
Abstract
Background:
The quest for optimal approaches to treating tibial shaft fractures in orthopedic surgery remains a topic of debate.
Purpose:
We sought to compare the patellofemoral and radiological outcomes of 2 surgical techniques for treating tibial shaft fractures: the suprapatellar and extra-articular lateral parapatellar (ELP) approaches, both used in intramedullary tibial nailing in a semi-extended position.
Methodology:
This retrospective analysis examined 73 adult patients treated for tibial shaft fracture from January 2018 to December 2023, divided into 2 groups: 42 in the suprapatellar group and 31 in the ELP group. Evaluation metrics included radiographic outcomes, clinical results, and complication rates, focusing on anterior knee pain (measured by visual analog scale) and knee function (Kujala and Lysholm scores).
Results:
No significant differences were found in union rate, nail apex distance, reoperation rate, or malalignment between the 2 approaches. However, the ELP approach was associated with significantly better clinical outcomes, with higher Lysholm scores and reduced anterior knee pain. Additionally, the suprapatellar approach (SP) was associated with a higher incidence of painful hemarthrosis during hospitalization.
Conclusion:
While this retrospective comparison found both techniques to be effective in treating tibial shaft fractures, the ELP approach was associated with superior functional outcomes as assessed by higher Lysholm scores and Kujala scores, less anterior knee pain, and a lower risk of painful hemarthrosis compared to the SP approach. Further study is warranted.
Keywords
Introduction
Tibial shaft fractures are the most common type of long bone fractures, with an annual incidence rate of 16.9 per 100 000 [18]. The intramedullary nail has become the gold standard for treating these fractures, particularly for tibial diaphyseal injuries, due to its ability to provide stability and facilitate early weight-bearing. Over the years, surgical techniques and implants have evolved significantly, broadening the scope of the nailing technique to include proximal and distal metaphyseal fractures as well [3,10]. A notable advancement in this field is the adoption of the semi-extended position for nailing, which mitigates the tension exerted by the extensor mechanism and facilitates improved management of the characteristic apex anterior deformity observed in proximal tibia fractures [17,21,23].
The semi-extended tibial nailing technique has been refined through various approaches. In 1996, Tornetta et al [30] introduced the medial parapatellar approach, which facilitated nail placement in a semi-extended position while allowing for lateral patellar subluxation. Subsequently, the suprapatellar approach (SP), described by Cole in 2006 [4,27], emerged as a novel technique involving a small incision just proximal to the superior pole of the patella and employing specialized instruments and protectors to prevent damage to the patellofemoral articular cartilage during canal reaming and nail insertion. More recently, in 2010, Kubiak et al [14] proposed the extra-articular lateral parapatellar (ELP) approach, which enables tibial nailing with medial patella subluxation and avoids direct entry into the joint.
The ELP approach has demonstrated significant advantages in enhancing knee function and reducing patellofemoral pain compared to the SP approach. Characterized by its minimal invasiveness to the knee’s structural integrity and patellar tendon, the ELP method involves an incision based on patellar laxity, followed by lateral or medial subluxation of the patella while preserving the synovial layer [6]. The semi-extended position, integral to the ELP approach, offers benefits such as reduced tension on the extensor mechanism and improved imaging for fracture reduction and nail placement [8,28]. Literature supports these advantages, with the ELP approach associated with improved maintenance of fracture reduction and decreased intra-articular reaming debris [24]. Comparative studies, though limited [2,22,25,33,34], generally support the equivalence of the SP and ELP approaches in fracture reduction and nail positioning. However, the ELP approach is associated with a significantly lower incidence of anterior knee pain, a common complication of tibial nailing [13]. Furthermore, the SP approach has been linked to higher rates of iatrogenic chondral damage, raising concerns about long-term patellofemoral complications [6,9,15,35].
Despite the growing interest in minimally invasive surgical techniques, there remains a gap in the literature comparing tibial nailing approaches in a semi-extended position, particularly concerning patellofemoral outcomes. We aimed to address this gap by comparing the clinical and radiographic outcomes of the SP and ELP approaches for tibial shaft fracture treatment, with a focus on evaluating knee functionality and patellofemoral pain to provide insight into the optimal surgical approach for managing these fractures.
Methods
This study was designed as a retrospective analysis and was conducted at a high-volume trauma center and university hospital. Adhering to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [31], this research spanned from January 2018 to December 2023. During this period, data were systematically collected from the institutional database on patients who underwent intramedullary tibia nailing, ensuring a minimum follow-up duration of 24 months. Written informed consent was obtained from all participants, allowing for the use of their personal data, clinical records, and follow-up information in this study.
Eligibility for this study was determined based on specific inclusion and exclusion criteria. Participants were required to be over 18 years of age and diagnosed with open and closed tibial shaft fractures classified as 42 type A, B, and C according to the Orthopedic Trauma Association (OTA/AO) classification, who subsequently underwent tibia nailing [20]. Exclusion criteria included patients with an initial diagnosis of non-union, failed tibia fractures, pathological fractures, skeletal immaturity, and those with a history of knee surgery.
