
Abstract
Background:
Adequate cam resection during hip arthroscopy for femoroacetabular impingement syndrome (FAIS) is necessary to restore femoral head-neck offset while avoiding under- or over-resection. The relationship between the extent of femoroplasty and postoperative patient-reported outcomes remains unclear.
Purpose:
We sought to answer the following questions: What is the association between the extent of cam femoroplasty resection and postoperative improvements? and is a 5% resection threshold associated with improved outcomes?
Methods:
We conducted a retrospective review of patients with adequate acetabular coverage who underwent primary hip arthroscopy with femoroplasty between January 2015 and December 2022 at our institution and had preoperative and 1- and/or 2-year postoperative modified Harris hip score (mHHS) and/or International Hip Outcome Tool (iHOT) scores. We included 400 patients (409 hips; ages 14–50 years). Outcomes included score changes and achievement of minimum clinically important difference (MCID) and substantial clinical benefit (SCB). Postoperative Dunn lateral radiographs quantified femoroplasty by resection depth percentage (resection depth/femoral head diameter), proximal resection angle, and postoperative α angle. Hips were classified as under-resection, neutral (0%–5%), or over-resection (>5%), and differences in outcomes were compared between resection groups. Multivariable regression analyses controlled for demographic, radiographic, and surgical variables.
Results:
Mean resection depth was 4.8%; mean proximal resection angle was 72.6°. No differences were observed in score improvements or MCID/SCB rates between groups with under-resection versus over-resection at 1 or 2 years. Greater resection depth was associated with larger 1-year mHHS and iHOT improvements and independently predicted 1-year iHOT MCID and SCB. Higher proximal resection angle predicted 2-year iHOT MCID.
Conclusion:
In this retrospective, single-institution cohort study, we found that in patients with FAIS, greater femoroplasty depth was associated with improved 1-year clinical outcomes.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Femoroacetabular impingement syndrome (FAIS) is a well-recognized cause of pain that may predispose young, active adults to osteoarthritis. 1 Arthroscopic treatment is a widely accepted approach to alleviate pain and dysfunction while potentially promoting joint preservation.2,3 Femoroplasty, which restores head-neck offset and reduces pathologic impingement, is often involved in the treatment of FAIS. However, over-resection of the cam lesion is a potential complication, as it may compromise femoral head-neck function integrity and hip stability. This risk exists especially with the emphasis on achieving adequate cam resection as data has linked residual cam deformity with revision hip arthroscopy. 4
Limited data exists on the clinical impact of cam over-resection following hip arthroscopy. Mansor et al reviewed preoperative radiographs of a group of patients indicated for revision hip arthroscopy. 5 The authors found that patients presenting with an over-resected cam (defined as >5% of the diameter of the femoral head) tended to have lower patient-reported outcome measures (PROMs). Another study evaluating 26 primary hip arthroscopy patients attempted to quantify the parameters of a cam over-resection and suggested that a resection depth >6% should be avoided, as greater values may affect clinical outcomes. 6 Although the reason for the lower PROMs in these studies is not clear, the suggestion is that there is an increase in hip microinstability or a loss of suction seal. This clinical data is supported by biomechanical data demonstrating reduced hip stability with cam over-resection and with femoral osteochondroplasty in general.7,8 However, an optimal resection depth has not been determined. While caution is commonly exercised regarding acetabuloplasty in the setting of mild acetabular undercoverage, there is less consensus on femoral-side resection in the treatment of FAIS. 9
This study aimed to evaluate the relationship between the extent of cam femoroplasty and postoperative PROMs in a large cohort of patients with FAIS undergoing primary hip arthroscopy. Our primary goal was to determine if a femoroplasty resection depth of ~5% provides for maximum improvement according to 2 following PROMs: the modified Harris hip score (mHHS) and the International Hip Outcome Tool (iHOT).
Methods
After receiving approval from our institutional review board, we used our institutional hip preservation registry to identify patients aged 14 to 50 years old who underwent primary hip arthroscopy between January 2015 and December 2022. Approximately 99% of these were performed by 2 high-volume hip arthroscopy surgeons. We identified 2708 hips and excluded patients without both pre- and postoperative PROMs. Patients had to have postoperative PROMs at 1 or 2 years to be included. Of the remaining 823 hips, we excluded 150 hips due to a lack of preoperative computed tomography (CT) data, 147 hips that did not undergo femoroplasty, 69 hips that we classified as borderline dysplastic (lateral center edge angle [LCEA] ≤25), 34 hips that occurred as a same-day bilateral surgery, and 14 hips for other reasons (past ipsilateral hip surgery, no imaging available, Tonnis grade ≥2 osteoarthritis, frank dysplasia (LCEA <18), etc.). After exclusions, 409 hips (400 patients) were included for analysis and review (Figure 1). Of the 409 hips included, 48% were in female patients (197/409) and the mean age was 29 years (range, 14–50 years).
