
Abstract
Background:
Basicervical (BC) hip fractures represent a unique proximal femur fracture pattern for which the optimal treatment approach remains uncertain.
Purpose:
We sought to evaluate demographic, perioperative, and outcome differences among patients with BC (31B3), intertrochanteric (IT; 31A1.2), and valgus femoral neck (VFN; 31B1.1) fractures treated with internal fixation.
Methods:
We conducted a retrospective review using prospectively collected data from October 2014 to March 2025 from a hip fracture database comprising 2 urban trauma centers. Patients with AO/OTA-classified 31B3, 31A1.2, or 31B1.1 fractures treated with non-arthroplasty fixation were included. Demographics, comorbidities, fracture characteristics, surgical constructs, and short- and long-term outcomes were compared. Multivariate regressions adjusted for baseline health and procedure type.
Results:
Of the 875 patients who met inclusion criteria, 122 had BC fractures, 523 had IT fractures, and 230 had VFN fractures. Patients with BC fractures were significantly younger than those with IT fractures; they had higher American Society of Anaesthesiologist scores and a greater proportion of household ambulators compared to those with VFN fractures, but were otherwise similar in comorbidity status. The BC cohort had significantly more minor in-hospital complications compared to the VFN cohort, even after multivariate adjustment. No significant differences were observed in 30-day mortality or major complications. Long-term outcomes were comparable across all groups. No significant differences in short- or long-term outcomes were observed across surgical constructs within the BC cohort.
Conclusion:
Despite differing in baseline health status and surgical fixation strategies, BC fractures demonstrated comparable long-term outcomes to IT and VFN fractures. However, higher rates of minor complications in the BC group, even after adjustment, highlight a potentially greater perioperative risk. These findings suggest that while fixation may be effective long-term, further research is warranted to optimize acute management strategies for this anatomically and clinically distinct fracture pattern.
Level of Evidence:
Level IV: Prognostic retrospective study
Introduction
Basicervical (BC) hip fractures are a rare subtype of proximal femur fractures, with a reported incidence of 1.8% to 4%.1-3 A recent systematic review by Yoo et al found that consensus on BC hip fractures is lacking, with wide variation in fracture definitions, healing timelines, ambulation protocols, and reported failure rates. 4 This uncertainty extends to management approaches. A review by Yoon et al found no difference in outcomes between dynamic hip screws (DHS) and cephalomedullary nailing (CMN), 5 while Gomez-Vallejo et al found success with percutaneous compression plates. 2 Yet, results remain inconsistent—hemiarthroplasty, cannulated screws, fixed-angle device, CMN, and DHS have all been reported as viable constructs.1,6-9
Despite high complication rates and a lack of management consensus, few studies compare BC fractures to other proximal femur fracture types. 10 This gap makes it difficult to determine whether BC fractures represent a distinct clinical entity or if they resemble other fracture subtypes. To address this uncertainty, we set out to compare BC (31B3) fractures to intertrochanteric (IT; 31A1.2) and valgus femoral neck (VFN; 31B1.1) fractures with respect to patient demographics, perioperative treatment patterns, short-term outcomes, and long-term recovery. (During the preparation of this work, we used ChatGPT [OpenAI] to improve the clarity and grammatical structure of the manuscript. After using this tool, we reviewed and edited the content as needed.)
Methods
We used an IRB-approved retrospective database of prospectively tracked hip fracture patients from October 2014 to March 2025. All patients were treated at 1 of 2 urban trauma hospitals that operate under a standardized algorithmic approach. 11 The dataset was queried for patients who suffered AO/OTA type 31B3, 31A1.2, or 31B1.1 fracture classifications and were treated with non-arthroplasty fixation. 12 Baseline patient data extracted included age, sex, race, body mass index (BMI), Glasgow coma scale (GCS), age-unadjusted Charlson comorbidity index (CCI), pre-injury ambulatory status and assistive device usage, American Society of Anaesthesiologist (ASA) score, and the Score for Trauma Triage in the Geriatric and Middle Aged (STTGMA). 13 STTGMA is a validated risk tool that has been used to predict inpatient mortality, transfusion requirements, readmissions, 1-year postoperative quality of life, and 1-year mortality. 14 The score is calculated using a regression model that incorporates high or low energy mechanisms, age, GCS, CCI, ambulatory status, and the Abbreviated Injury Scale scores for the head and neck, the chest, and the extremities. Although originally developed as a 0.00 to 1.00 estimate of inpatient mortality risk, the score is commonly interpreted as a continuous measure of overall physiologic vulnerability following orthopedic trauma. Injury and acute-treatment factors used included AO/OTA classification, energy of injury mechanism (high or low), and surgical fixation construct. Short-term outcomes were length of stay, in-hospital complications, 30- or 90-day readmissions, and 30-day mortality. Minor in-hospital complications included deep vein thrombosis, urinary tract infection, anemia, and decubitus ulcer, among other less frequent complications. Major complications included sepsis, myocardial infarction, pulmonary embolism, pneumonia, stroke, major wound dehiscence, major blood loss, and organ failure. Long-term outcomes were radiographic healing, return to baseline assistive device, and need for reoperation. Radiographic healing was classified by the treating surgeon and was based on either effacement of the fracture line with maintenance of hardware, presence of bridging callus on 3 cortices, or trabecular consolidation on a follow-up radiograph. Return to baseline assistive device use was determined by comparing the baseline device documented at the time of injury by the treating team with the device recorded by the attending surgeon at the most recent follow-up visit.
