
Abstract
Background:
To improve outcomes following anterior cruciate ligament (ACL) reconstruction, bridge-enhanced ACL restoration (BEAR) was introduced. Bridge-enhanced ACL restoration uses a collagen-based implant saturated with infused autologous blood to bridge the torn proximal and distal ACL fibers.
Purpose:
We sought to analyze the short-term complications, clinical outcomes, and patient-reported outcome measures (PROMs) in patients undergoing BEAR outside of the initial clinical trials.
Methods:
We conducted a retrospective cohort study of all skeletally mature patients who had a midsubstance or proximal ACL tear treated with BEAR by 2 surgeons at a single institution and had a minimum follow-up of 6 weeks. A total of 58 patients were included (average age was 38 years, average time from injury to surgery was 45 days). Data on demographic factors, functional outcomes, and complications were collected from electronic medical records. Patient-reported outcome measures and a descriptive return-to-activity survey were analyzed utilizing paired t-tests and Wilcoxon signed-rank tests.
Results:
All 58 patients demonstrated a grade of 1A on the Lachman test at 6 weeks postoperatively. At 6 months postoperatively, the mean active flexion was 135° ± 5°, and all patients achieved 0° extension. Although not all patients completed PROM questionnaires, among those who did we observed a significant increase in PROMs between preoperative and postoperative measurements; more than half achieved the minimal clinically important difference in all PROMs, and 26 patients (87%) had a 1-level decrease in function. There were no cases of retear or instability. Three patients (5%) had postoperative arthrofibrosis.
Conclusion:
Early results of this preliminary post-market approval study suggest that BEAR may provide a safe and non-inferior approach to ACL reconstruction in selected patients. Studies are needed to investigate the long-term outcomes of this novel technique.
Introduction
The anterior cruciate ligament (ACL) plays a critical role in knee biomechanics, providing anteroposterior and rotational stability [54]. ACL tears are the most common knee ligament injury, resulting from both contact and noncontact mechanisms [30]. Anterior cruciate ligament reconstruction (ACLR) is the most common surgical treatment of ACL tears; an annual incidence of 44 per 100,000 person-years has been estimated in the United States [26], with costs totaling nearly $1 billion [17].
The standard treatment of ACL injuries is ACLR with either autologous or allogenic tendon graft [54], but limitations include an increased risk of developing osteoarthritis (OA) after ACLR in the injured knee [15]. An ACLR may alter the biomechanics of the knee, as it does not precisely restore the complex ligament insertion or proprioceptive nerve fibers of the native ACL [19,25,27,53]. Consequently, recent research has focused on other methods to treat ACL tears [24].
The first described operative technique to treat an ACL tear was ACL repair [44], a method that had a high failure rate and poor outcomes in young and active patients [13,14,47]. The cells involved in wound repair and tissue regeneration are similar between the ACL and its collateral ligaments that can heal naturally [39,40]. However, in vivo, because the ACL is intra-synovial, it cannot form a fibrin clot [33], which is necessary for the ligament to heal. Studies have shown that the synovial fluid exerts inhibitory activity on ACL fibroblasts [2]. Furthermore, intra-articular plasmin actively works to break down formed clots [7,45].
The bridge-enhanced ACL restoration (BEAR) implant (Miach Orthopaedics, Inc.) was developed to address these biological limitations; it was cleared by the U.S. Food & Drug Administration in 2020. BEAR technology involves insertion of a cylindrical, hydrophilic, collagen-based implant saturated with autologous blood into the notch between the 2 torn ends of the native ACL following primary repair. This process creates a viscoelastic material that fills the gap, acting as a stable intra-articular bridging sponge that improves the environment for the native ruptured ACL to heal. The implant also retains blood in the tear site, allowing fibrin clots to form and release growth factors that stimulate ligament repair [6]. Preclinical studies reported favorable healing of the torn ACL [16,22,40,53] and a lower rate of post-traumatic OA in animal studies with BEAR compared with nonoperative treatment [34]. Clinical trials have reported an excellent safety profile associated with BEAR, non-inferior outcomes when compared to ACLR, and a conversion rate from BEAR to ACLR of 14% within the first 2 postoperative years [4,35,37].
We therefore aimed to analyze the short-term complications, clinical outcomes, and patient-reported outcomes in patients undergoing BEAR outside of the initial clinical trials.
Methods
Before the start of this retrospective case series, approval was obtained by the Hospital for Special Surgery Institutional Review Board. The electronic medical records of all ACLR procedures performed by 2 surgeons (S.M.S. and A.H.G.) between March 2022 and August 2023 were retrospectively reviewed. All procedures that did not utilize the BEAR protocol were excluded. All skeletally mature patients treated with the BEAR protocol were included in the final study (Fig. 1).