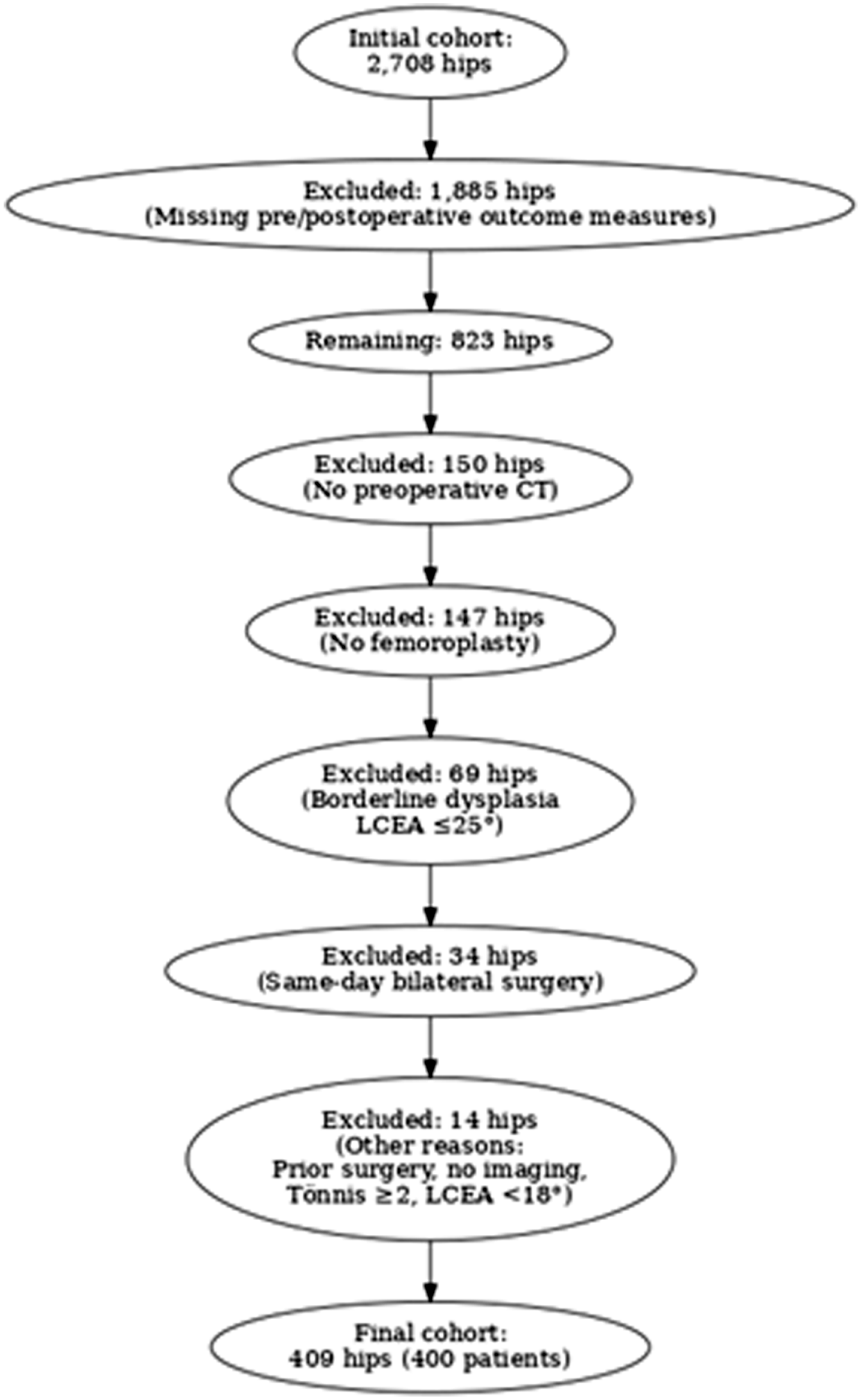
Inclusion/exclusion flow diagram.
Hip arthroscopies were performed supine on a traction table with a post and spinal anesthesia. Entry into the joint was obtained under fluoroscopic guidance, and an anterolateral portal was established, followed by a mid-anterior portal. An interportal capsulotomy was made to gain access to the central compartment, followed by diagnostic arthroscopy. The labrum was evaluated for impingement injury patterns and selectively repaired or debrided. In general, the anchors for the acetabulum were drilled from a distal anterolateral accessory portal. The peripheral compartment was entered, and a T-capsulotomy was performed in almost all patients to adequately visualize any head-neck offset deformity. A subsequent femoroplasty was performed, with attention paid to the femoral and acetabular version to guide the degree of resection. After completion of the femoroplasty, the capsule was routinely closed in an anatomic fashion with multiple non-absorbable sutures in an interrupted fashion.
Postoperative radiographs were reviewed and measurements characterizing the femoroplasty were made on the first available postoperative plain radiograph on the Dunn lateral view. An over-resection was defined as a depth of resection >5% of the diameter of the femoral head, as described by Mansor et al. 5 Resections ranging from 0% to 5% were defined as a neutral resection. Resections that had residual bone outside of a best-fit circle of the femoral head were considered under-resections (Figure 2). Femoroplasty depths were characterized categorically as above. Postoperative α angles were measured in addition to the most proximal extent of the resection (resection angle; Figure 2). Two orthopedic sports medicine fellows (H.P.B. and M.E.U.) and two trained research assistants (A.K.R and A.V.C.) performed these measurements. Inter- and intra-rater reliability was accessed in characterizing resection groups with five unique hips and had perfect accordance (each observer categorized each of the five hips the same as the other observers and the same as themselves in a second observation). PROMs, including the mHHS and iHOT, were collected prospectively using our institution’s electronic data capture system at baseline (preoperatively) and at standardized postoperative follow-up intervals of 1 and 2 years.
