
Abstract
Background:
The short-term efficacy of hip arthroscopy as a salvage procedure for acetabular dysplasia and concomitant femoroacetabular impingement syndrome (FAIS) in patients who are not candidates for periacetabular osteotomy remains unclear.
Purposes:
We sought to compare 2-year patient-reported outcome measures (PROMs) after hip arthroscopy for FAIS (control group) versus FAIS with acetabular dysplasia (dysplasia group) in patients over 40 years of age and/or with mild osteoarthritis (OA). We also sought to measure the rate of subsequent total hip arthroplasty (THA) on the same operative hip.
Methods:
We retrospectively reviewed prospectively collected data from patients who underwent hip arthroscopy for FAIS by a single surgeon between January 2021 and December 2024. Fourteen patients in the dysplasia group (mean lateral center-edge angle <23°, range 12-32; anterior center edge angle 20°, range 8-25; age 41.5 ± 11.4 years) and 140 controls (mean age 36.0 ± 12.5 years) were included. We analyzed the European Quality of Life – 5 Dimensions-5 Levels, Mental Health Inventory-5, International Hip Outcome Tool-12 (iHOT-12), Physical Function Short Form of the Hip Disability and Osteoarthritis Outcome Score (HOOS-PS), University of California at Los Angeles (UCLA) Activity Scale, Adult Single Item Measure physical activity, Patient-Acceptable Symptoms State (PASS) single item, and subsequent THA on the same operative hip.
Results:
The dysplasia group demonstrated lower PASS rates, iHOT-12 scores, and HOOS-PS scores compared to controls. THA conversion was higher in the dysplasia group than in the control group (50% vs 5%). In multivariate analysis, dysplasia negatively predicted all outcomes. Intraoperatively identified high-grade cartilage defects predicted THA conversion, but none of the PROMs.
Conclusion:
This retrospective case-control study suggests that hip arthroscopy alone for FAIS with acetabular dysplasia in patients over 40 years and/or with mild OA may increase the odds of clinical failure compared to arthroscopy for FAIS without dysplasia. High-grade cartilage defects identified intraoperatively were independent risk factors for conversion to THA regardless of dysplasia status.
Level of Evidence:
Level III: retrospective case-control study.
Introduction
Developmental dysplasia of the hip (DDH) is a congenital abnormality of the hip joint in which the femoral head is not adequately covered by the acetabulum. 1 Severity of DDH is commonly classified by the lateral center-edge angle (LCEA) of Wiberg, which can be measured on an anteroposterior pelvic view radiograph. A normal LCEA is between 25° and 39°; an LCEA between 20° and 25° is considered “borderline” dysplasia, and <20° is considered true dysplasia.2,3
Osteoarthritis (OA) is a common complication of DDH due to the smaller load-bearing area, which in turn results in increased contact pressure on the cartilage, causing degenerative changes. 4 To address this issue, periacetabular osteotomy (PAO) reorients the acetabulum to increase femoral head coverage and is considered a standard treatment for DDH. This procedure not only improves femoral head acetabular coverage, thereby improving gait and pain symptoms, but it also redistributes compressive loads to preserve the cartilage and prevent the early formation of OA. 4 However, timing of a PAO procedure is important; patients who undergo PAO after degenerative changes have begun in the hip have had lower patient-reported outcome measures (PROMs) and higher rates of conversion to total hip arthroplasty (THA). 5 For this reason, degenerative changes in the hip are generally considered a contraindication to PAO. 6
It is not uncommon for patients with DDH to also experience signs and symptoms of femoroacetabular impingement syndrome (FAIS). For example, 1 study found that 47% of patients with a diagnosis of FAIS also had concomitant DDH. 7 Similarly, another study found that between 17% and 23% of patients with hip pain had both radiographic signs of FAIS and DDH.8,9 Hip arthroscopy, when performed as an adjunct to PAO, has been demonstrated to be effective in treating symptomatic FAIS in patients with hip dysplasia.6,10-12 However, in the setting of DDH, the use of hip arthroscopy alone is more controversial. While arthroscopy is an effective treatment for FAIS, it does not alter the pathophysiologic anatomy of hip dysplasia, and symptoms are likely to persist, 13 and degenerative changes will progress. 14
The use of hip arthroscopy alone in patients with true dysplasia (LCEA or anterior center edge angle [ACEA] <20°) is associated with a higher rate of clinical failure and often leads to inferior clinical outcomes.14-17 However, there is a subset of patients who present with hip dysplasia and early osteoarthritic changes but are relatively old (age >40 years) to be a candidate for PAO. These patients have limited surgical options and are considered too young to undergo THA.18,19 A recent study has shown promising results in patients 40 years or older with borderline dysplasia treated solely with hip arthroscopy for FAIS. 20 However, it remains unclear whether there is a role for hip arthroscopy alone as an intermediate step to relieve symptoms prior to THA for patients with true hip dysplasia over age 40 years and/or with early osteoarthritic changes who have declined PAO surgery by open hip preservation surgeons.
