
Abstract
Background:
Perinatal opioid use disorder (OUD) remains prevalent in the United States and is associated with unfavorable breastfeeding outcomes, including low likelihood of initiation and decreased duration. Individuals with OUD face heightened risk for traumatic events across the life course, though we know little about how life stress impacts breastfeeding in those with OUD.
Method:
We investigated the differential and sequential impacts of adverse childhood experiences (ACEs) and past-year stressful life events (SLEs) on breastfeeding outcomes in a prospective cohort study of 50 pregnant individuals (100% identified as female, 42% non-Hispanic White, 42% Hispanic/Latina) in treatment for OUD, followed through 5 months postpartum.
Results:
Out of 50 participants, 37 (74.0%) initiated breastfeeding, 16 (32.0%) reported continued breastfeeding in any capacity at 2 months, and 5 (10%) reported exclusive breastfeeding at 2 months. Higher ACE scores were associated with increased odds of breastfeeding initiation (odds ratio [OR] = 3.48, 95% confidence interval [CI]: 1.11–16.34) and longer duration (B = 0.33, 95% CI: 0.04–0.60), suggesting resilience to early childhood adversity. Mediation analyses adjusted for demographic covariates revealed a significant indirect effect from higher ACEs to reduced likelihood of exclusive breastfeeding (β = −0.09, 95% CI: −0.09, −0.001, p = 0.04) via greater SLEs in the year prior to birth (β = 0.33, 95% CI: 0.06, 0.68, p = 0.01).
Conclusions:
Results highlight the importance of addressing both lifetime and recent trauma in clinical settings to improve breastfeeding outcomes in higher-risk populations. Interventions that incorporate social and behavioral support may be particularly beneficial to mitigate the negative impacts of stress on breastfeeding.
Keywords
Introduction
The prevalence of perinatal opioid use disorder (OUD) has increased over fivefold in recent decades from 1.5 per 1,000 hospitalized deliveries in 1999 to 8.2 per 1,000 deliveries in 2017. 1 A 2019 U.S. national survey found that 6.6% of pregnant individuals reported prescription opioid use during pregnancy, with 21.2% further reporting opioid misuse. 2 Perinatal OUD can result in numerous adverse effects for birthing individuals and their infants, including negative impacts on breastfeeding. In particular, studies report disparities in breastfeeding outcomes among individuals with OUD, including shorter breastfeeding duration and lower prevalence of exclusive breastfeeding compared with individuals without OUD.3–5 Breastfeeding contributes to the development of the mother–infant bond and has long-term benefits for infant health and development. 6 Recent population-level data suggest that longer duration of breastfeeding and exclusive breastfeeding are independently associated with lower odds of child language, social, and motor delays, and neurodevelopmental conditions, with the strongest positive effects shown for exclusive breastfeeding. 7 Breastfeeding also offers protective effects specific to perinatal OUD populations. For example, breastfeeding is associated with postpartum OUD treatment retention 8 and significantly improved outcomes for infants exposed to opioids prenatally, including reduced neonatal pharmacological treatment and length of hospital stay. 9 Despite compelling evidence that breastfeeding is advantageous for individuals with OUD and their infants, breastfeeding rates in this population remain suboptimal, indicating a need to identify factors that may support or undermine breastfeeding among birthing individuals with OUD.
Individuals with OUD are at heightened risk for traumatic and stressful life events (SLEs) across the lifespan.10,11 Adverse childhood experiences (ACEs) refer to potentially traumatic events occurring before the age of 18, such as abuse, neglect, and household dysfunction. 12 A substantial body of research has demonstrated that exposure to childhood trauma can disrupt neurodevelopment, leading to earlier initiation of substance use and increased risk for addiction, psychiatric comorbidities, and other health consequences in adulthood. 13 An ACE score of 4 or more is recognized as a clinically significant threshold associated with elevated rates of chronic disease, mental illness, and substance misuse. 14 Indeed, individuals with ACE scores above this threshold are 7–10 times more likely to develop a substance use disorder and have 15 times higher odds of recent opioid misuse. 13
While the association between ACEs and substance use is well established, fewer studies have explored links between ACEs and breastfeeding, and it remains unclear how early adversity may impact breastfeeding outcomes. Some studies suggest that higher ACE scores are associated with breastfeeding difficulties, 15 early cessation of breastfeeding, 16 and reduced likelihood of exclusive breastfeeding. 17 Interestingly, other research has found that elevated ACEs are linked to increased odds of initiating breastfeeding, though not necessarily sustaining it. 18 Still, other studies report no significant association between ACE scores and breastfeeding practices. 19 Further compounding this gap in knowledge, no research has examined the impact of ACEs on breastfeeding behaviors specifically among individuals with substance use disorders, including OUD.