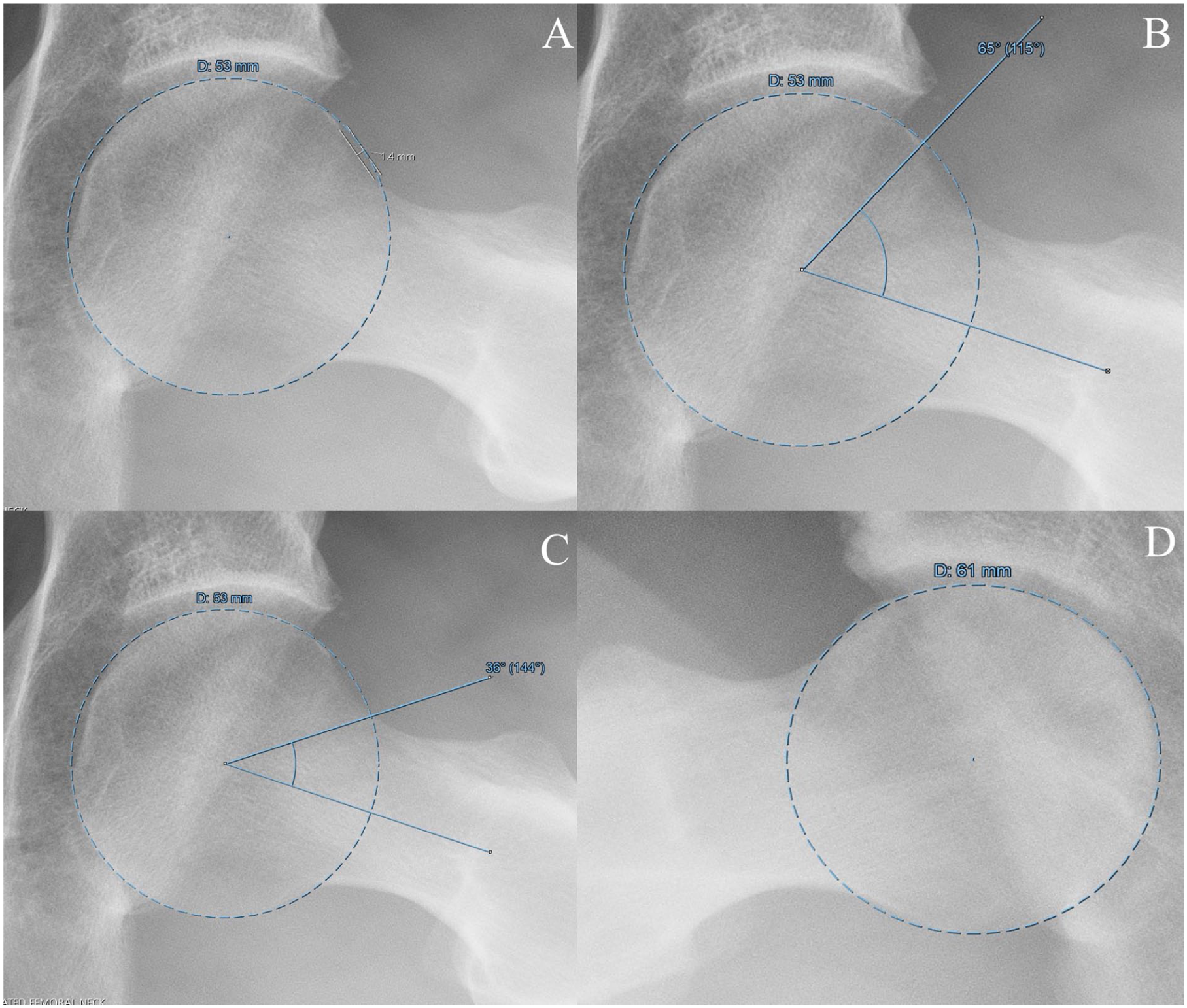
Example radiographic measurements. Resection depth percentage was calculated as the maximum depth of resection divided by the femoral head diameter (A), the most proximal extent of the resection was termed the proximal resection angle (B), postoperative α angle (C), and resections that have residual bone outside of the femoral head circle were considered under-resections (D).
Statistical Analysis
Standard descriptive statistics were performed on patient characteristics, surgical characteristics, the distribution and range of resection depths, and other clinical outcomes and collected variables. The primary outcome scores included the mHHS and the iHOT. While the iHOT-33 was utilized in older portions of our registry before the switch to the iHOT-12, it has been shown that these two measures are interchangeable and thus were treated as the same. 10 The rates of patients meeting a minimum clinically important difference (MCID), substantial clinical benefit (SCB) score, and patient acceptable symptomatic state (PASS) were calculated and based on previously published literature on the topic for 1- and 2-year outcomes. 11 To assess for differences in outcomes between resection groups, we compared 3 groups: under-resection, neutral resection, and over-resection. Additionally, to evaluate a possible depth cutoff other than that suggested by Mansor et al, 5 we performed a separate analysis by defining cam over-resection as a resection depth percentage >7.5% and compared outcomes among the resultant groups. We further grouped hips by proximal resection angle as <65°, 65° to 85°, and >85°. The rationale was to identify a central group of patients around the mean proximal resection angle (±2 SD) and compare the majority of proximal resection angles to the outliers. These data underwent a secondary analysis to lend insight into ideal resection characteristics.