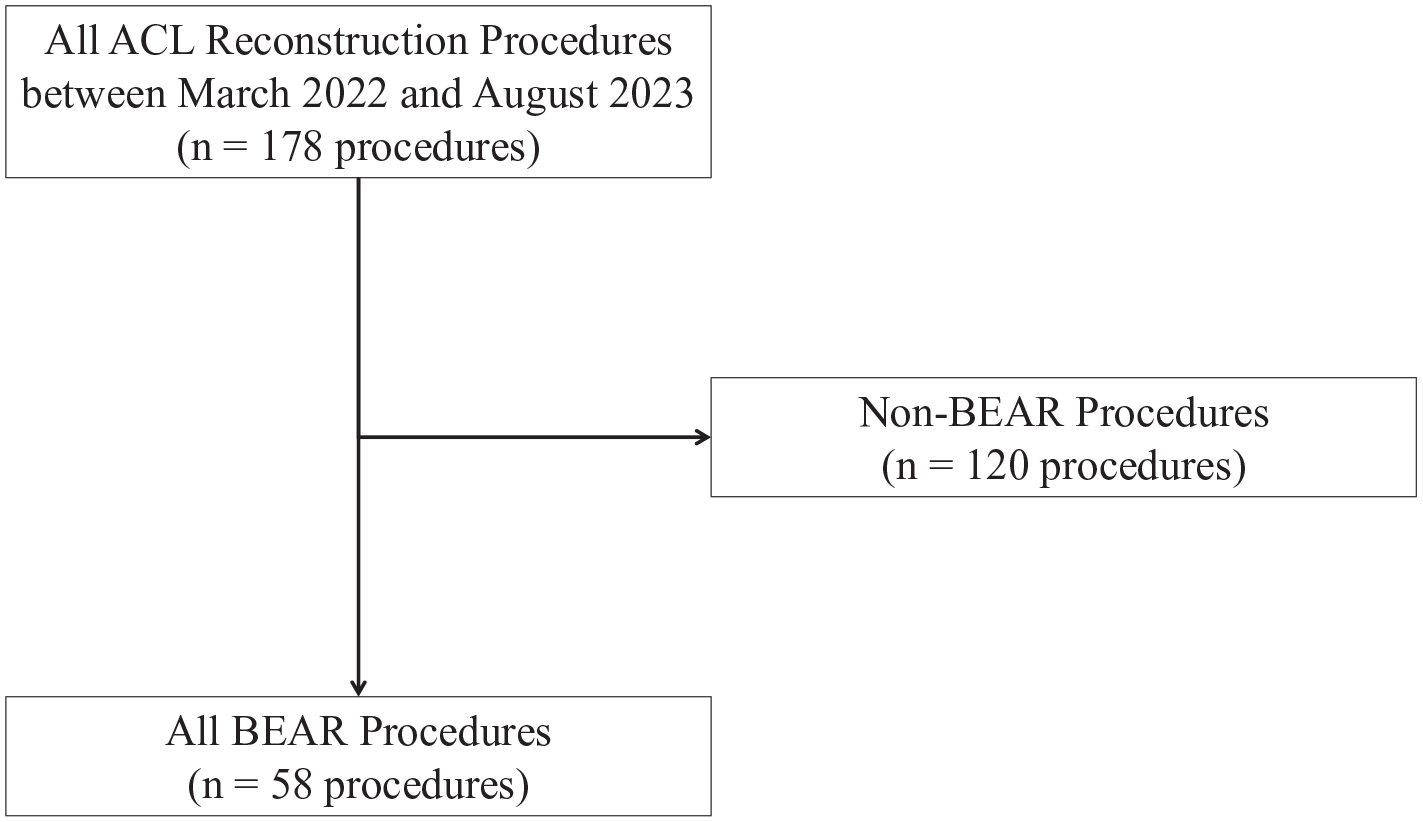
STROBE diagram of the patient cohort.
Both surgeons utilized an all-inside technique [41] and followed a modified BEAR protocol [6,36–38] for the repair. Concomitant intra-articular procedures were performed if other pathology was present. Patients were placed in a hinged knee brace immediately following the procedure. Patients were toe-touch weightbearing on the operative extremity, with the hinged knee brace locked in full extension for ambulation for 4 weeks. With clearance from the operative surgeon, patients advanced to weightbearing as tolerated, with crutch wean at 4 weeks. Patients were allowed to begin range of motion (ROM) exercises after the first 2 weeks. ROM was restricted to 0° to 90° from 2 to 4 weeks postoperatively and progressed to full ROM as tolerated after 4 weeks. Full ROM was defined as 0° to 135°. Formal physical therapy was initiated 1 week postoperatively, with crutches and braces discontinued under physical therapist supervision after patients achieved appropriate quadriceps function and tolerated weightbearing. Patients could return to sport at 36 to 52 weeks postoperatively if they had confidence when running, cutting, jumping at full speed, 90% contralateral values on hop tests, 90% quadriceps strength index, no functional complaints, and clearance by the operating surgeon [3].
Demographic data was collected, including age at surgery, sex, ethnicity, body mass index (BMI), smoking history, oral contraceptive use, previous surgery on the ipsilateral knee, and cause of injury. Perioperative data was also collected, including the time between the injury and surgery, operative time, and concomitant procedures.
The medical records of 58 patients were reviewed, and all patients met the inclusion criteria. The mean age of patients at the time of surgery was 38 ± 11 years (range: 14–64 years). The mean BMI was 24.0 ± 3.6 kg/m2 (range: 18.8–32.6). There were 41 female (71%) and 17 male patients (29%). All patients suffered a midsubstance or proximal ACL tear. The mechanism of injury was described as a twisting injury in 47 patients (81%). Injury due to skiing was most common (55%), followed by soccer (12%) and basketball (3%). Meniscal tears were identified in 21 patients (36%), with 8 patients, 10 patients, and 3 patients involving the lateral meniscus only (14%), medial meniscus only (17%), and both menisci (5%), respectively. The average clinical follow-up was 8.7 ± 4.1 months (range: 1.6–19.3 months). There were 31 patients (53%) who completed all patient-reported outcome measures (PROMs). The duration of follow-up of PROMs was not standardized; however, the mean, standard deviation, and range of the follow-up time was 9.3, 5.0, and 5.2 to 23.6 months, respectively. There were 28 patients (48%) who completed the return-to-activity survey at an average follow-up of 10.2 ± 4.8 months (range: 5.4–18.5 months; Table 1).
Demographic characteristics of BEAR patients.
