
Abstract
Background:
Synovial chondromatosis (SC), a rare disorder characterized by the formation of cartilaginous nodules and intra-articular loose bodies causing pain, swelling, and mobility issues, most often affects the knee in middle-aged individuals.
Presentation:
After having consulted several specialists, a 13-year-old girl presented for rheumatology evaluation of chronic left ankle pain with no history of trauma. She reported daily pain that was worse in the morning.
Diagnosis:
Differential diagnoses included tenosynovial giant cell tumor, chronic synovitis with rice bodies, SC, and juvenile idiopathic arthritis (JIA). Calcified intra-articular loose bodies were visible on plain radiographs that are not characteristic of the rice bodies seen in JIA and strongly favor SC. Based on the patient’s history, physical examination, imaging (radiographs and magnetic resonance imaging), and histological analysis, a diagnosis of SC of the talonavicular joint was confirmed.
Treatment:
The patient underwent surgical excision; 6 weeks later, she returned for superficial irrigation and debridement for Staphylococcus aureus infection of the surgical wound. At 6 months post-surgical excision, the patient had completed physical therapy and returned to all activities, including sports.
Takeaways:
The authors present the first known pediatric case of primary SC of the talonavicular joint. This report suggests that diagnosis in a child with atraumatic joint pain and swelling should take into account a variety of conditions, especially if the patient has not responded to typical treatments for JIA. It also underscores the need for careful imaging review.
Level of Evidence:
Level V, case report
Introduction
Synovial chondromatosis (SC) is an uncommon condition characterized by progressive synovial proliferation of joints, bursae, and tendon sheaths, resulting in intra- and peri-articular cartilaginous or osteochondral loose bodies. 1 Classically, SC affects adults in the third to sixth decade of life and has a predilection for larger weight-bearing joints, the most common being the knee (70%), hip (20%), shoulder, and elbow. 1 SC commonly arises in a susceptible joint secondary to trauma, osteoarthritis, osteochondritis dissecans, or neuropathic arthropathy. Primary (idiopathic) SC is rare, affecting patients in the 3rd to 4th decade of life. They may be asymptomatic or present with joint pain, crepitus, locking, swelling, or reduced range of motion. 2 Prompt identification and treatment can prevent adverse sequelae, including chronic pain and irreversible joint damage. Expedient treatment may also lower the risk of malignant transformation to chondrosarcoma, which has been reported in approximately 5% of longstanding or recurrent cases. 3 The definitive treatment is loose body removal with possible synovectomy. 4
This report presents the first known case of SC in the talonavicular (TN) joint in a child. The description of this unique pediatric presentation of SC in the midfoot may be helpful for physicians who encounter similar patterns of involvement.
History and Physical Examination
A 13-year-old girl presented with chronic left ankle pain that developed in the spring of 2023. (Written informed consent was obtained from the patient’s family prior to inclusion in this case report.) There was no preceding trauma. She saw a podiatrist, who recommended magnetic resonance imaging (MRI). Although the images and report were not available, family members said the MRI showed “fluid in the joint.” The patient was then referred to a sports medicine physician who, along with her pediatrician, began a workup for inflammatory disease. Tests for antinuclear antibodies, rheumatoid factor, and human leukocyte antigen-B27 were all negative. Because pain and swelling persisted, she was evaluated by a foot and ankle surgeon in October 2023. Although the examination findings were consistent with posterior tibial tendonitis, a repeat MRI was ordered. The results suggested moderate, complex-appearing TN fluid, which was thought to represent chronic synovitis with rice bodies. Based on this, the patient was referred to a rheumatologist. This examination was notable for foot swelling, and the patient was diagnosed with juvenile idiopathic arthritis (JIA, M08.00), enthesitis-related arthritis (M08.80) subtype. She was treated with nonsteroidal anti-inflammatory drugs (NSAIDs) (naproxen and diclofenac) and then sulfasalazine. When symptoms did not improve after 3 months of treatment, and she developed mild, intermittent abdominal pain with NSAIDs, a biologic agent was considered to treat persistent inflammation. At that time, her family sought additional opinions.
When evaluated by rheumatology at our institution, she reported daily pain that was worse in the morning. Initially, the MRI from October 2023 was not available, and so a repeat MRI was ordered in March 2024. It revealed prominent synovial distention of the TN joint recesses, with internal intermediate signal intensity foci suggestive of possible SC (Figures 1 and 2). While the MRI findings could also be consistent with JIA with rice bodies, the localized swelling and lack of treatment response brought this diagnosis into question. There was no blooming artifact suggestive of the hemosiderin deposition seen in tenosynovial giant cell tumor (TGCT, previously known as pigmented villonodular synovitis). When the October 2023 MRI became available, it was retrospectively reviewed. Although the study quality was suboptimal, the radiologist noted features suggestive of SC.