Categorical outcome variables between resection groups were compared utilizing χ2 analyses or Fisher’s exact tests, where applicable. Continuous outcome data between resection groups were compared with Student t-tests for normally distributed data and non-parametric tests for non-normally distributed data. We utilized appropriate regression analyses to study the effect of resection depth on continuous and categorical outcome variables. Within each regression we controlled for age, sex, labral repair, capsular closure, CT-based 3 o’clock acetabular version, CT-based femoral version, preoperative mHHS or iHOT where applicable, resection depth, postoperative α angle, and the resection angle as defined above.
Results
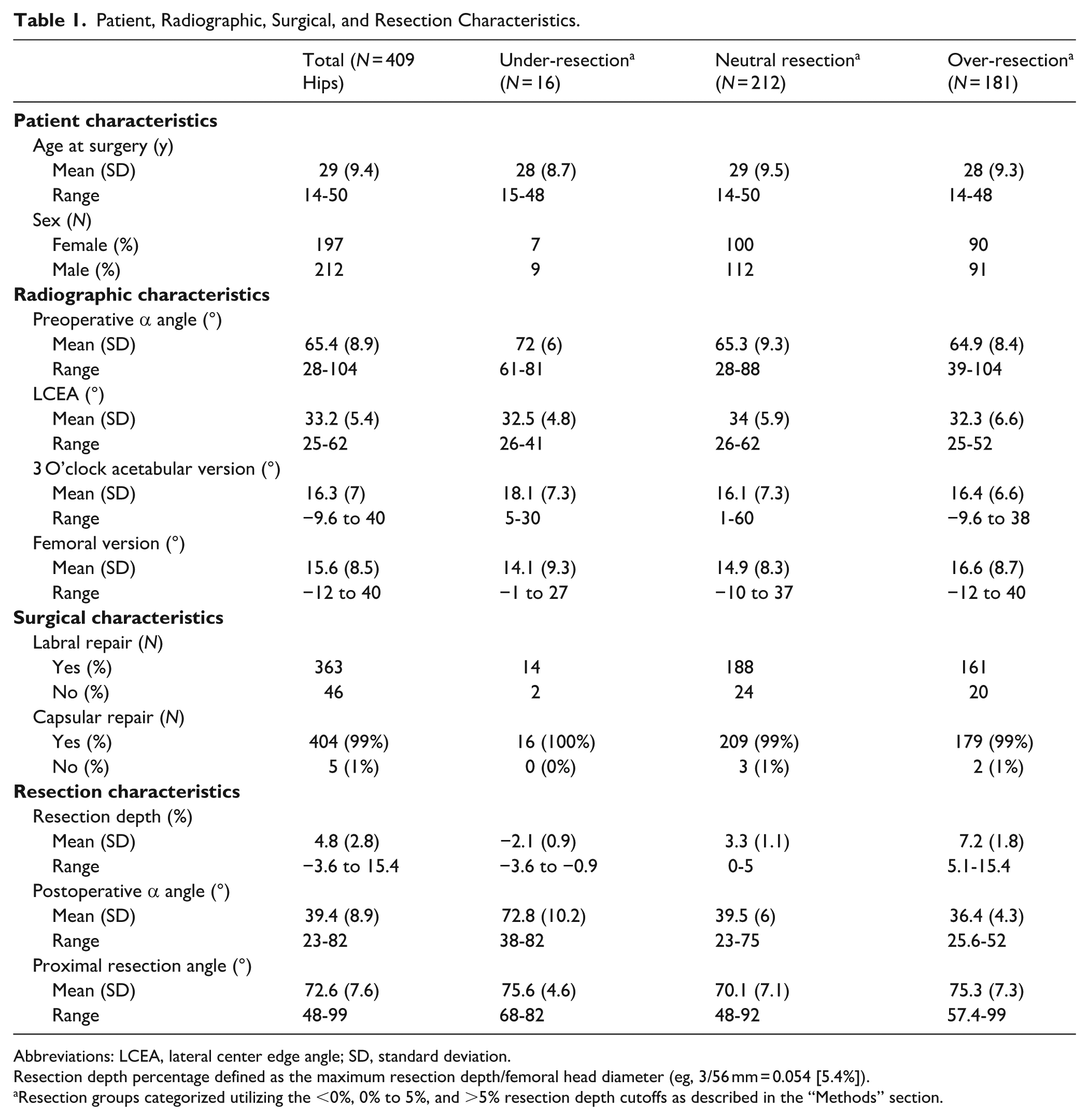
Capsular closure occurred in 99% of hips during hip arthroscopy (404/409), while labral repair occurred in 89% (363/409). Of the 409 hips studied, all had at least preoperative and 1- or 2-year postoperative PROMs for either mHHS or iHOT measures. Overall, ~90% had pre- and postoperative 1-year PROMs and 27% had pre- and postoperative 2-year PROMs. Regarding femoroplasty characteristics, the mean resection depth was 4.8% (range, −3.6% to 15.4%, SD ±2.7%) and the mean proximal resection angle was 72.6° (range, 48°-99°; Table 1). The mean postoperative α angle was 39.4° (range, 23–82).
