
Abstract
Background:
Reported data remains mixed on the extent to which insurer status as a surrogate for socioeconomic status (SES) affects perioperative outcomes in patients undergoing total knee arthroplasty (TKA).
Purpose:
This study evaluated postoperative outcomes utilizing insurance status as a surrogate for SES.
Methods:
This study retrospectively reviewed 8961 patients undergoing primary TKA at a single institution. Patients were grouped by insurance: Medicaid or non-Medicare commercial insurance. The primary outcome measure was revision surgery within 5 years of the index TKA. Time-to-event outcomes including reoperation, readmission, manipulation under anesthesia (MUA), and patient-reported outcome measures (PROMs) were analyzed.
Results:
Kaplan-Meier survival curves revealed greater time to revision survival probability in patients with Medicaid compared to patients with commercial insurance. No statistically significant differences were observed between groups for reoperation-free survival, readmission-free survival, or MUA-free survival. At both 1-year and 2-year postoperative follow-up, commercially insured patients had statistically significantly higher Knee Injury and Osteoarthritis Outcome Score Jr (KOOS Jr) scores compared with Medicaid patients. However, the absolute differences in KOOS JR scores at these time points did not exceed the previously established minimal clinically important difference.
Conclusion:
Despite having increased comorbidities and higher body mass index, Medicaid patients treated at this high-volume institution had improved revision-free survival and no difference in rates of reoperation or readmission, while achieving similar PROMs during the first 2 years following TKA.
Level of Evidence:
Level III, Prognostic study
Keywords
Introduction
The annual number of total knee arthroplasty (TKA) procedures performed in the United States is projected to reach 1.26 million by 2030, yet there is a documented underuse of TKA among patients from lower socioeconomic backgrounds.1-4 These patients often face longer surgical wait times and present with more severe degenerative joint disease than their higher socioeconomic counterparts.5,6 Social deprivation is a measure of socioeconomic disadvantage including financial insecurity, poor living conditions, and limited education, all of which contribute to poorer health outcomes and reduced quality of life. Higher levels of social deprivation are linked to reduced use of total joint arthroplasty, potentially worsening existing racial and ethnic disparities in orthopedic care.7,8 As the demand for TKA rises, it is critical to identify which populations are at risk for compromised results and mitigate outcomes with targeted interventions.
Currently, it is unclear whether socioeconomic status (SES) is linked to poorer patient-reported outcome measures (PROMs). Current post-TKA PROMs data yield mixed results when assessing the correlation between PROMs and SES, indicating that the question warrants further investigation.9-11 Non-white race, non-commercial insurance coverage, and a higher Charlson Comorbidity Index (CCI) are associated with worse pre-TKA PROMs and a poorer pain-function phenotype. 12 Lower SES is also linked with increased postoperative complications and emergency department utilization after TKA.13,14 Nonetheless, other studies have found that while patients from lower SES may have lower PROMs at a given postoperative visit, they achieve comparable therapeutic benefits from TKA with significant improvements from their preoperative scores. 15 Despite a significant need for TKA among these populations, substantial socioeconomic and racial barriers persist, highlighting the urgency for targeted interventions that accurately identify vulnerable patients. In addition to expanding access to care, it is also important to identify whether patients with limited access to care are at greater risk of complications after TKA and whether they achieve similar PROMs to the general population.
Many have proposed using payer status to stratify patients at a greater risk for postoperative complications.16,17 Patients with Medicaid are more likely to undergo TKA at lower-volume centers and by less experienced surgeons, often resulting in higher postoperative complication rates. 18 Given this, it may be proposed that populations at greater risk for postoperative complications would benefit from treatment at more specialized orthopedic centers. 19 However, neither the Centers for Medicare and Medicaid Services nor any commercial insurance payers currently incorporate race, ethnicity, or SES into their risk-adjustment algorithms. The exclusion of these factors may lead to the misclassification of hospitals that serve these vulnerable populations as lower-performing institutions.
In comparing outcomes between patients with commercial insurance and those covered by Medicaid, it remains unclear whether insurance status serves as a surrogate for SES when evaluating perioperative outcomes, 2-year revision risk, and readmission rates.