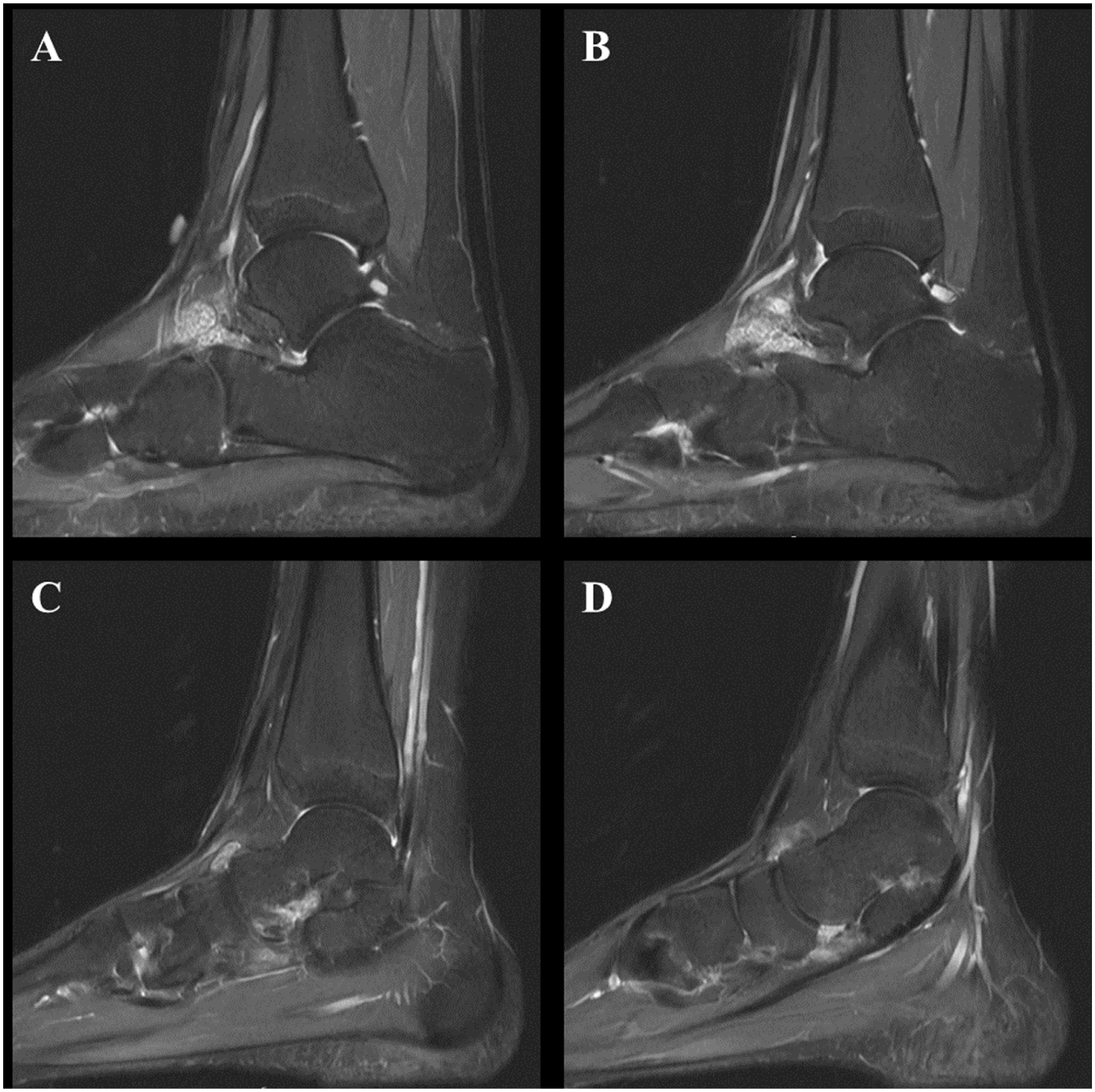
Representative cuts from a sagittal IR MRI series (lateral to medial from A to D) demonstrating synovial distension of the talonavicular joint and intermediate signal intensity foci in the recesses. IR, Inversion recovery; MRI, Magnetic resonance imaging.
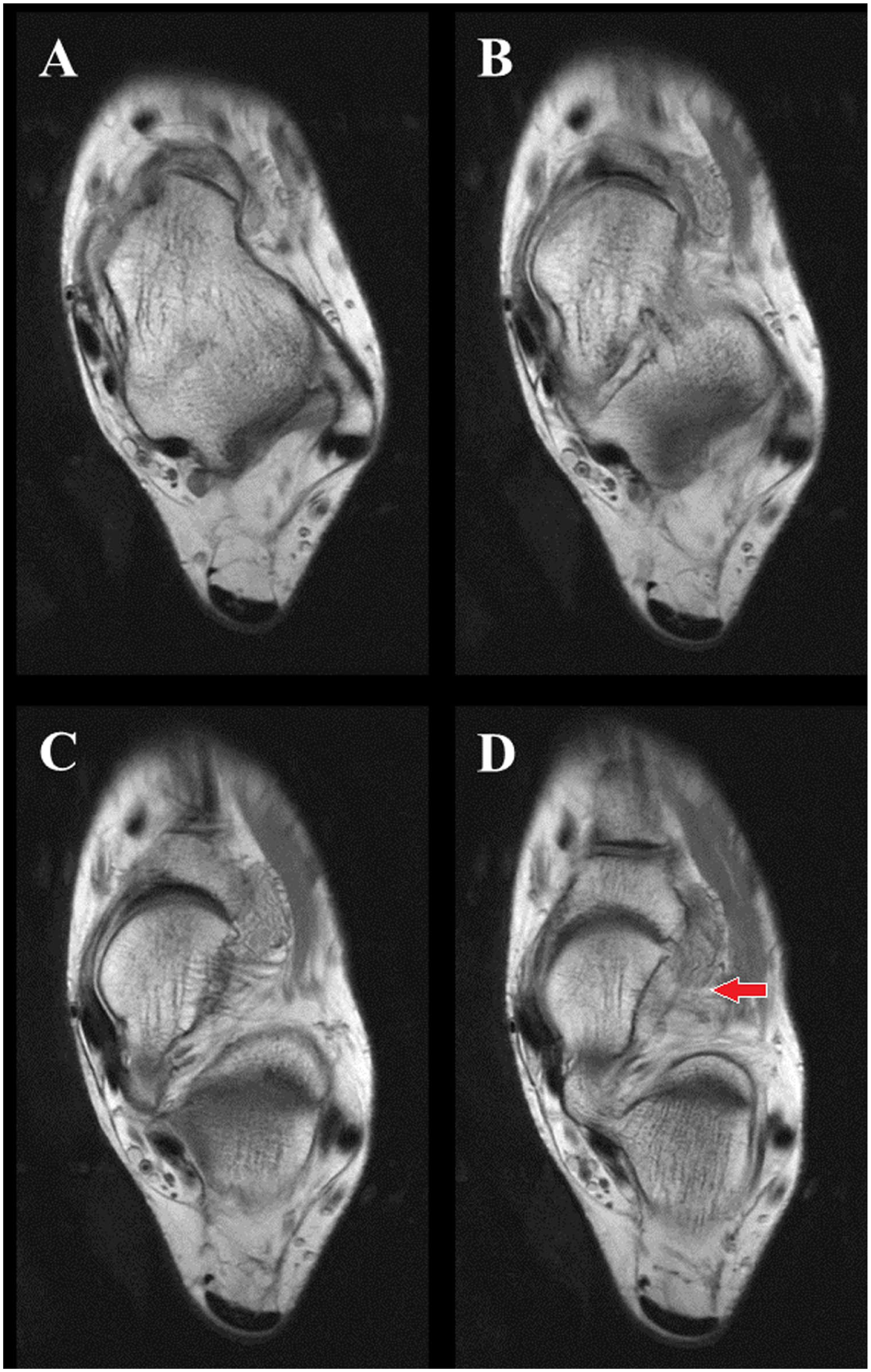
Consecutive slices from an axial PD MRI series (proximal to distal from A to D) demonstrating synovial distension of the talonavicular joint and a grouping of small foci lateral to the joint. PD, Proton density; MRI, Magnetic resonance imaging.