Patient, Radiographic, Surgical, and Resection Characteristics.
Abbreviations: LCEA, lateral center edge angle; SD, standard deviation.
Resection depth percentage defined as the maximum resection depth/femoral head diameter (eg, 3/56 mm = 0.054 [5.4%]).
Resection groups categorized utilizing the <0%, 0% to 5%, and >5% resection depth cutoffs as described in the “Methods” section.
There were 212 hips (52%) that were categorized as a neutral resection, 181 hips (44%) categorized as an over-resection, and 16 hips (4%) categorized as an under-resection. Utilizing the modified resection categories (>7.5% depth as cutoff for over-resection), there were 329 hips (80%) categorized as neutral resection, 64 hips (16%) categorized as an over-resection, and 16 (4%) categorized as under-resection. There were no statistical differences in preoperative mHHS or iHOT scores between standard or modified resection groups (standard resection: P = .354 and P = .512, respectively; modified resection: P = .517 and .944, respectively).
There were no differences noted between resection groups with respect to the pre- to postoperative change in 1- or 2-year mHHS or iHOT. Additionally, no differences were noted between resection groups in the rate of achievement of 1- or 2-year MCID, SCB, and PASS for mHHS and iHOT (Table 2). The modified resection categories also demonstrated no differences with respect to any of the above outcome variables. Lastly, hips with a proximal resection angle between 65° and 85° had a higher 1 year median change in mHHS score (22 vs 14, P = .031) and iHOT score (37 vs 24, P = .02) than the other resection groups.
Comparison of Categorical Outcome Variables between Resection Groups.
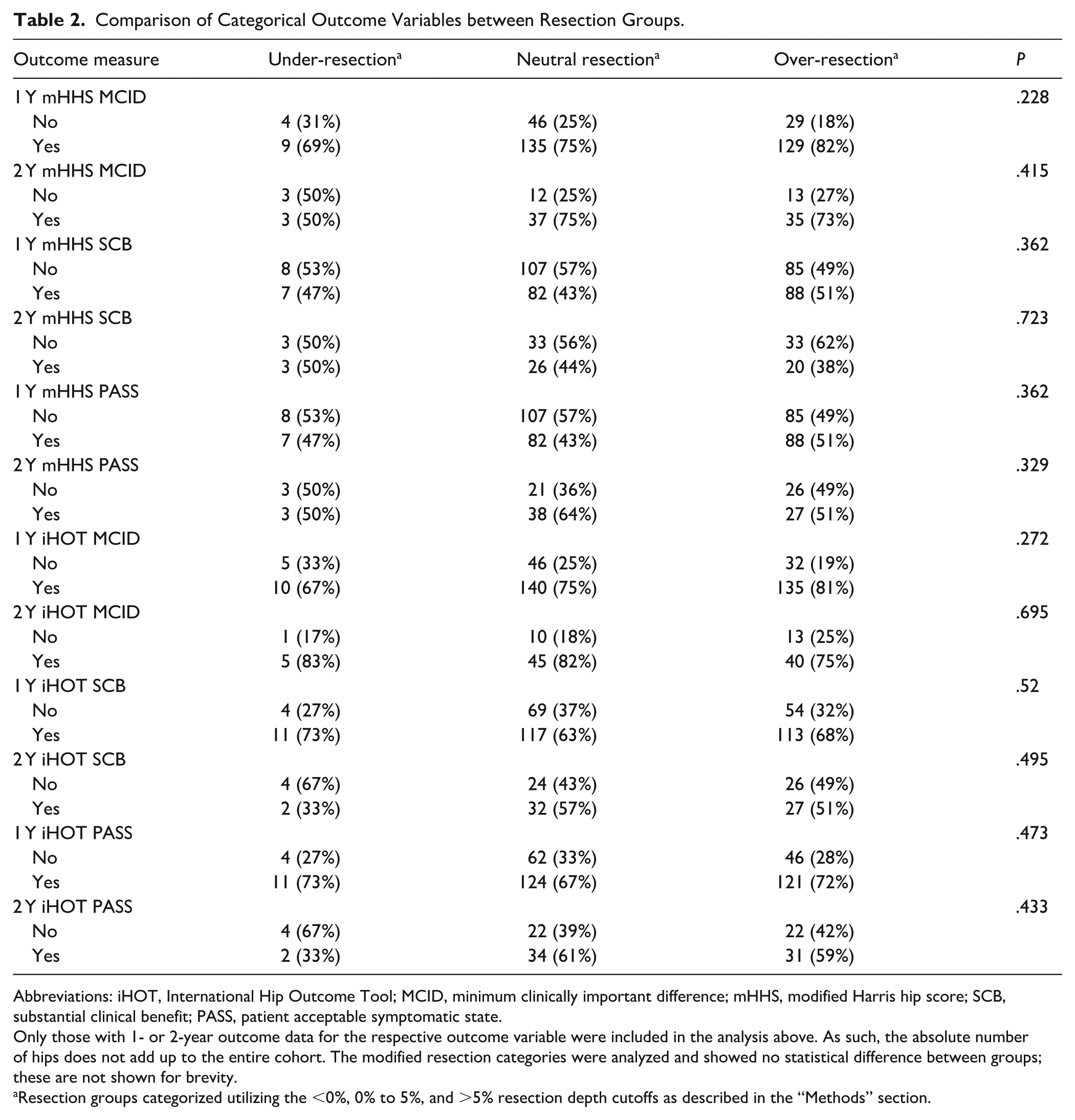
Abbreviations: iHOT, International Hip Outcome Tool; MCID, minimum clinically important difference; mHHS, modified Harris hip score; SCB, substantial clinical benefit; PASS, patient acceptable symptomatic state.
