
Abstract
Background: Hallux valgus (HV) is recognized as a triplanar deformity. A biplanar locking plate (BLP) system corrects this deformity through first tarsometatarsal joint (TMTJ) arthrodesis, with specialized reduction tools and cutting guides. Yet the optimal surgical technique and fixation construct for first TMTJ arthrodesis remains controversial. Purpose: We sought to compare the BLP system with a modified Lapidus (ML) technique with crossed-screw fixation in terms of radiographic outcomes, complications, and reoperations. Methods: In this retrospective multicenter study, we identified a series of consecutive patients who underwent first TMTJ arthrodesis for HV with either the ML procedure at institution A or the BLP system at institution B. Patients 18 years of age with a minimum of 6 months of postoperative radiographs were included. There were 130 patients, 65 in each group, including 121 women (93.8%) with a median age of 58 years and mean radiographic follow-up of 7.1 months. Data included preoperative and postoperative HV angle (HVA), intermetatarsal angle (IMA), and tibial sesamoid position (TSP), plus complications and reoperations. Statistical testing included Mann-Whitney U, Wilcoxon signed rank, Fisher exact, McNemar, and multivariable regression. Results: After adjusting for confounding variables, the BLP system was associated with significantly greater improvements in postoperative IMA and HVA but not TSP. There were no significant differences in rates of complications (ML: 18.4%; BLP: 9.2%) or reoperations (ML: 4.6%; BLP: 7.7%). Conclusion: This retrospective multicenter review found that the BLP system was associated with greater improvement in radiographic HV parameters compared with the ML procedure using crossed-screw fixation. Clinical significance is unclear as complication and reoperation rates were similar between groups. Further study in this regard is warranted.
Keywords
Background
Hallux valgus (HV) deformity is the most common forefoot condition in adults, affecting approximately 23% to 35.7% of adults [16]. Understanding of the anatomy, pathogenesis, and appropriate surgical techniques has advanced considerably. First tarsometatarsal joint (TMTJ) arthrodesis was introduced for HV correction in the early 20th century [1]. The Lapidus procedure, an operative technique including a non-instrumented arthrodesis of the first TMTJ and first intermetatarsal joint, was described by Albrecht [1] and Truslow [25] and later popularized by Paul Lapidus in 1931 [8,12,13]. When Lapidus introduced the procedure, only a single plane of instability, the axial plane, was addressed, with the goal to correct the increased 1–2 intermetatarsal angle (IMA). Subsequently, HV was understood as a triplanar deformity, leading to technique modifications.
The triplanar deformity of HV involves axial metatarsus varus and HV, sagittal hypermobility, and coronal pronation of the first metatarsal. Increasingly recognized is coronal plane rotation. First metatarsal pronation was found to be present in 87.3% of HV deformities evaluated using weightbearing computed tomography scans [11]. In addition, first TMTJ hypermobility is now recognized as contributing to both primary and recurrent HV. Unaddressed first metatarsal pronation and hypermobility have been implicated in deformity recurrence and may also negatively affect patient-reported outcome measures (PROMs)[5].
The anatomic center of rotation of angulation (CORA) of the HV deformity often lies at the TMTJ [23]. Thus, the triplanar nature of the deformity may be best addressed at the first TMTJ. Triplanar first TMTJ arthrodesis has the power to correct HV in all 3 anatomical planes at the apex of the deformity. To accomplish this, the surgeon must reduce the IMA in the axial plane, correct rotation of the first metatarsal in the coronal plane, and stabilize the medial column in the sagittal plane.
Despite numerous clinical and biomechanical cadaveric studies [2,13,26], the optimal surgical technique and fixation construct for first TMTJ arthrodesis remains controversial. In consideration of the technical difficulty of the modified Lapidus (ML) technique, the biplanar locking plate (BLP) system, known as “Lapiplasty” (Treace Medical Concepts, Inc., Ponte Vedra Beach, FL), was developed to reproducibly correct the triplanar deformity at the CORA, adjustable to the degree of correction required. The BLP system includes a cut guide, positioner, joint distractor and compressor, and biplanar 90° dorsolateral and medial locking plates, all of which is costlier than other fixation constructs. However, it is important to note that similar techniques and fixation can be employed to achieve triplanar correction without this specific system. As health care is increasingly value-focused, we sought to design a study to compare the BLP system with an ML technique with crossed-screw fixation. Information on the cost of the fixation systems was not part of the scope of this study and thus it was not collected for comparison between the techniques. However, we recognize that the average cost of anatomic locking plates and screws is typically higher than that of crossed-screw fixation. We hypothesized that patients undergoing first TMTJ arthrodesis for HV correction with the BLP system would have equivalent radiographic correction and similar reoperation and complication rates to include nonunion, recurrent HV, wound complications, sesamoiditis, symptomatic hardware, and extensor hallucis longus (EHL) tendon injury, when compared with patients treated with an ML technique and fixation.