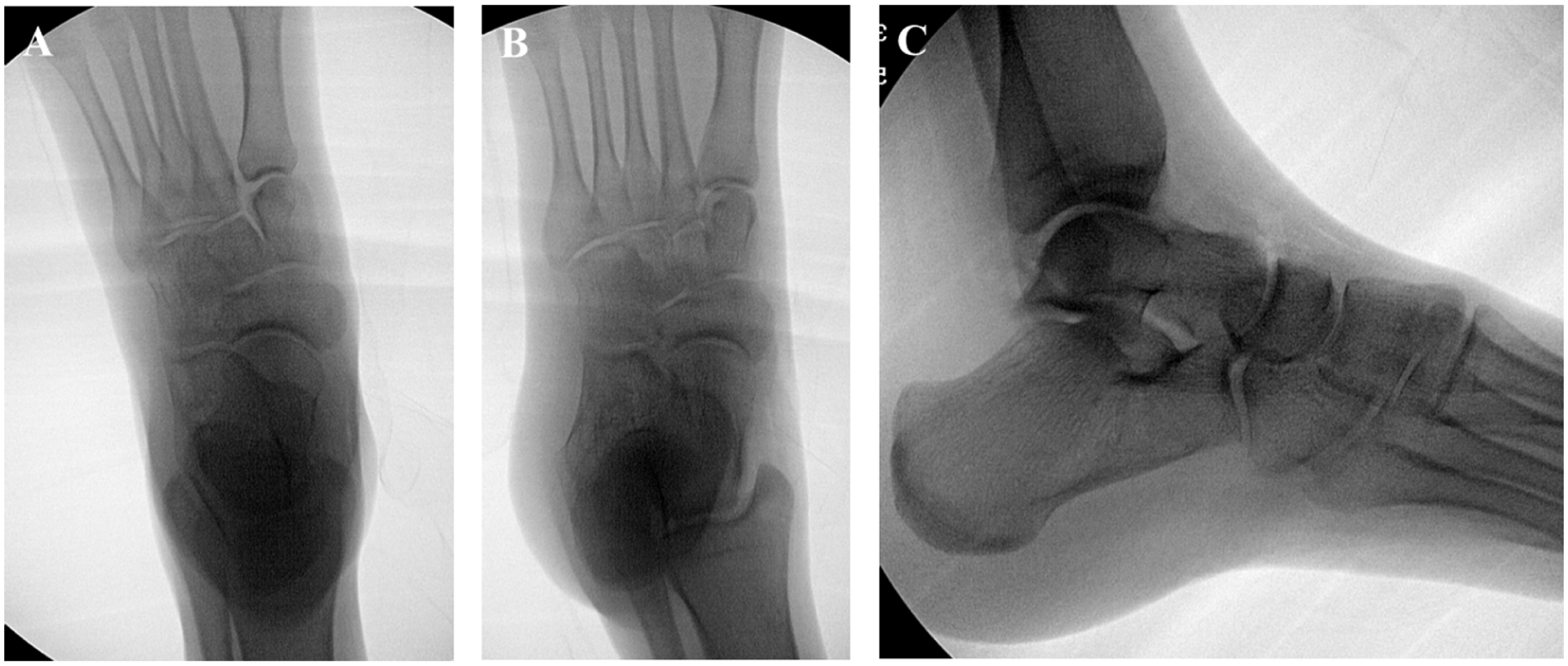
The patient was referred to pediatric orthopedics at our institution; that examination was notable for mild fullness over the medial midfoot/hindfoot and ankle, pain with hindfoot and ankle range of motion, reduced plantarflexion of 20° (compared with 50° in the contralateral ankle), and reduced hindfoot motion (only 5° of inversion/eversion compared to 15° in the contralateral foot). The surgeon obtained plain radiographs and noted calcifications over the talar head and neck (Figure 3).