We therefore sought to compare 2-year PROMs after hip arthroscopy as well as rates of subsequent THA on the same operative hip in 2 groups: patients who underwent hip arthroscopy for FAIS (control group) versus patients who underwent hip arthroscopy for FAIS with acetabular dysplasia and who were over 40 years of age and/or had mild OA (dysplasia group).
Methods
After obtaining Institutional Review Board approval, we retrospectively reviewed prospectively collected data from patients who underwent hip arthroscopy for FAIS by a single surgeon between January 2021 and December 2024. All participants or their legal guardians, in the case of minors, provided written informed consent prior to participation. Inclusion criteria were patients (1) with a diagnosis of FAIS, (2) between the ages of 14 and 65 years, (3) who were able to complete the study in English, (4) who underwent hip arthroscopy for FAIS between January 2021 and December 2024, and (5) with complete records available, including perioperative examinations and surgical records. Exclusion criteria were patients (1) <14 or >65 years old, (2) who were current prisoners or inmates or those with a conviction and a pending period of incarceration, (3) who underwent hip arthroscopy for diagnoses other than FAIS, or (4) with radiographs judged as Tönnis grade 2 or 3. Data were reviewed to identify patients with a diagnosis of acetabular DDH who did not undergo PAO after hip arthroscopy due to failure to meet established criteria at our institution’s hip preservation center (eg, age over 40 years or evidence of early arthritic change).
A total of 154 patients who were treated with arthroscopy for FAIS were included, 14 in the dysplasia group and 140 without signs of dysplasia (control group; Table 1). The cohort comprised 123 females, ages 14 to 62 years (mean 36.5 ± 12.5), and the mean time from surgery to 2 year PROMs was 2.91 years (± 0.65). In the dysplasia group, LCEA ranged from 12° to 32° (mean 23°) and ACEA from 8° to 25° (mean 20°), while in the control group, LCEA ranged from 26° to 51° (mean 34°) and ACEA from 22° to 59° (mean 35°). A comparison of notable cofounders is displayed in Table 1. Compared to controls, patients with dysplasia had higher rates of tobacco use and high-grade cartilage defects (Outerbridge 3-4), though regression analysis confirmed these were not confounders.
Study Group Characteristics.
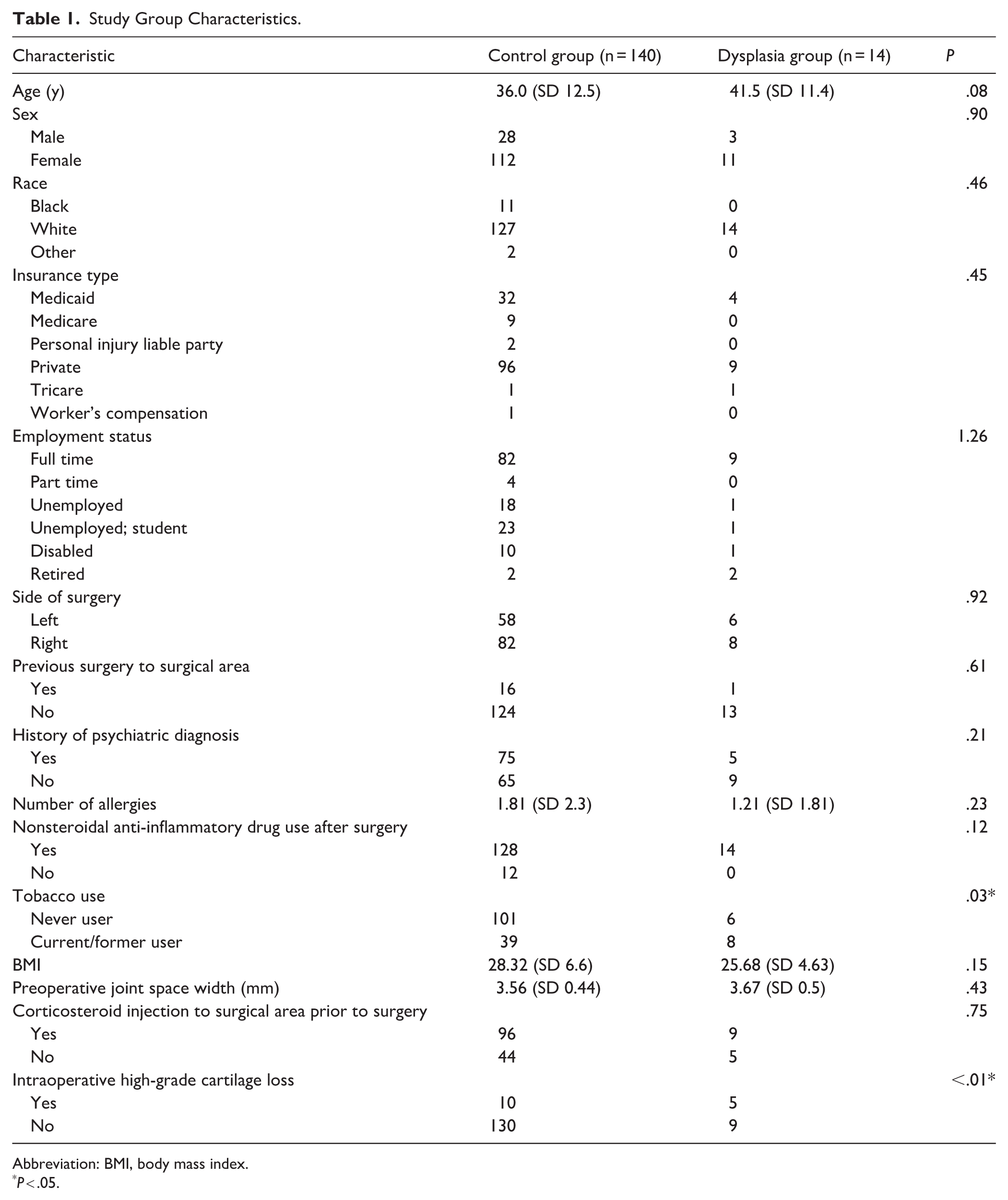
Abbreviation: BMI, body mass index.