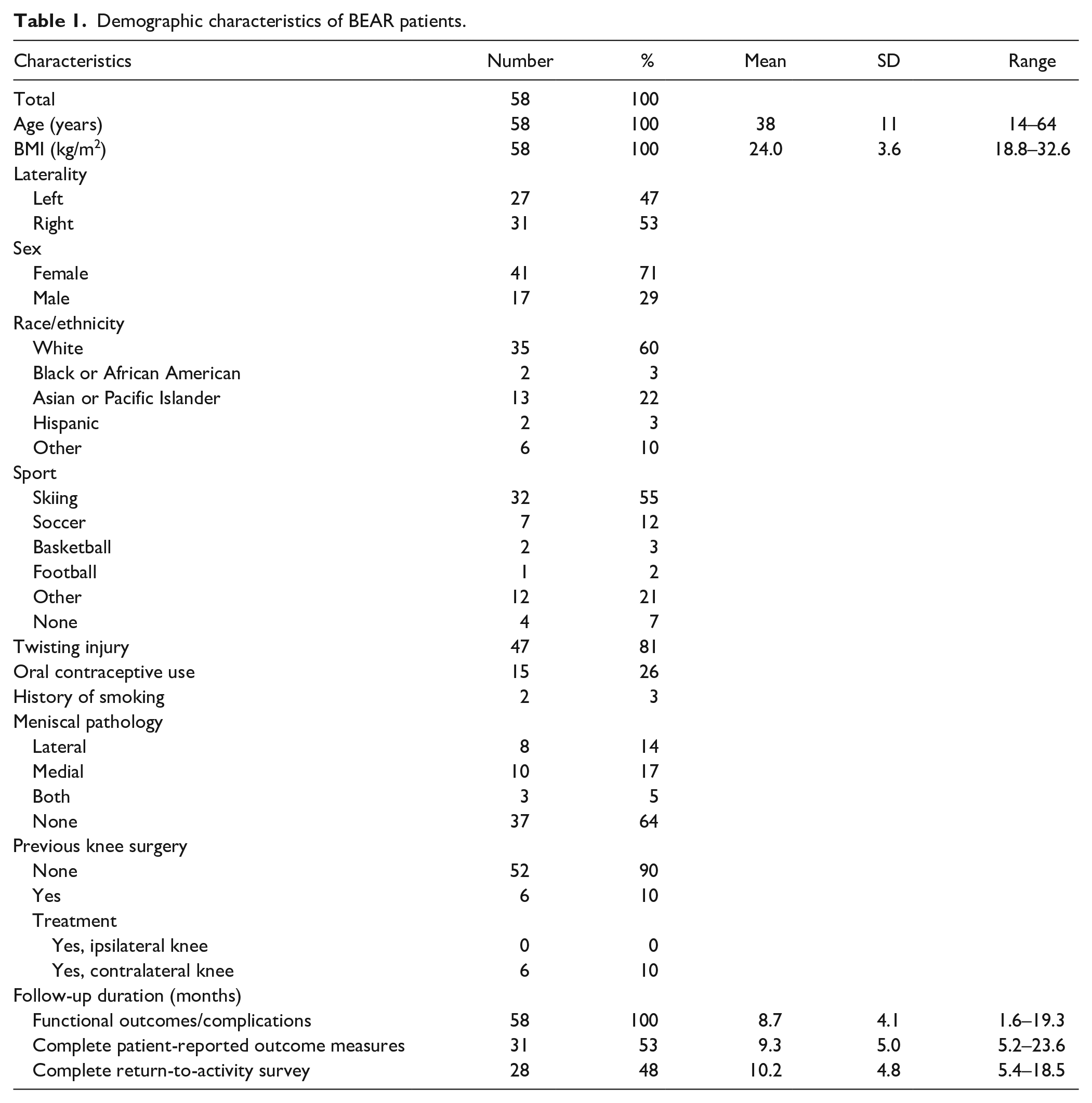
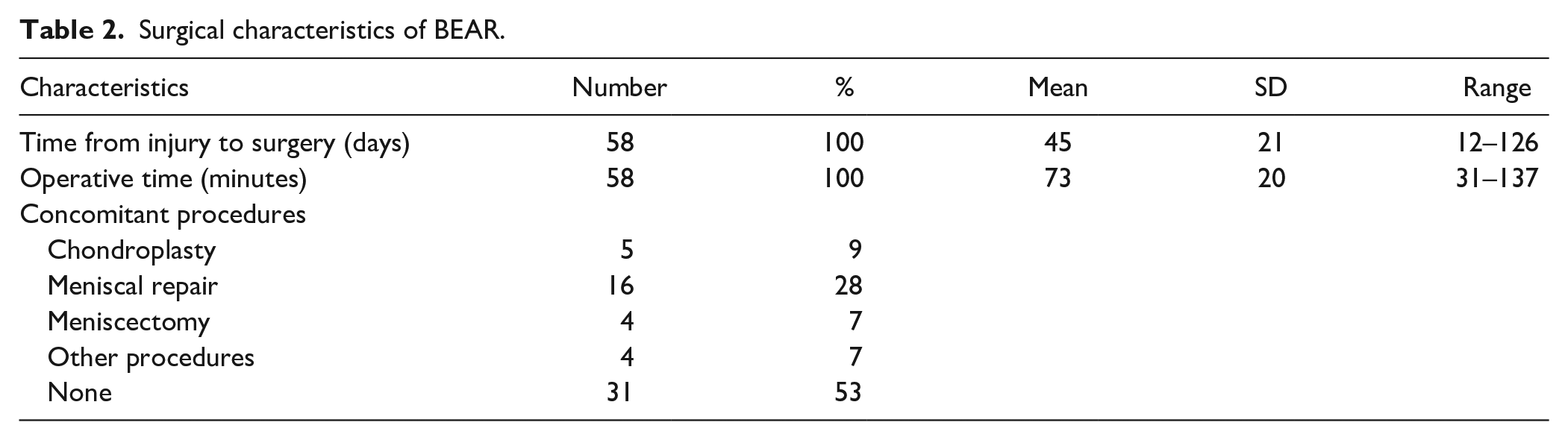
The mean time between injury and surgery was 45 ± 21 days (range: 12–126 days). There were 5 concomitant chondroplasties (9%), 16 concomitant meniscal repairs (28%), 4 concomitant meniscectomies (7%), and 4 other concomitant procedures (7%). There were 31 surgeries (53%) without a concomitant procedure. The mean operative time was 73 ± 20 minutes (range: 31–137 minutes; Table 2).
Surgical characteristics of BEAR.
