
Abstract
Background:
Hip fractures in older adults often lead to significant functional decline, dependence, and psychological distress. Fear of falling (FOF) is a common postoperative concern that may restrict mobility, delay rehabilitation, and worsen recovery, particularly among frail individuals. However, in frail older adults with hip fractures, the relationship between FOF and postoperative activities of daily living (ADLs) is not well established.
Purpose:
We sought to examine the prevalence of FOF and its relationship with frailty and ADLs after hip fracture surgery.
Methods:
We conducted a prospective descriptive cross-sectional study in the orthopedics and traumatology clinic of a tertiary university hospital between April 2024 and March 2025. Inclusion criteria were age 65 years or older, radiologically confirmed hip fracture caused by a fall, first hip fracture treated surgically, Mini-Cog score ≥3 indicating preserved cognitive function, Edmonton Frail Scale (EFS) score ≥5 indicating frailty, and provision of written informed consent. Exclusion criteria were major concomitant orthopedic trauma or pathological fracture, postoperative admission to the intensive care unit (ICU), death during ICU stay, and missing or incomplete data during follow-up. Data were collected using the EFS, Falls Efficacy Scale—International, a daily Likert-type FOF scale, and the Barthel Index. Assessments included pre-fracture recall and daily evaluations during the first 4 postoperative mobilization days.
Results:
Of 177 patients included in the study, the mean age was 77.2 years, and 67.8% were women. Pre-fracture FOF was moderate to high. ADL independence declined markedly on the first postoperative day and gradually improved thereafter. FOF peaked during the first mobilization and decreased over subsequent days. Higher FOF was significantly associated with greater frailty and lower postoperative Barthel Index scores. Regression analysis identified FOF, frailty, time to first mobilization, and number of chronic diseases as independent predictors of postoperative functional independence.
Conclusions:
This cross-sectional study found that FOF was highly prevalent after hip fracture surgery and was associated with frailty and reduced functional independence. The findings suggest that integrating routine FOF assessment and early targeted interventions into postoperative care may support safer mobilization and enhance recovery in frail older adults who sustain a hip fracture.
Level of Evidence:
Level IV, prospective cross-sectional study.
Introduction
The aging of the population has led to a steady increase in the incidence of falls and related injuries, making them a major public health concern. 1 Falls are among the leading causes of morbidity and mortality in older adults; approximately 10% result in fractures, most notably hip fractures, which may result in severe consequences.2,3 Individuals may never regain their pre-fracture functional capacity, leading to long-term dependence, reduced quality of life, and increased caregiver burden.4,5
Hip fractures in older adults frequently require surgical intervention, yet only 40% to 60% of patients return to their pre-fracture mobility, and 40% to 70% regain independence in activities of daily living (ADLs).6,7 Approximately 35% lose independent ambulation and 25% require long-term home care. 8 In addition to physical limitations, many patients experience psychological challenges such as depression, anxiety, and fear of falling (FOF). 9 This can contribute to avoidance behaviors, reduced participation in daily activities, loss of muscle strength and balance, social isolation, and further decline.10,11
FOF has been reported even among older adults without a history of falls, with a prevalence of 33% to 46%, while in those with a fall history, the prevalence may reach up to 85%. 12 FOF not only increases the risk of recurrent falls but also prolongs hospitalization and negatively affects rehabilitation.13,14 Furthermore, frailty, a multidimensional syndrome common among hip fracture patients, is closely associated with FOF and poor postoperative recovery.15,16
Despite the importance of FOF in older adults following hip fracture surgery, its relationship with frailty and its potential impact on postoperative functional outcomes remain insufficiently understood. Addressing this gap is critical to optimizing rehabilitation strategies for frail surgical patients. The aim of this study was to investigate the prevalence and severity of FOF, its relationship with frailty and postoperative ADLs, and the factors influencing these outcomes in frail older adults undergoing hip fracture surgery.
AI Use Disclosure: The authors used ChatGPT for language editing and correction during manuscript preparation; it was not used for literature search, data synthesis, or statistical analysis.
Methods
This prospective, descriptive cross-sectional study was conducted in the orthopedics and traumatology clinic of a tertiary university hospital between April 2024 and March 2025. The study was approved by the institutional review board at Celal Bayar University Hafsa Sultan Hospital in Manisa, Turkey. The population consisted of older adults admitted with hip fractures following a fall and treated surgically. Inclusion criteria were age 65 years or older, radiologically confirmed hip fracture caused by a fall, first hip fracture treated surgically, Mini-Cog score ≥3 indicating preserved cognitive function, Edmonton Frail Scale (EFS) score ≥5 indicating frailty, and provision of written informed consent. Exclusion criteria were major concomitant orthopedic trauma or pathological fracture, postoperative admission to the intensive care unit (ICU), death during ICU stay, and missing or incomplete data during follow-up.