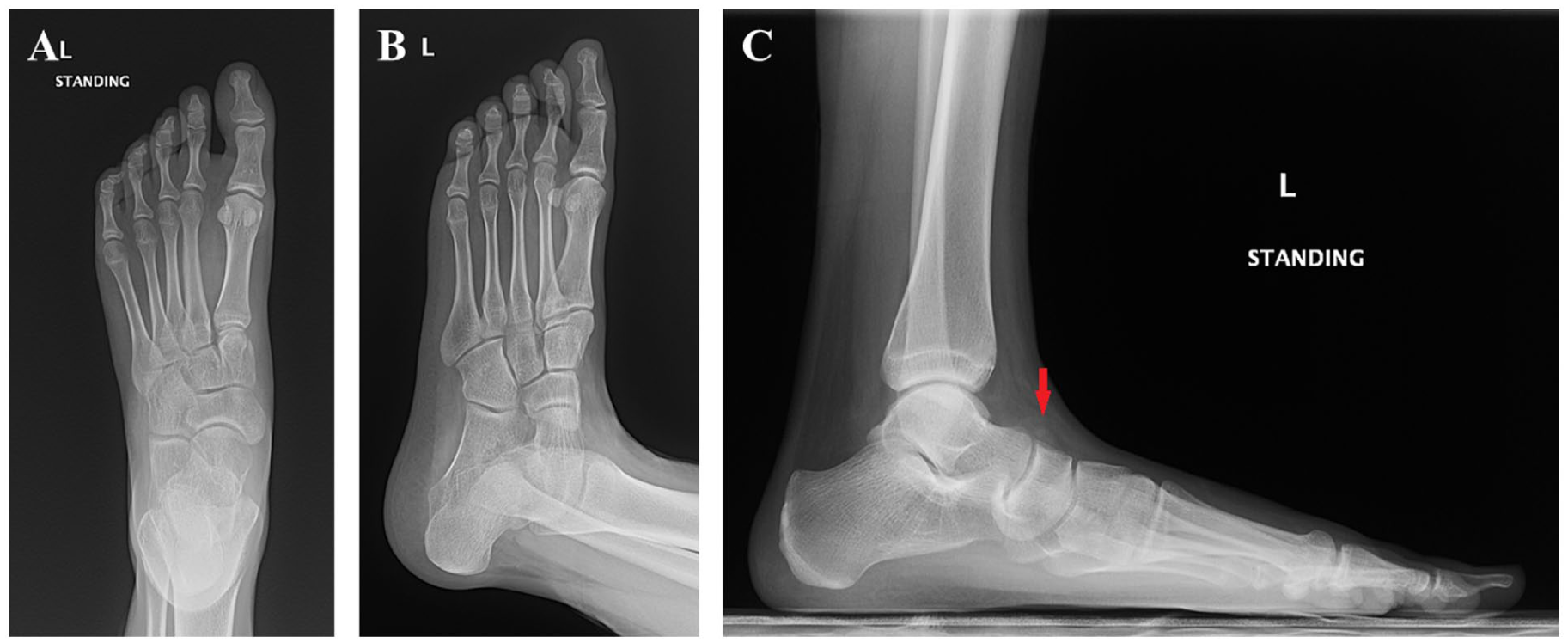
Anteroposterior (A), oblique (B), and lateral (C) plain radiographs of the left foot demonstrating calcifications over the dorsal aspect of the talonavicular joint, best seen on the lateral image (C).
Diagnosis
Giving these findings, other pathologies considered in the differential diagnosis included TGCT, chronic synovitis with rice bodies, SC, and, less likely, JIA. The decision was made to proceed with surgical excision.
The specimen received by pathology was described as “multiple irregular fragments of white and pink-tan rubbery and soft tissue” measuring 2.4 × 2.0 × 0.8 cm in aggregate. Histologically, the synovium was made up of “papillary hypertrophy and slight hyperplasia of the lining layer,” and the superficial stromal elements showed “nonspecific sclerosis with interstitial and perivascular mucoid degeneration.” The free-floating fragments were “hyaline cartilage containing chondrocytes demonstrating a micronodular growth pattern, without significant cytologic atypia or mitotic activity” (Figures 4 and 5). Some of these fragments also showed secondary ossification, and some showed partial surfacing by a synovial lining. No cytologic features concerning for malignancy were identified.