Methods
A retrospective multicenter review was conducted to identify a consecutive series of patients who underwent first TMTJ arthrodesis for HV correction, with use of either the ML and crossed-screw fixation at institution A or the BLP system at institution B. Approval from each institution’s institutional review board was obtained prior to study initiation. At institution A, a consecutive series of patients was identified from October 2016 to October 2018 using a prospectively collected registry. At institution B, records were queried from September 2016 to March 2021 using the current procedural terminology (CPT) code 28297. Inclusion criteria included age above 18 years, preoperative and postoperative weightbearing anteroposterior (AP) and lateral foot radiographs, and a minimum of 6 months postoperative radiographic follow-up. Exclusion criteria included primary conditions other than HV, previous first ray surgeries, ipsilateral hindfoot or midfoot arthrodeses, or other concomitant procedures that may alter postoperative recovery.
At institution A, patients underwent an ML procedure with 2 crossed screws, as previously described [14]. All procedures were performed by 1 of 7 foot and ankle fellowship–trained orthopedic surgeons. Lateral soft tissue release and/or calcaneal autograft were performed at the surgeon’s discretion. In all cases, fixation was performed with two 3.5-mm or 4.0-mm cortical screws in a crossed compression screw pattern. Postoperatively, patients were immobilized in a splint for 2 weeks with strict non-weightbearing. They transitioned to a controlled ankle motion (CAM) boot at 2 weeks and remained non-weightbearing for an additional 4 weeks. At 6 weeks, patients advanced their weightbearing in the walking boot and, at 10 weeks, returned to full weightbearing in supportive shoes with gradual return to activities.
At institution B, the BLP system was used for correction and fixation in all cases. All procedures were performed by 1 of 2 foot and ankle fellowship–trained orthopedic surgeons. A first ray positioner and three-dimensional cut guide were used to perform the joint-level resection. Fixation was performed using 2 BLPs, positioned dorsolaterally and medially. Additional fixation, including compression screws, was used at the surgeon’s discretion. No bone graft was utilized in the BLP patients. All patients in this cohort had a lateral soft tissue release performed through a separate incision over the first webspace. Postoperatively, patients were immobilized in a CAM boot and permitted heel weightbearing as tolerated immediately. At 6 weeks, patients transitioned into supportive shoes with gradual return to activities.
Patient demographics, comorbidities, and perioperative data were collected. Radiographic parameters, including hallux valgus angle (HVA), 1–2 IMA, and tibial sesamoid position (TSP) were measured preoperatively and at final follow-up (Fig. 1). Complications and reoperations were determined by review of all postoperative patient encounters and notes.
