
Abstract
Background:
Radiographic assessment is central to the diagnosis of femoroacetabular impingement (FAI) syndrome. However, the relationship between specific bony morphology and symptom severity remains unclear.
Purpose:
We sought to evaluate the relationship between FAI morphology, quantified through preoperative radiographic measures, and preoperative symptom burden in patients with FAI syndrome.
Methods:
We conducted a retrospective study of prospectively collected data that included a series of consecutive patients diagnosed with FAI syndrome who underwent hip arthroscopy by a single surgeon between January 2024 and October 2025. Inclusion criteria were (1) diagnosis of FAI syndrome and (2) availability of complete preoperative patient records, including X-ray images and preoperative patient-reported outcome measures. Exclusion criteria were (1) patients <14 or >60 years, (2) diagnosis that included FAI syndrome with concomitant intra-articular pathology, (3) hip surgery other than primary hip arthroscopy, (4) unavailable X-ray imaging, and (5) history of lower extremity osteotomy for abnormal rotational profile. Hip impingement measures were obtained on preoperative radiographs, including α angle, head-neck offset, anterior center-edge angle, and lateral center-edge angle, crossover sign, crossover ratio, and ischial spine sign. Preoperative symptom severity was assessed by the International Hip Outcome Tool-12 (iHOT-12). Multivariate models adjusted for demographics, mental health, physical activity, and corticosteroid injection history.
Results:
Among 285 patients (median age 34.9 years, 75.4% female), the median iHOT-12 score was 37.5. Proximal femur measures and acetabular coverage were not correlated with iHOT-12. The presence of crossover or ischial spine signs was associated with higher iHOT-12 on bivariate analysis and remained predictive of higher iHOT-12 after adjustment for demographics and injection status in multivariate modeling. All other radiographic measures were non-significant after further adjustment for mental health and activity level.
Conclusion:
Radiographic measures of retroversion are associated with better preoperative symptoms in patients with FAI syndrome. Other radiographic measures of hip impingement showed no meaningful association with preoperative symptom severity. For patients with FAI syndrome, psychological and functional factors exerted a larger influence on symptom severity than did impingement severity as reflected on radiograph.
Level of Evidence:
Level IV: retrospective case series.
Introduction
Femoroacetabular impingement (FAI) is a chronic hip condition that commonly affects young, active individuals who engage in repetitive hip-loading activities.1-3 FAI results from bony abnormalities that create atypical contact between the femoral head-neck junction and the acetabular rim.2,4 Ultimately, this can lead to chronic hip pain as well as progressive damage to the acetabular labrum, chondro-labral junction, and articular cartilage, which predisposes patients to early onset osteoarthritis.2,5 In 2016, the Warwick Agreement on FAI syndrome reached international consensus, defining FAI syndrome as the combination of symptoms, clinical signs, and imaging findings that differentiate symptomatic patients from those with asymptomatic FAI morphology. 6
Radiographic evaluation is central to the diagnosis of FAI. Based on the underlying bony morphologic variation found on radiographs, FAI is classified into 3 broad categories: cam, pincer, and mixed-type FAI. Pincer-type morphology results from overcoverage of the femoral head by the acetabulum, while cam-type impingement results from bony prominences found at the femoral head-neck junction, causing compression and shear forces against the acetabular rim.2,4 Mixed-type morphology refers to a combination of cam and pincer morphology with the coexistence of cam and pincer bony features. 4 While the prevalence of FAI type varies from study to study, cam morphology seems to be the most prevalent, followed by mixed and pincer type FAI. 7 Radiographically, cam type FAI can be determined via X-ray measurement of the α angle and the femoral head-neck offset, while pincer type FAI can be determined via X-ray measurement of the lateral center-edge angle (LCEA), anterior center-edge angle (ACEA), crossover sign, crossover ratio, and ischial spine sign.1,8,9
Although radiographic assessment provides valuable structural insight, the relationship between FAI morphology and clinical symptom severity remains incompletely understood. Previous studies have demonstrated that many individuals with cam or pincer morphology are asymptomatic, suggesting that bony abnormalities alone do not dictate symptom development.10-12 However, in some studies, greater severity of bony abnormalities—such as increased α angle and LCEA or increased anterior hip capsule volume relative to posterior hip capsule volume—has been associated with higher pain levels and impaired function, 13 while others have reported no significant correlation between radiographic parameters and patient-reported outcomes.3,14 Furthermore, factors such as general health status, mental well-being, and physical activity also likely interact with structural morphology to influence symptom perception. Understanding these associations may enhance preoperative risk assessment and better guide patient-specific management strategies for individuals with FAI syndrome.
The purpose of this study is to evaluate the relationship between FAI morphology (quantified through preoperative radiographic measures) and preoperative symptom burden (assessed using the International Hip Outcome Tool (iHOT-12) in patients with FAI syndrome. We hypothesize that greater cam and pincer severity will be associated with worse hip-specific and general health outcomes, lower physical activity levels, and reduced mental well-being.