There were 875 patients who met inclusion criteria for initial analysis. Patients were treated by specific faculty in accordance with the on-call schedule. Patients were classified in 3 groups: BC (31B3), IT (31A1.2), and VFN (31B1.1). All fractures were classified by the attending surgeon who operated on the patient. All patients were included in baseline/demographic analysis, injury/treatment analysis, and short-term outcome analysis. Short-term outcomes were defined as events occurring during the index hospitalization, readmissions within 90 days, and mortality within 30 days. Only patients who had a minimum of 6 months of follow-up with imaging were included in the long-term analysis of healing and function. Long-term follow-up was recorded based on the most recent clinic visit and ranged from 6 to 34 months.
The BC cohort was then scrutinized further to compare short- and long-term outcomes among different surgical constructs. Again, all BC patients were included in short-term analysis, and only those who had 6-month follow-up were included in long-term comparisons.
Statistical Analysis
Two-way analysis of variance (ANOVA) was used to compare continuous variables among classification groups. Results were reported as mean ± standard deviation (SD). Categorical variables were analyzed using χ2 analyses with standardized adjusted residuals. Following univariate analyses of all baseline and outcome variables, multivariate regressions were performed on all significant correlations to verify their independence from common confounds. Continuous variables were analyzed with linear regression and categorical variables with binary logistic regression. All regressions included STTGMA and procedure type as covariates to adjust for these possible confounds. The significance level was set at 0.05. SPSS software was used for all analyses (Version 28; IBM Corp., Armonk, NY, USA). We structured the manuscript using the STROBE checklist. We used ChatGPT (OpenAI) to improve the clarity and grammatical structure of the manuscript and reviewed and edited the content as needed.
Results
In terms of demographic and baseline health variables, significant differences were identified in age, sex, BMI, ASA, assistive device usage, and ambulatory status. The BC and VFN cohorts were significantly younger than the IT cohort (Table 1). The IT group had significantly more men, a higher BMI, and a higher rate of assistive device use compared to the VFN group. The BC cohort was not different from either IT or VFN in any of these variables. Both BC and IT cohorts had a significantly higher ASA compared to VFN. The BC cohort also had a significantly higher proportion of household ambulators compared to VFN, with the opposite trend for community ambulators. No differences were found in any of the cohorts regarding race, GCS, CCI, and STTGMA score. In addition, no differences were determined in the mechanistic energy of injury.
Demographic and Baseline Health Comparisons.
