
Abstract
Objectives:
To define the safe weight loss percentile threshold for the development of hypernatremia by using the “early weight loss nomograms.”
Methods:
This retrospective study included exclusively breastfed healthy neonates over 36 weeks’ of gestation. (n = 450). Daily percentage points of weight loss were plotted on the “early weight loss nomograms for exclusively breastfed neonates.” The presence of hypernatremia was checked if infants lost ≥5% of their birth weight. Hypernatremia was classified as mild, moderate, or severe. The relation of weight loss rates and percentiles to development of hypernatremia was assessed.
Results:
The mean gestational age was 38.6 ± 1.3 (36.0–42.3) weeks; the mean birth weight was 3,200 ± 482 g. The mean total weight loss percentage before discharge was 5.9% ± 1.6% (0.5%−17%). The weight loss percentages within first 24 hours were similar in infants born via cesarean section or vaginal delivery (6% ± 1.6% vs. 5.4% ± 1.7%). Mild or moderate hypernatremia developed in 145 infants (32.2%). ROC analyses showed that weight loss of ≥5.5% could predict the development of hypernatremia (AUC = 0.665) and weight loss of ≥7% could predict the development of moderate hypernatremia (AUC = 0.915). Weight loss percentile of ≥75 could also predict the development of hypernatremia with 73% sensitivity and 46% specificity (AUC = 0.622).
Conclusion:
To the best of our knowledge, this is the first study to evaluate the relationship between weight loss nomogram percentiles and the development of hypernatremia. Even if the weight loss is within the defined acceptable normal ranges and percentiles, hypernatremia may develop if the weight loss is greater than the 75th percentile values.
Introduction
Breast milk is a sustainable, safe, and nutritious food which is essential for the health and survival of babies. 1 After birth, the amount of colostrum consumed by the newborn is low. This is reflected in clinical practice as initial postnatal weight loss. Although this short period of low enteral milk intake and weight loss is well tolerated by many newborns, some may develop complications such as hyperbilirubinemia and hypernatremic dehydration. 2
Daily weight measurement after birth is important for neonatal follow-up because many decisions, such as the timing of discharge or the need for lactation support, are based primarily on weight loss rates. The excessive weight loss can result in hypernatremia in the newborn. Flaherman et al. have defined early weight loss nomograms in infants of gestational age ≥36 weeks according to mode of delivery, with the aim of developing a detailed graphical representation of early weight loss to aid clinical care of well newborns. They described the 50 to 95 percentiles of weight loss by hours since birth and concluded that more than a quarter of the newborn infants loose ≥10% of their birth weight by 72 hours of age. Their study was designed to predict the development of weight loss rates by age rather than the relationship between weight loss and the development of hypernatremia. 2 The aim of the present study is to evaluate the clinical validity of early weight loss nomograms to describe a safety percentile zone with respect to the development of hypernatremia in neonates.
Materials and Methods
This retrospective observational study was conducted in a baby friendly university hospital between December 2021 and January 2023, after local ethics committee approval. Written informed consent was obtained from the parents. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Exclusively breastfed healthy singleton neonates with a gestational age of 36 weeks or more were included in the study. The mothers had lactation consultancy prior to delivery and in the postpartum first day according to the baby friendly hospital policies. The antepartum history, perinatal data including gestational age, birth weight, sex, and mode of delivery were recorded. Neonates were cared in the well baby nursery and weighed daily while naked. Daily percentage points of weight loss were plotted on the weight loss nomograms for exclusively breastfed neonates defined by Flaherman, et al. 2 These early weight loss nomograms show the percentiles of weight loss by mode of feeding and are intended to be used for the early identification of neonates on a trajectory for greater weight loss and associated morbidities. The appropriate nomograms for exclusively breast feeding according to the mode of delivery of the newborn were used in the study. This study attempted to define the weight loss percentile threshold for the development of hypernatremia.