A total of 177 patients fulfilled the eligibility criteria and completed baseline assessments. Sociodemographic characteristics (age, sex, marital status, education, living arrangements, comorbidities, and fall history) and clinical variables (fracture type, surgical method, American Society of Anesthesiologists [ASA] classification, pain intensity, time to first mobilization, complications, and length of hospital stay) were obtained from patient interviews and medical records. Data collection was performed face-to-face during hospitalization at predefined time points: baseline (pre-fracture status recalled by patients or caregivers) and on the first 4 postoperative mobilization days.
Frailty was evaluated using the EFS, a multidimensional tool that provides a comprehensive assessment of an individual’s overall vulnerability by considering physical, psychological, and social aspects of health. 17 Total scores range from 0 to 17, with higher values reflecting a greater degree of frailty.
Cognitive status was determined with the Mini-Cog test, a brief screening instrument that combines 3-word recall with a clock-drawing task. 18 It allows rapid identification of patients with potential cognitive impairment. Scores below 3 are generally considered indicative of impaired function.
Pre-fracture FOF was assessed using the Falls Efficacy Scale—International (FES-I) instrument. 19 This includes 16 daily activities, which participants rate on a 4-point scale from “not at all concerned” to “very concerned.” Total scores range between 16 and 64, with higher values reflecting greater fall concern.
Postoperative FOF was measured with a single-item Likert-type question administered daily during the first 4 days of mobilization. Participants were asked, “Are you afraid of falling?” and their response was rated on a 4-point scale ranging from 1 (“not at all”) to 4 (“very much”). This pragmatic approach has been employed in previous orthopedic studies to capture patients’ immediate psychological responses to mobilization.20,21
Functional independence was measured using the Barthel Index of ADLs. 22 This scale assesses 10 essential activities—feeding, bathing, grooming, dressing, bowel and bladder control, toilet use, transfers, mobility, and stair climbing—and provides a score between 0 and 100. Higher scores indicate greater functional autonomy.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics 21.0. Descriptive statistics were reported as mean ± SD, median (interquartile range [IQR]), or frequency (%). Normality was assessed with the Shapiro-Wilk test, and non-parametric methods were used due to skewed distributions. Group differences were evaluated using Mann-Whitney U and Kruskal-Wallis tests, and categorical variables with chi-square tests. Associations between clinical and functional variables were examined with Spearman’s ρ. Changes in Barthel Index scores and daily FOF across postoperative days were analyzed using the Friedman test with Bonferroni-adjusted post-hoc tests. Multiple linear regression was performed to identify independent predictors of postoperative functional independence. Model assumptions and multicollinearity were checked before final analysis. Statistical significance was set at P < .05.
Results
A total of 177 patients were included in the study. The mean age was 77.2 years (SD 8.1; range 65-97), and two-thirds were female (67.8%). More than half of the participants were married (53.7%), and the vast majority were not employed (97.2%). Regarding body mass index, the most common categories were pre-obesity (36.7%) and obesity class I (24.3%). Half of the participants lived with their spouse (50.8%), while 19.2% lived alone. The prevalence of smoking was 14.1%, and the prevalence of alcohol consumption was 2.3%.
A history of falls was reported by 83.6% of the patients, and 54.2% used a walking aid. Polypharmacy was present in 75.7%, and 85.3% had undergone at least 1 previous surgery. The mean number of chronic conditions was 2.0, while only 3.4% had no comorbidities. The most common fracture type was intertrochanteric (83.6%). All patients underwent general anesthesia, and the majority were treated with intramedullary nailing (80.2%). According to the ASA classification, 64.4% were at intermediate risk and 29.4% at high risk. Postoperative complications occurred in 17.5% of patients. The mean time to first mobilization was 30.5 hours (SD 10.6), and the mean length of hospital stay was 7.0 days (SD 1.6).