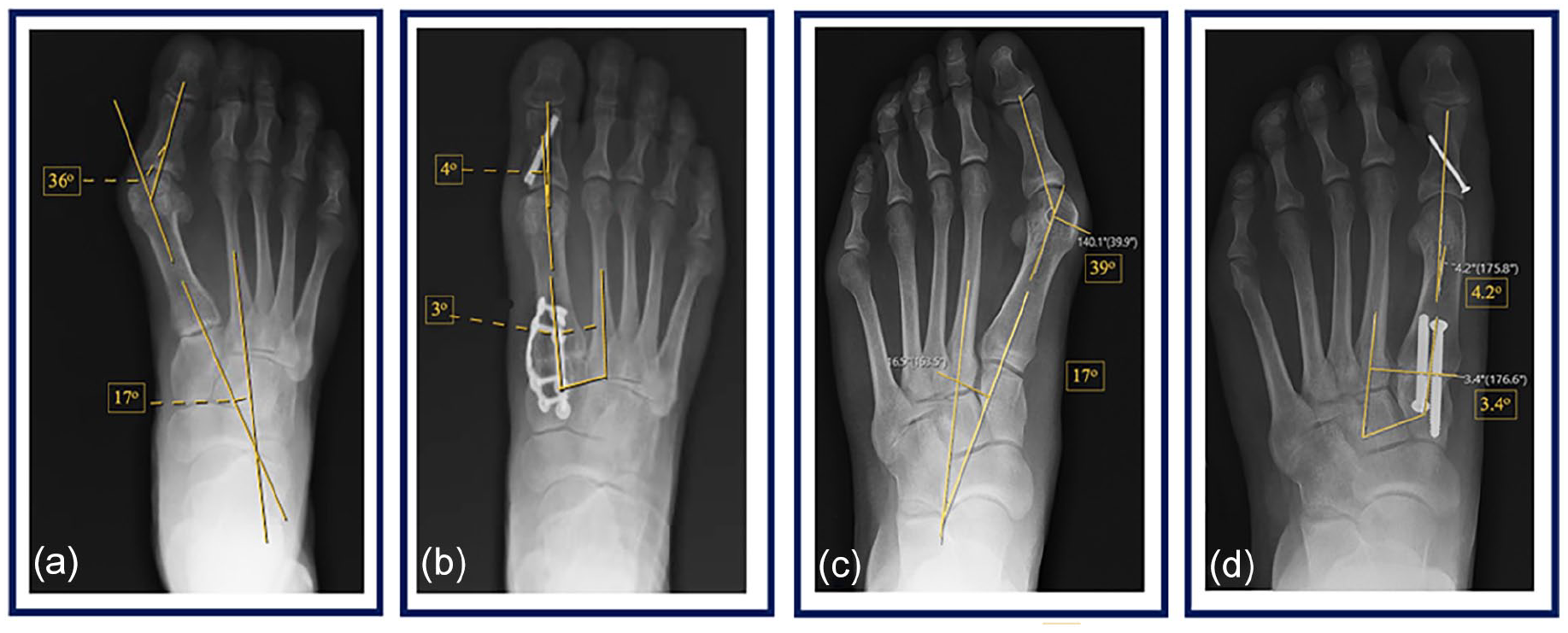
(a) Preoperative and (b) postoperative anteroposterior radiographs demonstrating hallux valgus (HV) correction with the biplanar locking plate fixation system versus (c) preoperative and (d) postoperative radiographs demonstrating HV correction with the modified Lapidus with crossed screws. Measurements of the hallux valgus angle (HVA) and 1–2 intermetatarsal angle (IMA) are shown.
A total of 130 patients, 65 in each cohort, were included (Table 1). There were 121 female patients (93.8%). The pooled median age was 58 (range 50–64) years, body mass index (BMI) 24.3 (range 22.3–28.8) kg/m2, and radiographic follow-up 7.1 (range 4.2–11.7) months. The BLP cohort had a greater average BMI (25.6 vs 23.2 kg/m2, P = .048). Otherwise, there were no significant demographic or comorbidity differences between groups. Concomitant procedures performed are outlined in Table 2. All patients in the BLP cohort had a lateral release compared with only 24 patients (36.9%) in the ML cohort. A concomitant Akin osteotomy of the first proximal phalanx was performed in 57 patients (87.7%) in the BLP cohort and 49 patients (75.4%) in the ML cohort. In addition, 26 patients (40%) in each cohort underwent concomitant correction of lesser toe deformities.
Demographics and comorbidities.

ASA American Society of Anesthesiologists.
Concomitant procedures.

Numbers represent n (percentage).
IC intercuneiform), MT metatarsal, TMT tarsometatarsal.
Lesser toe correction: Encompasses both flexible and rigid hammertoe and claw toe procedures for digits 2 to 5, including the following: Weil osteotomy, plantar plate repair, flexor to extensor tendon transfers, extensor tendon lengthening, proximal interphalangeal resection, and arthrodesis and so forth.
Statistical Analysis
An a priori power analysis was employed at the initiation of the study based on the following assumptions gathered from historic data from institution A: ML postoperative IMA: 5.0°, BLP postoperative IMA: 6.4°, and a standard deviation of 2.8° for both groups. To detect a difference of 1.4°, at a power of 0.80 and with even allocation between the 2 groups, a sample size of 128 or at least 64 patients in each group would be required. This calculation was done for a 2-sided test with a type I error of 0.05.