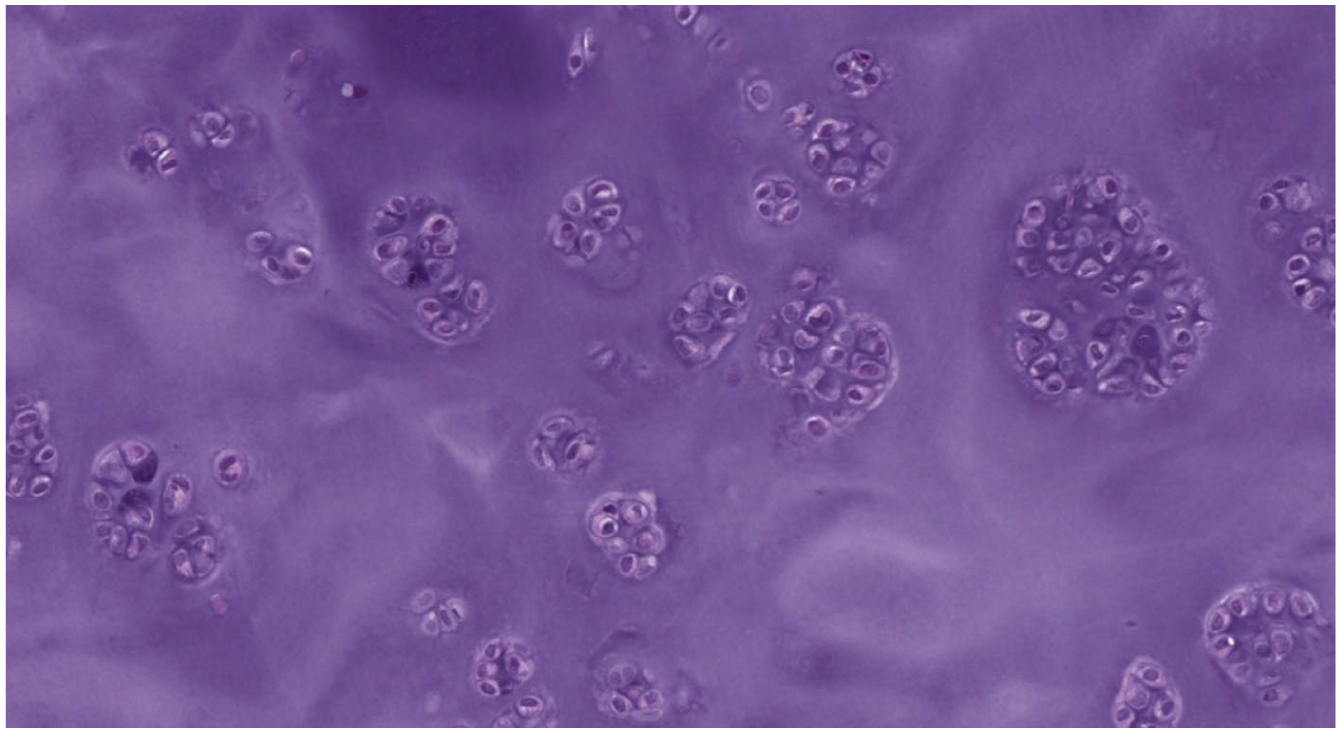
10× single cell: (hematoxylin & eosin, 10×) The image demonstrates clustered proliferations of chondrocytes in abundant hyaline cartilaginous matrix.
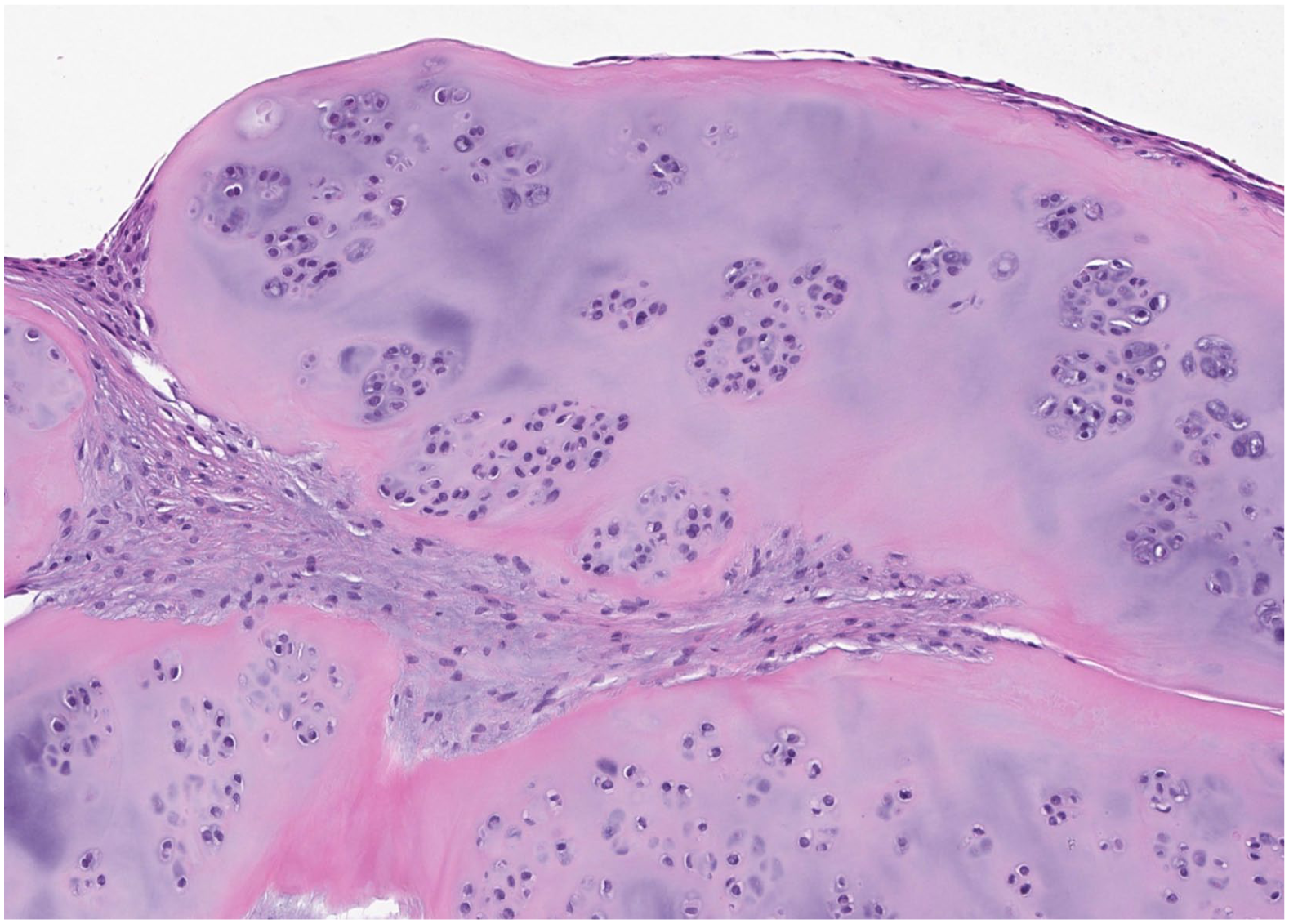
10× attenuated synovium: (hematoxylin & eosin, 10×) The image demonstrates an attenuated synovial lining (top) overlying fibrotic stroma containing several multinodular proliferations of hyaline cartilaginous matrix containing clustered proliferations of chondrocytes.