The presence of hypernatremia was checked in infants with a daily weight loss of 5% or more of their birth weight as per unit protocol. Neonatal hypernatremia is defined as mild, moderate, or severe according to the serum sodium (Na) levels of 145–149 mmol/L, 150–169 mmol/L, and above 170 mmol/L, respectively. 3
Statistical analysis was performed using IBM SPSS 28.0.0.0 (IBM SPSS for Windows version 28, Armonk, NY, USA). The Shapiro–Wilk test and histogram plots were used to test the normality of continuous variables. Descriptive statistics are presented as mean ± standard deviation, median (min–max) for continuous variables, and n (%) for categorical variables. Correlation analysis was performed using the Spearman correlation test. ROC analysis was performed to assess the diagnostic performance of weight loss percentage for the development of hypernatremia.
Results
A total of 450 infants were evaluated during the study period. The mean gestational age of infants was 38.6 ± 1.3 (36.0–42.3) and the mean birth weight at birth was 3,200 ± 482 g. Cesarean delivery rates were significantly higher than spontaneous vaginal deliveries (65.8% vs. 34.2%, p = 0.03). Nearly half of the infants were male (49.3%). Weight loss percentages within the first 24 hours were similar between infants born with cesarean delivery or spontaneous vaginal delivery (6 ± 1.6 vs. 5.4 ± 1.7). The mean total weight loss percentage before discharge was 5.9 ± 1.6 (0.5–17). The clinical and laboratory characteristics of the infants are detailed in Table 1.
Clinical and Laboratory Characteristics of Newborn Infants
Mild hypernatremia: serum Na level between 145 and 149 mmoL/L.
Moderate hypernatremia: serum Na level between 150 and 169 mmoL/L.
The relationships of the development of moderate hypernatremia with daily weight loss percentage and weight loss nomogram percentiles were assessed in the present study. According to the early weight loss nomograms of exclusively breastfed newborns, 67 newborns (14.9%) had weight loss rates below 50 percentiles of the nomogram and 109 infants (24.2%) had a weight loss rate of above 95 percentiles of the nomogram within first 24 hours. The percentile distribution of the infants is shown in Table 2.
Early Weight Loss Percentiles of Newborn Infants
Mild or moderate hypernatremia developed in 145 infants (32.2%). None of the infants developed severe hypernatremia (Table 1). A positive correlation was found between the percentage of weight loss and serum Na levels (r = 0.292; p = 0.001; p < 0.01).
ROC analyses showed that weight loss of 5.5% or more from birth weight could predict the development of hypernatremia with 72% sensitivity and 55% specificity (AUC = 0.665) and weight loss of 7% or more at 24 hours of life could predict the development of moderate hypernatremia with 90% sensitivity and 83% specificity (AUC = 0.915) (Fig. 1). The negative predictive values for weight loss of 5.5% or more and %7 or more for the development of hypernatremia were 53.2% and 61.9%, respectively. When plotted on nomograms, a weight loss of 5.5% in the first 24 hours corresponds to the 75th percentile on the Flaherman early weight loss nomograms, and a weight loss of 7% or more in the first 24 hours corresponds to the >95th percentile.