After application of selection criteria with a timeframe from 2018 to 2022, a total of 107 patients with tibial shaft fractures were initially screened for eligibility in this study. After a selection process, which involved excluding 7 patients due to incomplete medical records and disqualifying another 27 for not meeting the inclusion criteria, 73 patients were ultimately included for clinical and radiographic assessment. Notably, throughout the study, there was a 100% retention rate, with no patients declining participation or being lost at the final follow-up (Fig. 1).
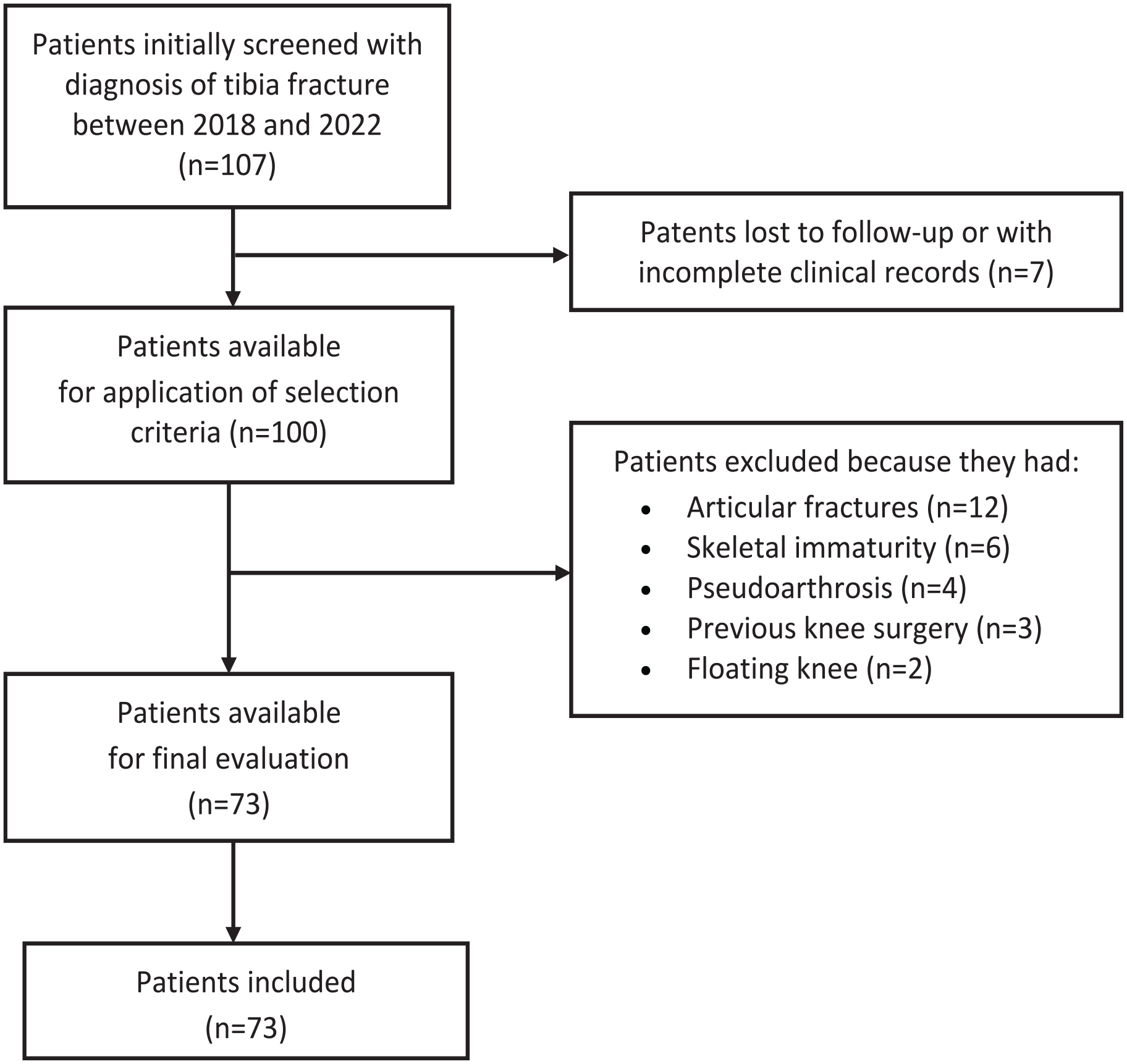
Flowchart for patient selection.
The study population was divided based on the surgical approach for tibial nailing: 42 patients (57.5%) underwent surgery using the SP approach, while the remaining 31 patients (42.5%) were treated using the ELP approach (Fig. 2). The mean follow-up duration for the cohort was 38.0 ± 14.0 months, ranging from 24 to 72 months (Table 1). Importantly, the demographic and baseline clinical characteristics were comparable across both groups, ensuring a balanced comparison.