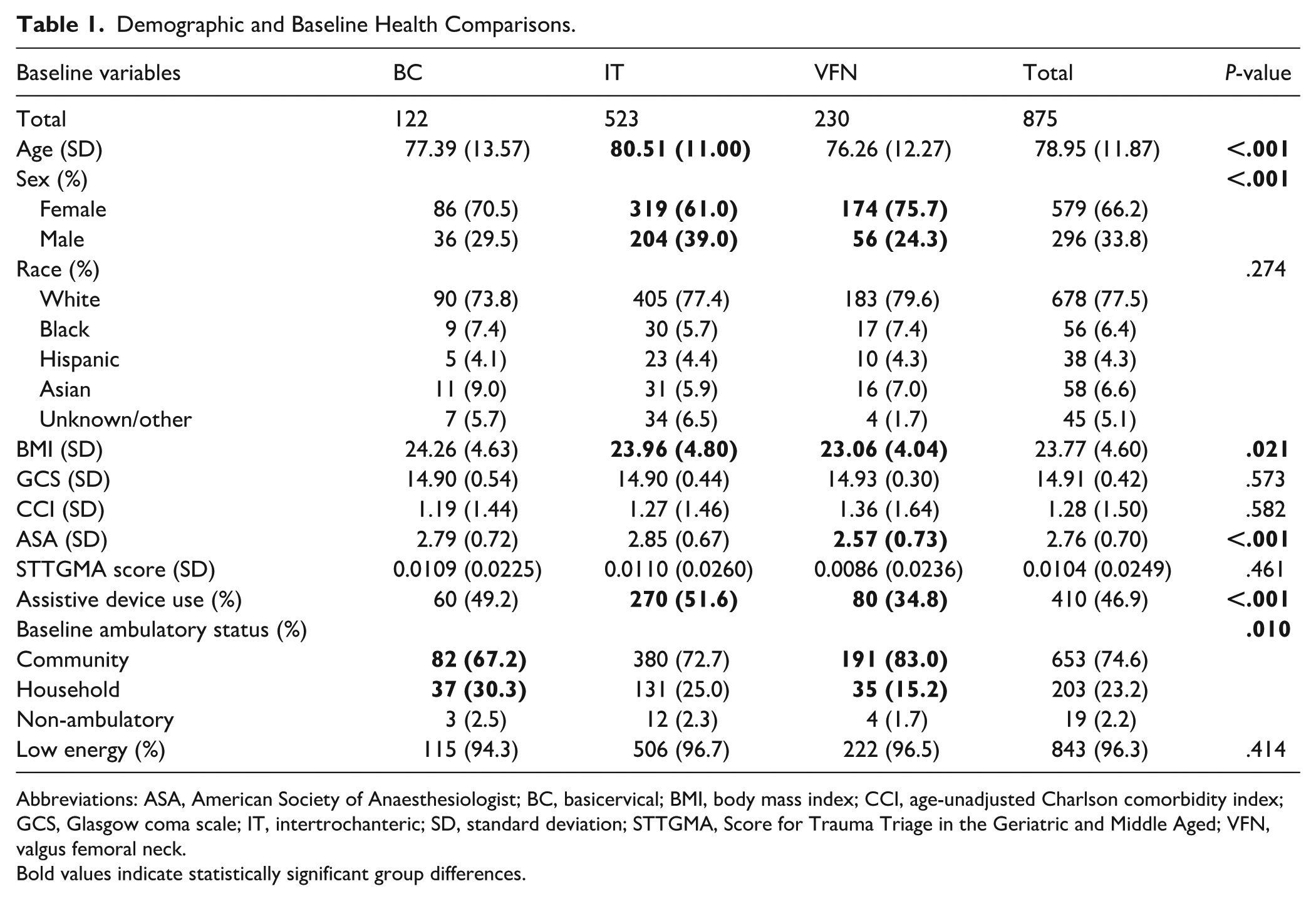
Abbreviations: ASA, American Society of Anaesthesiologist; BC, basicervical; BMI, body mass index; CCI, age-unadjusted Charlson comorbidity index; GCS, Glasgow coma scale; IT, intertrochanteric; SD, standard deviation; STTGMA, Score for Trauma Triage in the Geriatric and Middle Aged; VFN, valgus femoral neck.
Bold values indicate statistically significant group differences.
Regarding surgical constructs, the BC group was more commonly fixed with plates and screws than others (BC: 29.5%, IT: 6.7%, VFN: 1.3%; Table 2). IT had significantly more CMNs compared to both BC and VFN (BC: 69.7%, IT: 93.1%, VFN: 9.6%). VFN had significantly more closed reduction percutaneous pinnings compared to the other cohorts (BC: 0.8%, IT: 0.2%, VFN: 89.1%).
Surgical Constructs Utilized Among Classification Cohorts.