A Shapiro-Wilk test was applied to check the normality of the continuous variables, which demonstrated nonparametric data. Median and interquartile range were summarized for continuous variables and count, and percentage for discrete variables. To compare cohorts, Mann-Whitney U tests were applied for continuous variables and Fisher exact tests for discrete variables. To examine preoperative and postoperative differences, Wilcoxon signed-rank tests were applied for continuous radiographic outcomes and McNemar’s tests for binary outcomes. Multivariable linear regression models were used for IMA and HVA, and multivariable logistic regression was used for binary TSP outcome to examine the effect of surgical type, adjusted for preoperative radiographic measurement, age, sex, and BMI. Tibial sesamoid position was assessed as a binary variable, classified as TSP less than or equal to 4 and TPS greater than 4. Statistical significance was defined as P
Results
Both cohorts were observed to have significant improvements in HVA, IMA, and TSP preoperatively to postoperatively (Table 3). The procedures demonstrated an average HVA correction of 19.6° (P < .001) in the ML cohort and 29.0° (P < .001) in the BLP cohort. The BLP cohort achieved a greater normalization in postoperative HVA than the ML cohort (4.0° vs 11.4°, respectively; P < .001). The ML cohort had a significantly higher preoperative IMA compared with the BLP cohort (P < .001). The procedures achieved an average IMA correction of 10.6° (P < .001) in the ML cohort and 10.0° (P < .001) in the BLP cohort. The BLP cohort achieved a greater normalization in postoperative IMA (3.0° vs 5.8°, respectively; P < .001).
Radiographic outcomes of the Modified Lapidus group compared with the Biplanar locking-plate group.

HVA hallux valgus angle, IMA intermetatarsal angle, TSP tibial sesamoid position.
Median (Q1–Q3).
n (percentage).
There were between-group differences in terms of TSP, but these did not reach statistical significance. Most patients had a TSP of greater than 4 preoperatively (88% ML cohort, 75% BLP cohort; P = .112) and corrected to a TSP of less than or equal to 4 postoperatively (97% ML cohort, 100% BLP cohort; P = .4961).
After adjusting for age, sex, BMI, preoperative HVA, and preoperative IMA, the BLP system was associated with significantly lower/improved postoperative IMA (β = −2.03, 95% confidence interval [CI], −2.78 to −1.37, P < .001) and lower/improved postoperative HVA (β = −7.48; 95% CI, −9.69 to −5.26; P < .001), but not postoperative TSP.
There were no significant differences in the incidence of complications (P = .2034) or reoperations (P = .7178) between cohorts (Table 4). There were 12 (18.4%) complications in the ML cohort and 6 (9.2%) in the BLP cohort (P = .2034). The most notable complications included 1 (1.5%) nonunion in the BLP cohort, 1 (1.5%) hallux varus in the ML cohort, 3 (4.6%) delayed wound healing in the ML cohort, 3 (4.6%) cases of symptomatic hardware requiring removal in the ML cohort compared with 1 (1.5%) in the BLP, and 2 (3.1%) cases of recurrent HV in the ML cohort compared with 1 (1.5%) in the BLP. A reoperation involving the first ray was required in 3 (4.6%) ML patients and 5 (7.7%) BLP patients (P = .7178).
Complications and reoperations.

EHL extensor hallucis longus, MTP metatarsophalangeal, TMT tarsometatarsal.
Symptomatic hardware consequent to primary modified Lapidus or Lapiplasty fixation hardware.
Removal of primary fixation hardware (modified Lapidus crossing screws or Lapiplasty biplanar locking plates).
Discussion
This study of patients who underwent first TMTJ arthrodesis for HV correction with either the ML procedure with crossed-screw fixation at one institution or the BLP system at another institution found that use of the BLP system was associated with improved radiographic HV correction, as suggested by greater correction in the HVA and IMA. After adjusting for potential confounders and preoperative measurements, we found that the BLP system was associated with a mean 7.5° greater correction in HVA and 2.0° greater correction in IMA than the ML procedure. Correction of the TSP, a surrogate marker of rotational deformity, was not significantly different preoperatively or postoperatively between groups, nor were complication and reoperation rates.
