
Abstract
Background:
Total hip arthroplasty (THA) continues to shift from inpatient to outpatient facilities.
Purpose:
We sought to examine trends in THA settings, demographic differences, and comorbidity variations to inform patient selection, outcomes, and policy.
Methods:
We performed a retrospective study using data from January 1, 2019, to December 31, 2022, which we obtained from the Nationwide Inpatient Sample database and Nationwide Ambulatory Surgery Sample, from the U.S. Agency for Healthcare Research and Quality. Patients undergoing primary, elective THA were identified.
Results:
Of the 1 449 639 patients we identified who underwent elective THA, 843 824 underwent the procedure in a hospital-owned ambulatory facility and 605 815 in a hospital (inpatient setting). A total of 86% of THA volume migrated to outpatient centers from 2019 to 2022. Patients who underwent THA at an outpatient facility versus an inpatient setting were younger (65.3 vs 66.3 years). A higher percentage of female versus male patients had surgery in a hospital than in an outpatient center (56.2% vs 53.8%). White and black patients were more likely to be treated at an inpatient facility, whereas Hispanic patients were more likely to be treated at an outpatient facility. Medicare and Medicaid patients were more likely to undergo surgery as inpatients. Patients with medical comorbidities, as well as smokers and patients with opioid use disorder, were overwhelmingly more likely to undergo inpatient THA.
Conclusion:
This retrospective database analysis found that from 2019 through 2022, outpatient THA numbers increased each year, with 90% of THAs being performed in hospital-owned ambulatory facilities in 2022. Patients with significant medical comorbidities and Medicare/Medicaid insurance, as well as white and black patients, were more likely to have inpatient surgery.
Level of Evidence:
Level III, Retrospective Database Study.
Plain Language Summary
Total hip replacement is a common surgery to treat severe hip pain from arthritis. In the past, patients usually stayed in the hospital after surgery. But recently, more people have this surgery as outpatients, often in hospital-owned outpatient centers. This study looked at national data from 2019 to 2022 to see how this change happened and who was getting surgery in different settings. We studied over 1.4 million people who had planned hip replacements. Key findings include: There was a big shift to outpatient surgery. In 2019, only 5% of these surgeries happened in outpatient centers. By 2022, this jumped to 91%. Overall, 86% of the procedures moved from hospitals to outpatient settings during these years. People who had outpatient surgery were usually younger (average age 65.3 years) compared to those in hospitals (average age 66.3 years). More women had surgery in hospitals than in outpatient centers. White and black patients were more likely to have inpatient (hospital) surgery, while Hispanic patients were more likely to have outpatient surgery. Patients with Medicare or Medicaid insurance were more likely to stay in the hospital, while those with private (commercial) insurance were more likely to go home the same day. People with health problems (like heart disease, diabetes, lung issues, or kidney problems), smokers, or those with opioid use issues were much more likely to have surgery in the hospital. These changes happened because of better surgery techniques, improved pain control (like spinal anesthesia), new implants, and policy updates that allowed more procedures outside traditional hospital stays. This helps lower healthcare costs and lets healthy patients recover at home sooner.
Keywords
Introduction
Total hip arthroplasty (THA) is the gold standard treatment for end stage osteoarthritis of the hip and has high rates of patient satisfaction.1 -4 THA consistently provides pain relief and improves patient function and quality of life; it is one of the most commonly performed procedures in the United States, and, given the aging population and the growing incidence of osteoarthritis, its prevalence is expected to increase significantly in the coming years.5 -7 From 2000 to 2019, the estimated annual THA volume in the United States increased by 177%, and studies estimate that it will increase from current levels by over 100% by 2040 and over 450% by 2060. 7 Initially an inpatient procedure, over time THA has shifted to outpatient facilities like ambulatory surgery centers (ASCs). From 2010 to 2021, ~88% of THAs were performed on an inpatient basis, but this number decreased significantly after the procedure was removed from the inpatient-only list in 2020. 8 Outpatient THA has largely been driven by improvements in surgical technique, implant design, spinal anesthesia, postoperative pain protocols, and a national effort to decrease healthcare costs. 9
Prior studies demonstrate that patients with severe medical comorbidities including hypertension, cerebrovascular disease, chronic kidney disease, heart disease, and chronic obstructive pulmonary disease (COPD) may be more likely to receive surgery at an inpatient facility than at an ASC.10 -12 Patient race and gender may also influence surgical setting.8,9,13 -18 For example, recent literature has shown that black and female patients were less likely to undergo outpatient total joint arthroplasty (TJA) than white and male patients.19 -21 To date, no study has used a large, nationally representative database to explore the effects of patient demographics or comorbidities on the decision to perform THA in a hospital versus an ASC.