In addition to ACEs, individuals with OUD are at increased risk for proximal (i.e., past-year) SLEs, such as loss of income or housing, death of a loved one, or experiences of violence. 10 SLEs during pregnancy are linked with deleterious postpartum outcomes, including increased likelihood of developing mood disorders, 20 which in turn predict early cessation of breastfeeding, lower likelihood of exclusive breastfeeding, and postpartum substance misuse.21,22 Compared with the mixed literature on ACEs and breastfeeding practices, the effect of proximal stress on breastfeeding is less equivocal. Studies consistently link SLEs during pregnancy with shorter duration and early termination of breastfeeding,23,24 and lower prevalence of exclusive breastfeeding. 25 Understanding how traumatic and stressful experiences influence breastfeeding practices among individuals with OUD can inform interventions that may improve breastfeeding rates and support overall health for the birthing/breastfeeding individual and their infant.
While ACEs and later SLEs may independently influence breastfeeding behavior, it is also plausible that chronic stress—encompassing both early trauma and more proximal life stressors—exerts a cumulative and sequential impact on caregiving practices, including breastfeeding. Prior evidence indicates that early exposure to adversity can disrupt neurobiological and emotional regulatory systems and undermine one’s ability to adaptively respond to later stressors. 26 Several longitudinal studies have demonstrated a positive association between ACEs and later life stress, such that exposure to early stress not only increases the likelihood of subsequent stress exposures but may also diminish one’s capacity to manage or cope with the impact of stressors on functioning. 27 Moreover, chronic and cumulative stress are linked with compromised caregiving behaviors, including lower sensitivity, reduced responsiveness, and diminished emotional availability.28,29 Despite this theoretical foundation, the pathways linking early adversity and more proximal life stress to breastfeeding outcomes remain underexplored and warrant focused investigation.
The current study is the first to explore the differential and sequential impacts of ACEs and SLEs on breastfeeding practices among individuals with OUD. We first sought to document the independent effects of ACEs and SLEs on breastfeeding outcomes (i.e., breastfeeding initiation, duration, and exclusive breastfeeding). Consistent with prior evidence that caregivers with histories of traumatic and stressful experiences are less likely to initiate and maintain breastfeeding to recommended duration,17,21,22,24 we hypothesized that (1) ACEs and SLEs would be associated with lower likelihood of breastfeeding initiation and exclusivity, and shorter duration of breastfeeding; (2) past-year SLEs would have a larger impact on breastfeeding outcomes than more distal ACEs, given their proximity; and (3) pathways from ACEs to breastfeeding practices would be explained (i.e., mediated) by SLEs in the year prior to giving birth, such that ACE score would be positively associated with SLEs during pregnancy, which in turn would lead to lower breastfeeding initiation, duration, and exclusivity. Understanding the effects of stress on breastfeeding in this population can inform clinical guidelines and recommendations, such as promoting ACE/SLE screening and tailored breastfeeding education in perinatal and/or OUD treatment clinical settings.
Materials and Methods
Study population
Data were drawn from a prospective cohort study of pregnant people with OUD enrolled during the third trimester and followed through 5 months postpartum. 30 Participants were recruited in Tucson and Phoenix, Arizona, via clinical settings and community events. Eligible participants were (1) between the ages of 18 and 40 years, (2) at least 30 weeks gestation with an uncomplicated singleton pregnancy, (3) expected to live with the infant after childbirth, (4) enrolled in a treatment program for OUD with plans to continue treatment postpartum, and (5) fluent in English. Exclusion criteria included a planned long-distance move within the 6 months following enrollment.
Study procedures and measures
All study procedures were approved by the Institutional Review Board of the participating university. At the enrollment/baseline visit (gestational week 36 or beyond), participants provided informed consent and completed surveys to capture demographics and history of opioid use and treatment. Participants also completed an audio-recorded semi-structured interview of lifetime adversity exposure, which included the 10-item ACE scale 12 and the 14-item SLE scale. 31 On both scales, individual items were rated as 1 (present) or 0 (absent) and were scored as continuous count variables per developer instructions. Sum scores for ACEs and SLEs were included as predictors in analyses. After childbirth, on a daily basis, participants responded to a researcher-created item to capture how they fed their infants by reporting either (1) only breastmilk (via direct feeding or pumping), (2) a combination of breastmilk and formula, or (3) only formula. The daily assessment of infant feeding continued through 12 weeks postpartum, with additional daily assessments for 1 week preceding follow-up visits at postpartum months 4 and 5. Breastfeeding outcome variables included (1) whether participants initiated breastfeeding, defined as feeding the baby with their breastmilk (nursing or pumping) at any point during the study; (2) overall duration of breastfeeding in weeks, measured as the final study week in which the participant reported any breastfeeding and/or pumping; and (3) whether participants practiced exclusive breastfeeding at 8 weeks postpartum. We elected to measure exclusive breastfeeding at 8 weeks, as infants exposed to opioids in utero may spend up to several weeks in intensive care or specialized nurseries, 9 settings in which exclusive breastfeeding may not be possible. In the current sample, all infants for whom data were available were living at home with the birthing parent by 8 weeks postpartum, and all breastfeeding participants had initiated breastfeeding by this time point.