P < .05.
Early arthritic change was defined as Tönnis grade 1 OA on radiographs or Tönnis grade 0 OA with superior femoral or acetabular subchondral edema or cystic changes visible on MRI.21,22 Patients were then placed into 1 of 2 groups. Group 1 (control group) consisted of patients who underwent hip arthroscopy for a sole diagnosis of FAIS. Group 2 (dysplasia group) consisted of patients with a diagnosis of both FAIS and acetabular dysplasia who were not candidates for PAO and only underwent hip arthroscopy for treatment of FAIS (Figure 1). Dysplasia was defined by an LCEA or ACEA of <20°. 23 FAIS was defined by the presence of femoral cam morphology (alpha angle >55°) and/or pincer morphology (LCEA or ACEA >40° or a positive crossover sign), together with patient-reported symptoms consistent with hip impingement (eg, groin pain, pain with flexion or rotation, mechanical symptoms, and reproduction of anterior hip pain with flexion, adduction and external rotation and scout test).24-26 Intraoperative assessment of both acetabular and femoral cartilage surfaces was performed with the Outerbridge grading system; for this study, grade 3 and 4 defects were considered to be high-grade defects. 27
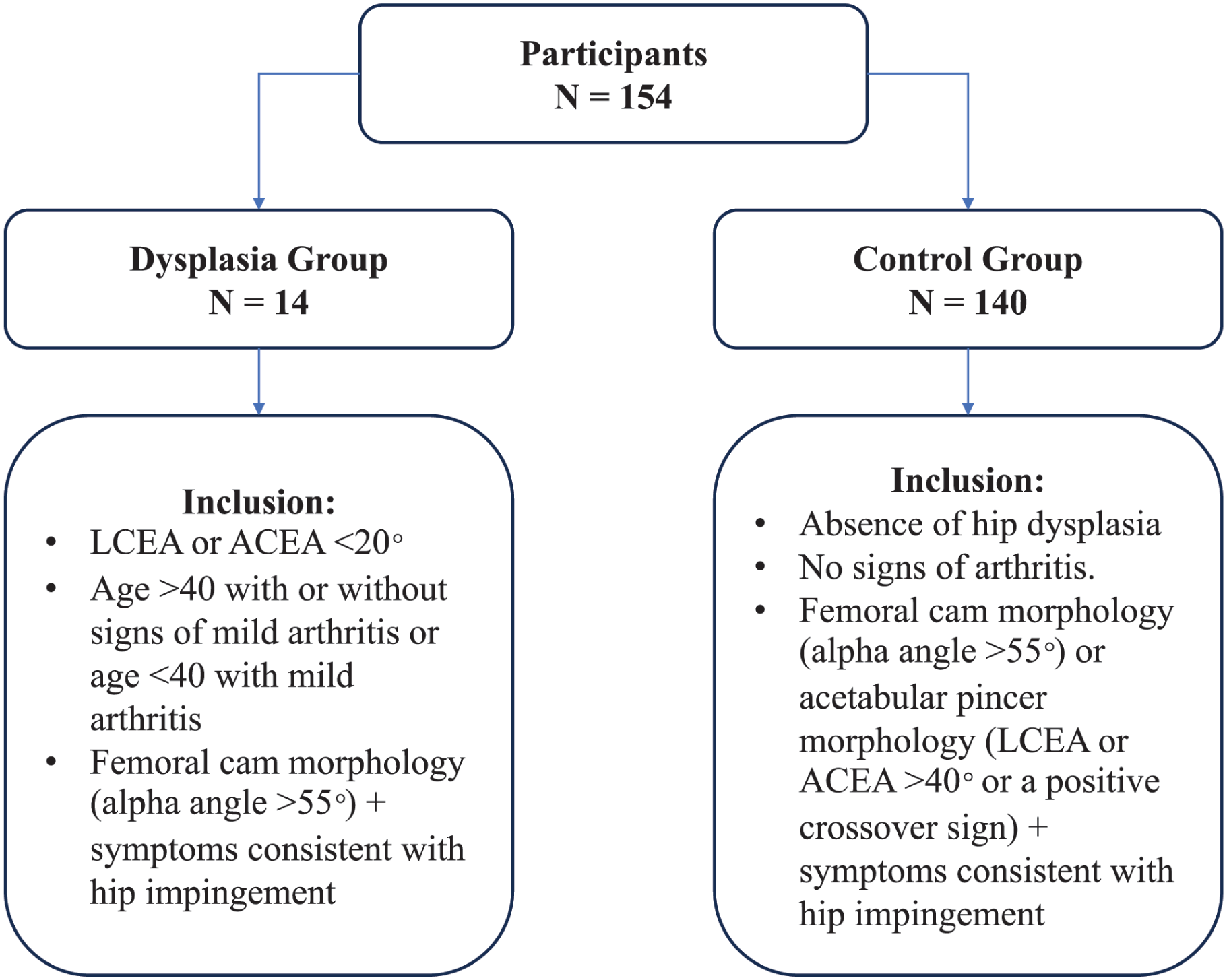
Description of the dysplasia and control groups.