This study, conducted at a single, high-volume orthopedic center, aimed to determine differences in postoperative revision rates within 5 years of index surgery, 90-day complication rates, and need for manipulation under anesthesia (MUA) in patients with commercial versus Medicaid insurance.
Methods
A retrospective cohort study was performed of adult patients who underwent primary, elective, unilateral TKA at a single institution between February 1, 2016, and December 31, 2023. This institution provides a high annual volume of TKAs by fellowship-trained arthroplasty surgeons. All TKAs were performed by fellowship-trained joint arthroplasty surgeons specializing in knee arthroplasty in a single, high-volume department performing approximately 32 000 TKAs during the study period. Patients were identified in the institution’s registry through the use of the current procedural terminology code TKA: 27447. Demographic information including age, sex, body mass index (BMI), race, smoking status, and comorbidities was collected. BMI was divided into subcategories of “BMI < 30,” “BMI 30-35,” “BMI 35-40,” and “BMI > 40.” Race was classified as “White or Caucasian,” “Black or African American,” “Asian, Native Hawaiian, or Other Pacific Islander,” “Other,” or “Patient Declined/Unknown.” All demographic and outcome data were obtained via electronic medical record system review after patients were identified via registry. Inclusion criteria included patients who had undergone elective TKA for primary osteoarthritis and were over 45 years old. Patients were excluded if they had Medicare insurance.
This study was approved by our Institutional Review Board (#2024-0560), which exempted it from evaluation, as all patient information was anonymized in accordance with the U.S. Health Insurance Portability and Accountability Act.
All TKA patients were divided into “Medicaid” or “commercial” groups based on insurance status at the time of the procedure; the commercially insured cohort served as the control group. All patients underwent preoperative testing and risk stratification performed by hospitalists. The TKA systems and implants used were not standardized in this study among surgeons within the department. Postoperatively, all patients engaged in physical therapy and were monitored at postoperative visits by their surgeon.
The primary outcome measure was the need for revision surgery within the first 5 years of primary TKA. Revision surgery was defined as a surgical procedure in which 1 or more components of the original knee prosthesis were removed, replaced, or added. Reoperation was defined as any surgical procedure performed on the same knee after the initial TKA that required returning to the operating room, including revisions. TKA-related complications included thromboembolic events, periprosthetic joint infection, bearing surface wear, implant loosening, neural deficit, osteolysis, or periprosthetic fracture.
Secondary outcome measures included 90-day complications rates, hospital readmission, need for MUA within 5 years (without revision or surgical lysis of adhesions through an incision), and Knee Injury and Osteoarthritis Outcome Score Jr (KOOS Jr). KOOS Jr scores were obtained preoperatively and postoperatively at 6 weeks, 1 year, and 2 years. Revision-, reoperation-, readmission- and MUA-free survival were calculated comparing Medicaid and commercial cohorts.
Statistical Analysis
Descriptive statistics were used to summarize baseline demographic and clinical characteristics of the Medicaid and commercially insured cohorts. Categorical variables were reported as frequencies and percentages and compared using χ2 or Fisher’s exact tests, as appropriate. Continuous variables were summarized using means with standard deviations or medians with interquartile ranges, depending on distribution, and compared using t-tests.
Time-to-event outcomes—including time to revision, reoperation, hospital readmission, and MUA—were summarized using Kaplan-Meier survival plots, with differences between insurance groups assessed using log-rank tests. Patients without an event were censored at the time of last clinical follow-up.
To estimate the association between insurance status and each time-to-event outcome, Cox proportional hazards regression models were constructed to calculate unadjusted and adjusted hazard ratios (HRs) with 95% confidence intervals (CIs). The commercially insured cohort served as the reference group. Adjusted models included covariates selected a priori based on clinical relevance and prior literature, including sex, race (White vs non-White), BMI category, CCI, and smoking status at the time of surgery. Proportional hazards assumptions were assessed using Schoenfeld residuals.