Statistical analyses
Study variables were examined prior to analyses to evaluate distributional assumptions for parametric statistics 32 and were found to be normally distributed. Descriptive statistics characterized participant demographics, ACEs, SLEs in the year prior to childbirth, and breastfeeding behavior. We performed regression analyses in R version 4.2.3. To assess the independent effects of stressors on breastfeeding behavior, breastfeeding variables were regressed on ACEs and SLEs using linear or logistic regression models depending on whether the outcome was binary (i.e., initiation, exclusive breastfeeding) or continuous (i.e., duration). Adjusted models included ACEs and SLEs as predictors and controlled for demographic covariates, including participant age, educational attainment (completed high school yes/no), and parity (number of births; range 1–8), as these factors have been associated with breastfeeding outcomes in prior studies.33,34 To assess whether ACEs and SLEs sequentially influenced breastfeeding behavior, we employed mediation with robust test statistics and standard errors and bias-corrected and accelerated 95% confidence intervals. We tested three mediation models with ACE score as the independent variable and SLE score as the mediator. Breastfeeding outcomes were included as dependent variables, with separate models predicting breastfeeding duration (continuous variable) using linear regression and breastfeeding initiation and exclusivity (binary variables) using probit regression. Mediation models controlled for demographic covariates described above. T-tests and chi-square analyses identified no statistically significant differences in study variables or participant demographic characteristics between those who completed only the baseline visit (n = 7) and those who returned postpartum (n = 43).
Results