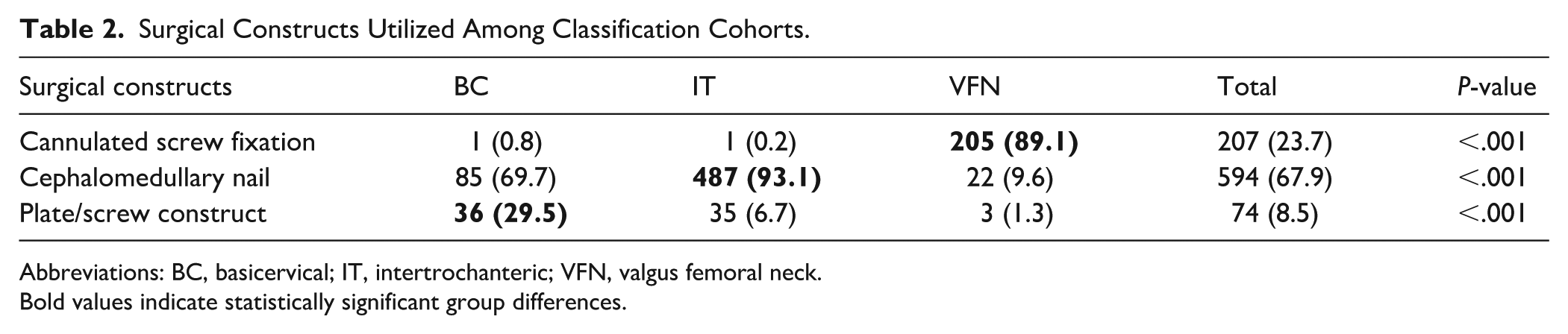
Abbreviations: BC, basicervical; IT, intertrochanteric; VFN, valgus femoral neck.
Bold values indicate statistically significant group differences.
In univariate short-term outcome analyses, IT had a significantly longer length of stay compared to VFN, while the BC cohort demonstrated no difference (BC: 6.47 ± 4.26, IT: 6.20 ± 3.87, VFN: 5.34 ± 5.86; Table 3). Both BC and IT cohorts had a significantly higher frequency of minor in-hospital complications compared to VFN (BC: 37.7%, IT: 31.7%, VFN: 20.4%). The BC and IT cohorts also had a significantly higher proportion of 90-day readmissions compared to the VFN group (BC: 14.8%, IT: 11.9%, VFN: 5.7%). All groups were similar in terms of major in-hospital complications, 30-day readmission, and 30-day mortality. In multivariate linear regression with STTGMA and surgical construct as covariates, length of stay was no longer significantly different among fracture type cohorts (P = .089). In binary logistic regression, the BC group was still significantly more likely to experience a minor complication compared to VFN (P = .049). Regression with 90-day readmission demonstrated no significance (P = .236). Moreover, fixation construct type within the BC cohort was not associated with differences in short-term outcomes (Table 4).
Short-Term Outcomes Among Classification Cohorts.
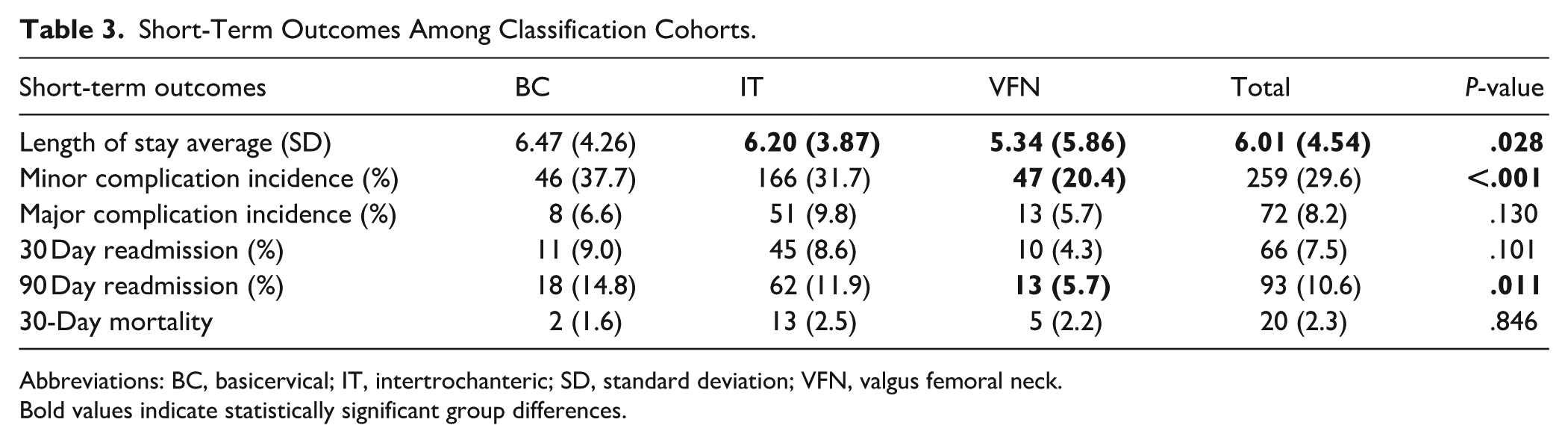
Abbreviations: BC, basicervical; IT, intertrochanteric; SD, standard deviation; VFN, valgus femoral neck.