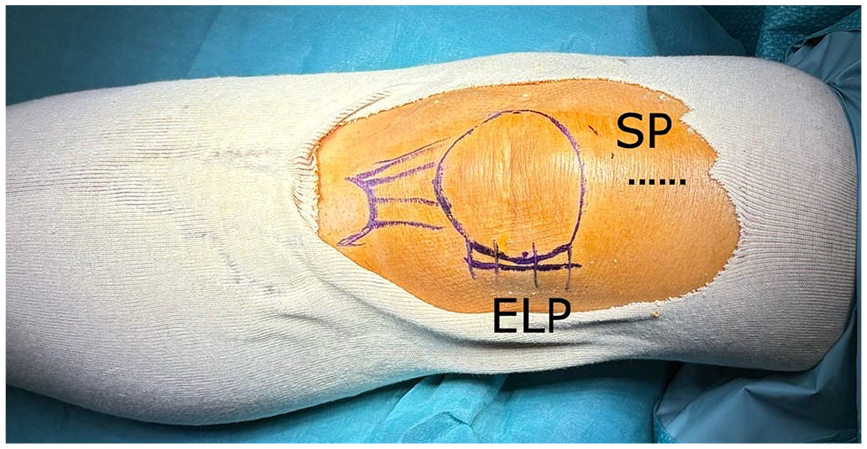
Schematic representation of different surgical approaches to perform semi-extended tibia nail. Image of a left knee in a semi-extended position with the representation of the skin incisions: the extra-articular lateral parapatellar (ELP) approach, and the suprapatellar (SP) approach.
Demographic and clinical features of patients.
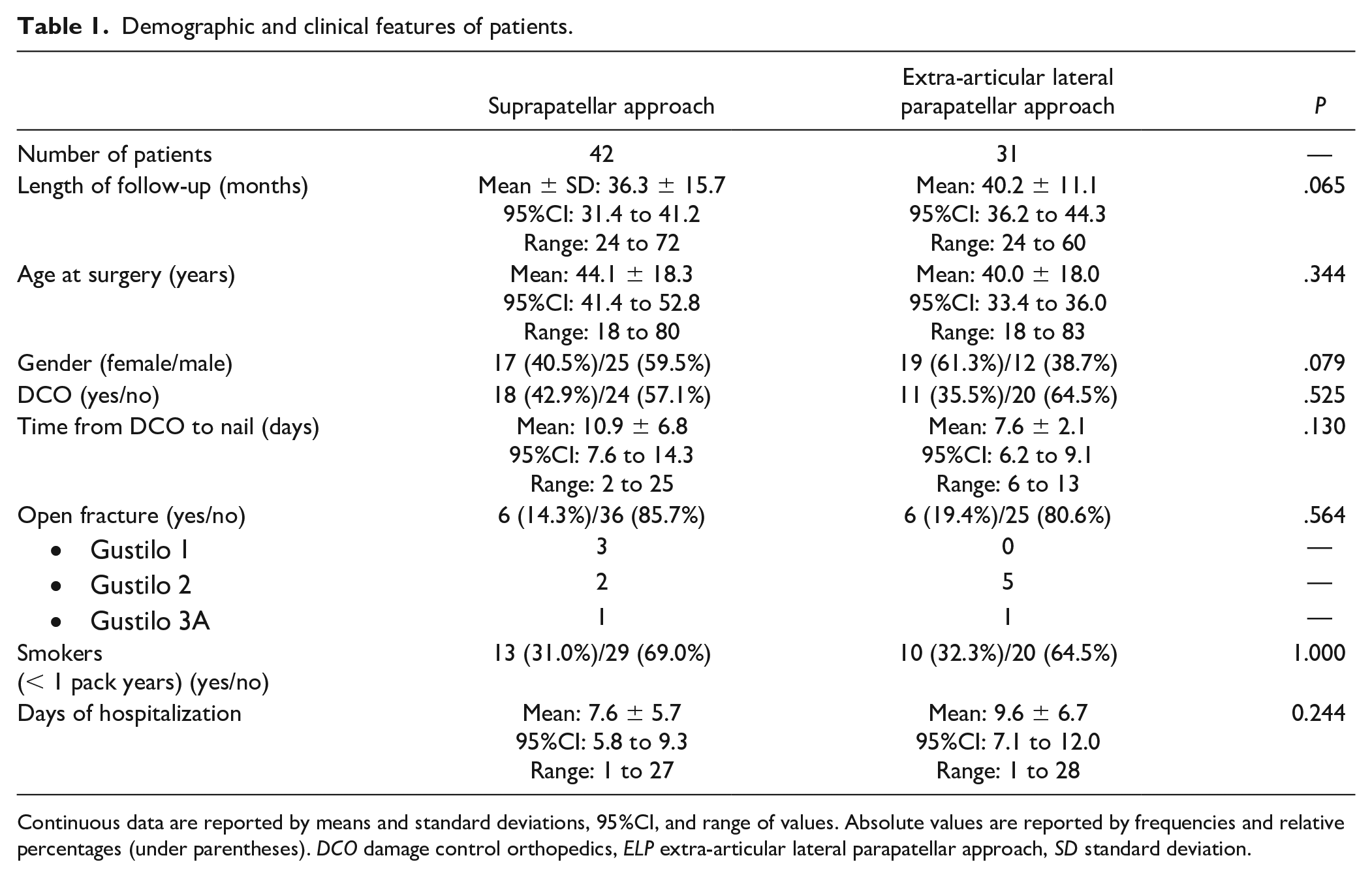
Continuous data are reported by means and standard deviations, 95%CI, and range of values. Absolute values are reported by frequencies and relative percentages (under parentheses). DCO damage control orthopedics, ELP extra-articular lateral parapatellar approach, SD standard deviation.