Participant characteristics are presented in Table 1. Fifty women enrolled in treatment for OUD were included in the study. Of the 50 participants who completed the prenatal baseline assessment, 43 (86%) completed at least one follow-up postpartum assessment to measure breastfeeding outcomes, and 38 (76%) were retained in the study at 8 weeks postpartum. The majority of participants were multiparous, with 2.88 births (inclusive of study infant) on average. The average ACE score was 6.2 (SD 2.6), and the average SLE score was 4.5 (standard deviation [SD] 3.0). Out of 50 participants, 37 (74.0%) reported initiating breastfeeding. The number of participants who reported continued breastfeeding in any capacity at 2 months was 16 (32.0%), with 5 participants (10%) exclusively breastfeeding at 2 months.
Sample Characteristics (N = 50)
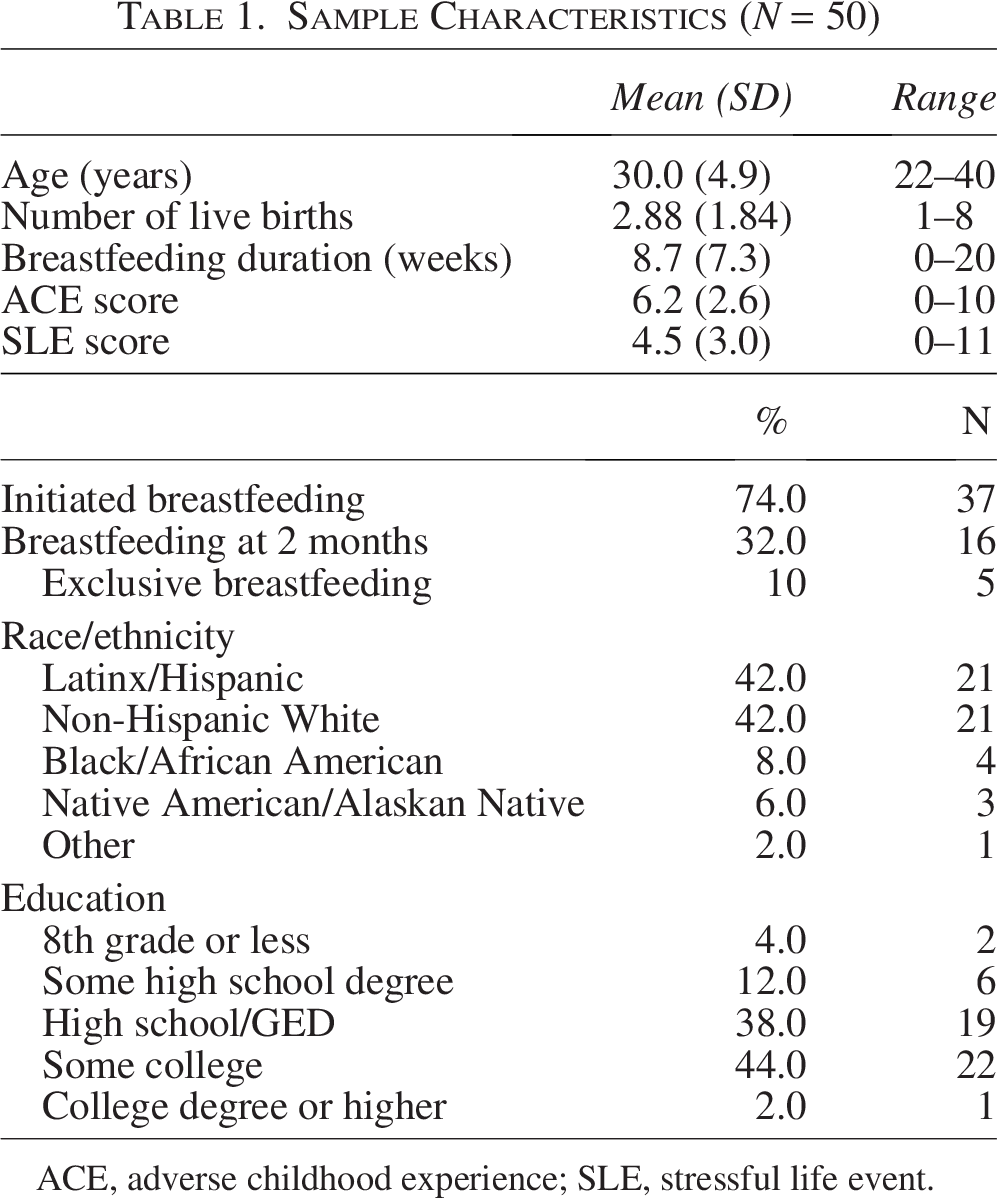
ACE, adverse childhood experience; SLE, stressful life event.
To test our first hypothesis that ACEs and SLEs would be differentially associated with breastfeeding outcomes, we regressed breastfeeding initiation, duration, and exclusive breastfeeding on ACE scores and SLE scores in unadjusted and covariate-adjusted models (Table 2). ACE scores were positively associated with all breastfeeding outcomes, though this effect reached statistical significance only in adjusted models predicting breastfeeding initiation (odds ratio [OR] = 3.48, 95% CI: 1.11–16.34) and duration (B = 0.33, 95% CI: 0.04–0.60). These results indicate that higher ACE score predicted greater likelihood of initiating breastfeeding and longer duration of breastfeeding above and beyond the effects of SLEs and demographic covariates. SLE scores were not significantly associated with breastfeeding outcomes in either unadjusted or adjusted models.
Unadjusted and Adjusted Effect Estimates of ACEs and Stressful Life Events on Breastfeeding Outcomes
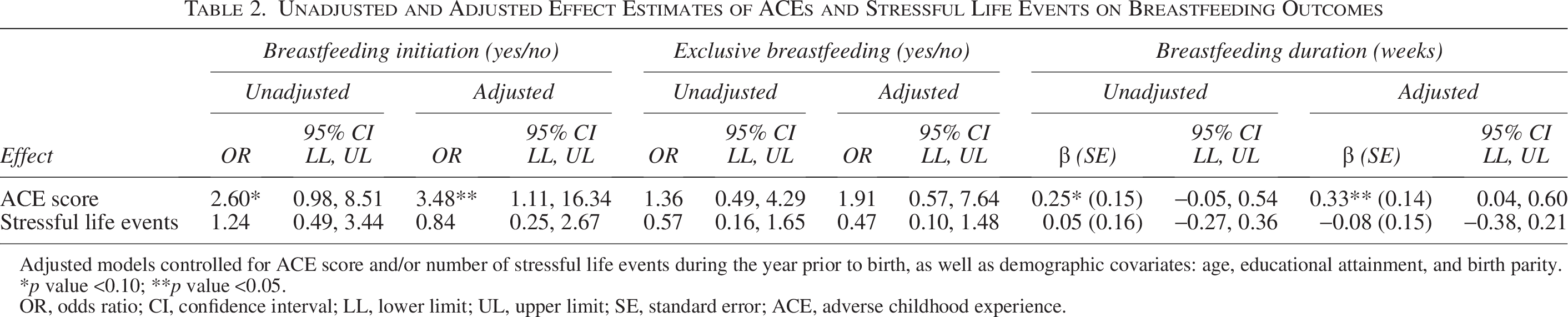
Adjusted models controlled for ACE score and/or number of stressful life events during the year prior to birth, as well as demographic covariates: age, educational attainment, and birth parity.
p value <0.10; **p value <0.05.