The pre-fracture level of FOF, assessed using the FES-I, was 37.02 (SD 12.98), reflecting a moderate-to-high degree of concern (Table 1). The mean EFS score was 7.84 (SD 2.86), indicating that the study population was, on average, in the mildly frail range. Functional independence, measured by the Barthel Index, declined markedly from a pre-fracture mean of 87.14 (SD 14.71) to 35.42 (SD 14.52) on the first postoperative mobilization day. Thereafter, scores gradually increased, reaching 45.84 on day 2, 46.47 on day 3, and 48.23 on day 4. Postoperative FOF, assessed with a single-item Likert scale, was highest on the first day of mobilization (mean 2.70 [SD 1.19]). By the second day, the mean had decreased to 2.19 (SD 1.17), and stabilized at 2.17 (SD 0.96) and 2.17 (SD 0.72) on the third and fourth days, respectively, demonstrating a general decline in fear over the mobilization period. In terms of categorical distribution, 36.2% of participants reported being “very fearful” on the first day, whereas by the second day, 41.8% reported being “not fearful at all.” Fear levels then remained relatively stable on days 3 and 4.
Frailty, Functional Independence, and FOF Before and After Hip Fracture Surgery.
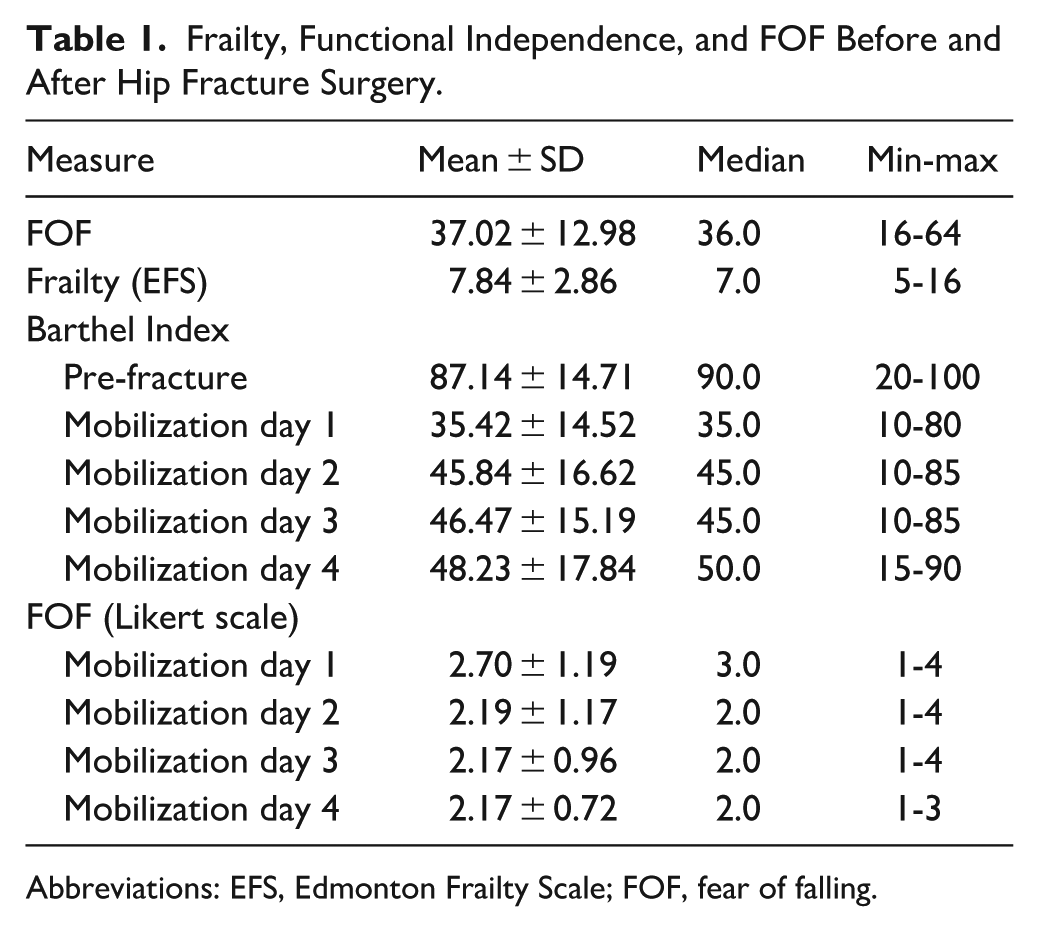
Abbreviations: EFS, Edmonton Frailty Scale; FOF, fear of falling.
Correlation analyses revealed significant associations among frailty, FOF, and functional independence (Table 2). Higher age, greater number of chronic conditions, higher pain scores, longer time to first mobilization, and prolonged length of hospital stay were all negatively correlated with the Barthel Index and positively correlated with both FOF and frailty. In contrast, higher Mini-Cog and Braden Scale scores were positively associated with functional independence and inversely related to frailty and FOF. Notably, frailty (EFS) demonstrated a strong negative correlation with Barthel Index scores (r = −0.41, P < .01) and a positive correlation with FOF (r = 0.36, P < .01). Similarly, higher FOF (FES-I) was significantly associated with reduced functional independence (r = −0.38, P < .01).