Bold values indicate statistically significant group differences.
Comparison of outcomes based on surgical constructs among the basicervical cohort (n = 122).
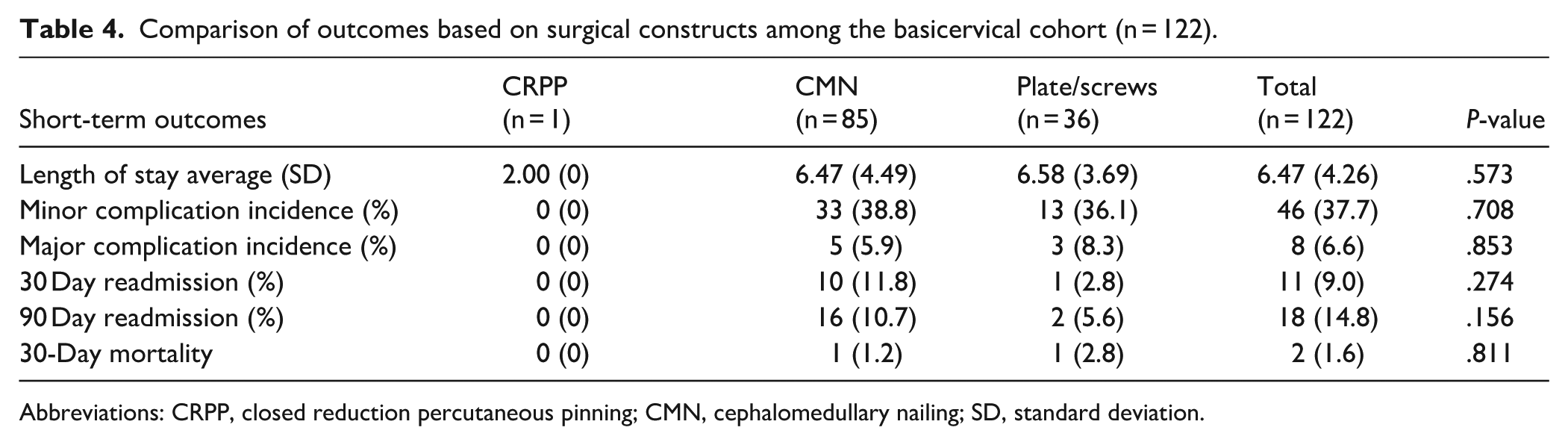
Abbreviations: CRPP, closed reduction percutaneous pinning; CMN, cephalomedullary nailing; SD, standard deviation.
Only 199 patients (22.74%) of the original cohort had 6-month radiographic follow-up. No differences were found in radiographic healing, return to baseline assistive device usage, and reoperation rates among the 3 groups (Table 5). Within the BC cohort, although the plate/screws group demonstrated a lower rate of healing and a higher rate of reoperation, these comparisons were not significant (Table 6).
Long-Term Outcomes Among Cohorts.
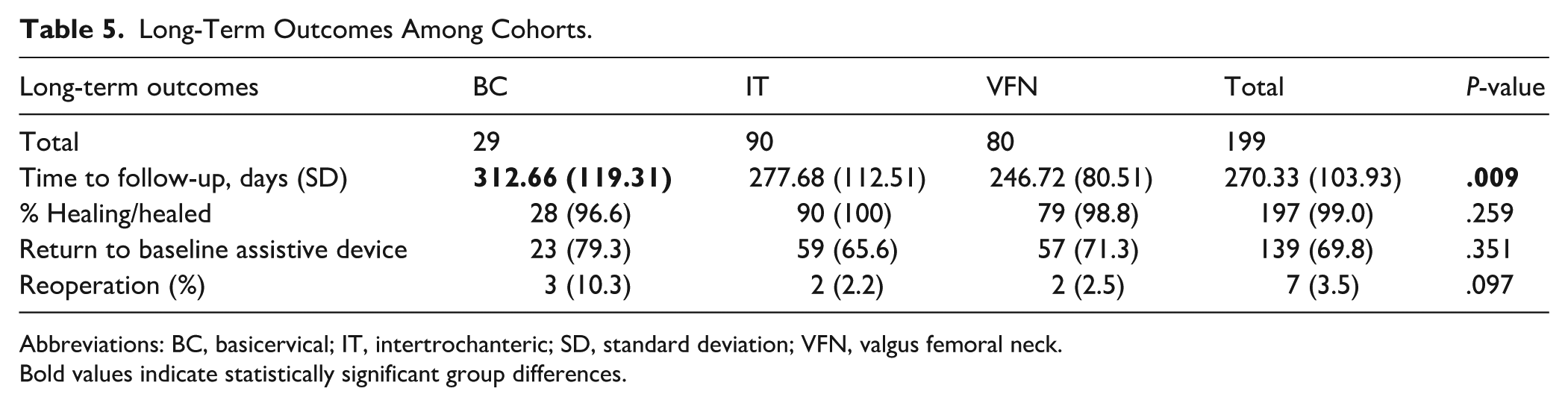
Abbreviations: BC, basicervical; IT, intertrochanteric; SD, standard deviation; VFN, valgus femoral neck.