Methods
This study was approved by our Institutional Review Board. We conducted a retrospective case series of prospectively collected data that included consecutive patients diagnosed with FAI syndrome who underwent surgical treatment with hip arthroscopy by a single surgeon between January 2024 and October 2025. FAI syndrome was diagnosed in patients who had bony impingement morphology (cam, pincer, or mixed-type morphology), as well as clinical symptoms related to the impingement. Specifically, anterior hip pain is reproduced with flexion, adduction, and internal rotation testing and/or with flexion, abduction, and external rotation testing. In cases where symptoms were ambiguous or not clearly reproducible on physical examination, a diagnostic ultrasound-guided intra-articular injection of local anesthetic was used to confirm the hip joint as the primary pain generator prior to proceeding with arthroscopic surgery. Inclusion criteria were: (1) diagnosis of FAI syndrome as defined above and (2) availability of complete preoperative patient records, including X-ray images and preoperative patient-reported outcome measures. Exclusion criteria were: (1) patients <14 or >60, (2) diagnosis that included FAI syndrome with concomitant intra-articular pathology (ie, osteoarthritis, femoral head avascular necrosis, and slipped capital femoral epiphysis), (3) hip surgery other than primary hip arthroscopy, (4) unavailable X-ray imaging, and (5) history of lower extremity osteotomy for abnormal rotational profile. We defined osteoarthritis as Tonnis grade 1 (mild) or higher radiographic osteoarthritis, which includes any sign of joint space narrowing, marginal osteophytes, or subchondral sclerosis of the femoral head or acetabulum. 15 Written informed consent was obtained from all included patients via the patient or a legally authorized representative.
A total of 471 patients were screened for inclusion. After applying exclusion criteria, 285 patients remained eligible and were included in the study. The median patient age was 34.9 (interquartile range [IQR] 22.8, 45.4), consisting of 75.4% (n = 215) females and 24.5% (n = 70) males (Table 1). The median iHOT-12 score was 37.5 (21.7-53.3). Further demographic statistics are summarized in Table 1. In total, 186 patients were excluded from the current study for reasons including revision surgery (n = 81), acetabular dysplasia (n = 62), osteoarthritis or intra-operatively identified high-grade cartilage defects (n = 31), femoral head avascular necrosis (n = 5), slipped capital femoral epiphysis (n = 5), and Legg-Calve-Perthes disease (n = 2).
Baseline Patient Demographics.
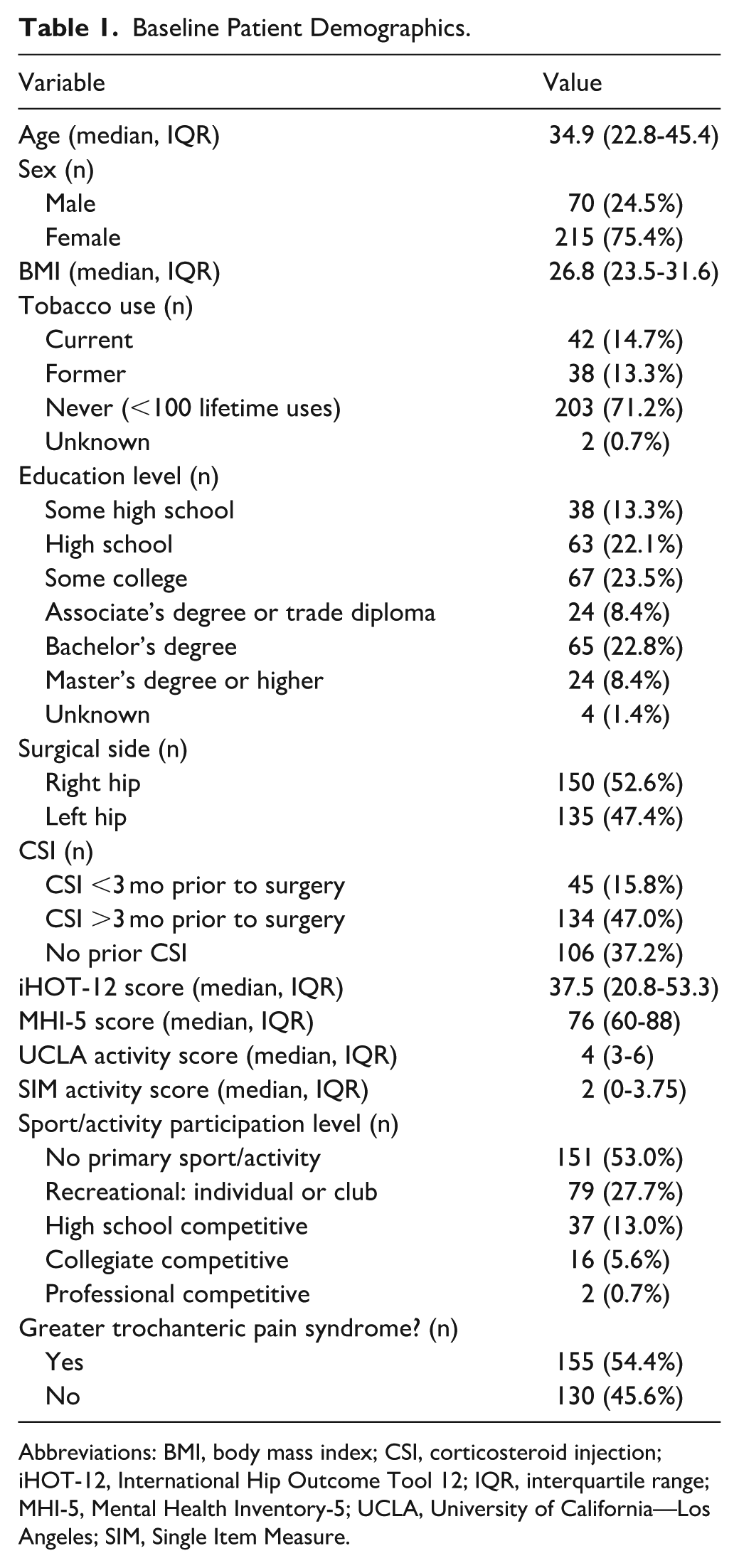
Abbreviations: BMI, body mass index; CSI, corticosteroid injection; iHOT-12, International Hip Outcome Tool 12; IQR, interquartile range; MHI-5, Mental Health Inventory-5; UCLA, University of California—Los Angeles; SIM, Single Item Measure.