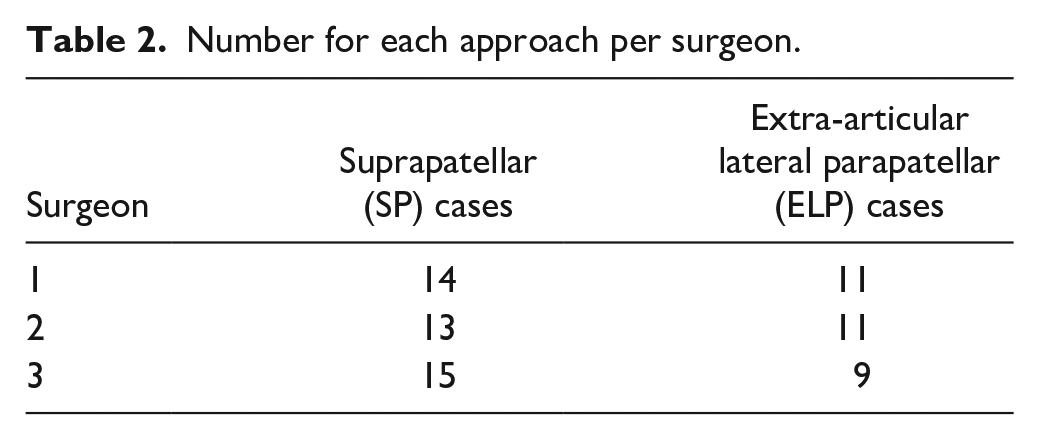
The surgical technique was tailored according to the surgeon’s preference, with procedures performed by 3 expert surgeons, each performing over 100 procedures per year (Table 2). It is assumed that all 3 surgeons possess equivalent surgical skills, ensuring comparability of outcomes across the approaches. The operating theater setup was standardized for both techniques utilizing spinal anesthesia, a supine position with a semi-extended knee, without a tourniquet, and under fluoroscopy guidance. The SP and the ELP approaches were employed, with the same tibia nail used for all cases (ZNN, Zimmer; Warsaw, IN).
Number for each approach per surgeon.
The operating room setup was the same for both techniques, with the procedure performed under spinal anesthesia, in a supine position with a semi-extended knee (from 20° to 30° of flexion), without a tourniquet, and under fluoroscopy guidance.
The SP approach was performed through a 2- to 3-cm longitudinal incision over the superior border of the patella. The quadriceps tendon was longitudinally incised in line with its fiber, and nailing was completed with dedicated instruments and a cannula for the SP nailing inserted into the patellofemoral joint. The ELP approach was performed through a 3-cm incision over the lateral aspect of the patella. The superficial and deep layers of the iliopatellar band [29] were longitudinally incised, with careful preservation of the synovial layer to avoid violation of the knee joint. The superolateral genicular artery was cauterized to avoid bleeding and impaired visualization. The nailing technique was then completed with medial patellar subluxation and a soft tissue protector to avoid knee capsule damage, as originally described by Kubiak et al [14]. The tibia nail was the same in all cases regardless of the preferred approach.
Data collected included demographics, length of stay, injury side, fracture pattern, soft tissue damage, surgical approach, and postoperative nail-to-apex distance. Open fractures were classified according to the Gustilo and Anderson classification [12]. Post-operative hemarthrosis was measured and graded according to Coupens and Yates scores [7], and grade 4 was recorded as painful hemarthrosis. Clinical and radiographic outcomes assessed included union rate, complication rate, and need for reintervention, with bone union and non-union defined by specific criteria [1,11,32]. Subjective functional outcomes and residual knee pain were measured using the Kujala score [16], the Lysholm score [19], and the visual analog scale (VAS) [5].
Radiographs were evaluated by 2 independent orthopedic surgery residents, blinded to approach and patient demographic information. Interobserver agreement for X-ray assessment was calculated to ensure reliability. Disagreements were solved with the evaluation of a third observer (senior author) to confirm the X-ray assessment.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics version 26.0. A post-hoc calculation was performed considering the Kujala score as the primary outcome measure for continuous endpoint and 2 independent sample studies. The resulting post-hoc power on the 73 patients (42 in the SP group and 31 in the ELP group) with an α value of 0.05 was 97.3%, demonstrating an adequate sample size.
Categorical variables were expressed as the absolute number of cases and/or percentage. The Shapiro-Wilk test was used to identify normally distributed parameters. Differences between means were calculated with independent samples t test for continuous variables and with the Mann-Whitney U test if not normally distributed. Differences between categorical variables were calculated using Fisher’s exact test. Interobserver reliability for radiologic assessment was evaluated using Cohen’s κ coefficient. A P value of < .05 was considered statistically significant.
Primary outcomes were assessed in terms of functional outcomes and pain evaluation. The Kujala score, which evaluates patellofemoral function, and the Lysholm score, which measures overall knee function, were analyzed using the independent samples t test for normally distributed data. Differences between means for these scores were expressed as difference (MD) with associated P values to evaluate statistical significance.