Patient-reported outcomes were assessed using the KOOS, JR. KOOS, JR scores were analyzed as continuous variables at each time point (preoperatively, 6 weeks, 1 year, and 2 years postoperatively). Between-group comparisons at each visit were performed using Kruskal-Wallis tests. Changes in KOOS, JR scores over time were evaluated descriptively, and observed differences were interpreted in the context of the established minimal clinically important difference (MCID) for KOOS, JR following TKA.
All statistical tests were 2-sided, and a P-value < .05 was considered statistically significant. Statistical analyses were performed using SAS (version 9.4).
Results
A total of 8961 patients undergoing primary TKA met inclusion criteria, including 299 patients insured by Medicaid (3.3%) and 8662 patients with non-Medicare commercial insurance (96.7%).
Patients insured by Medicaid differed significantly from commercially insured patients across multiple baseline characteristics (Table 1). Medicaid patients versus commercially insured patients were more commonly female (79% vs 60%, P < .001), had higher BMI (P = .0009), and had a greater burden of medical comorbidities as measured by the CCI (P < .001). Among BMI categories, the most common in the Medicaid cohort was BMI 30-35 (33.9%), while the most common in the commercial cohort was BMI < 30 (36.4%). Medicaid patients were also more likely to be current smokers (P < .001) and have a higher proportion of non-White race compared with commercially insured patients.