Only those with 1- or 2-year outcome data for the respective outcome variable were included in the analysis above. As such, the absolute number of hips does not add up to the entire cohort. The modified resection categories were analyzed and showed no statistical difference between groups; these are not shown for brevity.
Resection groups categorized utilizing the <0%, 0% to 5%, and >5% resection depth cutoffs as described in the “Methods” section.
Within the linear regression analysis there was a statistically significant positive association between resection depth and 1 year change in mHHS (P = .045) and iHOT score (P = .023; Table 3). For 2-year outcomes, increasing femoral version was a negative predictor for change in mHHS score (P = .048) while resection depth was not a statistically significant predictor. Higher preoperative mHHS and iHOT scores were associated with smaller improvements in postoperative scores at both 1 and 2 years (all P < .001).
Linear Regression Analysis of 1- and 2-Year Postoperative Change in iHOT and mHHS Scores.
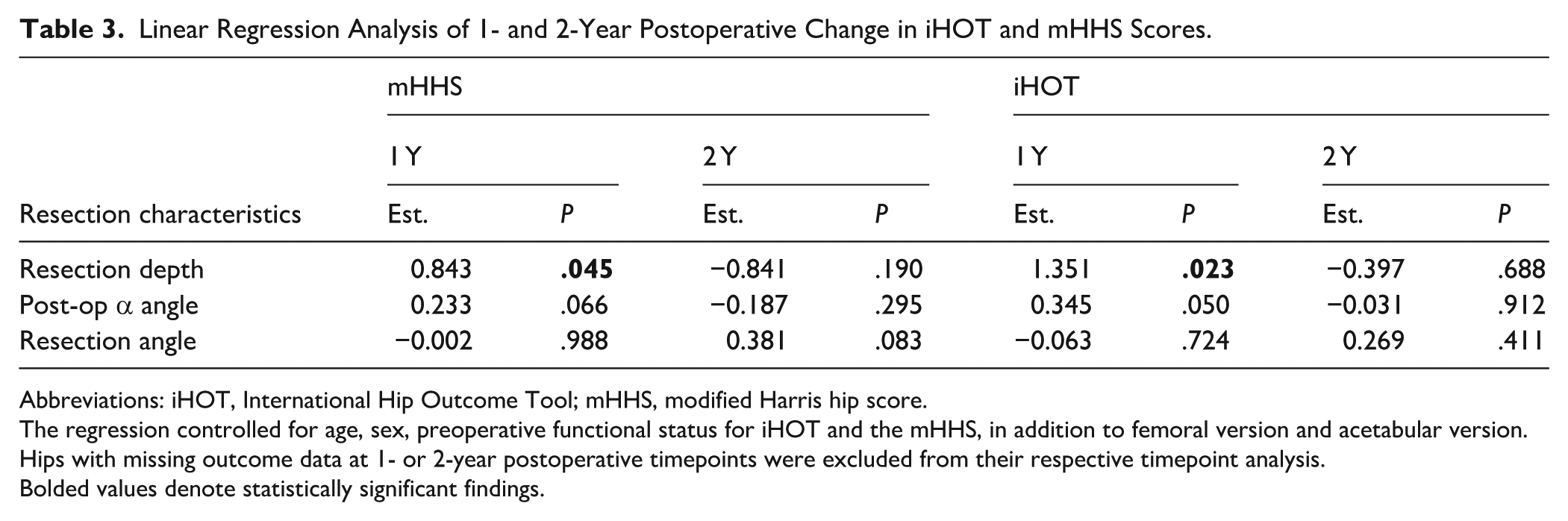
Abbreviations: iHOT, International Hip Outcome Tool; mHHS, modified Harris hip score.
The regression controlled for age, sex, preoperative functional status for iHOT and the mHHS, in addition to femoral version and acetabular version. Hips with missing outcome data at 1- or 2-year postoperative timepoints were excluded from their respective timepoint analysis.
Bolded values denote statistically significant findings.
Within the logistic regression, resection depth was not a predictor of 1- or 2-year MCID, SCB, or PASS for mHHS (Table 4). However, an increasing resection depth was a positive predictor for 1-year iHOT MCID (OR 1.17, 95% CI [1.01-1.37], P = .036) and SCB (OR 1.13, 95% CI [1.002-1.28], P = .049). Increased femoral version was associated with a decreased odds of meeting 2-year MCID for iHOT (OR 0.92, 95% CI [0.85-0.99], P = .049) while a higher resection angle was associated with greater odds (OR 1.19, 95% CI [1.07-1.38], P = .006).
Logistic Regression Analysis of 1- and 2-Year Outcomes for iHOT and mHHS Scores.