Secondary outcomes included complication rates, such as painful hemarthrosis, which were compared using Fisher’s exact test, with odds ratio (OR) and 95% confidence intervals calculated to quantify the relative risk. Secondary outcomes also included radiographic findings, which were assessed using variables such as union rate, nail apex distance, reoperation rate, and malalignment. The analysis of variance (ANOVA) was used to compare means of continuous normally distributed variables in 2 independent comparison groups.
Variables achieving the P value < .1 in univariate analysis were examined using multivariate linear regression analysis. A model P value of <.05 was considered statistically significant.
Results
There were no significant differences observed between groups in terms of union rate, nail apex distance, reoperation rate, and malalignment, suggesting comparable surgical success and alignment correction. Furthermore, the interobserver reliability for radiographic fracture classification and nail apex distance measurements was highly relevant, with values of .92 and .87, respectively, demonstrating excellent consistency between observers.
A detailed clinical evaluation suggested a significant advantage for patients who underwent the ELP approach in terms of functional outcomes and pain. Specifically, the Lysholm (MD = +16.3 points; P = .001) and Kujala scores (MD = +15.9 points; P < .001), which measure knee function and patellofemoral disorders, respectively, were significantly higher in the ELP group and reached the minimal clinical important difference (MCID) of 11.1 for the Lysholm and 9.1 for the Kujala scores [26]. Additionally, the ELP patients reported significantly less knee pain (MD = −1.4 VAS points; P < .001) (Table 3).
Clinical and radiographic outcomes at final follow-up.
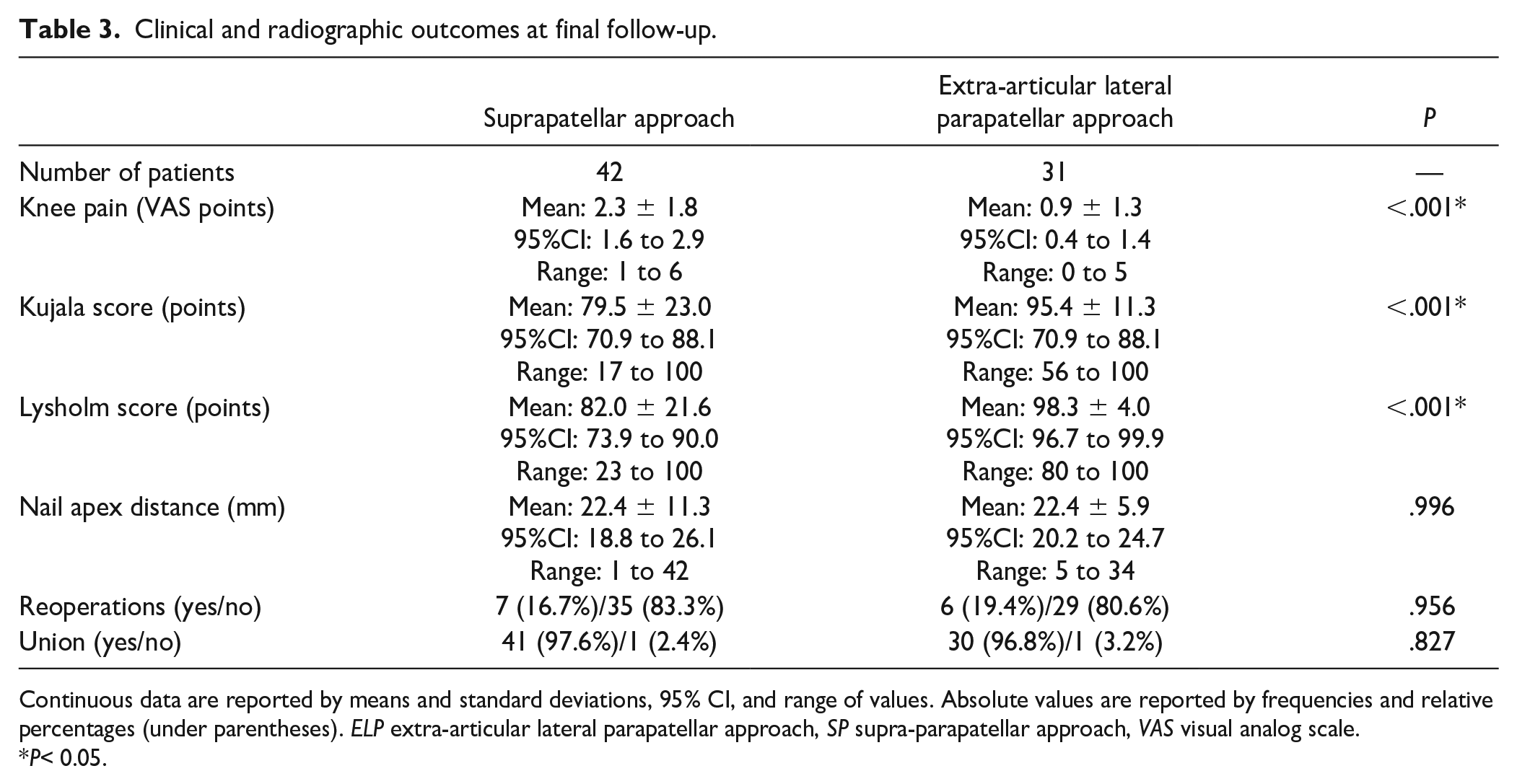
Continuous data are reported by means and standard deviations, 95% CI, and range of values. Absolute values are reported by frequencies and relative percentages (under parentheses). ELP extra-articular lateral parapatellar approach, SP supra-parapatellar approach, VAS visual analog scale.