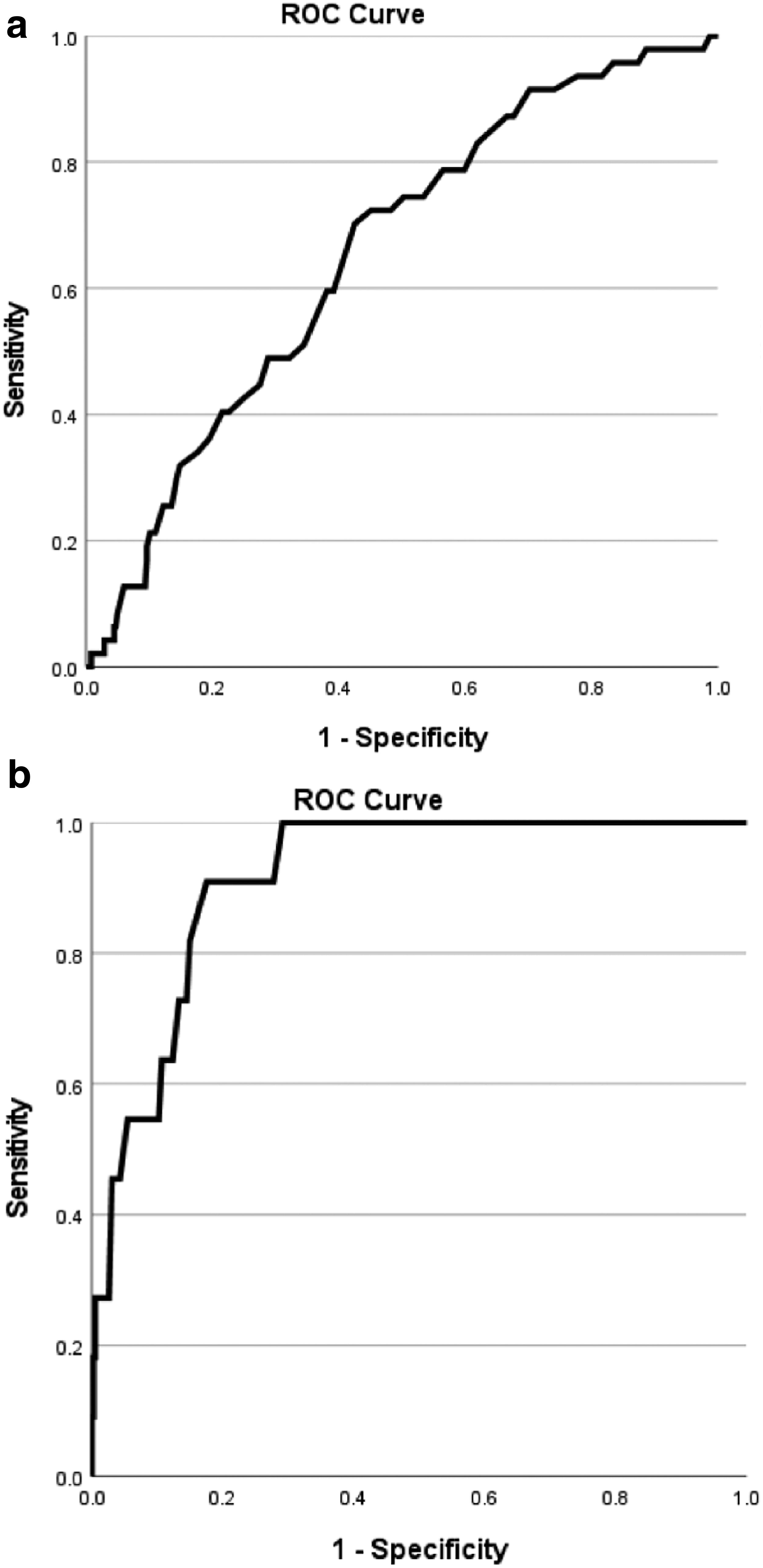
ROC analysis for weight loss percentage within first 24 hours and the development of hypernatremia.
It was also found that a weight loss per centile of 75 or higher could predict the development of hypernatremia with 73% sensitivity and 46% specificity (AUC = 0.622) (Fig. 2). The negative predictive value of weight loss below the 75th percentile for development of hypernatremia was 66.5%.