Baseline Characteristics of Study Groups.
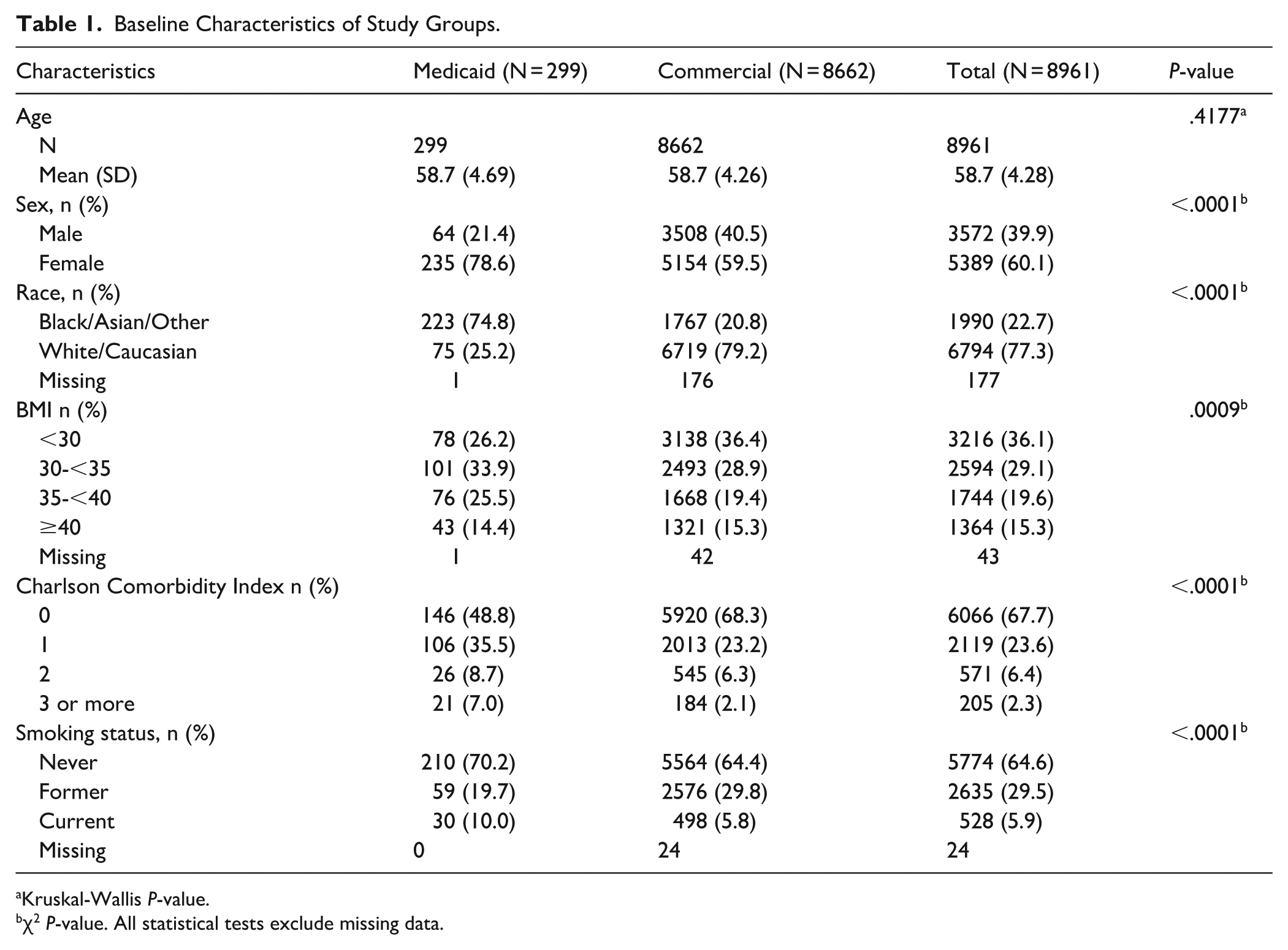
Kruskal-Wallis P-value.
χ2 P-value. All statistical tests exclude missing data.
Kaplan-Meier survival analyses demonstrated a statistically significant difference in revision-free survival between insurance groups, with Medicaid patients exhibiting greater revision-free survival compared with commercially insured patients (log-rank P = .046; Figure 1). At 5 years postoperatively, the revision rate was 1.0% in the Medicaid cohort and 2.1% in the commercially insured cohort.
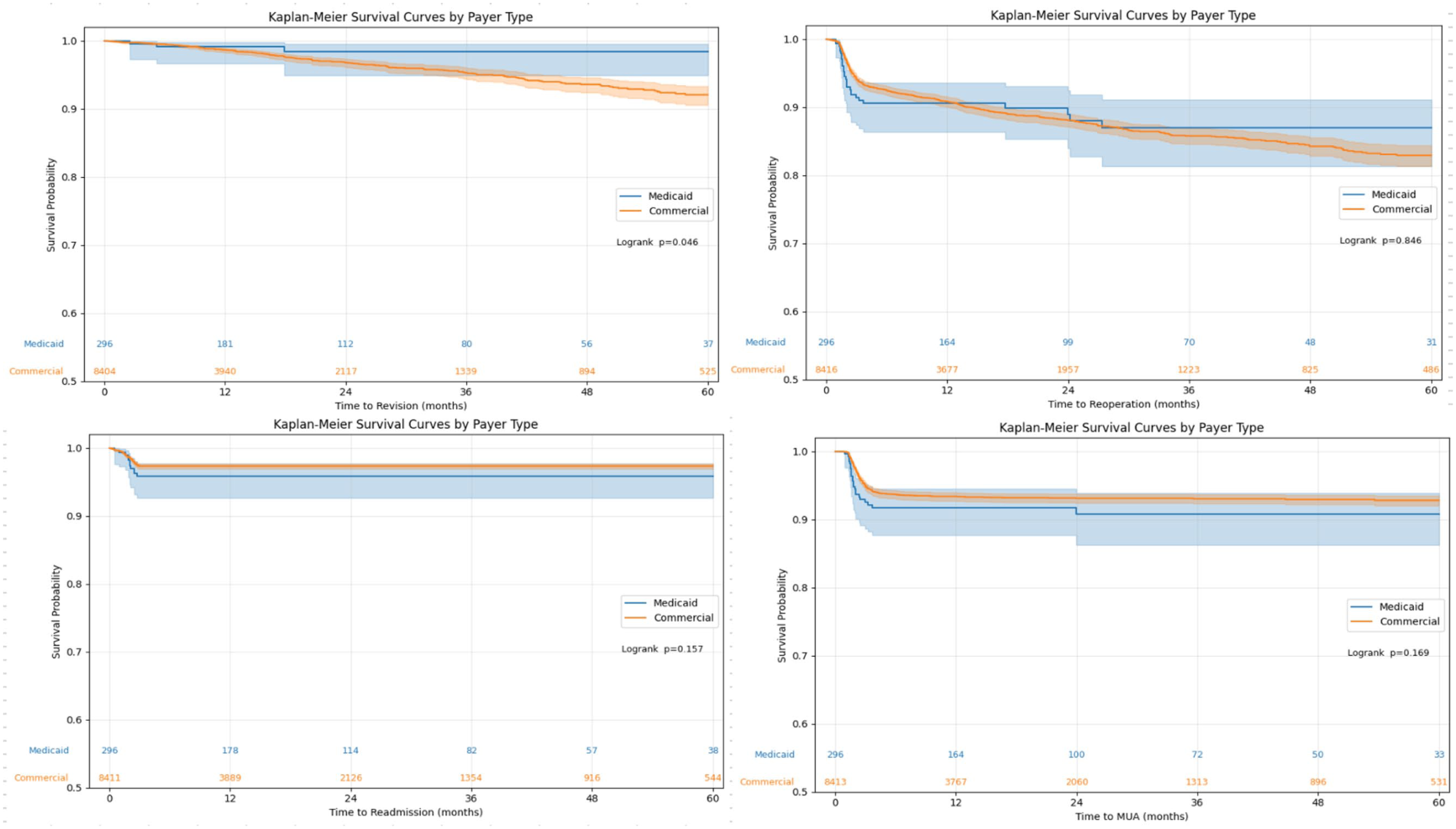
Kaplan-Meier survival curves for revision, reoperation, readmission, and MUA. MUA, Manipulation under anesthesia.
No statistically significant differences were observed between groups for reoperation-free survival (log-rank P = .846), readmission-free survival (log-rank P = .157), or MUA-free survival (log-rank P = .169). Five-year reoperation rates were 9.7% among Medicaid patients and 8.2% among commercially insured patients. Five-year readmission rates were 3.7% for Medicaid patients and 2.1% for commercially insured patients, while 5-year MUA rates were 7.7% and 4.9%, respectively (Table 2).
Comparison of Outcomes Between Study Groups.