This study has limitations. It is a retrospective review at risk of information and selection bias; we mitigated selection bias by reviewing consecutive patients who met inclusion criteria. In addition, heterogeneity exists between and within each cohort. Specifically, variations in the concomitant procedures performed—including lateral release, Akin osteotomy, and additional fixation—were potential confounding factors limiting comparison between cohorts. Elevation or shortening of the first ray was not measured in this study and could have had an impact on outcomes. In addition, some patients in the ML cohort received calcaneal autograft, whereas the patients in the BLP cohort received no supplemental bone grafting. Each institution may have had variability in radiographic technique, but this limitation was mitigated by the universal standard for orthogonal views and protocol for researcher evaluation with interrater reliability. This is also a multi-surgeon study without crossover in technique, which introduces bias from surgical performance. The postoperative protocol was different between cohorts, which may also have affected radiographic outcomes and complications. However, the BLP group showed an association with greater normalization of the IMA and HVA, and fewer wound healing complications, despite immediate weightbearing postoperatively. It is important to note the preoperative difference in the IMA between groups; however, we feel these cohorts remain comparable as there was no significant difference in HVA. Long-term follow-up is warranted for better evaluation of correction maintenance and HV recurrence rates. A final limitation of this study is the lack of PROMs. Evaluation of PROMs may help to determine whether or not differences in radiographic correction correlate with clinical improvement.
An evolved understanding of the triplanar deformity in HV and the contribution of hypermobility of the first ray has given rise to improved surgical techniques in HV deformity correction. The catalyst driving HV deformity remains controversial; contributing factors include coexisting equinus contracture, pes planus, metatarsus adductus, ligamentous laxity, and lesser toe deformities [18]. One well-researched factor thought to contribute to the progression of HV is hypermobility and pronation of the first ray, first described in 1935 [9,15,21,22,24]. Surgical correction techniques that neglect rotation result in recurrence rates of 30% to 75%, depending on the technique employed [3,10,17]. In addition, Conti et al [5] demonstrated an association between first metatarsal pronation correction with PROMs and recurrence rates in HV.
The original Lapidus technique consisted of a non-instrumented arthrodesis of the first TMTJ and the first intermetatarsal joint, simply sewing the joint capsules together [8,13]. When Lapidus introduced the procedure, the focus was only on a single plane of instability in the axial plane. Later, Clark and colleagues [4] described a modified technique with crossed screws without intermetatarsal fusion [4]. Over the past 2 decades, understanding of HV deformity has evolved to a new appreciation of the triplanar deformity, with involvement of the coronal plane [8]. Eventually, triplanar correction through first TMTJ arthrodesis was adopted and became an important focus in achieving adequate surgical correction. Both the BLP and ML procedures aim to address the three-dimensional, rotational component of the HV deformity by creating biomechanical stability of the first ray through a TMTJ arthrodesis. They differ, however, in the intraoperative system for deformity correction and final fixation. Given the increased cost of the BLP system, comparative studies are warranted to show a benefit compared with traditional techniques.
Willegger et al [26] conducted a meta-analysis of 29 studies including 1470 feet at an average of 28.5 months follow-up to determine the correction power and complications associated with first TMTJ arthrodesis for HV deformity. The authors concluded that first TMTJ arthrodesis provided better IMA correction in comparison with previously published meta-analysis data on proximal, diaphyseal, and distal metatarsal osteotomies. Of note, a subgroup analysis of corrective power indicated the highest degree of IMA normalization with a combined locking plate and screw fixation construct (12.41°) in comparison with screw fixation alone (9.12°). A total of 236 complications (16.05%) occurred, including nonunion (n = 59; 4.01%), HV recurrence (n = 33; 2.24%), and delayed union (n = 22; 1.49 %). Similarly, our results suggested greater normalization of the IMA as well as HVA with BLP, with similar complication rates. More recently, Do et al [8] published a systematic review of 45 studies, including 2344 feet, which measured the IMA, HVA, and TSP of patients undergoing the ML procedure, and reported an interquartile range of respective preoperative and postoperative values: IMA of 15.8° to 6.5°, HVA of 32.7° to 12.5°, and TSP of 5 to 2. Of note, this systematic review included only 2 studies using the BLP system; it reported complication rates of 4.4% for nonunion, 2.8% for hardware irritation, 2.0% for HV recurrence, 1.4% for hallux varus, and 1.3% for wound complications at 17.5 months. The most common causes of reoperation were painful hardware (2.7%), nonunion (1.5%), hallux varus (0.5%), and HV recurrence (0.6%). Our study’s complication results are comparable to these, but we report lower nonunion rates, with 1.5% (n = 1) in the BLP cohort and 0% in the ML cohort.