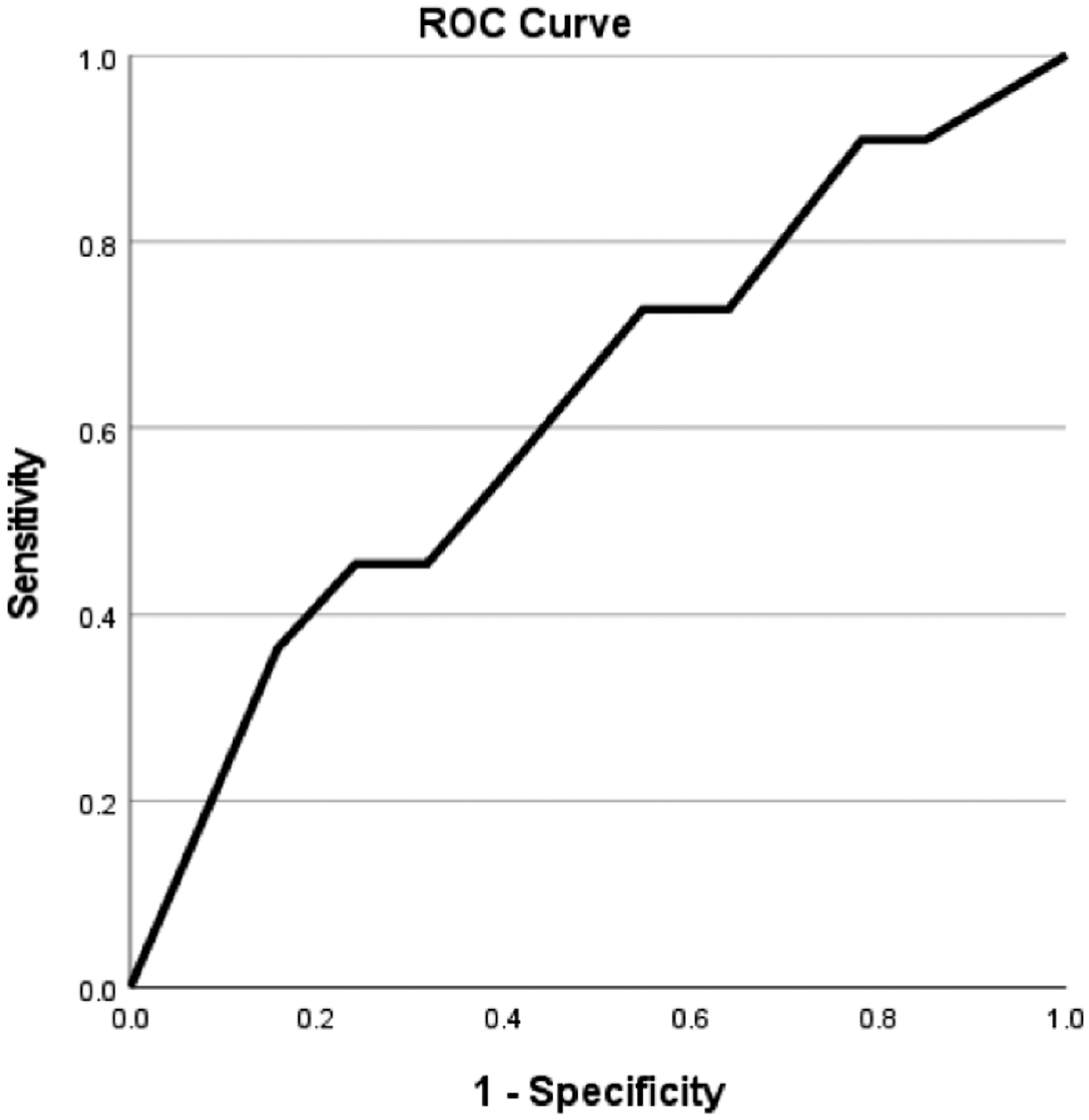
ROC analysis for weight loss nomogram percentile >75th and the development of hypernatremia.
Discussion
Healthy neonates lose weight as a result of body fluid adjustment and physiological diuresis of extracellular fluid following the transition to extrauterine life. The upper limit of normal physiological weight loss in exclusively breastfed newborns is accepted to be 5.5–6.6% of birth weight. This weight loss mostly occurs between the 2nd and 3rd day of life. 4 More recent guidelines recommend that normal physiological weight loss should be limited to 10% of birth weight. 5 There is a risk of developing hypernatremia if the maximum physiological limits for weight loss are exceeded. The development of hypernatremia should be assessed in cases of higher rates of weight loss. Flaherman et al. described “early weight loss nomograms for exclusively breastfed newborns,” which aims to allow early identification of newborns on a trajectory for greater weight loss. 2 These nomograms are clinically easy to use, may facilitate clinical follow-up of newborns in the first days of life, and may reduce blood sampling for assessment of hypernatremia.