Correlation of Clinical and Functional Parameters With Barthel Index, FOF, and Frailty.
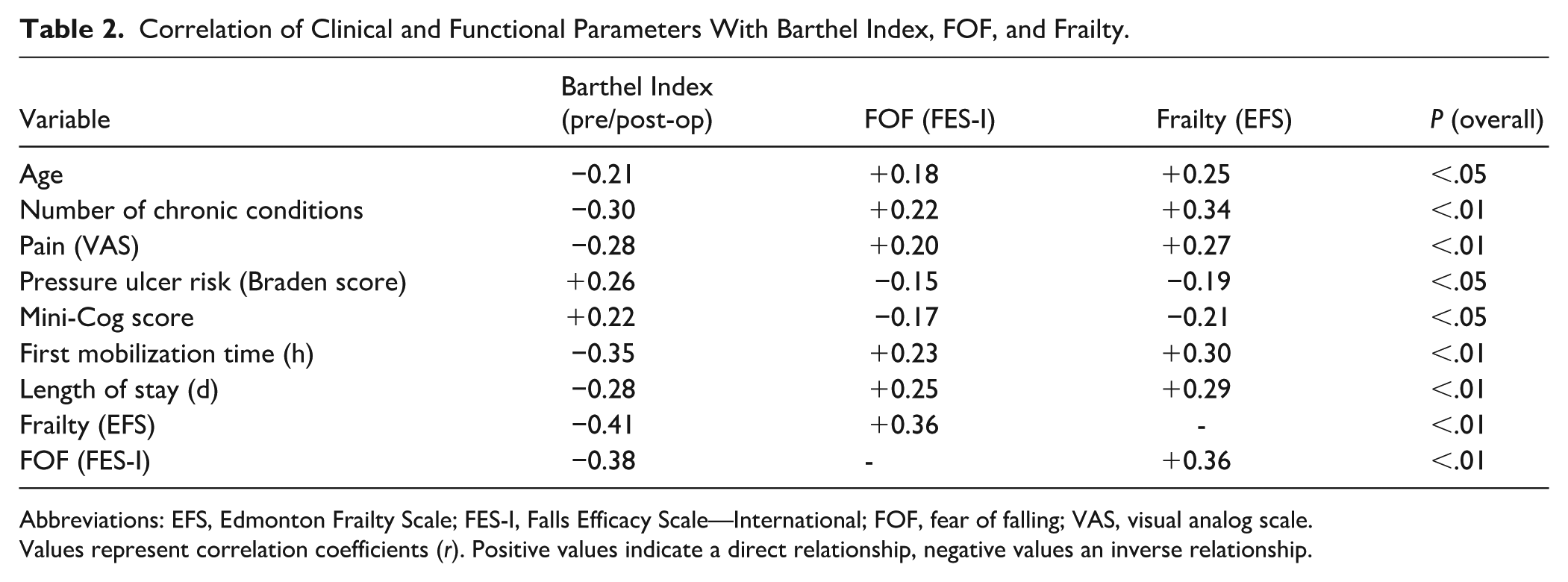
Abbreviations: EFS, Edmonton Frailty Scale; FES-I, Falls Efficacy Scale—International; FOF, fear of falling; VAS, visual analog scale.
Values represent correlation coefficients (r). Positive values indicate a direct relationship, negative values an inverse relationship.
Group comparisons revealed significant differences in functional independence, FOF, and frailty across several sociodemographic and clinical variables (Table 3). Women had lower Barthel Index scores and higher FES-I, EFS, and Likert fear scores than men (all P = .001-.002). Single participants demonstrated poorer functional outcomes, greater FOF, and higher frailty levels compared with married individuals (all P ≤ .009). Patients with polypharmacy, previous surgical history, walking aid use, or a history of falls exhibited significantly lower Barthel Index scores and higher FOF and frailty scores than those without these characteristics (all P < .05). Differences across BMI categories were observed only for frailty (P = .028), with higher EFS scores in obese groups, whereas Barthel Index, FES-I, and Likert fear scores did not differ significantly. Finally, higher ASA grades were associated with significantly lower Barthel Index scores (P = .001), greater frailty (P = .001), and higher FOF, as measured by both the FES-I (P = .017) and Likert scales (P = .020).
Associations Between Patient Factors and Outcomes of Functional Independence, FOF, and Frailty.
