christopher J. Dy in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231207632 – Supplemental material for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients
Supplemental material, sj-docx-3-hss-10.1177_15563316231207632 for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients by Brendan J. Navarro, Ling Chen and Christopher J. Dy in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231207632 – Supplemental material for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients
Supplemental material, sj-docx-4-hss-10.1177_15563316231207632 for Telemedicine Use Following Onset of the COVID-19 Pandemic Was Associated With Youth and White Race but Not With Socioeconomic Deprivation: A Retrospective Cohort Study of Orthopedic Patients by Brendan J. Navarro, Ling Chen and Christopher J. Dy in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christopher Dy reports relationships with the National Institutes of Health, the American Foundation for Surgery of the Hand, the Orthopaedic Research and Education Foundation, Sonex Healthcare, Springer, Orthocell, Johnson and Johnson, the American Orthopaedic Association, and the American Society of Peripheral Nerve. The other authors declared no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV, retrospective cohort study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.