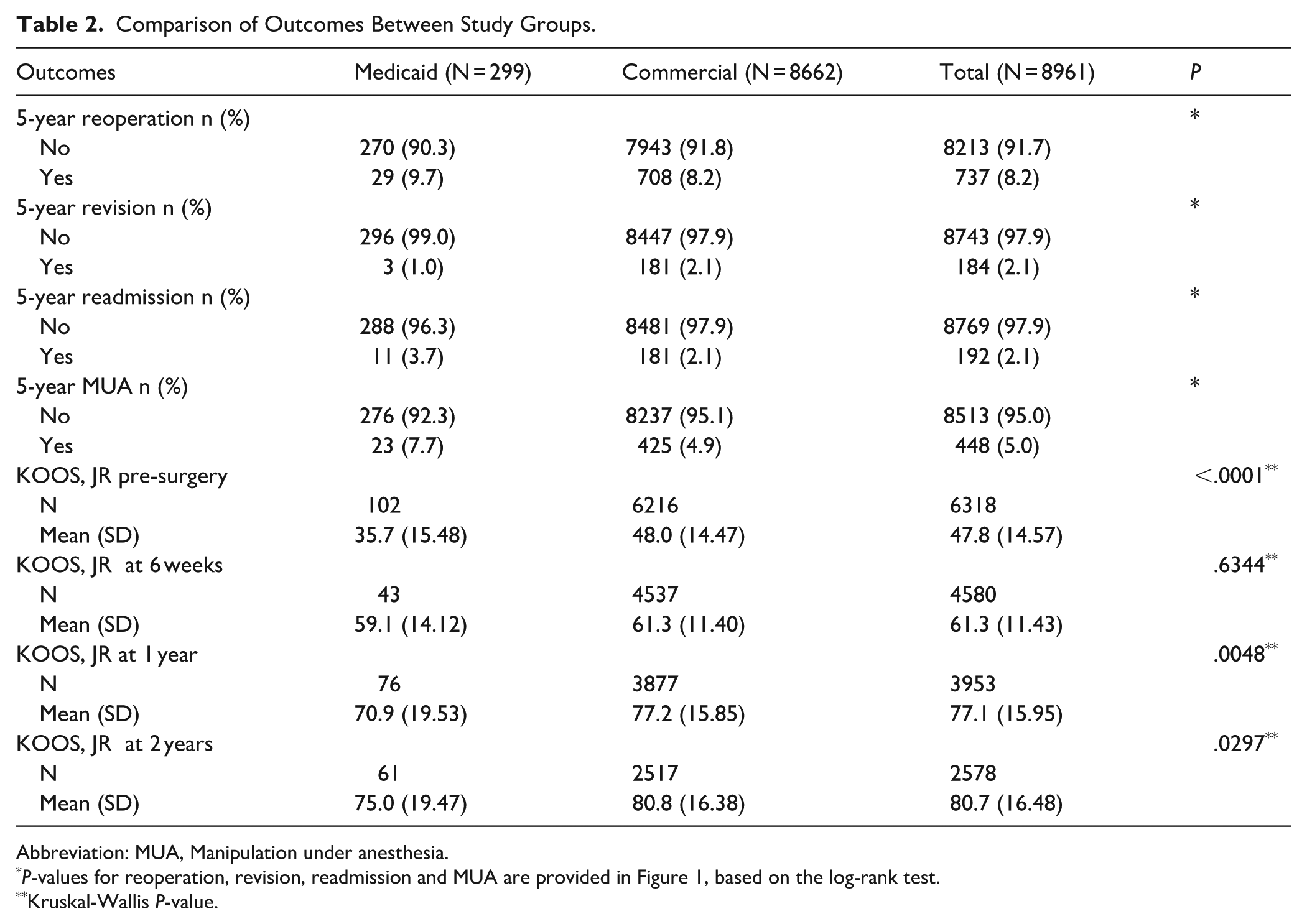
Abbreviation: MUA, Manipulation under anesthesia.
P-values for reoperation, revision, readmission and MUA are provided in Figure 1, based on the log-rank test.
Kruskal-Wallis P-value.
Unadjusted and adjusted hazard ratios for time-to-event outcomes are presented in Table 3. After adjustment for sex, race (White vs non-White), BMI, CCI, and smoking status, Medicaid insurance was not associated with a statistically significant difference in reoperation-free survival compared with commercial insurance (adjusted HR 0.776; 95% CI 0.528-1.142). Similarly, no significant difference was observed for MUA-free survival (adjusted HR 0.912; 95% CI 0.589-1.413).
Unadjusted and Adjusted Cox Regression Models Regarding Outcomes Between Groups.
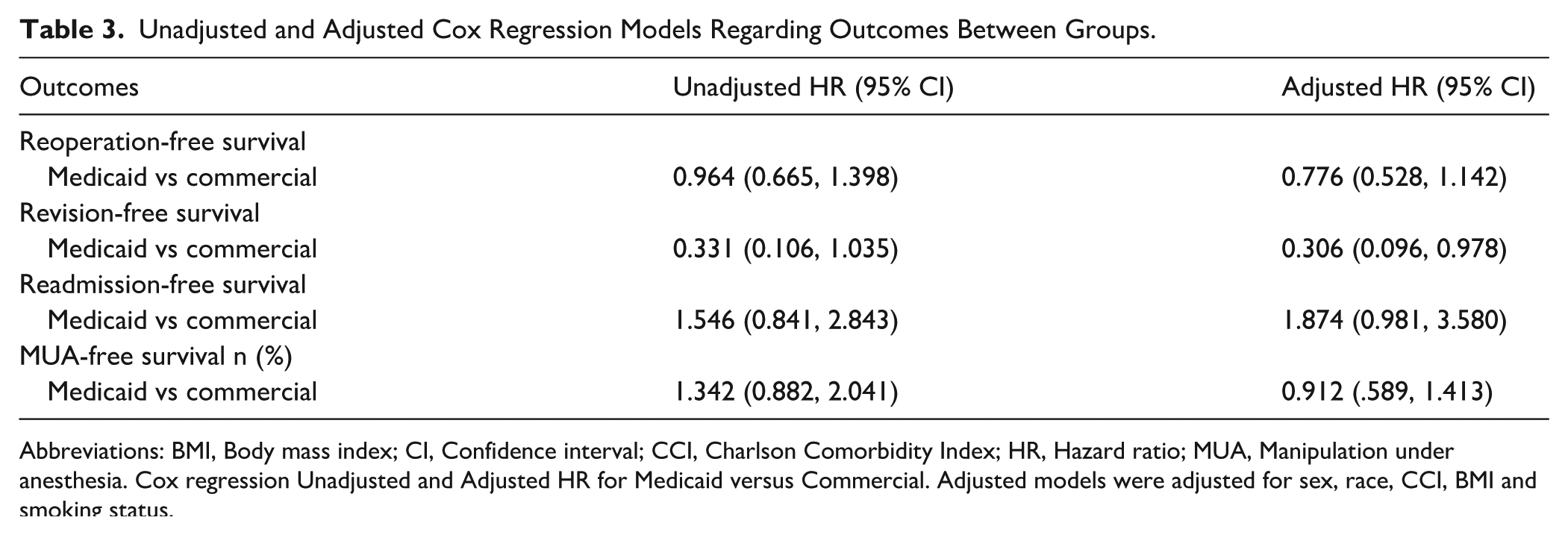
Abbreviations: BMI, Body mass index; CI, Confidence interval; CCI, Charlson Comorbidity Index; HR, Hazard ratio; MUA, Manipulation under anesthesia. Cox regression Unadjusted and Adjusted HR for Medicaid versus Commercial. Adjusted models were adjusted for sex, race, CCI, BMI and smoking status.
Medicaid insurance was associated with greater revision-free survival after adjustment for covariates (adjusted HR 0.306; 95% CI 0.096-0.978). A trend toward lower readmission-free survival was observed in the Medicaid cohort compared with the commercially insured cohort, although this did not reach statistical significance (adjusted HR 1.87; 95% CI 0.981-3.580).