OR, odds ratio; CI, confidence interval; LL, lower limit; UL, upper limit; SE, standard error; ACE, adverse childhood experience.
To assess our second hypothesis that ACEs and more proximal SLEs sequentially influence breastfeeding practices, we tested mediation models controlling for demographic covariates (Table 3). As predicted, ACEs were positively and significantly associated with SLEs in two of the three models, such that higher ACEs prior to age 18 predicted more SLEs in the year prior to childbirth (Fig. 1). Further, there were significant direct effect pathways from ACEs to breastfeeding initiation (β = 0.52, 95% CI: [0.06, 0.98], p = 0.03; Fig. 1A) and duration (β = 0.34, 95% CI: [0.08, 0.61], p = 0.01; Fig. 1C). SLEs did not significantly mediate these paths. Conversely, there was a significant indirect effect from higher ACEs to exclusive breastfeeding via SLEs (β = −0.09, 95% CI: [−0.09, −0.001], p = 0.04), such that ACEs predicted greater SLEs in the year prior to childbirth (β = 0.33, 95% CI: [0.06, 0.59], p = 0.01), which, in turn, predicted lower likelihood of exclusive breastfeeding (β = −0.27, 95% CI: [−0.41, −0.14], p = 0.001).
Mediation Results Showing the Effect of Adverse Childhood Experiences on Breastfeeding Initiation, Duration, and Exclusive Breastfeeding Through Stressful Life Events in the Year Prior to Childbirth
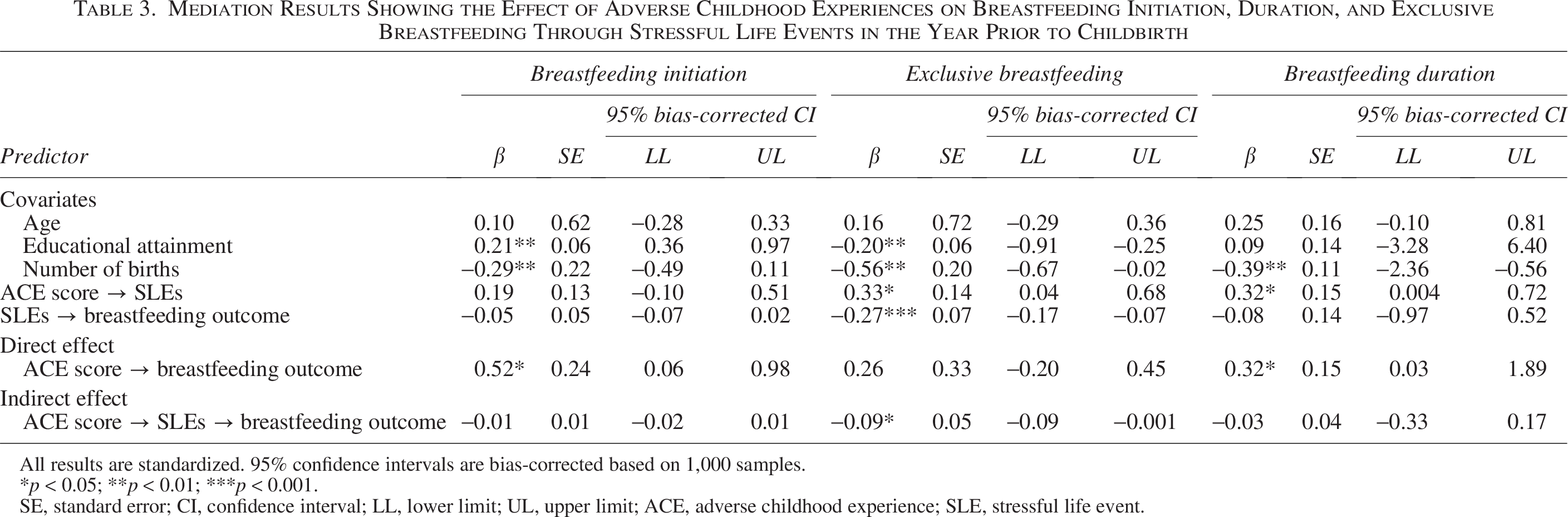
All results are standardized. 95% confidence intervals are bias-corrected based on 1,000 samples.
*p < 0.05; **p < 0.01; ***p < 0.001.
SE, standard error; CI, confidence interval; LL, lower limit; UL, upper limit; ACE, adverse childhood experience; SLE, stressful life event.