At a minimum 2-year follow-up, postoperative surveys included the following: European Quality of Life – 5 Dimensions-5 Levels (EQ-5D-5L), 28 Mental Health Inventory-5 (MHI-5), 29 International Hip Outcome Tool-12 (iHOT-12), 30 Physical Function Short Form of the Hip Disability and Osteoarthritis Outcome Score (HOOS-PS), 31 UCLA Activity Scale, 32 Adult Single Item Measure physical activity (SIM PA),33,34 Patient-Acceptable Symptoms State (PASS) single item, and subsequent THA on the same operative hip. For our study, clinical failure was defined as either a primary outcome measure that failed to achieve PASS or a need for conversion to THA on the same hip. Secondary outcome measures were postoperative EQ-5D-5L, MHI-5, iHOT-12, HOOS-PS, UCLA Activity Scale, and adult SIM PA scores.
Statistical Analysis
Statistical analysis was performed with a standard software package (JMP 17.2; SAS Institute). A power analysis was performed for the outcomes of interest (2 year postoperative iHOT-12 scores, HOOS-PS scores, rate of PASS, and rate of conversion to THA). The substantial clinical benefit threshold was selected to define a clinically meaningful difference between groups. There is no reported clinically important difference in rates of conversion to THA or achievement of PASS for FAIS or hip dysplasia. We believe any difference in THA or PASS rates exceeding 25% is clinically meaningful. The current study sample is adequate to detect these clinically meaningful differences with >80% power and α of .05. Bivariate statistics were generated with the presence or absence of acetabular dysplasia as the dependent variable. Further comparison was made according to the presence or absence of high-grade cartilage loss seen intraoperatively via χ2 analysis for categorical variables and analysis of variance (ANOVA) for continuous variables. A least significant difference post-hoc analysis was performed following ANOVA to identify which group means differed significantly from each other. Multivariate regression analyses were performed with PROMs (EQ-5D-5L, iHOT-12, HOOS-PS, PASS) and subsequent THA as the outcomes of interest. In the multivariate analysis, a forward selection method was utilized with the inclusion of any covariate (in decreasing order of effect size) that was a significant independent predictor of the outcome or that resulted in a 20% or greater change in effect size for the presence of dysplasia as a predictor of the outcome of interest. The presence of dysplasia had forced inclusion in the multivariate regression models regardless of significance level.
Results
The dysplasia group performed worse in all primary and secondary outcomes (Table 2). PASS was achieved by 55% of controls versus 14% of dysplasia patients (P < .01; OR 7.3; 95% CI [1.5-34.0]). At 2-year follow-up, THA conversion occurred in 50% of dysplasia patients versus 5% of controls (P < .001; OR 19.0; 95% CI [5.27-72.65]). Dysplasia patients also had lower mean iHOT-12 (38.1 vs 61.4, P = .03) and HOOS-PS scores (50.6 vs 70.1, P = .03). EQ-5D-5L scores were worse in the dysplasia group than in the control group (13.8 vs 9.4, P = .014), while MHI-5, UCLA activity, and adult-SIM PA scores were not significantly different (P > .05).
Two-Year Outcomes.