P< 0.05.
The overall complication rate was similar between the 2 groups, with one notable exception. The SP group had a significantly higher rate of painful hemarthrosis (OR = 4.2; 95%CI: 1.1 to 16.3; P = .029) during hospitalization, suggesting a potential area for improvement in managing postoperative care for these patients (Table 4).
Complications after surgical treatment of tibia shaft fracture, by surgical technique.
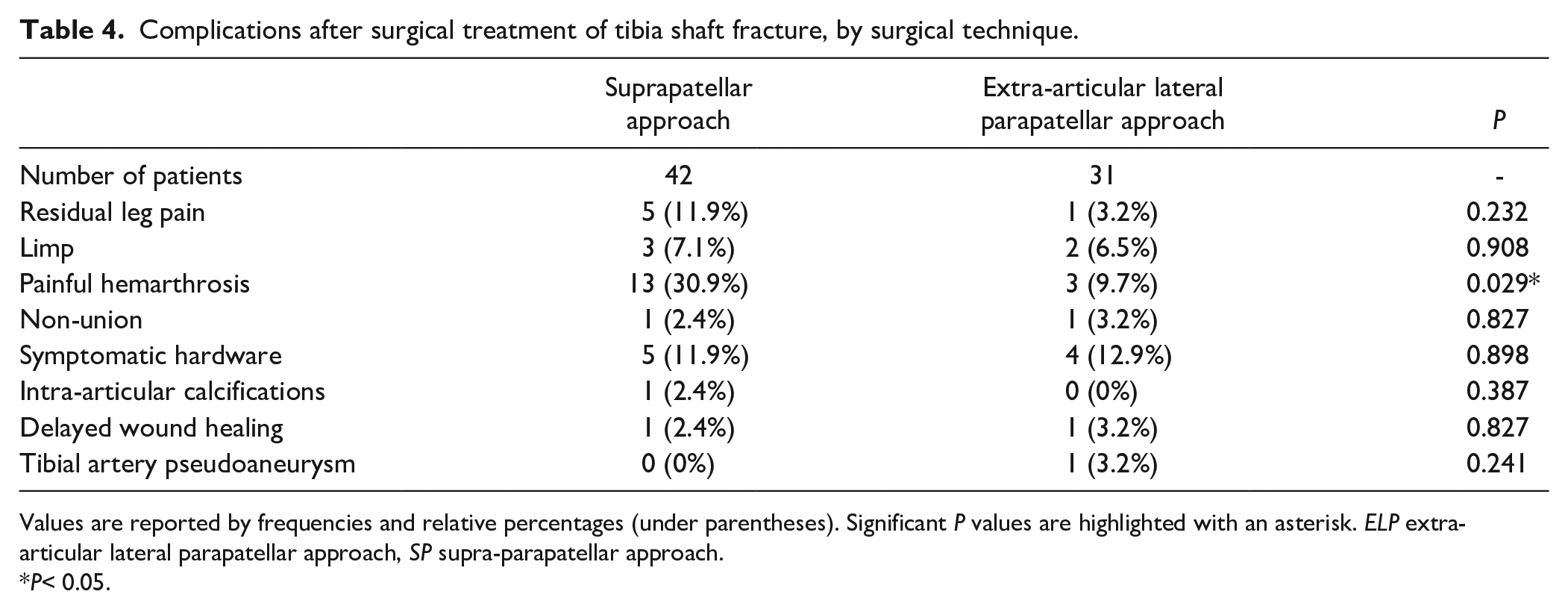
Values are reported by frequencies and relative percentages (under parentheses). Significant P values are highlighted with an asterisk. ELP extra-articular lateral parapatellar approach, SP supra-parapatellar approach.
P< 0.05.
Univariate analysis showed that age at surgery, the type of approach, the presence of an open fracture, and the presence of comorbidities had a significant impact on Lysholm score (P < .05), while only age at surgery and the type of approach had a significant impact on Kujala score (P = .004) (Table 5). Multivariate analysis confirmed that only lower age at surgery and the ELP approach were independently associated with a better Lysholm score (P < .001). Furthermore, a lower age at surgery and the ELP approach were also independently associated with a better Kujala score (P < .001) (Table 6). These findings suggest that age and surgical approach may be independent factors potentially affecting patient recovery, while open fractures, comorbidities, and complications had no statistically significant effect in this multivariable model.
Univariate analysis of the impact of different outcomes on the primary outcomes.