Postoperative functional follow-up assessment for each patient was conducted at 6 weeks, 3 months, and 6 months postoperatively and included functional outcomes including active ROM and Lachman score measured by the operating surgeon. ROM was not tested beyond neutral. All complications related to the ACL repair were included in the analysis. International Knee Documentation Committee Subjective Knee Form (IKDC) and Knee injury and Osteoarthritis Outcome Score (KOOS) and the subscales, including pain (KOOS-Pain), other symptoms (KOOS-Symptoms), function in activities of daily living (KOOS-ADL), function in sports and recreation (KOOS-Sport), and knee-related quality of life (KOOS-QoL), were obtained preoperatively and during the postoperative course at a non-standardized time point. The minimal clinically important difference (MCID) values for ACLR used for analysis for each PROM were obtained from previous studies. The MCID values were 9.5 for IKDC [42], 14.1 for KOOS-Pain, 14.5 for KOOS-Symptoms, 10.9 for KOOS-ADL, 18.8 for KOOS-Sport, and 20.2 for KOOS-QoL [23,43]. A return to activity survey [52] was also administered, which included questions about which sporting or fitness activity they had preferred before surgery, whether they were able to return to that activity after surgery, whether their level of function changed after surgery, and how satisfied they were with their return to activity (Supplemental Table 1).
Statistical Analysis
Descriptive statistics, including means, standard deviations, frequencies, and percentages, were used to evaluate patient characteristics. Data for the change in PROMs, including IKDC, KOOS-Pain, KOOS-Sport, and KOOS-QoL, were normally distributed per the results of the Shapiro-Wilk test; therefore, paired t-tests were used to evaluate differences from preoperative to postoperative PROMs. KOOS-Symptoms and KOOS-ADL failed the Shapiro-Wilk test; therefore, the Wilcoxon signed-rank tests were used to evaluate differences in PROMs. The categorical variables for the level of function question in the return to activity survey were redefined as numerical values for data visualization with 1 representing the worst level of function and 7 representing the best level of function. Statistical significance was determined at the α < 0.05 level. Data processing and statistical analysis were performed with RStudio.
Results
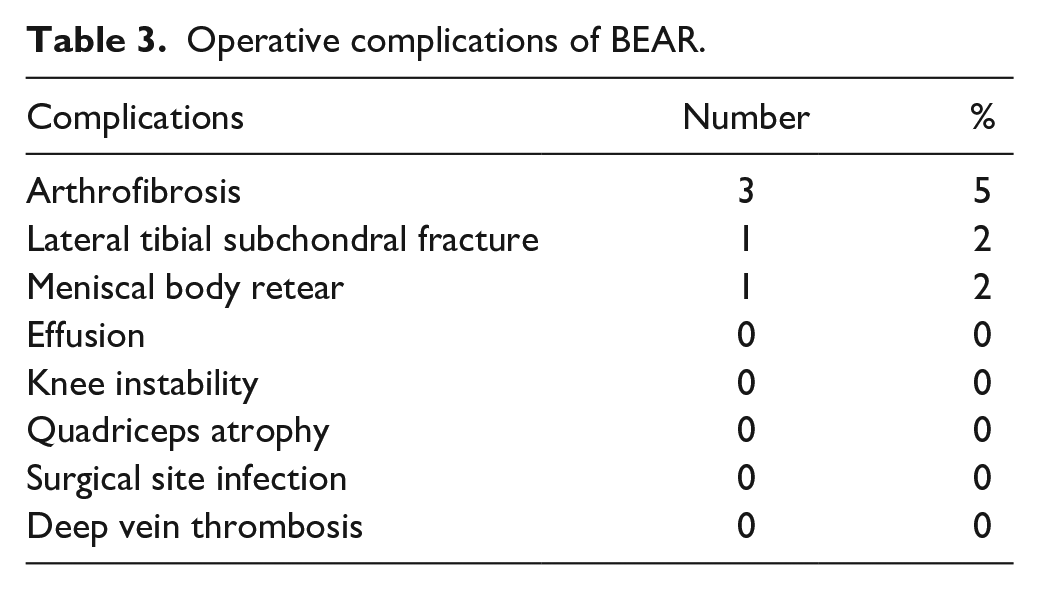
Among the 58 patients included, there were 5 complications (9%). There were 3 cases (5%) of postoperative arthrofibrosis requiring lysis of adhesions (LOA). LOA occurred on average 70 ± 7 days (range: 64–78 days) after the initial procedure. After LOA, all 3 patients progressed to achieve 0° to 135° of ROM. There was 1 case (2%) of postoperative lateral tibial subchondral fracture 16 months post-BEAR due to injury while playing tennis that did not require a second surgery. There was 1 case (2%) of anterior horn of the lateral meniscus retear requiring revision, partial lateral meniscectomy at 8 months post-BEAR. There were no cases of persistent effusion, instability, quadriceps atrophy, surgical site infection, deep vein thrombosis, or any other complications typically associated with ACLR (Table 3).
Operative complications of BEAR.