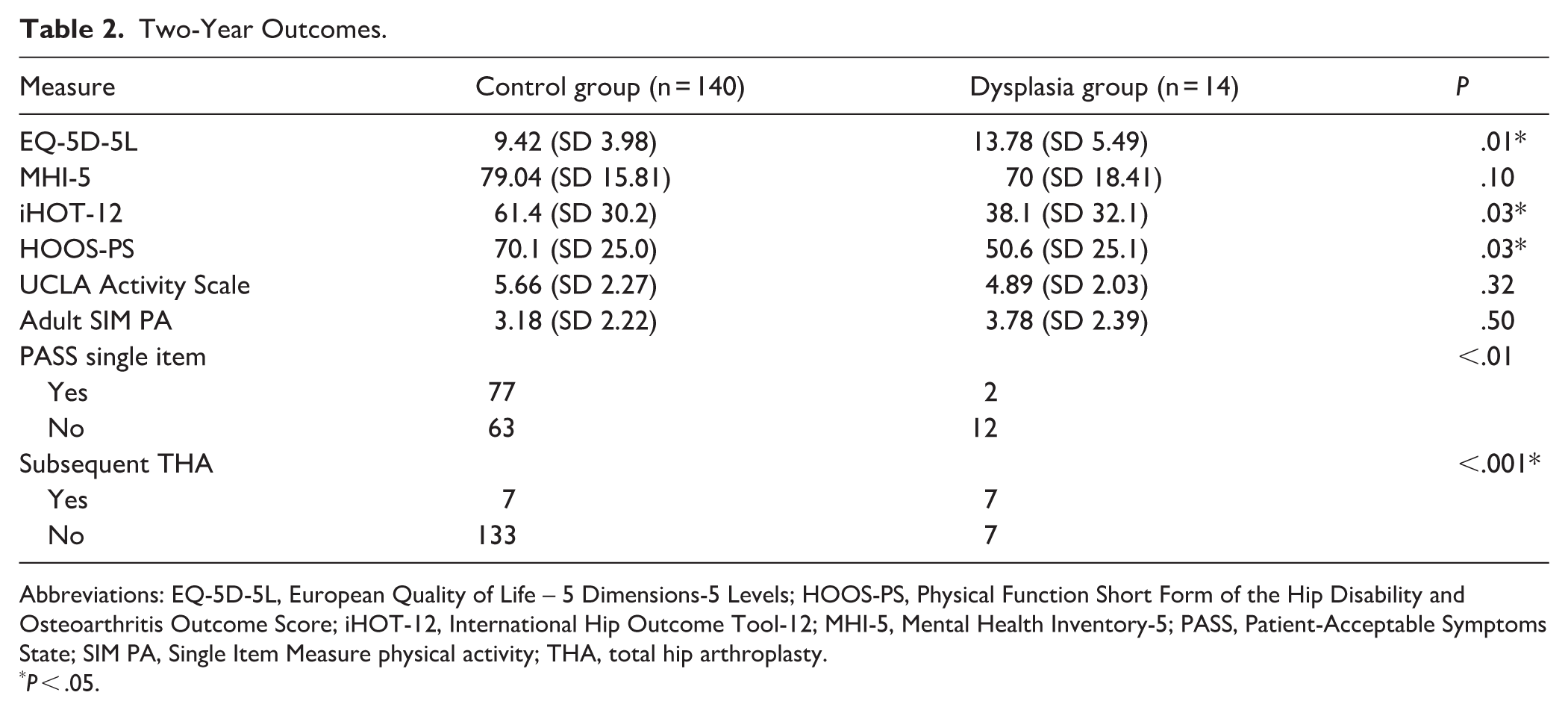
Abbreviations: EQ-5D-5L, European Quality of Life – 5 Dimensions-5 Levels; HOOS-PS, Physical Function Short Form of the Hip Disability and Osteoarthritis Outcome Score; iHOT-12, International Hip Outcome Tool-12; MHI-5, Mental Health Inventory-5; PASS, Patient-Acceptable Symptoms State; SIM PA, Single Item Measure physical activity; THA, total hip arthroplasty.
P < .05.
Among controls, outcomes differed significantly by cartilage defect status (Table 3). THA occurred in 1.5% of controls without defects, 50% of controls with high-grade defects, and 50% of dysplasia patients (P < .001). PASS and HOOS-PS were also worse in those with cartilage defects. Although ANOVA showed no overall difference in iHOT-12 (P = .08), post-hoc testing revealed significantly lower scores in dysplasia patients compared to controls without high-grade defects (P = .03).
Two Year Outcomes, Sub-Group Analysis.
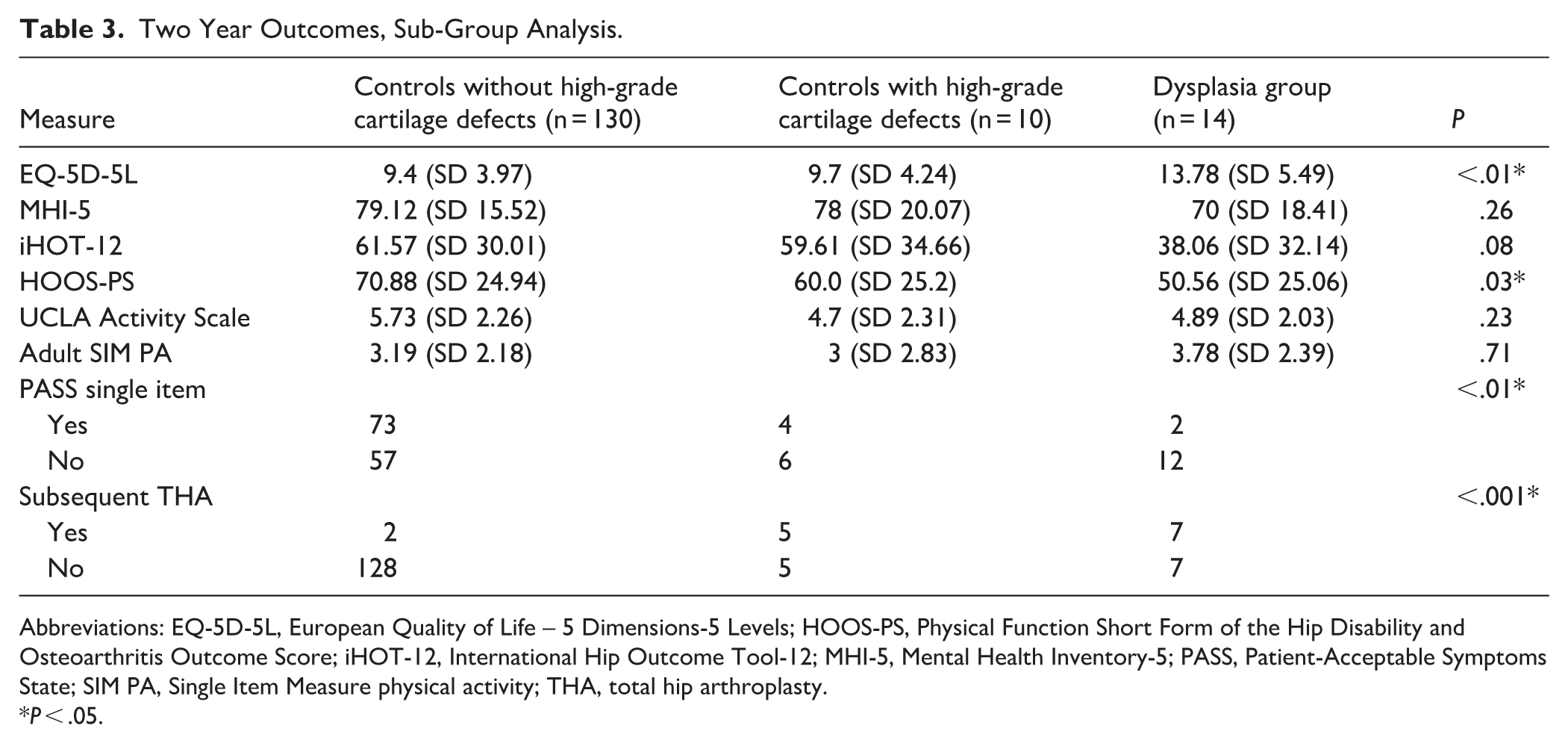
Abbreviations: EQ-5D-5L, European Quality of Life – 5 Dimensions-5 Levels; HOOS-PS, Physical Function Short Form of the Hip Disability and Osteoarthritis Outcome Score; iHOT-12, International Hip Outcome Tool-12; MHI-5, Mental Health Inventory-5; PASS, Patient-Acceptable Symptoms State; SIM PA, Single Item Measure physical activity; THA, total hip arthroplasty.
P < .05.
After multivariate analysis, dysplasia remained an independent risk factor for all outcome measures (Table 4). High-grade cartilage defects independently predicted worse HOOS-PS, lower PASS rates, and higher THA conversion rate, but not iHOT-12 scores. Tobacco use was associated with worse iHOT-12 and HOOS-PS, while higher body mass index (BMI) predicted worse iHOT-12 and HOOS-PS, but did not affect PASS or THA. BMI did not meet criteria as a confounder (>20% change in effect size) and was excluded from final models for PASS and THA.