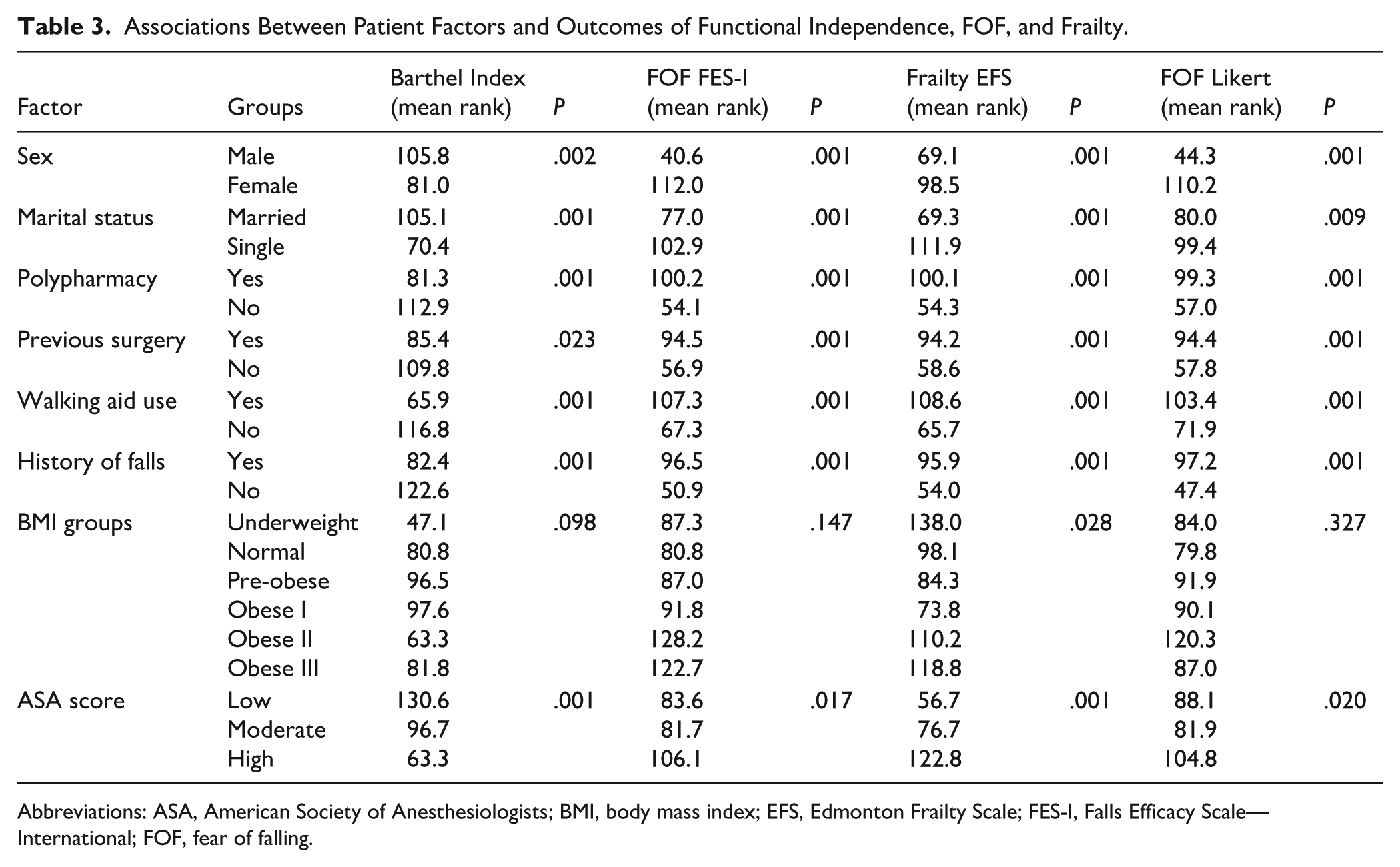
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; EFS, Edmonton Frailty Scale; FES-I, Falls Efficacy Scale—International; FOF, fear of falling.