Preoperative KOOS, JR scores were significantly lower in Medicaid patients compared with commercially insured patients (35.7 vs 48.0, P < .0001; Table 2). At 6 weeks postoperatively, Medicaid patients demonstrated a greater mean improvement from baseline compared with commercially insured patients (23.4 vs 13.3 points, respectively).
At both 1- and 2-year postoperative follow-up, commercially insured patients had statistically significantly higher KOOS, JR scores compared with Medicaid patients. However, the absolute differences in KOOS, JR scores at these time points did not exceed the previously established MCID of 12 points, indicating that these differences were not clinically meaningful. Both insurance groups demonstrated substantial improvement in knee pain and function following TKA during the first 2 postoperative years.
Discussion
The findings of this retrospective cohort study suggest that Medicaid and commercially insured patients experience similar revision, reoperation, and readmission rates after unilateral TKA performed by arthroplasty fellowship-trained surgeons at a high-volume center. Additionally, our findings suggest that Medicaid patients experience clinically significant improvement in KOOS, JR after TKA, comparable to commercially insured patients.
This study has several limitations. Studies assessing the risk of revision TKA require large sample sizes, often addressed in the form of database studies. Despite having a large TKA sample size for a single-institution study, our percentage of Medicaid patients relative to the total volume of TKA performed may be lower than other institutions. Additionally, non-English speakers and socioeconomic minorities are less likely to complete PROMs surveys, introducing the possibility of bias in our study. 20 The need for MUA is associated with poor pre-TKA range of motion. 21 It is well documented that Medicaid patients present with more advanced disease and wait longer for surgery, potentially driving higher rates of postoperative MUA, although this was not directly tested in this study. This study also has limitations inherent to retrospective reviews including but not limited to selection bias, information bias, and inability to establish causation. Additionally, conditions like rheumatoid arthritis and HIV can affect results, which may be impacted by medical management with immune-suppressing agents and viral load at the time of surgery. This was not investigated within the study. Lastly, as a single-institution study, including patients operated upon only by fellowship-trained arthroplasty surgeons, the results are not necessarily generalizable.