On the day of surgery, patients completed an unassisted preoperative multipart survey consisting of the following instruments: Mental Health Inventory-5 (MHI-5), iHOT-12, University of California—Los Angeles (UCLA) Activity Score, and the Adult Single Item Measure Physical Activity tool (Adult SIM-PA).16-20 This data was collected prospectively; as there were no incomplete forms, this resulted in 100% data capture among patients who met the inclusion criteria.
The iHOT-12 was chosen as the primary outcome measure because it is specifically validated for young, active patients with hip pathology, which best matched the population included in this study. 21 The iHOT-12 includes 12 questions that assess hip-related quality of life and changes following treatment interventions. The MHI-5 is a 5-question instrument that evaluates both positive and negative mental health attributes, including symptoms of anxiety and depression. 22 Scores range from 0 (poor mental health) to 100 (optimal mental health).22,23 The UCLA Activity Scale quantifies physical activity levels across a spectrum, ranging from “regularly participates in impact sports” to “wholly inactive, dependent on others, and cannot leave residence.” 19 The Adult SIM-PA tool is a validated single-item measure used to estimate general physical activity in adults.20,24 It correlates well with objective hip-worn accelerometer-based data 24 and records the number of days in the previous week during which an individual engaged in ≥30 minutes of moderate-to-vigorous physical activity sufficient to increase breathing rate.
After receiving training in each radiographic measurement under the supervision of the primary surgeon, 2 medical students (N.R.K. and M.A.R.-P.) independently performed the measurements while blinded to patient symptom status. Interclass correlation coefficient values for all measures ranged from 0.75 to 1.00, indicating good to excellent inter-observer reliability. 25 Radiographic evaluation for features consistent with FAI was performed on standardized weightbearing anteroposterior (AP), weightbearing false-profile, and supine Dunn view pelvis radiographs. The radiographic parameters measured included the LCEA, ACEA, α angle, femoral head-neck offset, femoral head diameter, presence of a crossover sign, crossover ratio, and ischial spine sign (all well-established metrics with defined thresholds for characterizing cam and pincer morphology in diagnosing FAI; Figure 1). The ACEA was measured using weightbearing false profile views, while the α angle was evaluated on supine Dunn view radiographs.
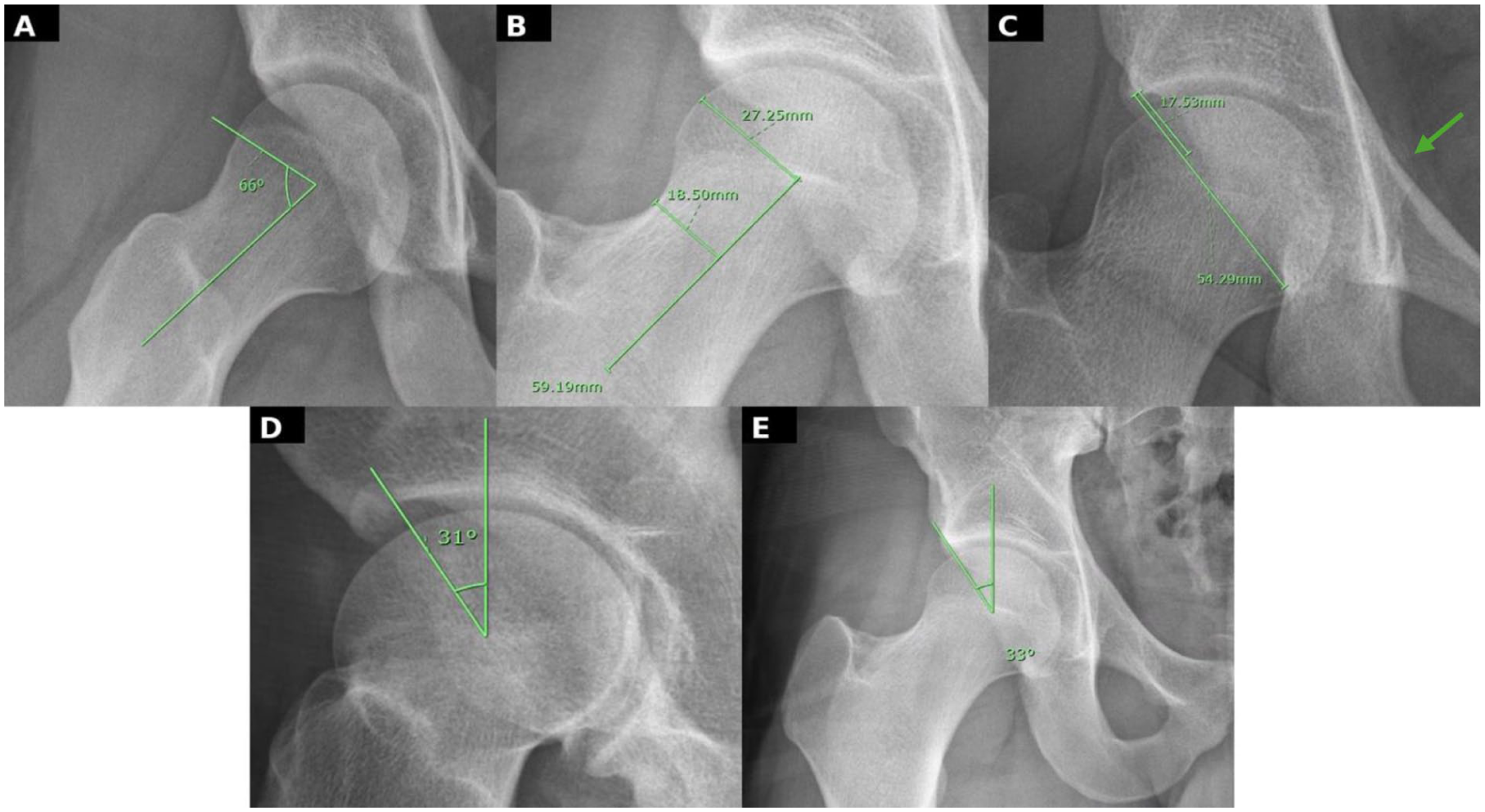
Radiographic measurements of acetabular and femoral bony morphology (A) α Angle, (B) femoral head-neck offset, (C) crossover sign, crossover ratio, and ischial spine sign (green arrow), (D) ACEA, and (E) LCEA.