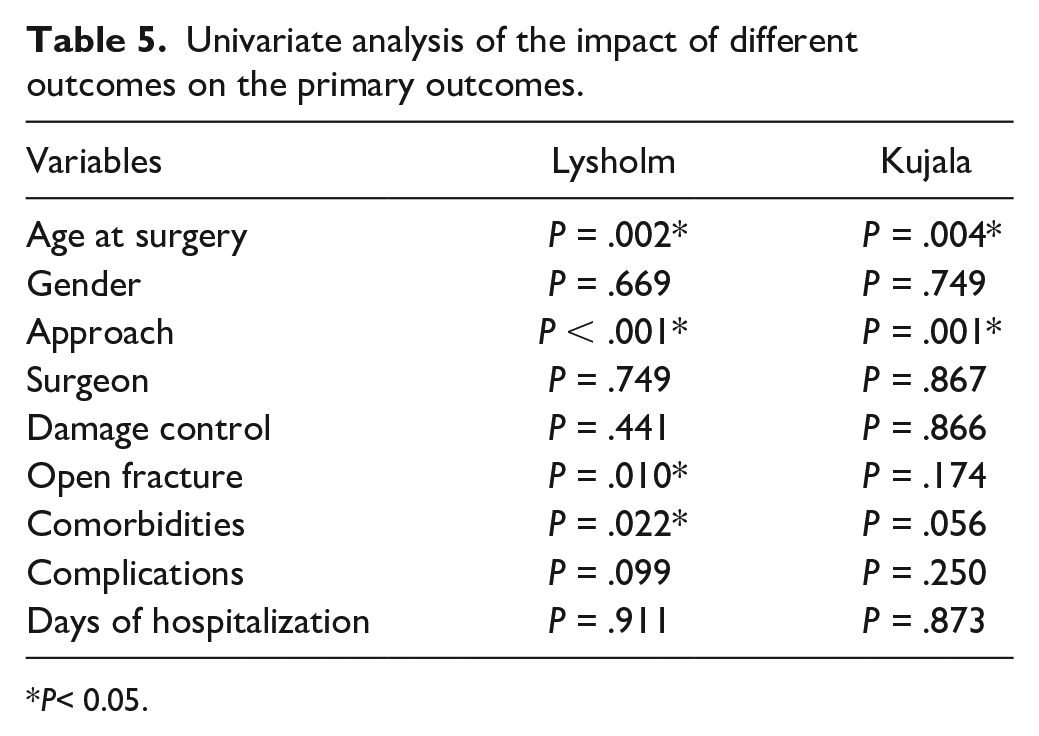
P< 0.05.
Multivariate analysis model of independent variables influencing the primary outcomes.
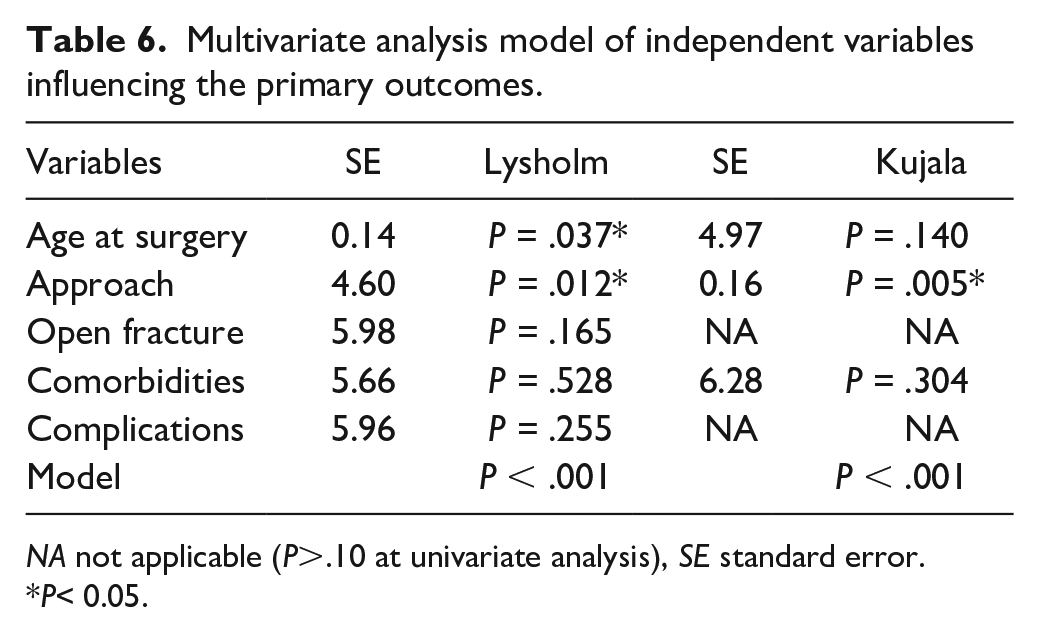
NA not applicable (P>.10 at univariate analysis), SE standard error.
P< 0.05.
Discussion
This retrospective study aimed to compare clinical and radiographic outcomes of 2 surgical techniques for intramedullary tibial nailing performed in a semi-extended position: the SP and the ELP approaches. We evaluated functional outcomes, as measured by the Lysholm and Kujala scores, and anterior knee pain, as assessed by the VAS. We found that the ELP approach yielded superior functional outcomes, with significantly higher Lysholm and Kujala scores, as well as reduced anterior knee pain, compared to the SP approach. Both techniques, however, showed comparable performance in terms of union rate, nail apex distance, reoperation rate, and malalignment. Notably, the SP approach was associated with a significantly higher incidence of painful hemarthrosis during hospitalization. These findings suggest the potential advantages of the ELP approach in minimizing postoperative complications and improving knee functionality. Our findings of a lower incidence of postoperative hemarthrosis and the integrity of the knee joint capsule following the ELP approach add another layer of evidence suggesting the ELP approach may be superior in minimizing complications and enhancing postoperative recovery (Fig. 3).