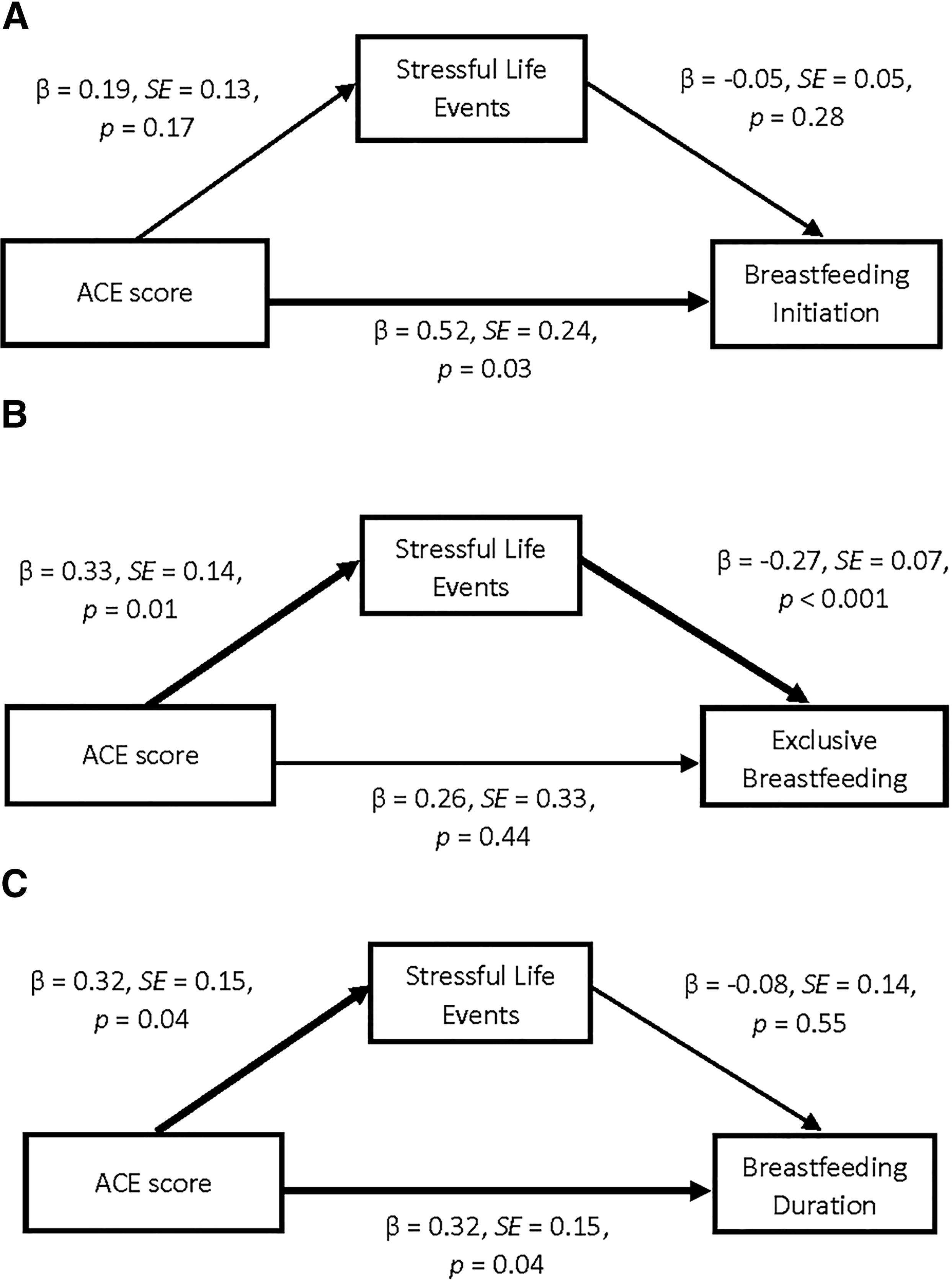
Figure 1 shows mediation pathways from adverse childhood experiences (ACEs) to breastfeeding outcomes via recent stressful life events (SLEs). Panels
Discussion
This study explored associations between ACEs, SLEs in the year prior to childbirth, and breastfeeding outcomes among a sample of 50 birthing individuals in treatment for OUD. Early adversity arose as a significant risk factor in this sample, with well over half of participants scoring above the clinically significant threshold of four ACEs. This high average ACE score aligns with prior evidence linking elevated childhood trauma exposure with the development of substance use disorders. 13 Furthermore, we found that while the majority of participants initiated breastfeeding (74.0%), the prevalence of continued breastfeeding (32.0%) and exclusive breastfeeding (10.0%) at 2 months was considerably lower than the national average of 45.3%. 35 Regression models demonstrated that higher ACE scores were linked with an increased likelihood of initiating breastfeeding and continuing it for a longer duration. Conversely, an indirect effect was observed for exclusive breastfeeding, such that individuals with higher ACE scores experienced more SLEs in the year prior to birth, which were associated with a reduced likelihood of exclusive breastfeeding.