The LCEA assesses the superolateral coverage of the femoral head by the acetabulum. 26 In this study, it was measured utilizing the Ogata method. 27 Values >39° indicate over-coverage of the femoral head by the acetabulum, which contributes to impingement by restricting flexion of the femoral neck. 28 The ACEA assesses the anterior coverage of the femoral head by the acetabulum. 26 An ACEA value of >39° is considered indicative of pincer impingement. 29
The presence of a crossover sign identifies the acetabulum as retroverted; its absence identifies the acetabulum as anteverted. A retroverted acetabulum has been linked to overcoverage and pincer impingement. 30 The crossover sign is assessed for on AP imaging; however, before determining its presence or absence, the image must be inspected to ensure there is not excessive pelvic tilt or rotation, which can lead to false-positive or false-negative results. 26 To confirm image quality, AP images were considered adequate if the tip of the coccyx was above and within 2 mm of the center of the pubic symphysis. While there is not as much data supporting a cutoff value for crossover ratio compared to other FAI measurements, current literature suggests that a ratio of >20% is a significant indicator of acetabular retroversion. 31
The ischial spine sign is also associated with increased acetabular retroversion. 26 Similar to the crossing sign, identification of the ischial spine sign requires a quality AP image; therefore, the same quality control measures were used to determine if each AP image was appropriate for assessing this sign. Head-neck offset was measured on AP imaging. In a healthy hip joint, maintenance of space between the femoral head-neck junction and the acetabular rim allows for unhindered hip movement. This requires an offset between the anterosuperior surface of the femoral neck and the corresponding surface of the femoral head. 28 The normal head-neck offset is 9 mm; an offset <9 mm is indicative of cam impingement. 28
The α angle assesses the head-neck offset in cam impingement. 32 In general, an angle >50° is considered the threshold for diagnosing cam morphology. 33
To further evaluate the interaction between femoral and acetabular morphology, several combination parameters were created for this study. LCEA categorization was used to group acetabular coverage as borderline dysplastic (20°-25°), normal (25°-40°), or over-coverage (>40°), consistent with established diagnostic thresholds for acetabular morphology.34,35 To capture global acetabular version abnormalities, a combined “crossover sign or ischial spine sign” variable was created, representing the presence of either radiographic indicator of acetabular retroversion. This allowed assessment of retroversion as a singular construct rather than as multiple independent findings. Additionally, 2 combined measures, “LCEA + α angle” and “ACEA + α angle,” were generated to examine the relationship between cam morphology and acetabular coverage. These metrics were designed to assess how cam deformity and acetabular over- or under-coverage may jointly contribute to hip impingement mechanics and symptom burden.