Independent Predictors of Survey Outcome Measures.
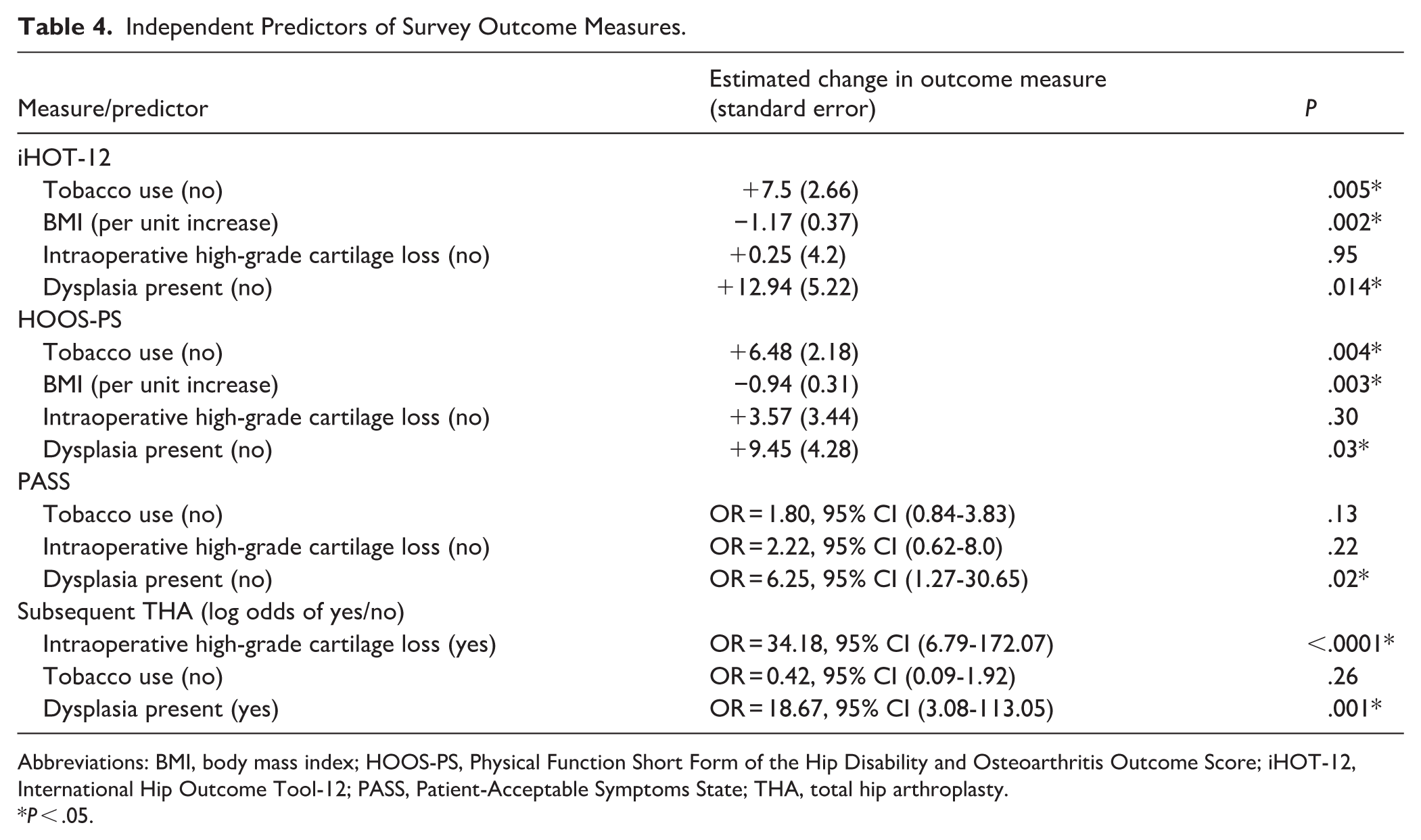
Abbreviations: BMI, body mass index; HOOS-PS, Physical Function Short Form of the Hip Disability and Osteoarthritis Outcome Score; iHOT-12, International Hip Outcome Tool-12; PASS, Patient-Acceptable Symptoms State; THA, total hip arthroplasty.
P < .05.
Discussion
The primary finding of this study was that patients with concomitant FAIS and acetabular dysplasia, particularly those over 40 years of age or with mild radiographic OA, had poor outcomes after undergoing a hip arthroscopy alone. Compared with non-dysplastic patients, those with dysplasia had a 41% lower PASS rate and a 19-fold greater odds of THA within 2 years. These results suggest the possibility of a high failure rate with arthroscopy alone in dysplastic patients and raise questions about whether it should be considered only when combined with PAO in age-appropriate patients.
This study had several limitations. Though intraoperatively identified high-grade cartilage defects are an important independent predictor of several outcome measures, the study was underpowered to assess these relationships. Furthermore, as a retrospective analysis of prospectively collected data, this study design had inherent bias. Preoperative iHOT-12 and HOOS-PS were not available, preventing consideration of preoperative symptom state as a predictor of the outcome measures of interest. Rates of conversion to THA may be influenced by regional practices among arthroplasty surgeons, and the conversion rates reported in the current study may not be generalizable to other geographic areas.