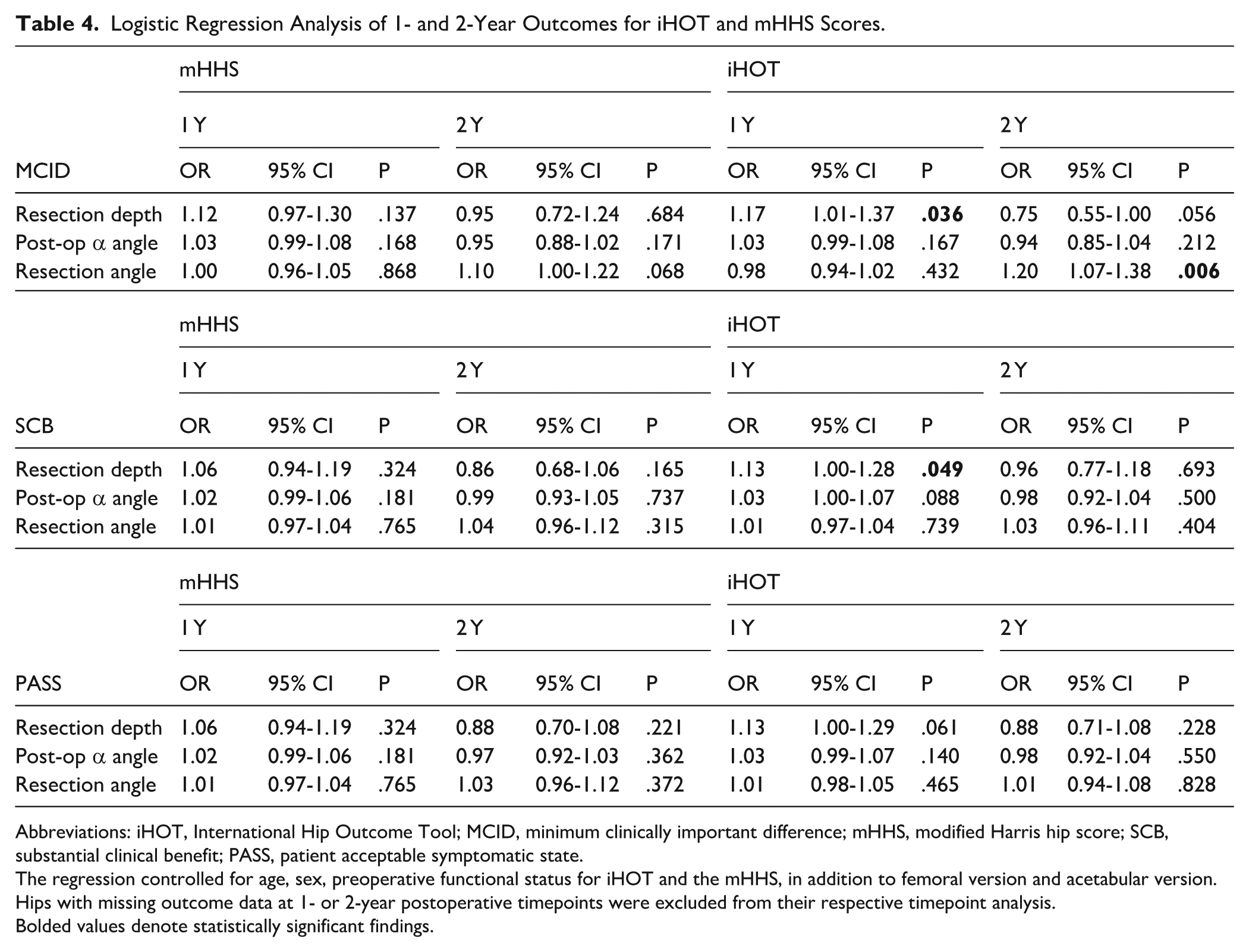
Abbreviations: iHOT, International Hip Outcome Tool; MCID, minimum clinically important difference; mHHS, modified Harris hip score; SCB, substantial clinical benefit; PASS, patient acceptable symptomatic state.
The regression controlled for age, sex, preoperative functional status for iHOT and the mHHS, in addition to femoral version and acetabular version. Hips with missing outcome data at 1- or 2-year postoperative timepoints were excluded from their respective timepoint analysis.
Bolded values denote statistically significant findings.
Discussion
This study describes femoroplasty in a large cohort of primary hip arthroscopy patients with a mean resection depth approaching 5%. When patients were categorized into groups based on the extent of resection, there was no difference found in postoperative outcomes between groups. However, during regression analysis, there was an association between deeper femoroplasty resection and improved 1-year outcomes.
The main limitation of this study was the limited number of hips after applying exclusion criteria due to a reduced collection rate of postoperative PROMs. The number of patients with 2-year PROMs data was relatively small compared to the overall cohort. The process of exclusions and a smaller sample size may introduce selection bias and expose the study to outlier effects. Additionally, the study reflects the experience of a high-volume tertiary referral center, which may limit external validity. Performing radiological measurements on a single Dunn lateral view does not consider the three-dimensional nature of the cam deformity and is a limitation. Additionally, femoroplasty was performed in some patients in this study without an elevated α angle. From our experience, this occurs because many imaging modalities do not comprehensively describe the cam deformity and thus intraoperative assessment drives the decision on whether to perform a femoroplasty. 12
Data on the mean femoroplasty resection depth in a primary hip arthroscopy cohort are lacking in the literature. Two previous studies investigated its impact on clinical outcomes.5,6 Mansor et al described a cohort of patients indicated for revision hip arthroscopy and showed that patients presenting with a femoroplasty depth >5% had significantly lower preoperative functional scores relative to those with a more shallow and even under-resected cam. 5 Absolute postoperative functional scores were worse in the over-resected group; however, the change in scores was similar. This study did not control for the effects of acetabular or femoral version, and the over-resected group constituted 20 patients. Acar et al evaluated 27 hips after primary hip arthroscopy and reviewed the differences in resection characteristics between those who achieved 2-year SCB and PASS for mHHS and Hip Outcome Score Activities of Daily Living HOSADL. 6 They noted that the mean resection depth was 4.7% in those who achieved mHHS PASS versus 8.4% in those who did not. Additionally, the proximal resection angle tended to be lower (82°) in those patients who met mHHS PASS compared to those who did not (92°). Notably, none of the patients in their cohort underwent capsular repair.