Statistical Analysis
All statistical analyses were performed with JMP Student Edition (JMP 17.2; SAS Institute). Descriptive statistics were generated for the entire sample. Continuous variables were summarized using medians with IQRs, as the data set was non-normally distributed, as assessed with the Kolmogorov-Smirnov goodness of fit test. Categorical variables were reported as counts and percentages. Normality of continuous variables was assessed using the Shapiro-Wilk and Anderson-Darling tests. All outcome measures were found to demonstrate non-normal distributions. As such, non-parametric tests were employed for statistical analysis. Spearman’s rank correlation coefficients (ρ) were calculated to evaluate associations between preoperative iHOT-12 scores and continuous radiographic measurements (LCEA, ACEA, ɑ-angle, head-neck offset, femoral head diameter, and crossover ratio). For categorical radiographic parameters, comparison to iHOT-12 was performed using the Wilcoxon rank-sum test (for 2 groups) or Kruskal-Wallis test (for 3 or more groups). Statistical significance was set at P < .05.
A forward stepwise multiple linear regression was performed to identify independent predictors of preoperative iHOT-12 scores. Entry and retention of variables in the multivariate model were guided by the minimum Bayesian Information Criterion and assessment of an effect size change of >20% with the addition of potential covariates. Potential variables considered for the initial multivariate model included all radiographic measures, patient demographics, history of intra-articular corticosteroid injection, and concomitant greater trochanteric pain syndrome (GTPS). Results of the multivariate model are reported as β coefficients (standard errors) with corresponding t ratios and P values. Statistical significance was defined as P < .05. In a secondary adjusted analysis, baseline factors including mental health status and baseline activity level were evaluated separately as these variables are highly correlated with iHOT-12 scores but could not be causally linked to radiographic morphology (Supplemental Material).
Results
Radiographic measurements demonstrated a median LCEA of 31° (IQR 26-36; Table 2). When broken down into LCEA category, 14.0% of patients demonstrated acetabular over-coverage (LCEA >40°), 72.0% demonstrated a normal acetabular coverage (LCEA 25°-40°), and 14.0% demonstrated a borderline dysplastic acetabulum (LCEA 20°-25°). A crossover sign was present in 18.6% of patients, and an ischial spine sign was found in 9.8% of hips.
Radiographic Measurements.
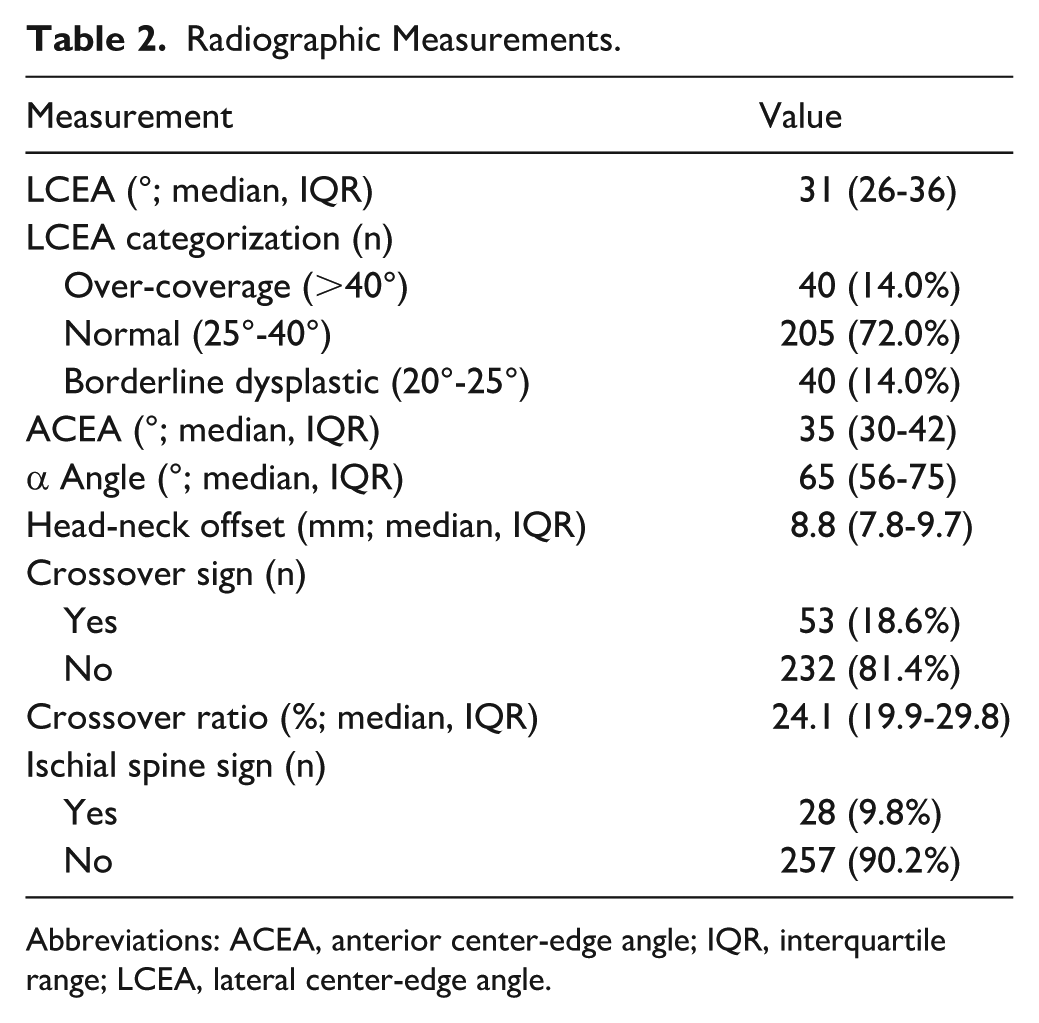
Abbreviations: ACEA, anterior center-edge angle; IQR, interquartile range; LCEA, lateral center-edge angle.