Bold values indicate statistically significant group differences.
Long-Term Outcomes Compared Among Surgical Constructs in the Basicervical Cohort.
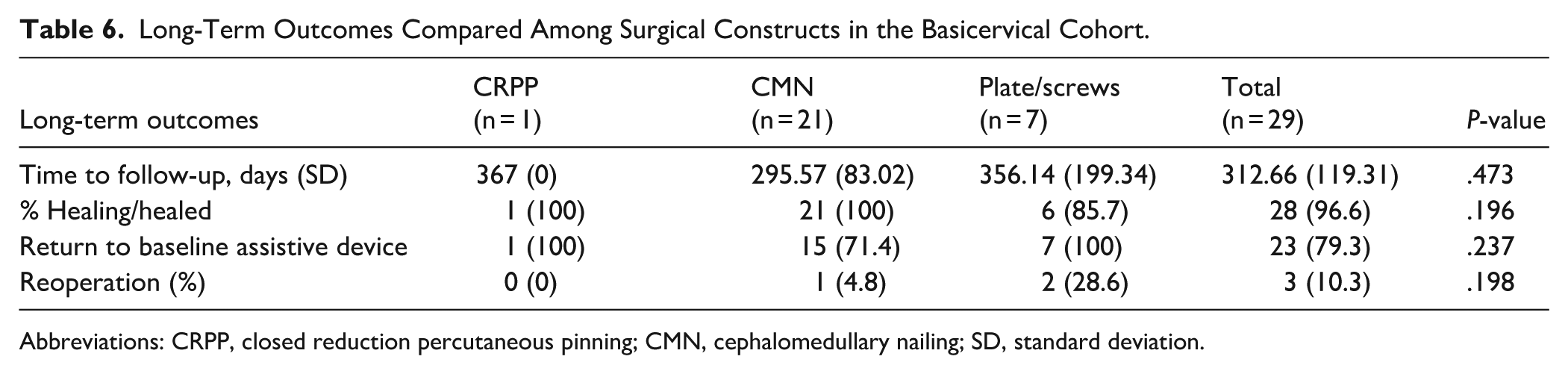
Abbreviations: CRPP, closed reduction percutaneous pinning; CMN, cephalomedullary nailing; SD, standard deviation.
Discussion
These results suggest that patients who sustained BC fractures were on average younger than IT patients and had a higher ASA and decreased baseline functionality compared to the VFN group. Fixation method also differed between groups, with BC fractures mostly undergoing fixation with CMN (69.7%) and plate/screw construct (29.5%), while the majority of IT underwent CMN fixation (93.1%) and the majority of VFN underwent closed reduction percutaneous pinning (CRPP) (89.1%). Finally, the only difference in baseline-controlled short-term outcomes was demonstrated in minor complications, in which BC fractures had a greater frequency than VFN. No differences were observed in long-term outcomes among fracture types, and within the BC group there were no differences in short- or long-term outcomes among surgical construct types.
While this study contributes to the current discussion regarding characteristics and outcomes of this rare subset of proximal femur fractures, these results have limitations. Although data was prospectively collected, the analysis is retrospective, which introduces the possibility of selection bias. Second, fracture classifications were assigned by attending surgeons and were not corroborated by a common independent source, raising concerns about interobserver variability or misclassification. 15 Third, the heterogeneity of fixation methods in the BC group, which were not randomly assigned, may have been influenced by unmeasured confounders such as fracture morphology, bone quality, or surgeon preference. Lastly, less than 25% of the initial cohort had 6-month follow-up data, introducing attrition bias, and small sample sizes in long-term follow-up limit our ability to detect differences. Because long-term follow-up was not standardized and it relied on the most recent follow-up visit, the return to baseline assistive device outcome may be confounded by interval variability. Future prospective studies with standardized fixation protocols and long-term follow-up are essential to guide evidence-based management of this understudied yet distinct fracture pattern.