The steep declines in breastfeeding and low prevalence of exclusive breastfeeding observed in our sample are consistent with findings from extant studies among individuals with substance use disorders, including a New Mexico study reporting 10% exclusive breastfeeding at 2 months 3 and a Boston study reporting only 6% of birthing individuals with OUD maintained exclusive breastfeeding at 3 months. 4 These findings reflect persistent disparities in breastfeeding practices among women with substance use disorders, particularly in sustaining exclusive breastfeeding during the early postpartum period. This is especially concerning given clinical recommendations for breastfeeding among those with OUD. 36
Despite overall lower breastfeeding rates, our results provide novel insights into the potential role of early life adversity in shaping maternal caregiving behaviors. Specifically, higher ACE scores were significantly associated with a greater likelihood of breastfeeding initiation and longer breastfeeding duration, even after controlling for demographic variables and recent life stress. These findings align with prior work suggesting that early adversity does not uniformly impair maternal functioning and may, in some cases, foster compensatory caregiving behaviors or resilience in adulthood.37,38 It is likely that individuals in our treatment-seeking sample had access to mental health counseling, supportive resources, and trauma treatment, which may have bolstered their capacity to process and cope with early adversity. In addition, it is plausible that some individuals with greater childhood trauma exposure were actively striving to break negative intergenerational cycles. Parents may be particularly motivated to provide nurturing and responsive care to their children in spite of—or even because of—their own experiences of childhood vulnerability. 39 Qualitative evidence from survivors of child maltreatment supports this hypothesis, indicating that many parents with high ACE scores aim to provide better care for their own children than they received in childhood. 40 In the current sample, participants with high ACE scores may have recognized the numerous benefits of breastfeeding for their own emotional well-being, for their child’s physical and developmental health, and for enhancing the parent-child bond,6,7,9 thus leading to increased motivation to initiate and sustain breastfeeding. Notably, these potential resilience effects emerged only in covariate-adjusted models, suggesting that demographic and contextual variables may obscure the impact of ACEs on breastfeeding practices in unadjusted analyses.
In contrast, SLE scores were not significantly associated with breastfeeding outcomes in either unadjusted or adjusted regression models, suggesting that proximal stress in the year prior to childbirth may not independently predict whether individuals with OUD initiate or maintain breastfeeding. However, our mediation analyses offered a more nuanced illustration of how compounding ACEs and SLEs influence maternal behavior. As hypothesized, ACE scores were positively and significantly associated with SLEs, consistent with the well-documented cascade of adversity across the life course.26,27 While direct effects from ACEs to greater likelihood of breastfeeding initiation and longer breastfeeding duration remained significant in these models, a significant indirect effect pathway emerged for exclusive breastfeeding. Namely, higher ACEs predicted more SLEs, which in turn predicted lower likelihood of exclusive breastfeeding. This finding underscores the specific vulnerability of exclusive breastfeeding to recent or proximal stress and suggests that while early adversity may foster resilience in breastfeeding initiation and continuation, this protective effect can be disrupted by cumulative or ongoing stressors.
Importantly, the distinction between breastfeeding initiation and exclusive breastfeeding is clinically meaningful. Exclusive breastfeeding requires sustained effort, consistency, and access to resources and support, which may be more easily disrupted by acute stress and environmental instability. 25 In this sample, birthing individuals with high ACEs demonstrated motivation to initiate breastfeeding and had adequate coping capacity to maintain some level of breastfeeding across the early postpartum. However, few were able to maintain exclusive breastfeeding through 2 months postpartum, suggesting that exclusive breastfeeding demands a level of continuity and support that is less attainable in the context of ongoing life stress. These findings highlight the importance of distinguishing between different breastfeeding outcomes, and recognizing the complex effects of cumulative stress, including potential deleterious impacts of early stress on the successful negotiation of later stressful experiences.26,27 For birthing individuals with OUD, recent or ongoing stressors may undermine the capacity to meet exclusive breastfeeding goals, even in the presence of earlier trauma-related resilience. Without adequate support and intervention, these breastfeeding parents and their infants may miss out on the known benefits of exclusive breastfeeding. 7
Strengths and limitations
Though prior studies have focused on breastfeeding outcomes in the context of OUD treatment, the present study is the first to investigate how potentially traumatic experiences, including ACEs and proximal SLEs, shape breastfeeding in this population. Our sample, while relatively small, offered adequate variability in ACEs, SLEs, and breastfeeding practices to test hypothesized pathways. This study is further strengthened by the use of validated measures of early adversity and life stress and repeated assessments of breastfeeding across the postpartum. Despite these strengths, several limitations qualify the interpretation of study findings while pointing to directions for future research. First, samples of pregnant and postpartum individuals with OUD are traditionally difficult to recruit and retain (e.g., due to competing treatment demands; fear of legal and child protective consequences 41 ). As a result, modest sample size and participant attrition meant this study was potentially underpowered to detect more subtle associations, and we were not able to model complex causal pathways (e.g., cross-lagged models, moderated mediation). Furthermore, although our sample was racially and ethnically diverse, recruitment was limited to one southwestern U.S. state, potentially limiting the generalizability of study findings. Next, all participants were enrolled in OUD treatment, which may have led to a relatively higher functioning sample of individuals with OUD. Lastly, all data were based on self-report and may have been influenced by social desirability and/or recall bias.