In our study, only 16.7% of dysplastic patients achieved PASS at 2 years compared to 55% of non-dysplastic patients. The PASS rate in non-dysplastic patients was consistent with prior reports of outcomes after hip arthroscopy for FAIS. 35 The low rate among dysplastic patients may be explained, in part, by instability created during capsulotomy. While capsulotomy is necessary to access the hip joint, it can lead to postoperative microinstability, often presenting as persistent pain. 36 Given the underlying instability from reduced acetabular coverage in dysplasia, when it is not surgically addressed, capsulotomy may further predispose these patients to ongoing symptoms. 2 Although cadaveric studies show that capsular repair can restore mechanical function, patients with unhealed or partially healed capsules after hip arthroscopy for hip dysplasia have inferior PROMs.37-39 Another explanation may involve the presence of arthritis. More than half of the dysplastic patients in our study (55.6%) had arthritic changes at surgery. Prior literature has linked OA to inferior arthroscopy outcomes in FAIS, 40 likely related to cellular-level inflammatory changes. 41 Synovial inflammation and associated cytokines sensitize nociceptors, contributing to pain. 41 Even in the absence of radiographic OA, elevated pro-inflammatory cytokines such as IL-6 have been implicated in postoperative pain, inflammation, and tissue trauma. 42 In our subgroup analysis, both dysplastic patients and controls with OA had significantly lower PASS rates (P = .006) and higher THA conversion rates (P < .0001) than controls without OA. These findings suggest that the inflammatory cascade triggered by arthroscopy may exacerbate preexisting joint inflammation, leading to worse outcomes in patients with dysplasia or OA.