The demographic and baseline functional profiles observed suggest that BC fracture patients occupy a unique intermediate clinical space. While younger than IT patients, they demonstrated greater medical comorbidity and functional limitations compared to those with VFN fractures. While most other baseline factors did not display significance, the differences that were identified may demonstrate that the BC population represents a distinct clinical phenotype. This supports the notion that BC fractures are not merely a variant of femoral neck or IT fractures but may warrant their own classification and treatment approach. Although this exact comparison has not been replicated in the literature, Cha and Yoo found no demographic differences between femoral neck fracture patients and BC fracture patients. 16 Similarly, Su et al found no differences in age or sex between BC and IT fracture patients. 17 However, both studies had samples under 100, which makes their analyses relatively underpowered compared to this analysis. Further research is warranted regarding baseline health profile differences between BC fracture patients and other hip fracture types.
Within the BC cohort, there was substantial variation in fixation technique, with a mixture of nails and plate/screw constructs. Unlike IT fractures, which are almost always fixed with a nail, and VFN fractures, which are usually treated with a pinning, there remains a lack of a standardized approach for BC fixation. This study’s analyses demonstrated no differences in short- or long-term outcomes across surgical constructs. Although the sample size within the BC cohort was underpowered, these results are in line with the lack of consensus in previous literature and could represent true clinical equivalence. Lee et al found that extramedullary plating with a DHS was a significant risk factor for fracture site collapse and fixation failure compared to intramedullary nail with a helical blade. 18 Saarenpää et al report better results with DHS or gamma nail compared to hemiarthroplasty or screw osteosynthesis, 1 a finding which is corroborated by Kim et al, though they note that higher complication rates with osteosynthesis can be reduced through the use of CMN. 19 Indeed, several studies report success with CMN as well as DHS.3,20,21 Yoon et al found that while DHS takes a longer time for fracture union, cut-out and reoperation rates are similar between DHS and CMN. 5 Similarly, Yoon et al compared outcomes of IT and BC fractures treated with proximal femoral nail or CMN and found that BC fracture pattern was positively correlated to screw cut-out regardless of fixation method used. 22 Despite these prior efforts to evaluate the optimal fixation method for BC fractures, there remains a need for high-quality evidence to inform standardized treatment protocols.
Furthermore, after adjusting for STTGMA and surgical construct, most short-term outcomes in this analysis were similar across groups. Minor in-hospital complications remained significantly more frequent in the BC group compared to VFN after baseline health controls were implemented. This may reflect a greater physiologic burden or perioperative complexity associated with BC fractures. Most previous studies comparing these patterns to other hip fractures did not scrutinize in-hospital and short-term outcomes. However, Saha et al’s study of 26 BC fracture patients found a similar length of stay of 7 days compared to 6.47 days found in this study. 23 These findings, along with limited prior literature, reinforce the need to more closely examine the clinical trajectory and perioperative risks specific to BC fractures. This study enhances the existing literature by providing detailed short-term outcome data, leveraging a robust sample size and a wide array of clinical variables.
In terms of long-term outcomes, no differences were found across fracture types. However, as less than a quarter of the original cohort was included in this analysis, it is likely this represents a lack of power. The BC group had a reoperation rate of 10.3%, which was substantially higher than 2.2% for IT and 2.5% for VFN. However, this difference was not significant, likely due to the small sample size. High incidence of adverse outcomes following BC fractures has been reported several times. Lee et al found that 24.6% of patients with BC fractures experienced collapse of the fracture site, while 8.6% underwent conversion to arthroplasty secondary to fixation failure. 18 Conversely, other studies report no incidence of nonunion or fixation failure.24-26
Some of this variation in adverse outcomes may be related to characteristics of the fracture itself. For instance, Sundkvist et al found that nondisplaced BC femoral neck fractures had a treatment failure rate of 3% with internal fixation, while displaced BC femoral neck fractures had a much higher failure rate of 16%. 27 Heterogeneity in reported complication rates could also be due to the rarity of the fracture, limiting datasets from being able to provide powerful, generalizable statistics.