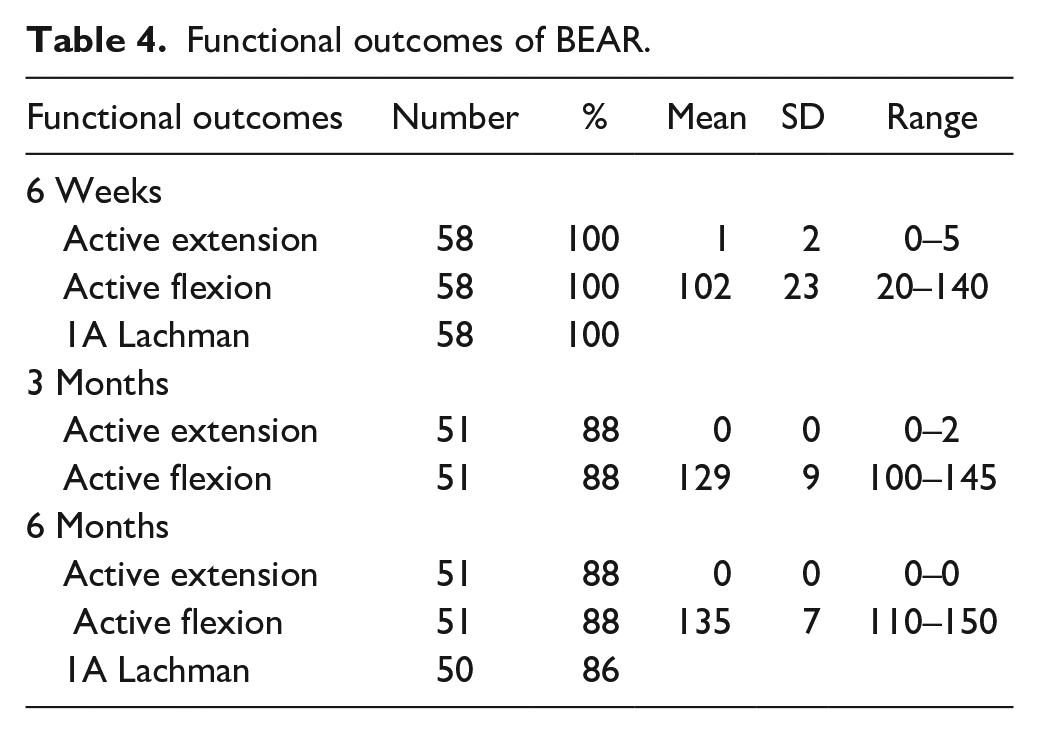
All patients (100%) completed a 6-week follow-up visit. At 6 weeks postoperatively, the mean extension was lacking 1° ± 2° (range: 0°–5°), and the mean flexion was 101° ± 22° (range: 20°–140°). There were 17 patients (29%) who had 90° of flexion or less at 6 weeks. Of the 47 patients (81%) who had completed 3 months of follow-up, all had full extension, and the mean knee flexion was 129° ± 9° (range: 100°–145°). Of the 51 patients (88%) who had completed 6 months of follow-up, all maintained full extension, and the mean maximal knee flexion was 135° ± 5° (range: 125°–150°). At the 6-week and 6-month time points, all patients, except 1, demonstrated a 1A Lachman score on clinical examination (Table 4).
Functional outcomes of BEAR.
There were 53 patients (91%) and 40 patients (69%) who answered the preoperative IKDC and all KOOS subscales, respectively. There were 43 patients (74%) and 31 patients (53%) who answered the postoperative IKDC and all KOOS subscales, respectively. The mean, standard deviation, and range of the duration of follow-up for IKDC was 9.3, 5.0, and 5.2 to 23.6 months, respectively. The mean, standard deviation, and range of the duration of follow-up for KOOS subscales was 8.4, 3.7, and 5.2 to 18.9 months, respectively. There was a significant increase in IKDC (P < .001), KOOS-Pain (P < .001), KOOS-Symptoms (P < .001), KOOS-Sport (P < .001), KOOS-QoL (P < .001), and KOOS-ADL (P < .001) compared with the baseline measurements. Fifty-two percent of patients who completed PROMs achieved the MCID for each PROM (Table 5).
Patient-reported outcome measures of BEAR.
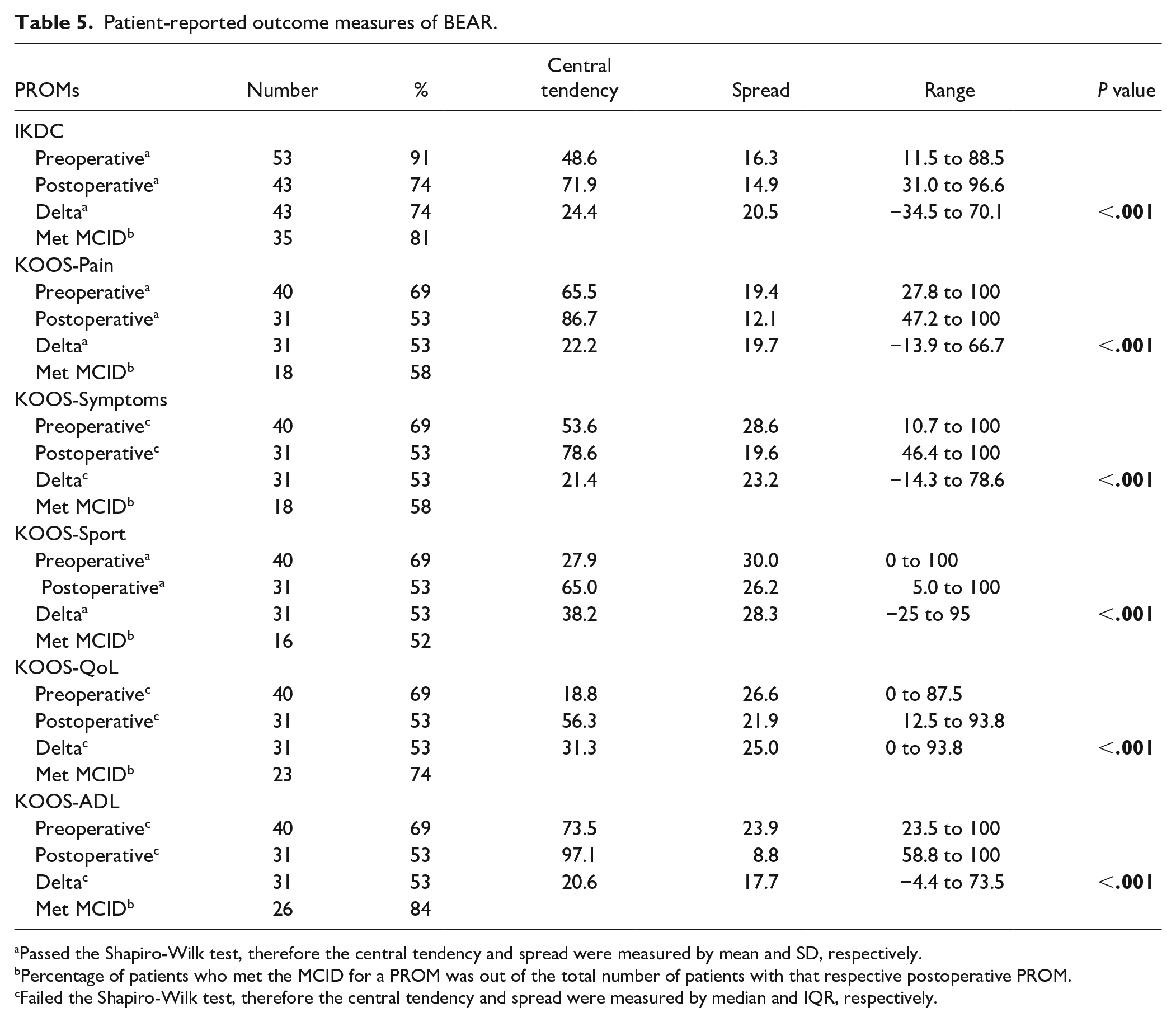
Passed the Shapiro-Wilk test, therefore the central tendency and spread were measured by mean and SD, respectively.