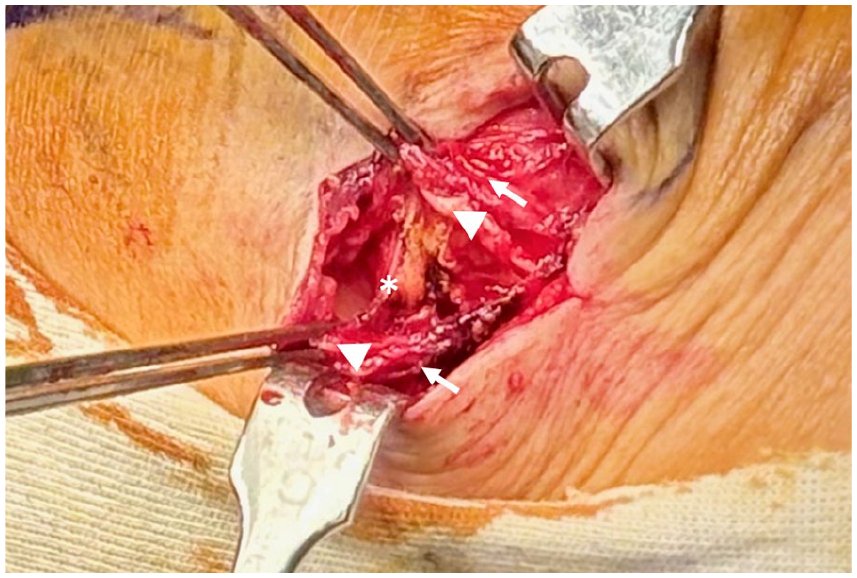
Intra-operative view of extra-articular lateral parapatellar approach showing the superficial (with arrows) and the deep layer (white triangles) of the iliopatellar band longitudinally incised to identify of the lateral genicular artery (asterisk). Synovial layer is preserved to avoid intra-articular penetration.
Despite these promising findings, the study is not without limitations. The retrospective design, non-randomized nature, and variability in surgeon experience may introduce biases that could affect the reliability of the findings. Additionally, the reliance on functional scores without corroborating imaging data to assess cartilage damage represents a gap in the comprehensive evaluation of the 2 approaches. Nevertheless, its strengths, including its comparative design, blinded outcome assessment, and robust sample size, provide a foundation for future research. The extended follow-up period and minimal drop-out rates further enhance the reliability of the study’s conclusions, making a compelling case for the preferential use of the ELP approach in tibial nailing procedures.
In conclusion, this retrospective comparison found the ELP approach to tibial nailing in a semi-extended position was associated with reduced postoperative knee pain and lower risk of patellofemoral complications. The findings contribute valuable insights into the ongoing debate over the optimal surgical approach for tibial nailing, with implications for both clinical practice and future research. The comparative analysis reveals no significant difference between the 2 approaches in terms of union rate, nail apex distance, reoperation rate, and alignment, indicating that the choice of approach can be tailored to the surgeon’s expertise without compromising the surgical outcome. However, the results highlight a strong association between the ELP approach and improved functional outcomes.
Supplemental Material
sj-docx-1-hss-10.1177_15563316251326505 – Supplemental material for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach
Supplemental material, sj-docx-1-hss-10.1177_15563316251326505 for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach by Mattia Alessio-Mazzola, MD, Valerio Alpi, MD, Elena Ghezzi, MD, Giacomo Placella, MD and Vincenzo Salini, MD in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316251326505 – Supplemental material for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach
Supplemental material, sj-docx-2-hss-10.1177_15563316251326505 for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach by Mattia Alessio-Mazzola, MD, Valerio Alpi, MD, Elena Ghezzi, MD, Giacomo Placella, MD and Vincenzo Salini, MD in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316251326505 – Supplemental material for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach
Supplemental material, sj-docx-3-hss-10.1177_15563316251326505 for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach by Mattia Alessio-Mazzola, MD, Valerio Alpi, MD, Elena Ghezzi, MD, Giacomo Placella, MD and Vincenzo Salini, MD in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316251326505 – Supplemental material for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach
Supplemental material, sj-docx-4-hss-10.1177_15563316251326505 for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach by Mattia Alessio-Mazzola, MD, Valerio Alpi, MD, Elena Ghezzi, MD, Giacomo Placella, MD and Vincenzo Salini, MD in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316251326505 – Supplemental material for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach
Supplemental material, sj-docx-5-hss-10.1177_15563316251326505 for A Retrospective Study With 2-Year Follow-up Comparing Semi-Extended Tibia Nailing Techniques: The Suprapatellar Versus the Extra-Articular Lateral Parapatellar Approach by Mattia Alessio-Mazzola, MD, Valerio Alpi, MD, Elena Ghezzi, MD, Giacomo Placella, MD and Vincenzo Salini, MD in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Informed Consent
Informed consent was obtained from all patients included in this study.
Level of Evidence
Level III: Retrospective Therapeutic Study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.