Our reported TKA survivorship is consistent with previously reported large national registry studies.22,23 In our cohort of 8961 patients, there was improved revision-free survival in Medicaid patients compared to commercially insured patients. Nonetheless, there was no difference in reoperation rates or time to MUA. Rajahraman et al 24 did not find any difference in revision rates or readmission among patients of varying SES at a shorter follow-up of 2 years. In contrast to our findings, a prior systematic review found that patients with Medicaid and Medicare experienced greater morbidity and mortality after total joint arthroplasty when compared to commercially insured patients. 11 Researchers have sought to explore the relationship between insurer status and postoperative complications through national database studies. While these studies benefit from large sample size, these registries are composed of a large proportion of surgeries conducted at low-volume centers. Patients with Medicaid are more likely to receive care from lower-volume surgeons, and this has been linked with higher rates of postoperative complications. 19 Our data suggest that at high-volume TKA centers, clinical outcomes are consistently excellent independent of insurance status. Rajahraman et al 24 focused on a similar population to our study with patients receiving care at a high-volume orthopedic specialty hospital without compromised outcomes in this vulnerable population. Prior studies have also demonstrated comparable outcomes in high-risk TKA patients including those with multiple comorbidities and the morbidly obese when the surgeries are performed at high-volume centers.25,26 Our findings suggest that interventions designed to improve access to orthopedic care should direct patients who are at higher risk for complications (ie, those with more comorbidities and obesity) to specialized centers experienced in managing these patient cohorts, as these centers may be protective against revision rates.
In accordance with prior studies, we found that patients with Medicaid insurance had lower baseline KOOS and JR scores. Suleiman et al 5 revealed that low income was associated with higher radiographic osteoarthritis severity at the time of surgical consultation as measured by the Kellgren-Lawrence grade. In our study, while differences in KOOS and JR scores between the groups were statistically significant, they are not clinically significant as the differences do not meet the MCID score. 27
In conclusion, our retrospective cohort study at a single high-volume orthopedic specialty center found that despite increased comorbidities, higher BMI, and lower SES, Medicaid patients had greater time to revision survival and no difference in time to reoperation and readmission survival. All patients underwent TKA by arthroplasty-fellowship-trained surgeons, which may play a role in explaining the differences found in this study.28,29 Both Medicaid and commercially insured cohorts demonstrated significant improvement in KOOS and JR scores, with Medicaid patients achieving a greater mean improvement at 2 years postoperatively. Prior studies have suggested that higher-volume orthopedic centers are best equipped to reduce complication rates following TKA in Medicaid patients. We found no compromise in outcomes across payer status. This may highlight the value of high-volume orthopedic centers with fellowship-trained arthroplasty surgeons, although future studies designed to assess this relationship are needed.
Supplemental Material
sj-docx-1-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-1-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-2-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-3-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-4-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-5-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-6-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316261456312 – Supplemental material for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution
Supplemental material, sj-docx-7-hss-10.1177_15563316261456312 for Comparable Outcomes After Total Knee Arthroplasty in Medicaid and Commercially Insured Patients at a High-Volume Institution by Andrew J. Sama, Branden Sosa, Nicolas Pascual-Leone, Patricia Friedmann, Michael Parides, Douglas Padgett and Alejandro Leali in HSS Journal®
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was waived from all participants included in this study by the IRB at Hospital for Special Surgery.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors Branden Sosa, MD, and Alejandro Leali, MD, are members of the Editorial Board of HSS Journal. The authors did not take part in the peer review or decision-making process for this submission. Additional potential conflicts of interest include: Douglas Padgett, MD, reports relationships with Enovis, PSI, Journal of Arthroplasty, and Hospital for Special Surgery Board of Trustees. The other authors declare no potential conflicts of interest.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.