Percentage of patients who met the MCID for a PROM was out of the total number of patients with that respective postoperative PROM.
Failed the Shapiro-Wilk test, therefore the central tendency and spread were measured by median and IQR, respectively.
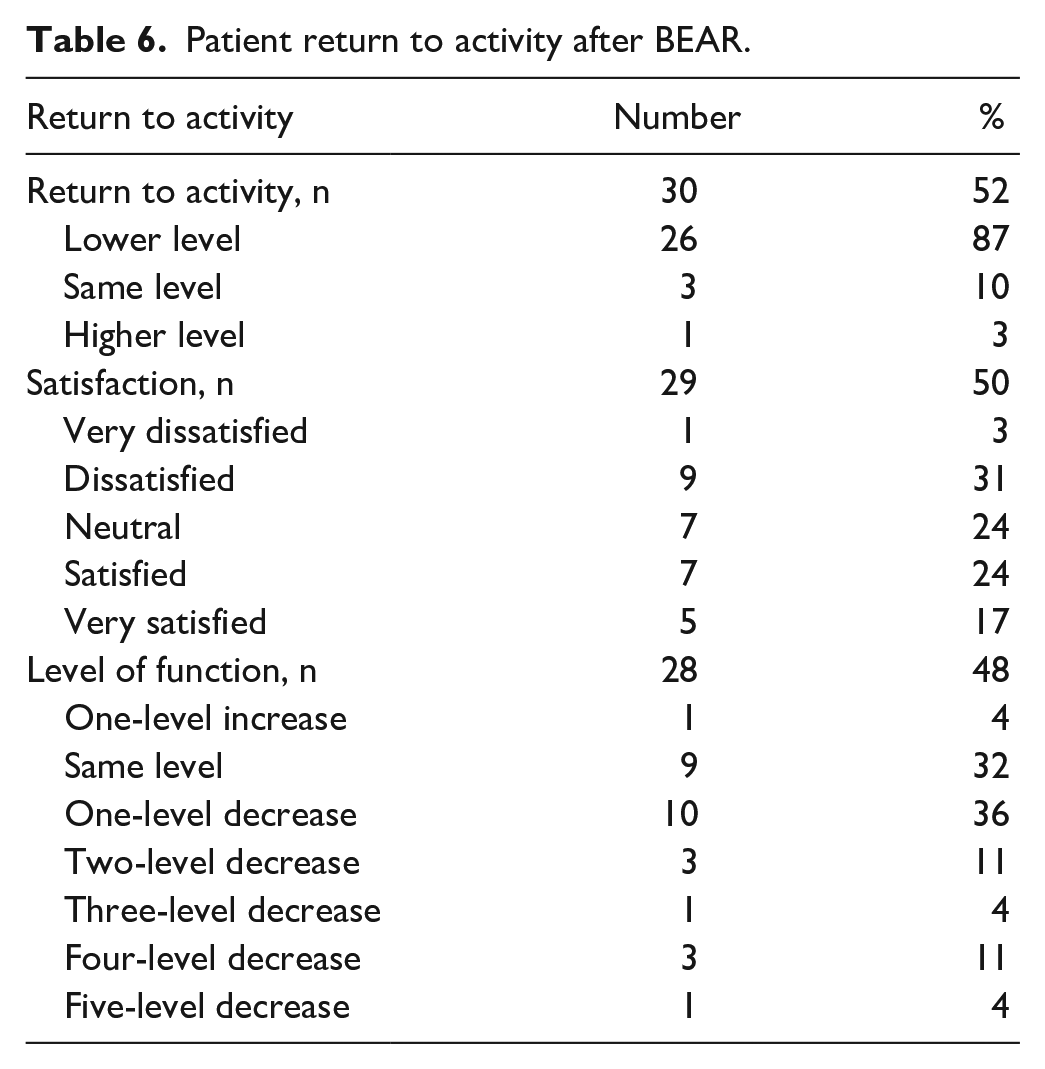
There were 30 patients (52%) who answered 1 or more sections of the return to activity survey. There was 1 patient (3%) who was able to return to a higher level of activity, 3 patients (10%) who returned to the same level of activity, and 26 patients (87%) who returned to a lower level of activity. There were 29 patients (50%) who answered the satisfaction portion of the return to activity survey. Of the respondents, 5, 7, 9, and 1 individual answered that they were very satisfied (17%), satisfied (24%), neutral (24%), dissatisfied (31%), and very dissatisfied (3%) with their return to activity (Table 6).
Patient return to activity after BEAR.
Of the 28 patients (48%) who completed the level of function portion of the survey, 9 patients (32%) reported no change in the level of function, 10 patients (36%) reported a 1-level decrease in function, 3 reported a 2-level decrease in function (11%), 1 patient (4%) reported a 3-level decrease in function, 3 patients (11%) reported a 4-level decrease in function, 1 patient (4%) reported a 5-level decrease in function, and 1 patient (4%) reported a 1-level increase in function (Fig. 2).