This retrospective study aimed to address 3 research questions: (1) What are the trends in the distribution of primary THA between hospitals and ambulatory surgical centers in the United States? (2) Are there differences in demographic characteristics between patients undergoing THA in hospital versus ambulatory settings? and (3) Is there a difference in the comorbidity profiles between patients treated in these 2 settings? By answering these questions, we sought to analyze the ongoing shift in THA care and its implications for patient selection and healthcare delivery.
Methods
This retrospective study was performed using data from January 1, 2019, to December 31, 2022, which was obtained from the Nationwide Inpatient Sample (NIS) and Nationwide Ambulatory Surgery Sample (NASS) databases. (Institutional review board approval was not needed because this study used de-identified, publicly available data, which does not involve direct patient contact or identifiable private health information, exempting it from human subjects research regulations.) The NIS is the largest inpatient healthcare database within the federal Healthcare Cost and Utilization Project (HCUP); it is sponsored by the Agency for Healthcare Research and Quality (AHRQ). It provides national estimates of inpatient outcomes, access, charges, utilization, and quality by collecting data from community hospitals in states participating in HCUP. The data collected ~20% stratified sample of U.S. community hospitals with a self-weighted design to reduce the margin of error for estimates. The NASS, also developed by AHRQ through a federal-state-industry partnership, is the only all-payer U.S. ambulatory surgery database. It provides national estimates of high-volume or high-cost therapeutic ambulatory surgeries performed in hospital-owned facilities, such as freestanding ASCs or hospital-based outpatient facilities. For our study, “outpatient” refers to procedures performed in hospital-owned ambulatory facilities (as defined by the NASS), which may include hospital-based outpatient departments or hospital-affiliated ASCs. This differs from payer/insurance designations of “outpatient” status, which can vary independently of the physical facility. The NASS is restricted to hospital-owned facilities and excludes freestanding (non-hospital-owned) ASCs. In contrast, “inpatient” in this study refers to procedures captured in the NIS, which include hospital stays in community hospitals (non-federal, short-term, acute care facilities), regardless of length of stay.
Patients who underwent primary, elective, unilateral THA were identified in the NIS using a previously validated algorithm based on a combination of International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS), and Diagnosis Related Group. 22 This approach has been shown to reduce miscoding by over 20%. Patients with the same procedures were identified with a modified algorithm in the NASS database by using Current Procedural Terminology codes 27130. Bilateral, non-elective, and revision surgeries were excluded.
Patient demographics were extracted from the respective databases, including age, sex, race, ethnicity, and insurance payer. Differences in patient comorbidities between surgery settings were determined using the modified AHRQ Elixhauser 38 comorbidities; smoking and opioid use were also recorded. Opioid use was identified using ICD-10-CM codes for opioid use disorders or long-term use of opioids (F11.XXX and Z79.891), consistent with prior NIS database studies evaluating opioid exposure. 23
Statistical Analysis
All data analyses were performed using SPSS version 27 for Windows (IBM Corp). Descriptive statistics were obtained for all variables used within the study. Missing values were excluded from the analysis. For comparisons, we used χ2 and binary logistic regression to calculate odds ratios with their respective 95% confidence intervals. Statistical significance was assigned at the P < .05 level. The REporting of studies Conducted using Observational Routinely-collected health Data checklist was used in preparing this report.
Results
We identified a total of 1 449 639 patients who underwent elective THA. Of these, 843 824 patients underwent the procedure in an ASC and 605 815 in a hospital. From 2019 to 2022, 86% of THA volume migrated from hospitals to outpatient centers. In 2019, 5% of THAs were performed in an ambulatory setting; by 2022 this percentage had grown to 90% (Figure 1).