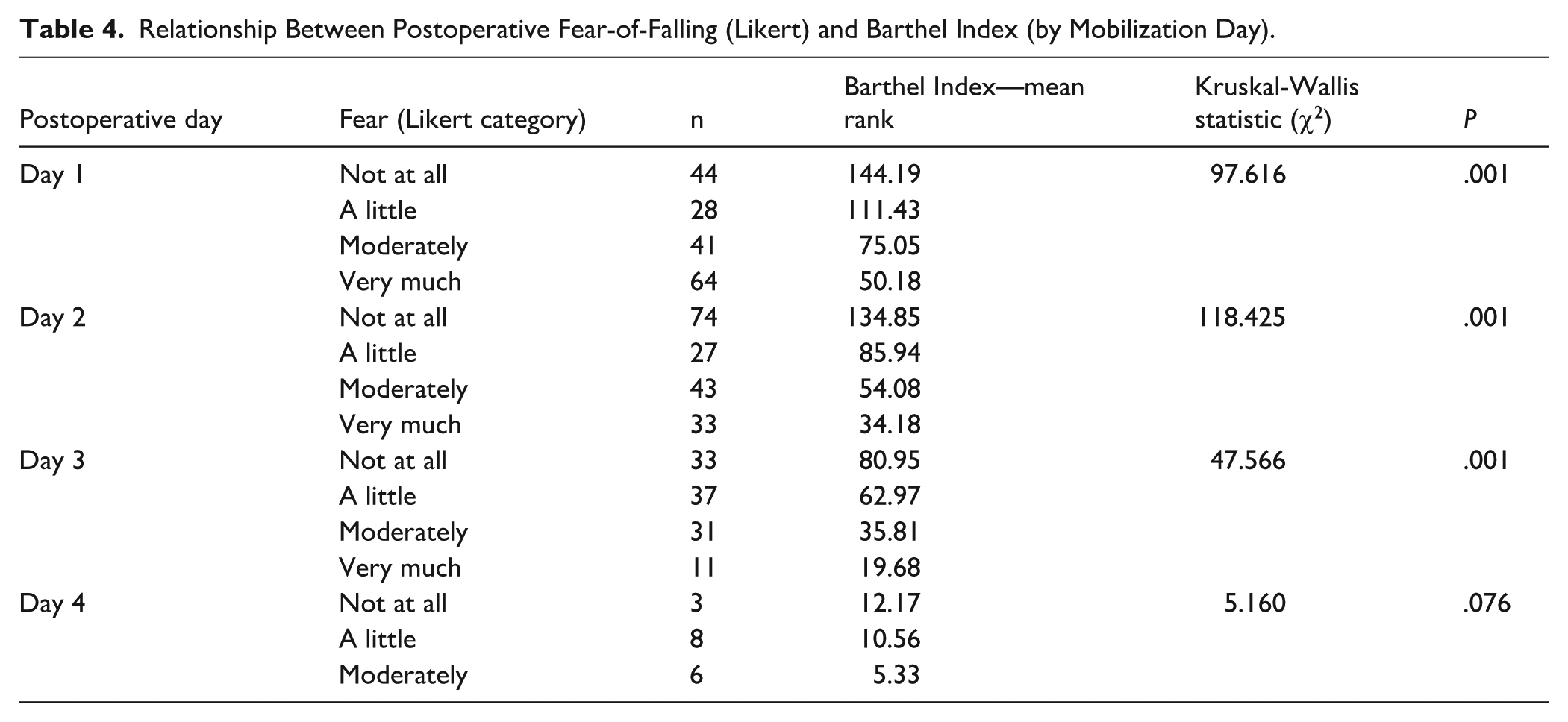
A significant inverse association between FOF and functional independence was observed in daily Kruskal-Wallis analyses (Table 4). On postoperative days 1 to 3, patients who reported “very much” fear consistently had the lowest Barthel Index scores, whereas those with “no fear” demonstrated the highest levels of independence. By day 4, most patients had been discharged, and due to the absence of responses in the “very much” fear category, this pattern persisted but was no longer statistically significant (Figure 1).
Relationship Between Postoperative Fear-of-Falling (Likert) and Barthel Index (by Mobilization Day).