Several factors may explain why our data contradict the available literature. First, the report by Mansor et al deals with a different patient population than ours. 5 Their patients were already indicated for revision surgery, while ours were undergoing primary hip arthroscopy. Second, it is unclear what capsular management these patients had at their index hip arthroscopy; only 60% of those in the over-resected cohort had capsular repair at the time of their revision hip arthroscopy. The same capsular management differences exist in the Acar et al study. 6 This is important, as the stabilizing effects of capsular closure have been demonstrated in the literature. In fact, capsular closure has been shown to biomechanically stabilize the hip in the setting of a femoroplasty.8,13 Thus, the hip microinstability effect of relative cam over-resection within reason may be negated with capsular repair. Third, the sample size in prior studies possibly exposed the analysis to outlier effects or selection bias. Lastly, femoral and/or acetabular version may affect hip stability and postoperative PROMs and were controlled for in the present study.
Cam over-resection can become clinically relevant, although this is rare. 14 Regardless of capsular management or a patient’s bony morphology, a deeper resection can lead to complications such as femoral neck weakening, iatrogenic instability, and increased risk of femoral neck fracture.15,16 Unfortunately, the depth that predisposes to these complications may be affected by patients’ bone mineral density, level of disuse osteopenia postoperatively, pre- and postoperative activity level, or other factors. Ideally, the optimal cam femoroplasty could eventually be determined by a patient’s bony morphology, labral integrity, and capsular management.
The strengths of the study include the CT-based data on femoral and acetabular version that were factored into the regression analysis. Our selection criteria involved selecting a patient cohort that would traditionally be thought of as “stable” hips, based on their lateral acetabular coverage. However, this may have limited the effect of resection depth on clinical outcomes and may also restrict conclusions outside of this morphologic cohort.
In conclusion, within this large cohort of patients with FAIS undergoing primary hip arthroscopy with capsular repair, an increasing resection depth was associated with improved outcomes, particularly 1 year postoperatively. These data should be interpreted in the setting of the cohort characteristics including the LCEA criteria, the narrow variance with respect to resection depth, and nearly ubiquitous capsular repair. Based on this cohort’s data, a femoroplasty that resects 5% to 6% of neck width to achieve sufficient offset with a proximal resection angle between 65° and 85° may result in better outcomes, particularly 1 year postoperatively. A future cohort of patients with longer-term follow-up may further define outcomes related to femoroplasty characteristics.
Supplemental Material
sj-pdf-1-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-1-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-2-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-2-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-3-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-3-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-4-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-4-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-5-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-5-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-6-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-6-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-7-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-7-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-8-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-8-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Supplemental Material
sj-pdf-9-hss-10.1177_15563316261459986 – Supplemental material for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study
Supplemental material, sj-pdf-9-hss-10.1177_15563316261459986 for Hip Arthroscopy Femoroplasty Resection Characteristics as They Relate to Postoperative Clinical Outcomes: A Retrospective Cohort Study by Mason E. Uvodich, Hayden P. Baker, Alex V. Capitano, Akshay K. Raghuram, Danyal H. Nawabi, Anil S. Ranawat, Struan H. Coleman, Bryan T. Kelly and Stephanie S. Buza in HSS Journal®
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was waived for all participants included in this study by the IRB at Hospital for Special Surgery.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Danyal H. Nawabi, MD, declared relationships with BetterPT, CONMED Corporation, HS2, HSS West Side ASC, HSS ASC Development Network, Joint Effort Administrative Services Organization (JEASO), and Vitalis. Anil S. Ranawat, MD, declared relationships with AGelity Biomechanics, Bodycad, USA, Cervos, Conformis, Enhatch, HSS ASC Development Network, HS2, NewClip, Overture, JEASO, Smith & Nephew, and Strathspey Crown. Struan H. Coleman, MD, PhD, declared relationships with BetterPT, Copper Fit, HS2, HSS ASC Development Network, HSS ASC West Side, JEASO, Johnson & Johnson, Legent Health, Motive Health, Stryker Endoscopy, and Shelter Island Ventures. Bryan T. Kelly, MD, declared relationships with Arthrex, Inc, BICMD, Inc, My Medical Images, Parvizi Surgical Innovation, Relief Labs, SeeALL AI, Vincera Institute, ZEO ScientifiX, and the Hospital for Special Surgery Board of Trustees. Stephanie S. Buza, MD, declared a relationship with JEASO. The other authors declared no potential conflicts of interest.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.