Several studies have compared BC fracture outcomes to other fracture types. Kwak et al assessed outcomes following CMN for pertrochanteric fractures and found that BC fracture components were a risk factor for later osteonecrosis of the femoral head. 28 Su et al compared BC fractures to both stable and unstable IT fractures. 17 They found that while greater than 10% fracture collapse was significantly more likely with BC fractures compared to stable IT fractures, this did not hold true compared to unstable IT fractures. However, while patients with BC fractures reported less pain compared to unstable IT fractures, there were no other significant differences in clinical outcomes scores between BC and stable or unstable IT fractures. While this result may suggest that BC fractures possess greater biomechanical instability, Massoud suggests that BC and trochanteric fractures have similar instability characteristics such as axial and rotary instability, warranting similar treatment of these 2 fracture patterns. 29
The current study similarly demonstrated that patients who sustain BC, IT, and VFN fractures have comparable long-term outcomes; however, surgical technique was significantly different between fracture type. This suggests that while these fracture patterns all pose challenges with regard to stability, careful consideration of fracture type is warranted to identify an optimal management strategy.
Many studies comparing BC outcomes are limited by small sample size. Our study, specifically the short-term analysis, provides a more robust sample size and an updated review. Promisingly, we find that despite more frequent minor complications compared to intracapsular VFN patients, subsequent outcomes including healing, revision, and readmission rates are similar between BC and IT and femoral neck fractures. Further research on optimal acute treatment strategies may help mitigate these initial adverse outcome rates.
In conclusion, this retrospective analysis suggests that BC hip fractures may be associated with a higher frequency of minor in-hospital complications compared to VFN fractures but demonstrate similar short- and long-term outcomes compared to IT and VFN fractures. No fixation method demonstrated clear superiority within the BC cohort. Further research is needed to refine fixation strategies and improve perioperative outcomes in this distinct fracture subtype.
Supplemental Material
sj-pdf-1-hss-10.1177_15563316261429896 – Supplemental material for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures?
Supplemental material, sj-pdf-1-hss-10.1177_15563316261429896 for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures? by Benjamin Hammond, Chloe Fong, Dillon Murugesan, Abhishek Ganta, Sanjit Konda and Kenneth Egol in HSS Journal®
Supplemental Material
sj-pdf-2-hss-10.1177_15563316261429896 – Supplemental material for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures?
Supplemental material, sj-pdf-2-hss-10.1177_15563316261429896 for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures? by Benjamin Hammond, Chloe Fong, Dillon Murugesan, Abhishek Ganta, Sanjit Konda and Kenneth Egol in HSS Journal®
Supplemental Material
sj-pdf-3-hss-10.1177_15563316261429896 – Supplemental material for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures?
Supplemental material, sj-pdf-3-hss-10.1177_15563316261429896 for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures? by Benjamin Hammond, Chloe Fong, Dillon Murugesan, Abhishek Ganta, Sanjit Konda and Kenneth Egol in HSS Journal®
Supplemental Material
sj-pdf-4-hss-10.1177_15563316261429896 – Supplemental material for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures?
Supplemental material, sj-pdf-4-hss-10.1177_15563316261429896 for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures? by Benjamin Hammond, Chloe Fong, Dillon Murugesan, Abhishek Ganta, Sanjit Konda and Kenneth Egol in HSS Journal®
Supplemental Material
sj-pdf-5-hss-10.1177_15563316261429896 – Supplemental material for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures?
Supplemental material, sj-pdf-5-hss-10.1177_15563316261429896 for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures? by Benjamin Hammond, Chloe Fong, Dillon Murugesan, Abhishek Ganta, Sanjit Konda and Kenneth Egol in HSS Journal®
Supplemental Material
sj-pdf-6-hss-10.1177_15563316261429896 – Supplemental material for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures?
Supplemental material, sj-pdf-6-hss-10.1177_15563316261429896 for Fixation of Basicervical Hip Fractures: Are Outcomes Distinct from Neighboring Valgus Neck and Intertrochanteric Fractures? by Benjamin Hammond, Chloe Fong, Dillon Murugesan, Abhishek Ganta, Sanjit Konda and Kenneth Egol in HSS Journal®
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was waived from all participants included in this retrospective study by the IRB at NYU Langone Orthopedic Hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Adult Learner Clinical Explorer Program at NYU Langone Orthopedic Hospital is supported in part by Depuy Synthes, although the research reported in this article was not funded by any particular entity.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sanjit Konda, MD, declares relationships with Stryker and AAOS. Abhishek Ganta, MD, declares a relationship with OTA. Kenneth Egol, MD, declares relationships with Exactech and Wolters Kluwer. The other authors declared no potential conflicts of interest.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
AI Use
The authors declared the following use of artificial intelligence (AI) tools in the writing or editing of this article: The authors used ChatGPT (OpenAI) to improve the clarity and grammatical structure of the manuscript. After using this tool, the authors reviewed and edited the content as needed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.