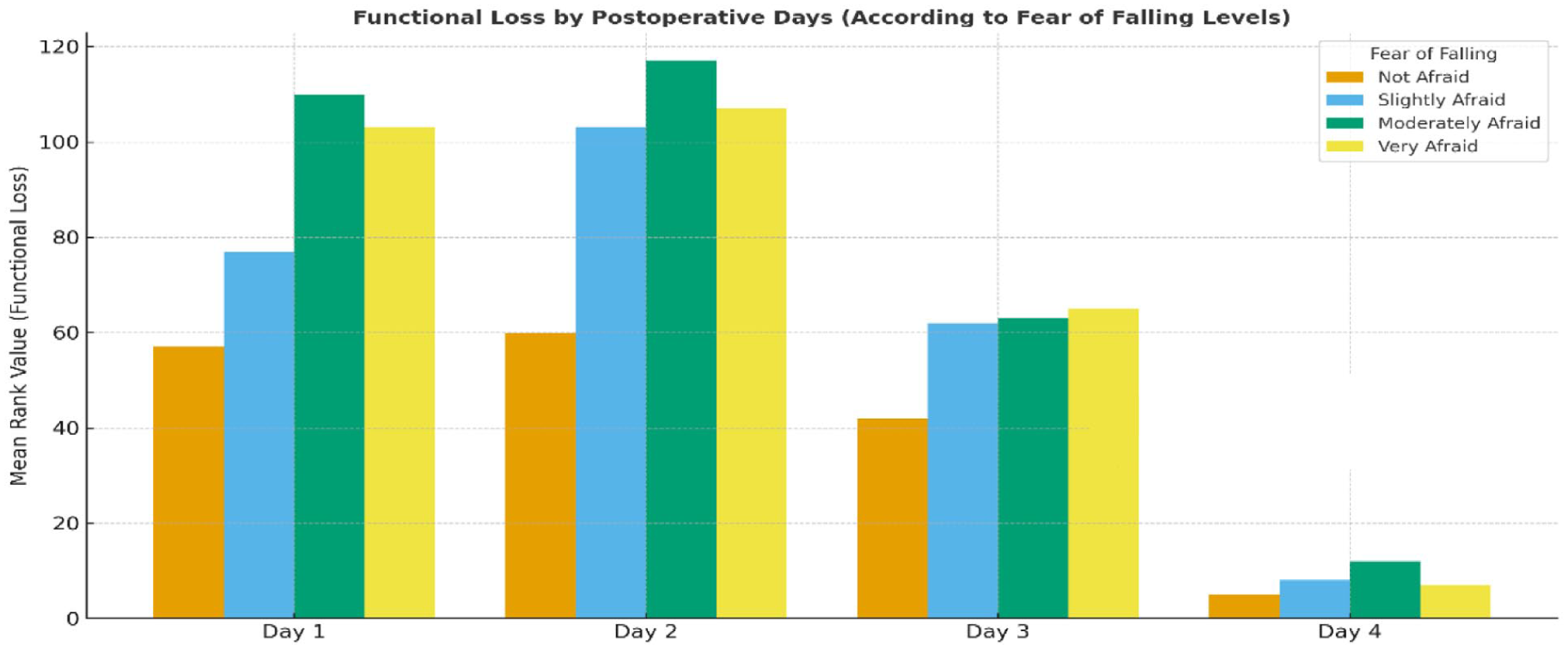
Functional loss by postoperative days according to fear of falling levels.
The Friedman test further confirmed within-subject changes across postoperative days. FOF was highest on the first mobilization day (mean = 3.50) and declined progressively to 3.03 on day 2, 2.18 on day 3, and 1.29 on day 4. In contrast, functional independence decreased sharply from the pre-fracture level (mean = 5.00) to 1.18 on day 1, followed by gradual recovery over days 2 to 4 (2.21, 2.88, and 3.74, respectively). Overall, these findings demonstrate an inverse trajectory between FOF and functional recovery; higher fear was associated with lower functional independence, particularly during the early postoperative period.
In the multiple linear regression model predicting postoperative Barthel Index scores, significant independent predictors included FOF (β = −.32, P < .001), frailty score (β = −.28, P = .002), time to first mobilization (β = −.30, P = .001), and number of chronic diseases (β = −.25, P = .004). The overall model was significant and explained 41% of the variance in functional independence (R2 = 0.41).
Discussion
This cross-sectional study examined the relationship between FOF, frailty, and postoperative functional independence among frail older adults undergoing hip fracture surgery. The findings suggest that FOF may be both highly prevalent and clinically significant in this population, with a measurable negative association with measures of early postoperative functional recovery. Functional independence, as assessed by the Barthel Index, declined sharply following surgery and did not return to pre-fracture levels during hospitalization. FOF peaked during the initial postoperative mobilization and decreased gradually over the following days. These findings suggest that during the rehabilitation process, FOF may act as both a psychological barrier and a behavioral constraint.
This study has several limitations. First, it was conducted at a single tertiary center, which may limit the generalizability of findings to other institutions or populations. Second, although the use of a Likert-type scale for postoperative FOF is common in orthopedic settings, it lacks full psychometric validation, which may limit interpretability. Third, the study relied on patient recall for pre-fracture functional status and fear levels, introducing the potential for recall bias. Fourth, only early postoperative outcomes were assessed, and long-term follow-up data—such as readmission, re-fracture, or mortality rates—were not collected. Lastly, the cross-sectional design does not permit causal inferences. To minimize selection bias, strict inclusion and exclusion criteria were applied, and all participants were consecutively recruited from the same tertiary hospital during the study period. Standardized assessment tools were used across all data collection points to reduce measurement bias. However, recall bias may have affected the accuracy of pre-fracture functional status, as some baseline information was self-reported or reported by caregivers.