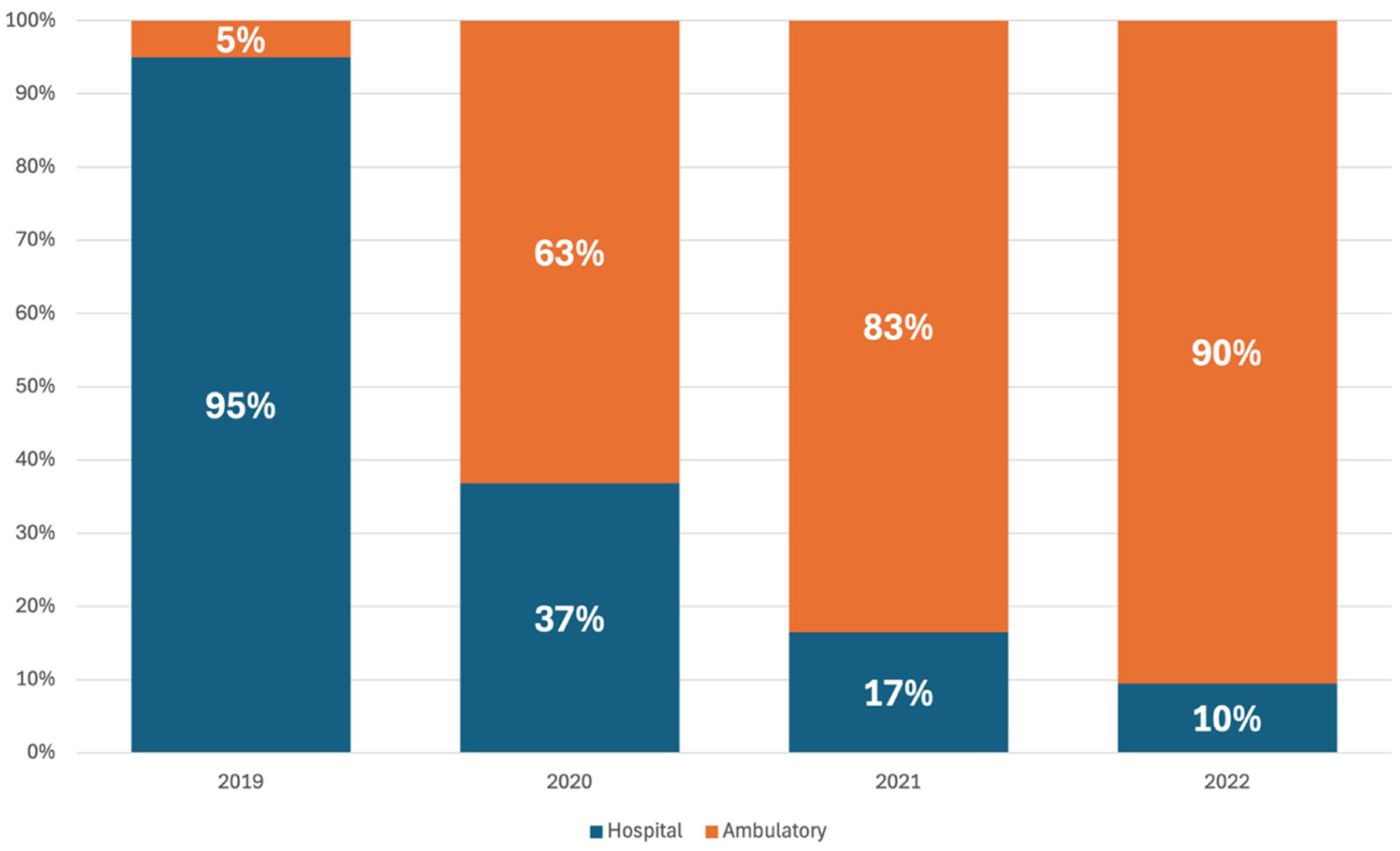
Proportion of total hip arthroplasties performed in an inpatient setting versus hospital-owned ambulatory facilities from 2019 to 2022, showing a shift toward ambulatory surgery.