On bivariate analysis, no continuous radiographic parameter was found to be significantly correlated with preoperative iHOT-12 scores (Table 3). However, the presence of a crossover sign (P = .04) and the combined presence of a crossover sign or ischial spine sign were associated with higher iHOT-12 scores (P = .02), indicating less preoperative symptom burden. No other categorical parameters were found to be significantly associated with iHOT-12 scores.
Bivariate Analysis of iHOT-12 by X-ray measurements.
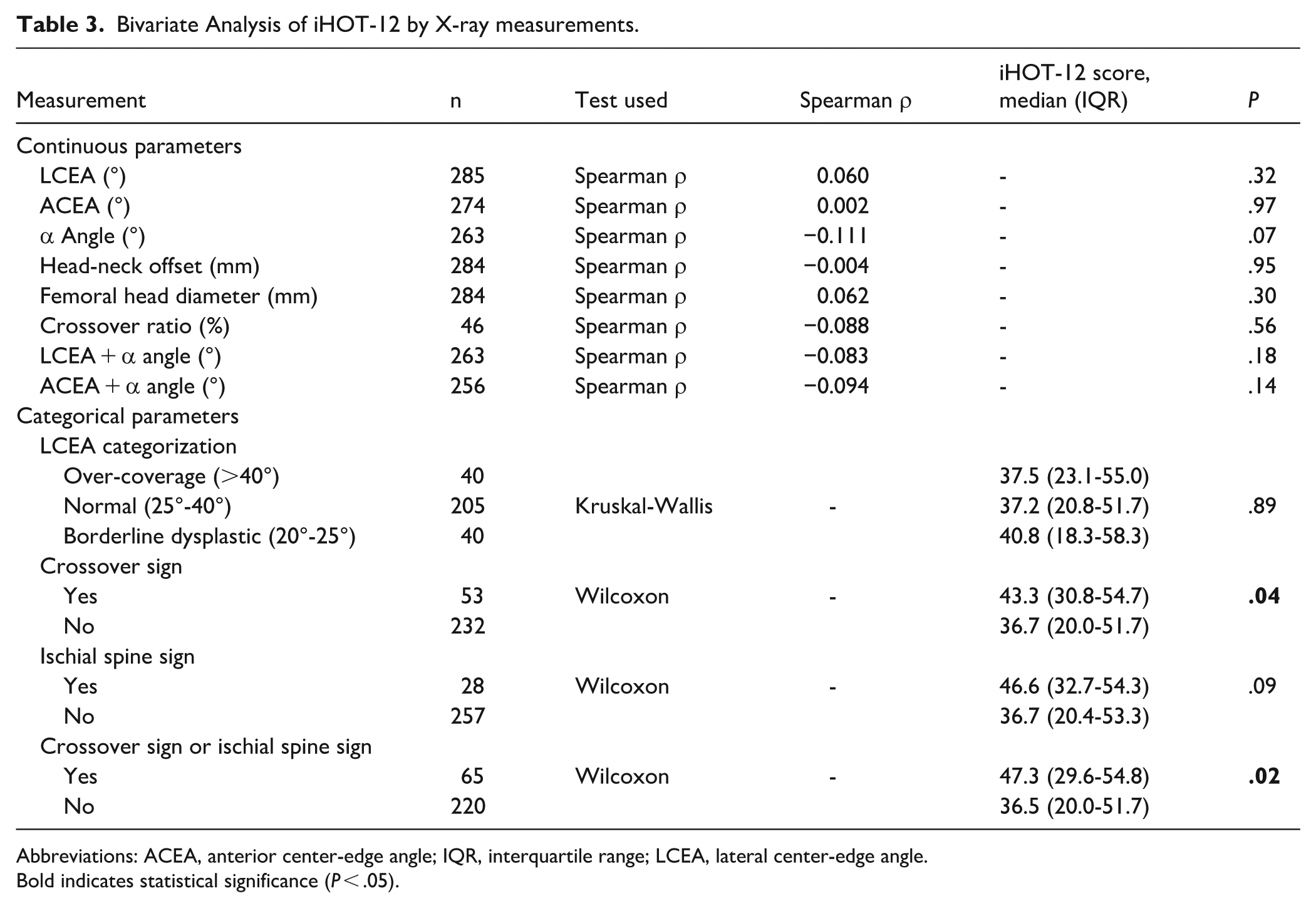
Abbreviations: ACEA, anterior center-edge angle; IQR, interquartile range; LCEA, lateral center-edge angle.