Based on the patient’s history, physical examination and imaging findings (new plain radiographs along with the MRI), and histological analysis, a diagnosis of SC of the TN joint was confirmed.
Discussion and Treatment
SC is a rare disorder characterized by the formation of cartilaginous nodules resulting in intra-articular loose bodies that can cause pain, swelling, and mobility issues. Most cases are found in the knee and in middle-aged individuals. 5 Etiology is thought to be metaplastic transformation of synovial cells; however, it is still not fully understood. 6 Early intervention can prevent long-term sequalae, including pain, joint degradation, and possible transformation to chondrosarcoma. 3 Although talonavicular SC has been described in rare adult cases treated with surgical excision, these reports did not describe the diagnostic challenge presented here, in which the pediatric presentation initially raised concern for JIA.7,8 To our knowledge, this is the first case report describing SC of the TN joint in a child.
The original diagnosis based on the initial evaluation of this case was JIA, a heterogeneous group of disorders that cause chronic inflammatory arthritis in childhood. Because this is a clinical diagnosis, laboratory testing may be normal. Imaging—including plain radiographs, ultrasound, or MRI—can help support the diagnosis. Typically, JIA is characterized by marked synovial lining hyperplasia with villous hypertrophy and dense inflammatory infiltrates composed of T and B lymphocytes, plasma cells, macrophages, and dendritic cells. Increased vascular proliferation and endothelial activation are also commonly observed, reflecting chronic synovial inflammation. 9 Plain films can show osteopenia, joint space narrowing, and bony erosions. Rice bodies, free bodies of synovial origin with a cartilage-like appearance, are indicative of chronic synovitis and can be present in cases of JIA (Figures 6-8). MRI findings of unmineralized nodules that demonstrate typical chondroid signal characteristics 10 may be similar to those in SC. However, it is important to note that rice bodies are not typically calcified and, therefore, are not often visible on plain X-ray. Therefore, the intra-articular calcifications present on plain films in this case were unlikely to be caused by JIA.
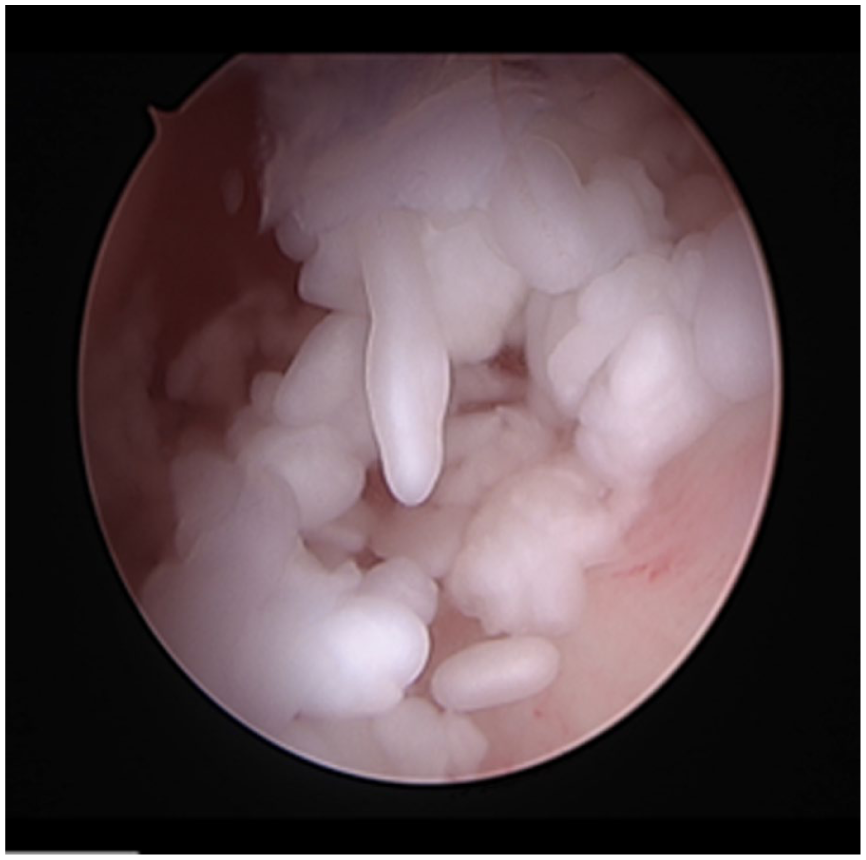
Arthroscopic imaging of rice bodies.