With regard to the BLP system, Dayton et al [7] conducted a comparison of prior and final postoperative correction of IMA, HVA, and TSP in 109 feet after triplanar TMTJ arthrodesis with BLP at a mean follow-up of 17.4 months. The mean changes in radiographic values preoperatively to postoperatively were −14.9° for HVA, −7.7° for IMA, and −2.6 for TSP, suggesting significant postoperative correction. They reported no significant complications or reoperations, with a 0% nonunion rate. Furthermore, Shah et al [20] evaluated 99 feet treated with the BLP system, finding an average HVA decrease from 31.34° to 15.05° and IMA decrease from 14.99° to 6.62° at final follow-up. The HV recurrence rate was 3.03% at an average of 5.4 months. Similarly, Ray et al evaluated 62 feet treated with the BLP system and early weightbearing for triplanar first TMTJ arthrodesis at 4 institutions. Significant radiographic improvements were noted in IMA (13.6° to 6.6°), HVA (24.2° to 9.7°), and TSP (5.0 to 1.9) from preoperative to final follow-up at 13.5 months [19]. They reported an HV recurrence rate of 3.2% (2/62 feet) and symptomatic nonunion rate of 1.6% (1/62 feet). Compared with these studies, we report a slightly higher degree of correction at a final follow-up, with an HVA of 4.0° (correction 29.0°) and IMA of 3.0° (correction 10.0°), with similarly low complication rates.
In our study, postoperative ML patients were non-weightbearing for 6 weeks; BLP patients were permitted to bear weight immediately. Crowell et al [6] performed a systematic review assessing the rate of nonunion with early weightbearing following first TMT arthrodesis. The authors included 8 studies (443 arthrodeses) with a minimum of 1-year follow-up permitting an early weightbearing protocol (≤2 weeks) to find a nonunion rate of 3.61% (n = 16). Fixation constructs included 2 crossed screws (n = 203, 46%), compression screw with plate (n = 147, 33%), 2 screws (n = 51, 12%), a mini-rail external fixation with or without a compression screw (n = 25, 5%), and an anatomic plate (n = 17, 4%). This was later supported by Ray et al [19], who included 62 feet from 4 institutions that were permitted immediate postoperative weightbearing with the BLP system and a subsequent 1.6% nonunion rate. The low nonunion rate reported with early weightbearing is important to consider as extended periods of immobilization and non-weightbearing may preclude certain patient populations from undergoing this procedure.
In conclusion, this retrospective multicenter study found that the use of the BLP system was associated with improved radiographic HV deformity correction, as suggested by greater normalization of the IMA and HVA, when compared with the ML technique. There were similar rates of complications and reoperations in the 2 groups. The clinical significance of these radiographic findings is unclear. Future research assessing more homogeneous cohorts, long-term and patient-reported outcomes, and cost-benefit analysis will be necessary to further compare techniques and fixation systems.
Supplemental Material
sj-docx-1-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-1-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-2-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-3-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-4-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-5-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-6-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316241288514 – Supplemental material for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison
Supplemental material, sj-docx-7-hss-10.1177_15563316241288514 for Radiographic and Clinical Outcomes of First Tarsometatarsal Joint Arthrodesis With a Biplanar Locking Plate System Versus the Modified Lapidus Technique With Crossed-Screw Fixation: A Retrospective Multicenter Comparison by Amanda N. Fletcher, Lindsey G. Droz, Robert Fuller, Lavan Rajan, Jiaqi Zhu, Mark E. Easley, James A. Nunley and Elizabeth A. Cody in HSS Journal®
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JAN reports a relationship with Treace Medical, the manufacturer of a product used in this study. MEE reports relationships with Paragon 28 and Treace Medical, the manufacturers of products used in this study, as well as Wolters Kluwer, Exactech, and Vilex. EAC reports relationships with Paragon 28, the manufacturer of a product used in this study, and Stryker. The other authors declared no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study by the institutional review boards at Hospital for Special Surgery (HSS; 2013-038) and Duke University Medical Center (Pro00107825).
Level of Evidence
Level III, retrospective cohort study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.