Bold indicates statistical significance (P < .05).
On multivariate analysis, the presence of a crossover sign or ischial spine sign was the only imaging measure that was independently predictive of iHOT12 scores after consideration for patient age, sex, prior corticosteroid injection, educational status, or tobacco use status (β = −3.11, SE = −1.47, P = .035). No other measures of acetabular or femur morphology remained significant after adjusting for crossover sign/ischial spine sign (P > .05).
A separate multivariate model including baseline factors known to reflect symptom severity demonstrated that mental health, activity level, and the presence of GTPS were all strongly associated with preoperative iHOT-12 scores. Higher MHI-5 score (β = .28, SE = 0.06, P < .0001), higher baseline UCLA activity score (β = 2.57, SE = 0.45, P < .0001), and presence of GTPS (β = 3.17, SE = 1.04, P = .003) were independently associated with higher iHOT-12 scores. In this model, the presence of a crossover or ischial spine sign was not significant (β = −1.72, SE = −1.20, P = .151). Collectively, these variables explained 28.7% of the variance in iHOT-12 scores (R2 = 0.287). These symptom-related factors showed larger effect sizes and stronger associations with iHOT-12 score than any radiographic measure, suggesting that they represent components of overall symptom burden rather than independent predictors of hip morphology-related pain. Therefore, these confounders were not included in the adjusted analysis as they are highly associated with iHOT-12 scores, but causation could not be established.
Discussion
The primary outcome of this retrospective study was that signs of retroversion were the only radiographic impingement morphologic features associated with preoperative symptom severity in patients with FAI syndrome. This relationship persisted after adjusting for demographic variables and prior corticosteroid injection, although the effect size was small. Measures of preoperative mental health, activity level, and presence of concomitant GTPS had a much greater association with hip pain and function compared to radiographic morphologic severity alone.
This study had several limitations. Not all radiographs passed quality control measures for pelvic tilt, which limited the number of patients we could evaluate for crossover and ischial spine signs. Similarly, differences in acquisition date, X-ray equipment, and technicians contributed to variability in image quality across patients, which may have reduced the accuracy of measurements in cases with suboptimal imaging quality. Because hip impingement is influenced by dynamic bony and soft-tissue interactions, it is possible that some patients without radiographic abnormalities demonstrated functional impingement from unmeasured factors, such as femoral torsion. In addition, while we used validated patient-reported outcome measures, the perception of symptoms may be influenced by psychosocial or biomechanical factors, which can result in response bias. Because this study represents a single surgeon series, it may not be generalizable to other FAI syndrome populations.
The relationship between radiographic impingement morphology and impingement symptoms is complex and often inconsistent across the literature. According to Murphy et al, although acetabular version and α angle demonstrated association with earlier onset of FAI syndrome, patient-related factors, including sex, activity level, and healthcare access, were more significant predictors of patient-reported outcomes as measured by the iHOT-33. 1 Similarly, our data showed a limited correlation between bony parameters and patient-reported function. In contrast, other studies have found no significant relationship between MRI or radiographic impingement severity measures and functional scores such as iHOT-12 or the Hip Disability and Osteoarthritis Outcome Score.11,14 This variability may reflect differences in imaging modality (2D radiography vs 3D MRI or computed tomography), thresholds for defining cam or pincer morphology, study sample composition, or the use of diverse patient-reported outcome tools. The relatively modest α angles observed in this cohort likely reflect the inclusion of mixed and pincer-type impingement, as well as the predominantly female study population; in prior literature, both have been associated with lower α angles compared to cam-predominant and male-dominant cohorts.5,7
Notably, the presence of crossover or ischial spine signs (both indicative of acetabular retroversion) was the only morphology associated with symptom burden prior to adjustment for confounders. While prior biomechanical models suggest that acetabular retroversion increases anterior labral contact pressures and alters joint loading, potentially eliciting pain,13,36-39 our findings contrast these models by demonstrating that radiographic signs of retroversion were associated with better preoperative symptom scores. Crossover and ischial spine signs on AP radiographs are sensitive to patient positioning. Thus, differences from prior studies may reflect compensatory postures or other individual factors that mitigate symptom burden in the presence of retroversion. In addition, other research has emphasized that psychosocial well-being and physical activity patterns can strongly influence symptom perception and hip-specific outcomes, even more so than morphologic severity.1,4 Given the varying magnitude of these associations, it is likely that pain and dysfunction in FAI syndrome arise from a multifactorial interplay between osseous and soft-tissue morphologic variations, capsulo-labral integrity, mental health, compensatory movement patterns, and activity level. On its own, radiographic morphology doesn’t explain the patient’s symptoms.