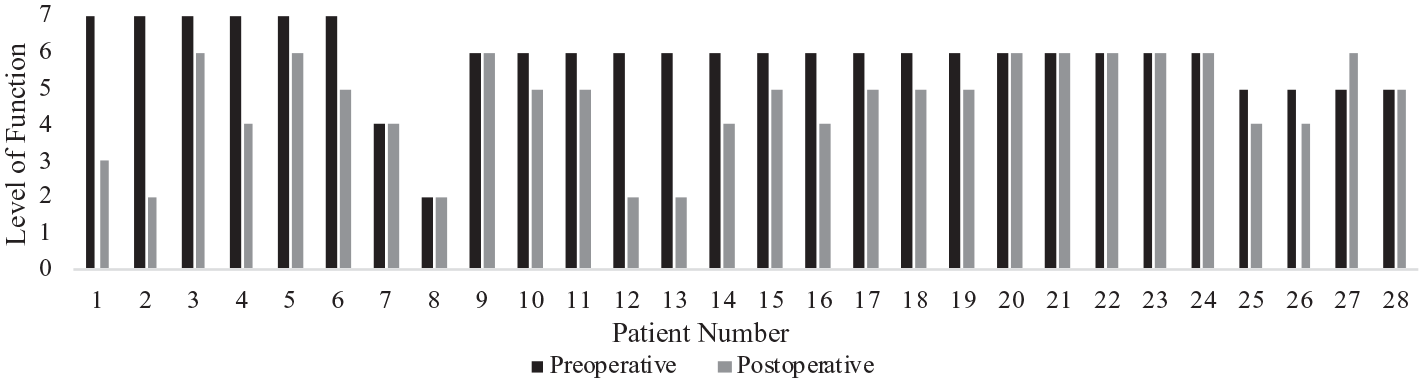
Patients’ level of function change after BEAR.
Discussion
This preliminary retrospective cohort study is the first post-market evaluation of BEAR outcomes for the treatment of a midsubstance or proximal ACL tear. We found that BEAR offered a low complication rate and overall satisfactory short-term outcomes. Specifically, the mean ROM at 6 months was 0° to 135°. There were 5 postoperative complications: 3 cases of arthrofibrosis, 1 of tibial subchondral fracture, and 1 of meniscal body retear. There was a significant increase in PROMs from preoperative to postoperative evaluation, and 52% of patients who completed PROMs achieved the MCID for each PROM.
Several limitations should be acknowledged. This is a preliminary study with some patients yet to achieve 6 months of follow-up; therefore, the results may change when all patients achieve 6 months of follow-up. The non-randomized nature prevented a direct comparison between BEAR and ACLR. The short-term follow-up limits the conclusions that may be made regarding long-term functional outcomes and complications. The small sample size limits study generalizability and prevents subgroup analyses of which patients would benefit from BEAR. Patients who participated in post-injury presurgical physical therapy may have had improved preoperative PROMs, which could have confounded the results. Finally, not all patients completed PROMs and return to activity questionnaires, and this missing data potentially limits the generalizability of our findings.
This study aimed to assess the clinical efficacy of a novel surgical technique beyond the age inclusion criterion given by previous clinical trials. The age of included patients ranged from 14 to 64 years, which more effectively represents the patients affected by ACL tear in clinical practice. The broader age inclusion criterion employed in this study offered a more precise representation of short-term outcomes and complications associated with BEAR, which could lead to improved external validity and increased clinical applicability.
The BEAR II Trial enrolled patients only aged 13 to 35 years who had a complete ACL tear and were less than 45 days from their injury [35,37]. The patients undergoing BEAR in the BEAR II Trial had an average age of 17 and ranged from 16 to 20. Our study included an average age older than the maximum inclusion age in the BEAR II Trial. Furthermore, our study had an average time between injury and surgery greater than the maximum cutoff for the BEAR II Trial. In studies of ACLR, it has been shown that a shorter time between injury and surgery is associated with increased postoperative PROMs [12] and a decreased risk of secondary meniscal injury [8,18,21,48], chondral defects [8,18], contralateral ACL tears [10], symptomatic OA [18], and future total knee arthroplasty [18].
While not part of the inclusion or exclusion criteria, this study had a higher percentage of female patients than the BEAR II Trial. This study had a similar BMI distribution and distribution of patients with a noncontact injury. There were a higher percentage of patients undergoing concomitant procedures in the BEAR II Trial compared to this study [35,37].
At 2 years, 53% and 97% of the patients in the BEAR II Trial receiving BEAR and ACLR, respectively, had an “A” ROM IKDC objective score [35]. In this study, all patients with 6 months of follow-up had a full ROM comparable to the “A” ROM IKDC objective score. In addition, 93% and 90% of the patients in the BEAR II Trial receiving BEAR and ACLR, respectively, had a grade A Lachman. In this study, all patients had a 1A Lachman at 6 weeks. Furthermore, as patients progressed through their rehabilitation process, they generally improved regarding their ROM and activity level. Despite the broader inclusion criteria, this study showcased functional outcomes that were similar to patients in the BEAR II Trial.