To the best of our knowledge, there are no reports evaluating the development of moderate hypernatremia in relation to the early weight loss nomograms. The present study showed that infants with weight loss >5.5% of birth weight or weight loss percentage above the 75 percentile of nomograms may develop hypernatremia. The weight loss of 5.5% within first 24 hours corresponds to 75th percentile on the nomograms for early weight loss defined by Flaherman. Early weight loss nomograms can be easily used for clinical assessment of physiological weight loss. 2 The present study showed that infants with a weight loss above the 75 percentile should be monitored for the development of hypernatremia.
The early weight loss nomograms made the clinical care of healthy newborns easy by showing hour-by-hour percentiles of weight loss. These early weight loss nomograms represent a population with a large diversity of ethnicity including Hispanic and Asian neonates. 2 An important consideration for the widespread clinical use of these nomograms was whether or not these nomograms differed for populations of different ethnic origins. Therefore, validation of early weight loss nomograms became clinically important to recommend their widespread use. In addition, there is no reference to the development of hypernatremia in relation to these nomograms. External validation of the early weight loss nomograms was performed by Schaefer et al. in a geographically distinct population, immediately after the nomograms were defined, and the weight loss percentile curves in that study were found to be generally similar to those described by Flaherman. 6 They concluded that early weight loss nomograms can be used with greater confidence in different geographical areas and in populations of different ethnicities (6). Another study reporting data from the low and middle-income countries also concluded that the trajectories of initial neonatal weight loss in Nepal, Pakistan, and Uganda were similar to United States norms. 7 Based on these studies, it was concluded that early weight loss nomograms can be used with confidence on a large scale in different geographical areas and income levels. In our study group, the mean rates of weight loss within the first day of life were also similar to those of the nomograms.
Neonatal hypernatremia is a serious condition that can occur in healthy newborns with feeding difficulties. Severe hypernatremia can cause short-term and long-term complications, mainly neurological problems such as seizures, brain edema and intracranial hemorrhage.8,9 Almost all neonates lose weight after birth, and a weight loss of more than 7–10% has been reported to be significantly associated with the development of hypernatremia.10,11 However Gonzalez et al. reported that hypernatremia can develop even in infants with a weight loss percentage below the classically established limits. 12 According to their study, a weight loss of more than 4.8% for a male newborn born by cesarean section to a multiparous mother with a higher education may be the higher level of acceptable limits. In the present study, a weight loss of 5.5% or more was found to be associated with the development of mild or moderate hypernatremia, so we recommend measuring serum Na levels in weight loss rates of 5.5% or more to avoid missing the development of hypernatremia. Breastfeeding assessment and breastfeeding counseling for mothers are also essential to maintain good neonatal health.
The relationship between early weight loss percentages and hypernatremia has been reported in many studies, but the relationship between weight loss percentiles and the development of hypernatremia has not been reported in any study. To the best of our knowledge, the present study is the first to evaluate the relationship between weight loss nomograms and the development of hypernatremia, showing that even if the weight loss is within the defined acceptable normal ranges and percentiles, hypernatremia may develop. This study found that hypernatremia can develop when the weight loss exceeds 75th percentile. The main strength of the study is that it is the first to show the association between weight loss percentiles and the development of hypernatremia. Belong with this the relatively small number of patients, the lack of subgroup analysis by gestational age or intrauterine growth pattern are the main limitations.
In conclusion, early weight loss nomograms are widely used in most countries to aid the clinical follow-up of neonates. Despite their widespread use, these nomograms should be used with great caution in clinical practice to avoid the development of hypernatremia. Serum sodium levels should be routinely measured if the weight loss exceeds 5.5% or 75th percentile on the nomograms.
Footnotes
Authors’ Contributions
B.Y. and A.C. conceptualized and designed the study. B.Y., M.B., A.B.K., and G.K. collected the data. B.Y., M.B., L.B., Z.I., and A.C. analyzed and interpreted data and performed the literature search. B.Y., Z.I., and A.C. drafted the article and wrote the article. All authors contributed to the article and approved the submitted version.
Disclosure Statement
The authors have no conflicts of interest.
Funding Information
There is no funding source for the study and the article.