The mean age and gender distribution of the sample were consistent with prior research on hip fracture epidemiology, with women comprising nearly two-thirds of the participants.23,24 The predominance of women aligns with known sex differences in bone density, hormonal changes after menopause, and longer life expectancy.25,26 Moreover, the high prevalence of comorbidities, polypharmacy, and previous falls observed in this study echoes findings from prior geriatric cohorts.27,28 These characteristics likely contribute to both increased frailty and elevated FOF, reinforcing the multifactorial vulnerability of this population.
In our study, pre-fracture FOF levels were moderate to high and significantly associated with postoperative functional loss. This finding parallels previous studies demonstrating that pre-existing FOF not only predicts recurrent falls but also delays mobility and reduces participation in rehabilitation.29,30 Importantly, FOF in the current sample remained high immediately after surgery, likely reflecting anxiety related to pain, weakness, and the fear of reinjury. As shown in other orthogeriatric literature, early mobilization often evokes intense apprehension, especially during the first postoperative attempt to stand or walk.20,21 Although FOF gradually declined over time, its persistence may indicate the need for structured psychological and educational interventions during rehabilitation.
The observed inverse correlation between FOF and Barthel Index scores suggests that psychological factors significantly influence functional recovery after hip fracture. Similar associations have been documented by Jaatinen et al 31 and Izadi-Avanji et al, 32 who noted that heightened FOF leads to avoidance of activity, muscular deconditioning, and diminished confidence in balance. This creates a self-reinforcing cycle in which inactivity perpetuates dependence and fear, a phenomenon sometimes referred to as the “fear-avoidance model” of mobility limitation. 10 Thus, our results underscore the importance of addressing psychological barriers concurrently with physical rehabilitation.
Frailty also emerged as a strong predictor of poor functional outcomes and increased FOF. This relationship has been substantiated in prior research, suggesting that frailty predisposes individuals to both physical and psychological vulnerability.16 -33 Frail patients often demonstrate slower recovery, higher complication rates, and prolonged hospitalization following hip surgery.34,35 In the present study, frailty was more pronounced among women, single individuals, and those with polypharmacy; this is consistent with earlier studies.36,37 These findings suggest a need for frailty-sensitive care models that incorporate early psychological support and comprehensive discharge planning.
From a clinical perspective, delayed mobilization emerged as a major determinant of poor recovery. Patients with higher FOF and frailty scores tended to mobilize later, which was associated with longer hospital stays and greater functional decline. Early mobilization protocols have consistently been shown to reduce complications and improve recovery trajectories in orthopedic populations. 38 However, fear often inhibits participation in early ambulation efforts. 39 These findings underscore the bidirectional nature of FOF and mobility: fear limits mobilization, and delayed mobilization sustains fear. Multidisciplinary strategies involving nursing, physiotherapy, and psychological counseling are therefore essential to break this cycle.
Overall, this study suggests that FOF is both an emotional response and a modifiable clinical factor. Addressing it through structured screening and targeted interventions such as patient education, cognitive-behavioral strategies, and graded exposure to mobility tasks may improve functional outcomes.40,41 Nurses, who are at the forefront of postoperative care, play a critical role in recognizing patients’ fear-related cues, fostering their confidence during ambulation, and coordinating multidisciplinary support.
In conclusion, in frail older adults after hip fracture surgery, we observed a high prevalence of FOF. FOF peaked during the early postoperative phase, when early mobilization is crucial, and was significantly associated with reduced functional independence, frailty, and delayed recovery. These findings suggest that FOF may be both psychological and a determinant of postoperative outcomes. Frailty and vulnerabilities such as polypharmacy, previous falls, and limited support further heighten FOF and hinder rehabilitation. Our findings suggest that routine screening of FOF and frailty should be incorporated into postoperative care. Early psychological support, patient education, and confidence-building during mobilization may support recovery. Collaborative approaches among nurses, physiotherapists, and geriatricians can promote independence and quality of life in this population. Future studies should examine the long-term effects of FOF on community reintegration and death rates and evaluate interventions such as cognitive-behavioral therapy, balance training, and telerehabilitation.
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Consent to Participate
Informed consent was obtained from all participants included in this study per the IRB at Celal Bayar University Hafsa Sultan Hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.