The previous clinical trials have established that the BEAR procedure has higher IKDC and KOOS subscale outcomes at early time points postoperatively when compared to ACLR patients [5,37]. The IKDC and KOOS scores in this study were similar to what was previously reported in the literature. In a systematic review of 30 studies and 2253 patients who underwent ACLR, Agarwalla et al established that the difference between the preoperative and 6-month postoperative IKDC means was 26.3 points [1]. In our study, the mean difference between the preoperative and postoperative IKDC scores was 24.4 points (Table 5), at an average postoperative time of 9.3 months, which is similar to the rate established in the literature. Agarwalla et al further established that the differences between preoperative and 6-month postoperative KOOS-Pain, KOOS-Symptoms, KOOS-Sport, KOOS-QoL, and KOOS-ADL scores were 14.2, 15.7, 26.9, 25.9, and 12.1, respectively [1]. Patients in our study surpassed those values by a margin of 8.0, 5.7, 11.3, 5.4, and 8.5, respectively. Furthermore, the majority of patients achieved 2-year ACLR MCID values for each PROM prior to having 2 years of follow-up. Despite the broader inclusion criteria and differences in postoperative involvement, this study demonstrates that PROMs were non-inferior to the BEAR patients in the BEAR II trial and established ACLR rates in the literature. As there is evidence that maximum PROM improvement after ACLR occurs up to 1 year after surgery [1] and is preserved at 6 and 10 years postoperatively [31], it suggests that further study and follow-up of the patients in this study is warranted.
Of the return to activity survey respondents, 10 patients (34%) were not satisfied with their activity level. This could be due to the patients having inflated preoperative perspectives regarding their postoperative return to activity with the new BEAR procedure which results in disappointment with their true postoperative activity level. The majority returned to a lower level of activity, and two-thirds either maintained their level of function or had a 1-unit decrease in their level of function in their respective activities. Similar to the BEAR II trial, the early resolution of symptoms and functional recovery did not translate to an improved return of activity [5]. This is a similar finding to a previous study analyzing the return to sport after ACLR with IKDC [5,28]. Furthermore, patients after ACLR reach a patient-acceptable symptom state 12 months after their surgery [32], and 67% of elite athletes return to a lower level of function in their sport after ACLR [20]. This warrants the need for long-term follow-up of the patients in this study to understand the return to activity of BEAR patients 1 year after their surgery.
Arthrofibrosis is a well-described complication after ACLR, with a reported incidence of 2% to 35% [9,11,29,49,50]. There were 3 (5%) cases of arthrofibrosis seen in this study. Of note, 2 of those patients underwent a concomitant medial meniscal repair and one of those patients underwent a concomitant medial meniscectomy. The 3 patients had an average age of 42 ± 7 years (range: 35–48 years), an average BMI of 25.0 ± 4.3 kg/m2 (range: 20.8–30.0 kg/m2), and 47 ± 4 days (range: 44–52 days) between injury and surgery. After treatment of the arthrofibrosis with LOA, the patients progressed to full ROM. Only 1 of the 3 patients answered PROMs, and they saw improvements in their PROMs after treatment of the arthrofibrosis. This result is similar to previous studies that have documented improvement in ROM after intervention for arthrofibrosis [9,46,51]. There were no reported instances of arthrofibrosis in the BEAR patients in the BEAR II Trial [4,35,37].
There was 1 case (2%) of a 1B Lachman at 6-month follow-up with subsequent repeat pivot shift injury at 17 months post-BEAR while playing tennis. This patient has had improvement in their IKDC and KOOS subscale scores, returned to a slightly lower level of activity, and has had to decrease their level of function to moderate recreational activities. There was 1 case (2%) of meniscal retear of the anterior horn of the lateral meniscus requiring partial lateral meniscectomy at 8 months post-BEAR. This patient had a decrease in the IKDC and KOOS-Symptoms scores but maintained the same KOOS-QOL score and saw increases in KOOS-Pain, KOOS-ADL, and KOOS-Sport. The patient was able to return to the same level of activity but had a decreased level of competitive sports. The rate of meniscal complications in the follow-up period is markedly lower than the incidence of postoperative meniscal complications in the BEAR II Trial, which was 23% [35]. Finally, the major complication in the BEAR II Trial was conversion to ACLR within the first 2 postoperative years in 14% of the population [4,35,37]. None of the patients required conversion to ACLR in this study, but further follow-up is needed.
In conclusion, despite the broader inclusion criteria used in this preliminary post-market approval study compared with the BEAR II trial, we found that patients treated with BEAR demonstrated non-inferior clinical outcomes and a low complication rate for the treatment of proximal or midsubstance ACL tears. Among patients who completed the questionnaires, we found improvements in PROMs similar to those previously reported in the literature. Although early and mid-term results presented by the BEAR trials are promising, it remains to be seen whether this procedure will outperform ACLR. Although this study was limited by the retrospective nature, short follow-up, and small cohort, it adds to the growing bank of external data on BEAR. These early results suggest that BEAR may provide a safe and non-inferior approach to ACLR in selected patients. Future studies need to be conducted to confirm the long-term outcomes of this novel technique.
Supplemental Material
sj-docx-1-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-1-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-2-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-3-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-4-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-5-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-6-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316241265351 – Supplemental material for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications
Supplemental material, sj-docx-7-hss-10.1177_15563316241265351 for A Preliminary Study of Post-Market Bridge-Enhanced ACL Restoration (BEAR) Suggests Non-Inferior Short-Term Outcomes and Low Complications by Aakash K. Shah, Morgan E. Rizy, Ava G. Neijna, Tyler J. Uppstrom, Andreas H. Gomoll and Sabrina M. Strickland in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andreas H. Gomoll, MD, reports relationships with Arthroscopy Association of North America, Bioventus, CartiHeal Inc, Cartilage, Engage, ICRS, JRF, Knee Surgery, Sports Traumatology, Arthroscopy, Linvatec Corp., Miach Orthopaedics Inc. (the manufacturer of the implant studied), Moximed Inc., Organogenesis Inc,. Orthopaedic Journal of Sports Medicine, Pacira Pharmaceuticals Inc., Stryker, Smith & Nephew Inc., and Vericel. Sabrina M. Strickland, MD, reports relationships with Arthroscopy Association of North America, American Journal of Sports Medicine, American Orthopaedic Society for Sports Medicine, Engage, Miach Orthopaedics, Inc. (the manufacturer of the implant studied), Moximed Inc., Smith & Nephew Inc., Stryker, and Vericel. The other authors declared no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for all patients included in this study by the IRB of Hospital for Special Surgery.
Level of Evidence
Level IV: retrospective cohort study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.