Patients who underwent THA at an outpatient facility were younger than those who had surgery in a hospital (65.3 vs 66.3 years, P < .01; Table 1). A higher percentage of female patients had surgery in a hospital than in an outpatient center (56.2% vs 53.8%, P < .01). A higher percentage of B patients underwent THA at an inpatient facility whereas a larger percentage of Hispanic patients were treated at an outpatient facility (P < .01). Medicare and Medicaid patients were more likely to undergo surgery at an inpatient facility, whereas patients with commercial insurance were more likely to undergo THA at an outpatient center (P < .01).
Comparison of Demographic Characteristics of Patients Having Primary Total Hip Arthroplasty in Inpatient Hospitals Versus Hospital Owned Ambulatory Facilities in the NIS and NASS Database, 2019 to 2022.
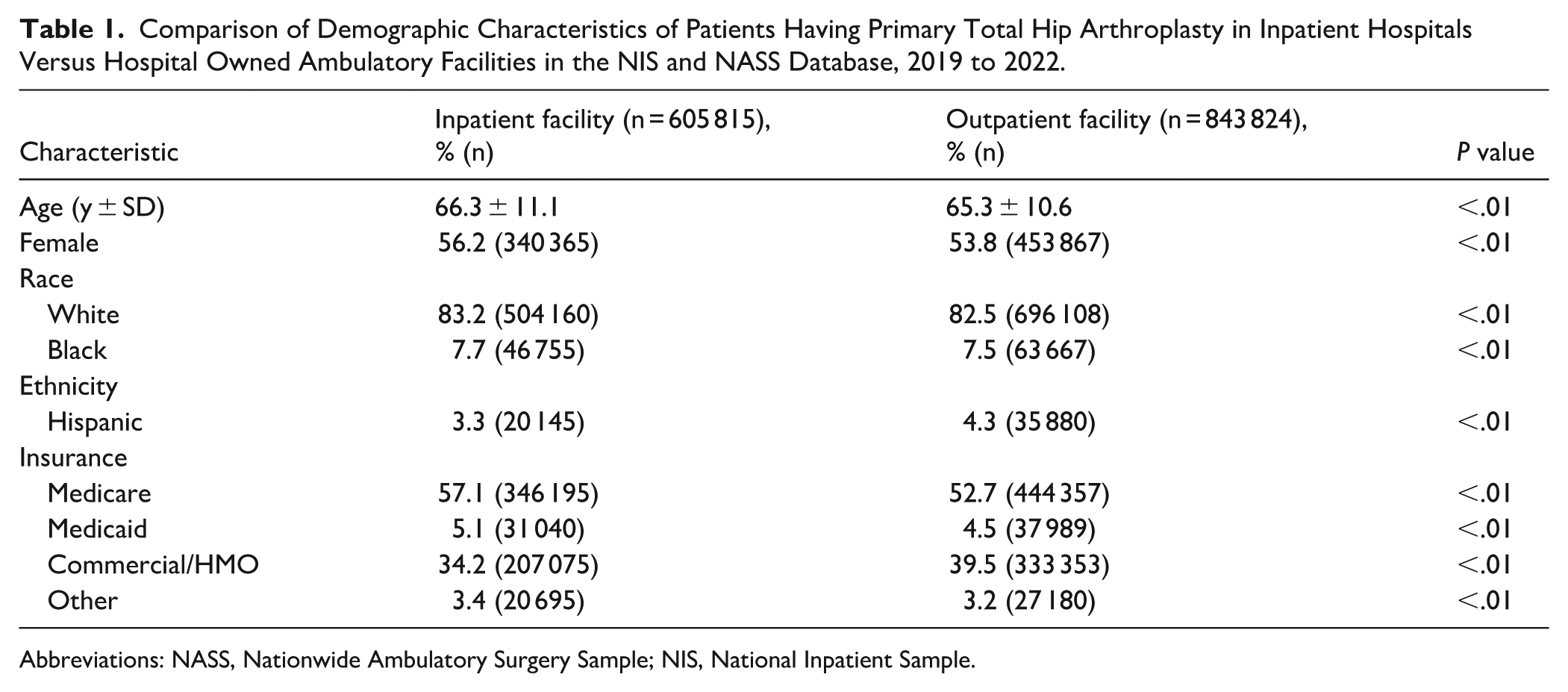
Abbreviations: NASS, Nationwide Ambulatory Surgery Sample; NIS, National Inpatient Sample.