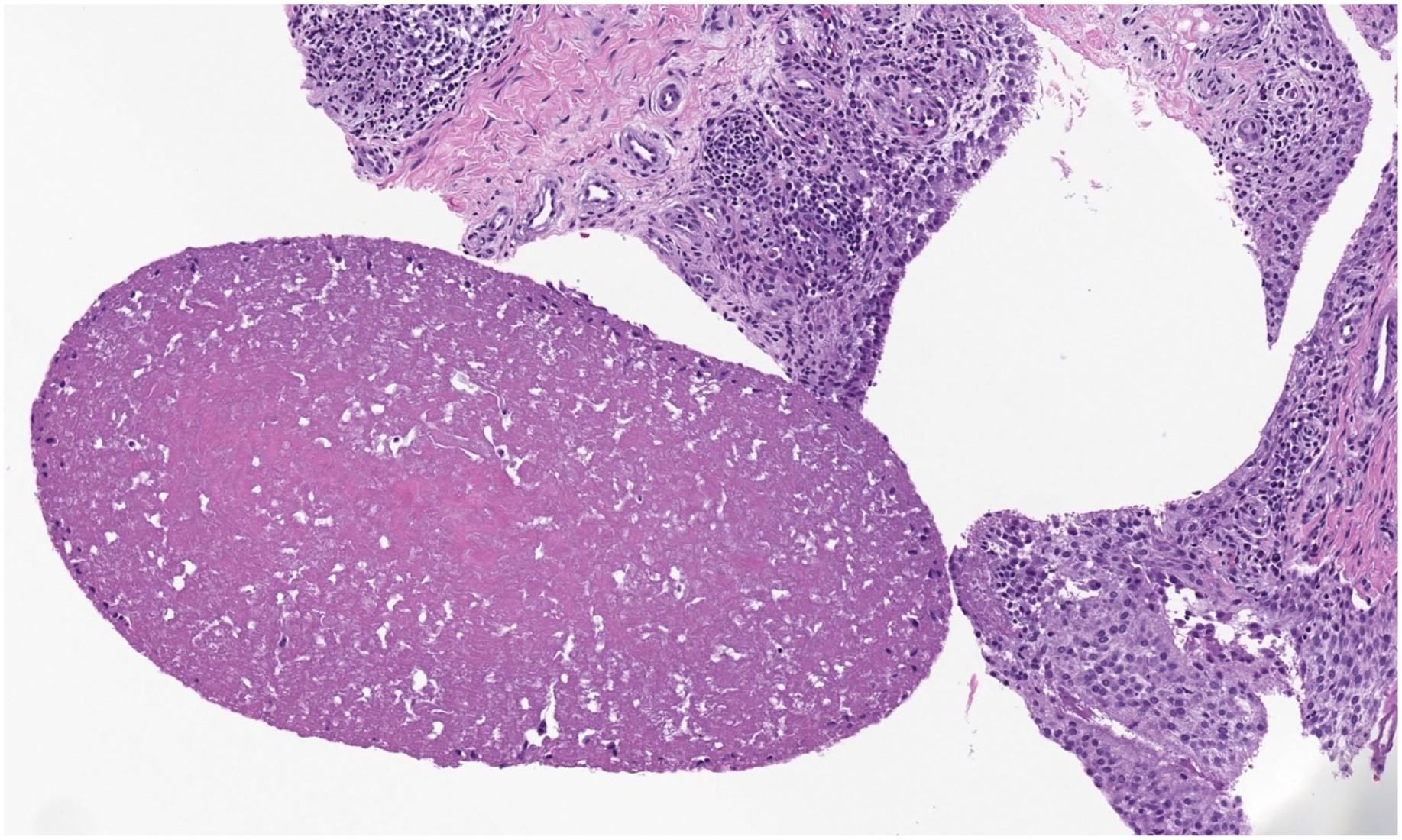
Pathology of rice bodies. Synovial hyperplasia with fibrinous loose bodies.

Sagittal T2-weighted MRI sequence of the left knee demonstrates scattered tiny intra-articular bodies in a “rice body” appearance throughout the joint. There is mass-like hypertrophied synovium along the popliteus hiatus with very mild chondral thinning over the medial compartment and free edge blunting of the medial meniscus. MRI, Magnetic resonance imaging.
Diagnostic distinction between the 2 conditions is critical because the treatment is radically different. Whereas the mainstay treatment for JIA is medication (conventional and biologic disease-modifying agents), treatment for SC is typically surgical resection. The risk of recurrence after excision is reported to be between 3% and 24% 11 ; however, there is a lack of evidence, especially in pediatric patients, due to the rarity of the condition. There is also a risk of future arthrosis that could cause pain or loss of range of motion. If severe, treatment could require an arthrodesis of the joint. The decision was made to proceed with surgical excision and pathologic analysis.