The weak correlation between symptoms and radiographic morphology may have several biomechanical causes. Compensatory motion patterns may redistribute joint forces away from the areas of bony impingement, reducing pain in some individuals despite pronounced deformity.40,41 Conversely, patients with milder deformities may experience pain because of altered neuromuscular control, repetitive sport-specific loading, or lower pain thresholds.42-44 In addition, subtle labral or chondral injury may be more symptomatic than gross morphologic abnormality alone, as even minor disruption of the labrum can heighten intra-articular pressure and nociception.45,46 While acetabular retroversion has been shown to increase anterior labral stress in biomechanical models, thereby potentially increasing pain, our findings suggest that patients with radiographic markers of retroversion may actually report better preoperative symptom scores. This paradox may be explained by the dynamic nature of retroversion markers, which are influenced by pelvic tilt and patient positioning. Unlike fixed bony deformities (cam or pincer morphology), retroversion-related impingement may be controlled through voluntary postural adjustments, allowing patients to sit, stand, and move in positions of maximum comfort. As pain perception is partially under conscious control, patients may naturally adopt positions that minimize discomfort, allowing them to modulate their symptoms more effectively. Biomechanical studies have demonstrated that retroversion shifts the impingement zone anteriorly and enlarges the area of contact during flexion and internal rotation, elevating joint pressures.37,39 However, these findings reinforce that labral and soft-tissue stress, particularly when modifiable through dynamic patient-controlled movement, may have a more substantial role in symptom severity than static osseous morphology alone.
As a multitude of factors influence symptomology in patients with FAI syndrome, a diagnosis and treatment plan should be multifaceted. Because labral and soft-tissue stress may be the primary symptom drivers, in determining surgical candidacy, radiographic findings should be interpreted in conjunction with a thorough assessment of symptoms, mental health, and functional status. Based on this study, clinicians should avoid overemphasis on minor radiographic abnormalities. Failing to do so places patients at risk of overtreatment of anatomic variants that may not be the true source of patients’ pain. Instead, when considering treatment options, surgeons should incorporate a comprehensive patient-centered approach to care that accounts for modifiable risk factors such as mental health, physical activity, and coexisting pain conditions that may exacerbate symptomology. Incorporating patient-reported outcome screening tools, such as the MHI-5 and UCLA Activity Scale, into preoperative assessments may help identify patients whose symptoms are disproportionately influenced by psychological or functional limitations. Targeted rehabilitation aimed at addressing these contributors through physical therapy and optimization of mental well-being may help improve outcomes. However, should non-operative treatments fail to improve hip pain and dysfunction, surgical correction of concomitant intra-articular pathology (such as labral tears or chondral defects) and addressing underlying osseous morphology has been shown to further enhance outcomes by restoring joint stability, reducing nociceptive input, and improving the mechanical environment of the hip.47-50
Future studies should aim to address the complexity of FAI syndrome, further exploring the radiographic morphology, soft-tissue pathology, and psychological factors that influence symptom expression. Prospective studies that incorporate serial imaging and patient-reported outcome measures can help to define how the morphologic progression of FAI evolves over time. In addition, the inclusion of advanced imaging, such as MRI, may help to clarify the associations between labral, chondral, and capsular pathology and persistent symptoms in the presence of FAI. The development of a multidimensional model of FAI syndrome using radiographic, biomechanical, and psychological domains will help optimize treatment planning.
In conclusion, we found that radiographic measures of retroversion were associated with better preoperative symptoms in patients with FAI syndrome. Other radiographic measures of hip impingement showed no meaningful association with preoperative symptom severity. These findings suggest that for patients with FAI syndrome, psychological and functional factors may have exerted a larger influence on symptom severity than did hip impingement.
Supplemental Material
sj-docx-1-hss-10.1177_15563316261460402 – Supplemental material for Symptom Severity due to Femoroacetabular Impingement Syndrome Is Correlated With Radiographic Signs of Acetabular Retroversion but No Other Impingement Parameters
Supplemental material, sj-docx-1-hss-10.1177_15563316261460402 for Symptom Severity due to Femoroacetabular Impingement Syndrome Is Correlated With Radiographic Signs of Acetabular Retroversion but No Other Impingement Parameters by Nicholas R. Kossoff, Manuel A. Romero-Padron and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316261460402 – Supplemental material for Symptom Severity due to Femoroacetabular Impingement Syndrome Is Correlated With Radiographic Signs of Acetabular Retroversion but No Other Impingement Parameters
Supplemental material, sj-docx-2-hss-10.1177_15563316261460402 for Symptom Severity due to Femoroacetabular Impingement Syndrome Is Correlated With Radiographic Signs of Acetabular Retroversion but No Other Impingement Parameters by Nicholas R. Kossoff, Manuel A. Romero-Padron and Joshua S. Everhart in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316261460402 – Supplemental material for Symptom Severity due to Femoroacetabular Impingement Syndrome Is Correlated With Radiographic Signs of Acetabular Retroversion but No Other Impingement Parameters
Supplemental material, sj-docx-3-hss-10.1177_15563316261460402 for Symptom Severity due to Femoroacetabular Impingement Syndrome Is Correlated With Radiographic Signs of Acetabular Retroversion but No Other Impingement Parameters by Nicholas R. Kossoff, Manuel A. Romero-Padron and Joshua S. Everhart in HSS Journal®
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was obtained from all participants included in this study per the IRB at Indiana University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.