Patients with nearly all Elixhauser comorbidities were overwhelmingly more likely to undergo inpatient THA (P < .01). Patients who smoked and those with opioid use disorder were also more likely to have surgery in a hospital setting (Table 2).
Comparison of Comorbidity Profile Based on the Elixhauser Index of Patients Having Primary Total Hip Arthroplasty in Hospitals Versus Ambulatory Centers in the NIS and NASS Database, 2019 to 2022.
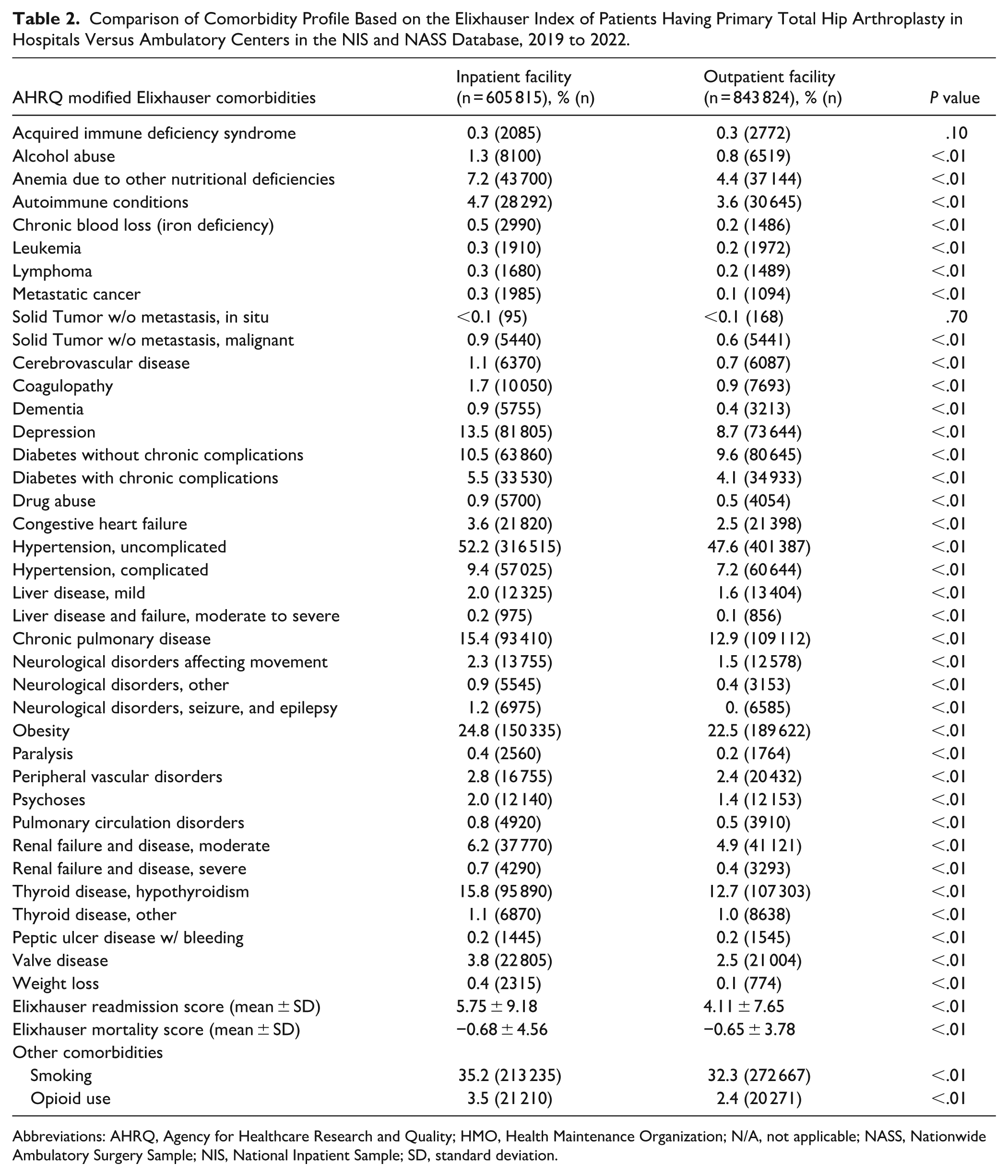
Abbreviations: AHRQ, Agency for Healthcare Research and Quality; HMO, Health Maintenance Organization; N/A, not applicable; NASS, Nationwide Ambulatory Surgery Sample; NIS, National Inpatient Sample; SD, standard deviation.