Surgical Technique and Follow-Up
A longitudinal incision was made over the dorsal midfoot, lateral to the TN joint and the extensor tendons. The interval between the extensor tendons and the extensor digitorum brevis was exploited to reach the TN joint. On the superficial aspect of the joint capsule, there was a reddish-white mass surrounded by small, white cartilaginous fragments. The mass was excised, and the TN joint capsule was opened. There was hypertrophic synovium within the joint and cartilaginous fragments filling the joint space (Figure 9). The hypertrophic synovial tissue continued up the talar neck. At this point, an additional longitudinal incision was made dorsal to the tibialis posterior tendon to approach the joint from the medial side. Hypertrophic synovium and cartilaginous fragments, both intra- and extra-articular, were identified on the medial side of the TN joint, as well. Working through both incisions, all visualized hypertrophic synovium was excised, and the joint was copiously irrigated until there were no visible cartilaginous fragments remaining. Fluoroscopy was used to confirm that the dorsal fragments visualized on preoperative radiography had been removed (Figure 10). The wound was copiously irrigated and closed with 3-0 Vicryl subcutaneous sutures and 3-0 nylon horizontal mattress sutures in the skin. The patient was placed in a short leg splint and discharged as non-weight-bearing on postoperative day zero.

Intraoperative photo of a portion of the cartilaginous fragments removed from the talonavicular joint.
Anteroposterior (A), oblique (B), and lateral (C) intraoperative fluoroscopic images of the left foot showing removal of calcifications seen on preoperative radiographs dorsal to the talonavicular joint.
The patient remained non-weight-bearing for 2 weeks in the short leg splint, at which time she was taken out of the splint, sutures were removed, and she transitioned to weight-bearing as tolerated in a walking boot. She began physical therapy, with a focus on gait training, lower extremity strengthening, and conditioning out of the boot. At 6 weeks postoperatively, she returned to the clinic with a concern for a superficial infection of the surgical wound. There was fluctuance, erythema, and swelling at the proximal aspect of the incision. She underwent superficial irrigation and debridement and was discharged the same day, weight-bearing as tolerated. The cultures grew Staphylococcus aureus, and she completed a 10-day course of cephalexin. Sutures were removed at 2 weeks, and the incision healed well without evidence of infection or dehiscence. She continued physical therapy.
By 3 months postoperatively from the excision (6 weeks after the superficial irrigation and debridement), she had completed physical therapy and had returned to all activities, including volleyball. Her ankle range of motion was full and pain free. At 6 months postoperatively, she continued to be pain free and participate in volleyball. Of note, she suffered a gastrocnemius strain in the interim that was unrelated to her surgery.
The patient was contacted 1 year after surgery and reported that she had no joint swelling, pain, or limitation.
Takeaway Lessons
This case highlights the importance of considering alternative conditions when making a diagnosis in a pediatric patient with atraumatic joint pain and swelling, especially if the patient does not respond to typical treatments for JIA. Although rare (no other pediatric cases have been found in the literature of SC of the hindfoot/midfoot), SC should remain in the differential diagnosis for isolated, persistent monoarticular swelling, especially if laboratory evaluation for inflammatory arthritis is negative and response to typical medical treatment is limited.
This case also underlines the importance of careful imaging review. Calcified intra-articular loose bodies visible on plain radiographs strongly favor SC and are not characteristic of rice bodies seen in JIA. Earlier recognition of these calcifications, along with critical reassessment of MRI findings, may have prompted surgical referral sooner and prevented prolonged exposure to anti-inflammatory and disease-modifying medications. We hope this case leads others to consider SC as a diagnosis in a child with isolated ankle/foot swelling, particularly 1 that is refractory to traditional JIA treatment.
What to Read Next
Supplemental Material
sj-docx-1-hss-10.1177_15563316261457143 – Supplemental material for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child
Supplemental material, sj-docx-1-hss-10.1177_15563316261457143 for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child by Julia Klauss, Taylor Cogsil, Mark F. Megerian, Daniel Ramirez, David M. Scher and Karen B. Onel in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316261457143 – Supplemental material for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child
Supplemental material, sj-docx-2-hss-10.1177_15563316261457143 for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child by Julia Klauss, Taylor Cogsil, Mark F. Megerian, Daniel Ramirez, David M. Scher and Karen B. Onel in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316261457143 – Supplemental material for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child
Supplemental material, sj-docx-3-hss-10.1177_15563316261457143 for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child by Julia Klauss, Taylor Cogsil, Mark F. Megerian, Daniel Ramirez, David M. Scher and Karen B. Onel in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316261457143 – Supplemental material for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child
Supplemental material, sj-docx-4-hss-10.1177_15563316261457143 for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child by Julia Klauss, Taylor Cogsil, Mark F. Megerian, Daniel Ramirez, David M. Scher and Karen B. Onel in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316261457143 – Supplemental material for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child
Supplemental material, sj-docx-5-hss-10.1177_15563316261457143 for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child by Julia Klauss, Taylor Cogsil, Mark F. Megerian, Daniel Ramirez, David M. Scher and Karen B. Onel in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316261457143 – Supplemental material for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child
Supplemental material, sj-docx-6-hss-10.1177_15563316261457143 for Diagnostic Assessment and Surgical Management of Synovial Chondromatosis of the Midfoot in a 13-Year-Old Child by Julia Klauss, Taylor Cogsil, Mark F. Megerian, Daniel Ramirez, David M. Scher and Karen B. Onel in HSS Journal®
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was obtained from the family of the patient included in this case report per the IRB at the Hospital for Special Surgery.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.