Future studies should aim to recruit larger and nationally representative samples of pregnant individuals with OUD and perform repeated assessments with objective measurements beyond the early postpartum to both replicate and expand the current findings. Longitudinal studies are needed to confirm these pathways and to evaluate whether interventions targeting trauma and stress can improve breastfeeding outcomes in women with OUD. In particular, there is a need for future research to explore additional mechanisms—such as resilience, maternal identity, and support systems—linking childhood adversity to caregiving behaviors. Furthermore, measuring stress biomarkers such as cortisol can add a physiological component that complements self-report data.
Clinical implications
The current findings highlight the importance of trauma-informed care in both perinatal and substance use treatment settings. Screening for ACEs and recent SLEs can help identify birthing individuals who, despite significant adversity, demonstrate motivation to breastfeed and who could benefit from targeted support—particularly to sustain exclusive breastfeeding. While breastfeeding initiation rates in our sample were close to national averages (74.0% versus 83.2%), the rates of continued and exclusive breastfeeding were substantially lower (10.0% versus 45.3%). 35 This pattern of relatively high breastfeeding initiation with substantial reductions in breastfeeding by 2 months postpartum suggests that although many mothers with OUD begin breastfeeding, additional support is needed to maintain it over time. Mothers with substance use disorders often encounter unique challenges to sustained breastfeeding, including stigma, limited postpartum follow-up, and inconsistent provider messaging. 5 Enhanced education for both patients and health care providers regarding the safety and benefits of breastfeeding while taking medication for OUD may help minimize misinformation and encourage longer breastfeeding duration.
Further, lactation support beyond hospital discharge may be particularly beneficial for helping mothers with OUD. Peer counseling, home visits, and community-based lactation services have shown promise in improving breastfeeding outcomes in high-risk groups. 42 Integrated or multidisciplinary care models may also improve breastfeeding outcomes for individuals with OUD. For example, Hensel and colleagues 43 reported a 95% breastfeeding initiation rate among mothers receiving multidisciplinary perinatal care, though ongoing and exclusive breastfeeding outcomes were not assessed. Integrated care can provide consistent, nonjudgmental support across clinical domains, thereby enhancing patient trust and continuity of care. In addition, economic and social supports, including stable housing, childcare, and food security, may reduce external stressors that can interfere with exclusive breastfeeding. 5 In summary, our findings suggest that higher ACE scores may be linked to increased breastfeeding initiation and duration—possibly reflecting resilience or compensatory caregiving behaviors. However, exclusive breastfeeding remains markedly low and appears more vulnerable to the effects of recent life stress, highlighting the value of comprehensive support.
Authors’ Contributions
L.B.L.-K.: Conceptualization (equal); data curation (lead); investigation (supporting); formal analysis (lead); methodology (equal); software (lead); visualization (equal); writing—original draft (equal); review and editing (equal). C.J.R.: Conceptualization (equal); data curation (supporting); methodology (equal); visualization (equal); writing—original draft (equal); review and editing (equal). L.R.: Conceptualization (supporting); funding acquisition (supporting); investigation (supporting); methodology (supporting); writing—review and editing (equal). S.T.: Conceptualization (supporting); funding acquisition (supporting); investigation (supporting); methodology (supporting); writing—review and editing (equal). A.M.A.: Conceptualization (equal); funding acquisition (lead); investigation (lead); methodology (supporting); supervision (lead); writing—review and editing (equal).
Footnotes
Author Disclosure Statement
The authors have no disclosures or conflicts of interest to report.
Funding Information
Funding for this work was provided by NIH/NICHD DP2HD105541 awarded to the senior author.