Discussion
This retrospective database analysis evaluated U.S. migration patterns of primary THA from the inpatient to the outpatient setting, as well as the associations between surgical setting, demographic variables, and comorbidities. From 2019 to 2022, 86% of THA volume migrated from hospitals to ASCs, a significant and rapid increase in outpatient surgery. This shift to outpatient THA has been driven by changes in reimbursement, the removal of THA from the inpatient-only list, improvements in surgical technique, implant design, use of spinal anesthesia, and pain control. Healthy patients without significant medical comorbidities, patients with private insurance, and Hispanic patients were more likely to undergo outpatient surgery than their counterparts. These findings indicate that economic and racial disparities remain with regard to healthcare equity.
This is a retrospective database study, which comes with inherent limitations. The databases we used relied on specific codes, meaning the integrity of the database can be affected by errors in coding or misclassifications. As with many databases, certain variables are not reported including outcomes data, complications, severity of comorbidities, and preoperative function. Given the retrospective nature of this study, we found many significant associations, but could not prove causality. A key limitation is that the NASS excludes freestanding ASCs, which may perform a small but growing portion of THAs, estimated at 8% to 9% of TJAs by 2022. 24 This could result in an underestimation of the total outpatient THA volume in our study, although hospital-owned settings (including hospital outpatient departments) represent the majority of outpatient cases. Future studies incorporating data from freestanding ASCs (eg, via commercial claims databases) could provide a more comprehensive view. Additionally, the study period includes the COVID-19 pandemic, which led to significant deferral of elective procedures (particularly in 2020), potentially affecting THA volumes and contributing to the accelerated adoption of outpatient settings as hospitals prioritized shorter stays upon resumption of elective cases.
Our findings are consistent with prior studies that have shown an increase in the use of outpatient THA. We found 5% of THAs were performed in an ambulatory setting in 2019, increasing to 90% of THAs in 2022. The observed increase in outpatient THA, especially post 2020, corresponds to Centers for Medicare and Medicaid Services policy changes removing THA from the inpatient-only list (effective 2020) and adding it to the ASC-covered procedures list (effective 2021), which primarily impacted Medicare patients later in the data set. Pasqualini et al found that outpatient THA increased by 751%, after the removal of THA from the inpatient-only list, and that complication rates remained low; the authors concluded that outpatient THA is safe and effective with appropriate patient selection and preoperative optimization. 8 Multiple studies have similarly found that outpatient THA is safe and effective without increases in complication or readmission rates when compared with inpatient THA.9 -11,25 -29 Ng et al evaluated cost savings from outpatient versus inpatient THA, finding that 90 day costs were reduced by more than $16 000/patient in the outpatient cohort. 27 In addition to changes in policy, outpatient TJA is further driven by improvements in perioperative pain control, spinal anesthesia, and patient education.30,31 As research, technology, and perioperative protocols continue to improve, we will likely continue to see increased utilization of outpatient THA.
In our study, female, Hispanic, and Medicare/Medicaid patients were more likely to have inpatient THA, whereas a larger percentage of white, black, and privately insured patients underwent outpatient THA. As with prior research, these findings indicate that demographic variables continue to be associated with differences in access to care. Medicare and Medicaid insurance status has consistently been linked to higher rates of inpatient TJA. 21 Interestingly, we found that black patients were more likely to have outpatient THA, whereas prior literature overwhelmingly suggests that black patients are more likely to receive inpatient TJA. In 2022, Amen et al reported on differences in the relative utilization of same-day discharge versus inpatient TJA between white and black patients. The authors concluded that black patients were significantly less likely to undergo outpatient THA. 19 Connolly et al studied factors likely to be predictive of patients who were initially booked for outpatient THA but required conversion to inpatient status and found that black race, age over 65, and female gender were all significantly associated with a conversion to inpatient status. 21 Interestingly, a study by Piponov et al found that black, Hispanic, and Asian patients were all more likely than white patients to undergo outpatient TJA, although these findings were not specific to THA. 17 While our findings suggest that improvements in health equity and access to care have been made, further research is needed to truly elucidate the associations between demographic variables and outpatient THA.