An important consideration in treating dysplastic patients is that prior hip arthroscopy has been shown to worsen outcomes after subsequent THA, with higher pain levels, inferior PROMs, greater complication rates, and increased risk of revision.43-47 In our study, dysplastic patients with mild arthritic change underwent arthroscopy because they did not meet current guideline thresholds for THA, 48 although 50% required conversion to THA within 2 years, compared with only 5% of non-dysplastic patients. This pattern suggests that arthroscopy not only fails to provide durable relief in this subgroup but may also compromise the success of later arthroplasty. Moreover, this finding has implications for both patients and the healthcare system, as a second surgery incurs added costs and risks. The absence of consensus on how best to manage dysplastic patients with early arthritic change underscores an important gap in current guidelines. Our findings, together with existing evidence, raise the argument that direct THA may be a more effective and definitive treatment strategy, even before arthritis severity has advanced to levels established by present criteria. Revisiting current thresholds and incorporating dysplasia-specific considerations into surgical decision-making may improve long-term outcomes for this high-risk population.
Given our finding of a high rate of clinical failure after hip arthroscopy in dysplastic patients who do not undergo concomitant PAO, we suggest that alternative treatment strategies be considered. Dysplastic hips are prone to accelerated OA progression, and our findings show a markedly higher rate of THA conversion in this population. 4 Thus, we recommend proceeding with THA once symptomatic arthritis develops. We also recognize hesitancy to operate outside guideline criteria and therefore suggest that non-surgical options may also be appropriate. Corticosteroid injections (CSI) are effective for hip pain but are limited by their association with accelerated arthritis and increased infection risk in patients later undergoing THA, necessitating a 3 month delay between CSI and surgery. 49 Intraarticular ketorolac, by contrast, has demonstrated comparable efficacy to CSI but without deleterious effects on cartilage or ligaments, making it a safer long-term option for pain management. 50 Activity modification, particularly reducing high-impact activities, may further delay OA progression. 51 Although PAO in the setting of OA has been avoided due to inferior outcomes and higher THA conversion rates, emerging evidence challenges this paradigm. In comparing patients with Tönnis grade 1 and grade 2 OA who underwent PAO, Zhang et al found no difference in outcomes or THA conversion rates at 5 years. 52 Similarly, recent literature suggests that carefully selected patients over 40 with Tönnis grade 0 to 2 OA may still benefit from PAO.53-55 Notably, Lee et al demonstrated favorable outcomes in patients over 45 years of age when PAO was performed in conjunction with arthroscopy to address intraarticular pathology. 53 These findings suggest that age alone should not preclude PAO and that combined PAO and arthroscopy may offer superior outcomes compared with arthroscopy alone in dysplastic patients with early OA.
In conclusion, the findings of this retrospective case-control study suggest that arthroscopy alone may pose a high risk of clinical failure or conversion to THA in patients with FAIS and concomitant acetabular dysplasia over the age of 40 years and/or with early radiographic OA. We also found that the presence of intraoperatively identified high-grade cartilage defects was associated with increased odds of conversion to THA, regardless of dysplasia status.
Supplemental Material
sj-docx-1-hss-10.1177_15563316261459104 – Supplemental material for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study
Supplemental material, sj-docx-1-hss-10.1177_15563316261459104 for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study by Allison R. Garden, Ameya V. Belamkar, Joshua T. Finerty, Manuel A. Romero-Padron, Nicholas R. Kossoff and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316261459104 – Supplemental material for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study
Supplemental material, sj-docx-2-hss-10.1177_15563316261459104 for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study by Allison R. Garden, Ameya V. Belamkar, Joshua T. Finerty, Manuel A. Romero-Padron, Nicholas R. Kossoff and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316261459104 – Supplemental material for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study
Supplemental material, sj-docx-3-hss-10.1177_15563316261459104 for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study by Allison R. Garden, Ameya V. Belamkar, Joshua T. Finerty, Manuel A. Romero-Padron, Nicholas R. Kossoff and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316261459104 – Supplemental material for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study
Supplemental material, sj-docx-4-hss-10.1177_15563316261459104 for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study by Allison R. Garden, Ameya V. Belamkar, Joshua T. Finerty, Manuel A. Romero-Padron, Nicholas R. Kossoff and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316261459104 – Supplemental material for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study
Supplemental material, sj-docx-5-hss-10.1177_15563316261459104 for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study by Allison R. Garden, Ameya V. Belamkar, Joshua T. Finerty, Manuel A. Romero-Padron, Nicholas R. Kossoff and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316261459104 – Supplemental material for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study
Supplemental material, sj-docx-6-hss-10.1177_15563316261459104 for Hip Arthroscopy Alone for Salvage Treatment of Femoroacetabular Impingement and Concomitant Acetabular Dysplasia Has Poor Outcomes: A Retrospective Case-Control Study by Allison R. Garden, Ameya V. Belamkar, Joshua T. Finerty, Manuel A. Romero-Padron, Nicholas R. Kossoff and Joshua S. Everhart in HSS Journal®
Footnotes
Acknowledgements
The authors acknowledge the patients who participated in this study and took the time to complete the surveys. Their contribution was essential to the success of this research.
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was obtained from all patients or their legal guardians included in this study per the IRB at Indiana University School of Medicine.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.