Patients with nearly all comorbidities, those who smoked, and those with opioid use disorder were significantly more likely to undergo inpatient THA than patients without medical comorbidities. Our findings are consistent with prior literature. Greenky et al compared complication rates in Medicare patients undergoing inpatient versus outpatient THA. 14 The authors found that independent risk factors for requiring inpatient stay included general anesthesia, body mass index >35, diabetes, COPD, congestive heart failure, hypertension, malnutrition, age >75 years, female gender, and minority ethnicity. Despite these findings, a recent article by Patel and Buller suggests that patients with multiple comorbidities may be able to undergo outpatient TJA with appropriate medical optimization, evidence-based perioperative protocols, patient education, protocolized postoperative management, and a safety net in the rare instance of postoperative complication. 32 As THA was performed on an outpatient basis more than 90% of the time in 2022, it is likely that patients with multiple comorbidities are increasingly being treated in ASCs today. Further research and standardization of patient selection and perioperative protocols must be adopted on a larger scale to safely treat more complex patients in the outpatient setting.
In conclusion, this retrospective database analysis found that outpatient THA (performed in hospital-owned ambulatory facilities, including hospital outpatient departments and hospital-affiliated ASCs) continued to increase annually, with over 90% of cases in such settings in 2022. Patients with significant medical comorbidities, Medicare/Medicaid insurance, and white and black patients were more likely to have inpatient surgery, whereas healthy patients with commercial insurance and Hispanic patients were more likely to have outpatient surgery. Our results suggest that outpatient THA is safe and effective for most patients. Future studies should further evaluate the disparities in access to care based on ethnicity, sex, and insurance status.
Supplemental Material
sj-docx-1-hss-10.1177_15563316261431234 – Supplemental material for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022)
Supplemental material, sj-docx-1-hss-10.1177_15563316261431234 for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022) by Joseph S. Geller, Aneesh Samineni, Ronald M. Swonger, David Constantinescu, Natalia Cruz-Ossa and Michele R. D’Apuzzo in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316261431234 – Supplemental material for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022)
Supplemental material, sj-docx-2-hss-10.1177_15563316261431234 for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022) by Joseph S. Geller, Aneesh Samineni, Ronald M. Swonger, David Constantinescu, Natalia Cruz-Ossa and Michele R. D’Apuzzo in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316261431234 – Supplemental material for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022)
Supplemental material, sj-docx-3-hss-10.1177_15563316261431234 for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022) by Joseph S. Geller, Aneesh Samineni, Ronald M. Swonger, David Constantinescu, Natalia Cruz-Ossa and Michele R. D’Apuzzo in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316261431234 – Supplemental material for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022)
Supplemental material, sj-docx-4-hss-10.1177_15563316261431234 for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022) by Joseph S. Geller, Aneesh Samineni, Ronald M. Swonger, David Constantinescu, Natalia Cruz-Ossa and Michele R. D’Apuzzo in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316261431234 – Supplemental material for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022)
Supplemental material, sj-docx-5-hss-10.1177_15563316261431234 for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022) by Joseph S. Geller, Aneesh Samineni, Ronald M. Swonger, David Constantinescu, Natalia Cruz-Ossa and Michele R. D’Apuzzo in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316261431234 – Supplemental material for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022)
Supplemental material, sj-docx-6-hss-10.1177_15563316261431234 for The Outpatient Surge in Total Hip Arthroplasty: National Trends in Volume Migration, Demographic Disparities, and Comorbidity Profiles (2019-2022) by Joseph S. Geller, Aneesh Samineni, Ronald M. Swonger, David Constantinescu, Natalia Cruz-Ossa and Michele R. D’Apuzzo in HSS Journal®
Footnotes
Ethical Considerations
All the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was waived for all patients included in this database study by the IRB at University of Miami Miller School of Medicine.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michele R. D’Apuzzo, MD, and Natalia Cruz-Ossa, MD, both declared relationships with Zimmer, OREF, AAOS, Florida Orthopedic Society, and Miami Orthopedic Society. The other authors declared no potential conflicts of interest.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.