
Abstract
Objective:
Addressing the need to further characterize socioeconomic status (SES) to understand its influence on breastfeeding, we sought to identify patterns of breastfeeding at discharge by both race and educational attainment, as well as whether social support, stress, and employment status mediated these patterns.
Methods:
This secondary analysis of the Measurement of Maternal Stress Study included 636 pregnant individuals who were surveyed on perceived stress, social support, and hours worked outside the home in their second and third trimesters. Race was categorized as white or People of Color (POC) (Black or Latine), and educational attainment was categorized as low-SES (less than high school), mod-SES (high school and some college), or high-SES (college degree or more). Infant feeding at discharge was abstracted from medical records. Logistic regressions tested associations between race, SES, and race/SES with any breastmilk feedings.
Results:
In adjusted models we observed that low-SES POC had the lowest odds (adjusted odds ratio (OR): 0.10, 95% Confidence Interval (CI): 0.04, 0.23) of breast milk feeding at discharge when compared with high-SES white participants, and higher SES was associated with greater odds of breast milk feeding in all racial/ethnic groups. In adjusted models, working more hours and increased social support were not associated with greater odds of breast milk feeding. Perceived stress was not associated with breast milk feeding in unadjusted or adjusted models.
Conclusions:
Breastfeeding initiation rates were driven by both educational attainment and race/ethnicity. Social support, stress, and employment status did not explain differences in breastfeeding outcomes. Our results highlight the importance of considering the combined effect of race/ethnicity and SES in strategies to achieve breastfeeding equity.
Introduction
Breastfeeding provides multiple health benefits for parents and infants. The benefits of breastfeeding for the infant include immune development, gut microbiome colonization, and decreased likelihood of sudden/unexpected infant death. 1 Breastfeeding parents have a decreased risk of developing ovarian cancer, breast cancer, and cardiovascular disease. 1 Because of these benefits, the World Health Organization recommends breastfeeding should be initiated within the first hour of birth and remain exclusive for the first six months of life. 2 However, there are persistent racial/ethnic and socioeconomic inequities in breastfeeding outcomes, with breastfeeding initiation rates among Black (74.5%), American Indian or Alaskan Native (77.7%), and other Pacific Islanders (79.4%) falling below the United States national average (84.0%). 3 In addition, low-income families enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) report lower rates of “still breastfeeding at 6 months” compared with those ineligible for WIC benefits. 4 To effectively reduce these inequities and improve breastfeeding outcomes for birthing parents and infants, it is imperative that we implement interventions that prioritize populations with breastfeeding inequities due to systemic racism and/or discrimination.
Previous research examined the relationship between breastfeeding inequities by race/ethnicity and socioeconomic status (SES) as separate indicators.5,6 Scholar Kimberlé Crenshaw coined the term intersectionality to refer to the oppressive experiences resulting from an individual’s combined identities. Discrimination can be multifaceted based on an individual’s gender, race, social class, and/or sexuality. 7 Therefore, it is necessary to acquire an intersectional approach to racial health disparities and better characterize patterns of inequity, as we showed in a prior analysis of a nationally representative cohort. 8 Race/ethnicity and SES intersect to compound inequity, with People of Color (POC) being more likely to also experience socioeconomic disadvantage. 8 Inequities in breastfeeding outcomes by both race/ethnicity and SES suggest that factors related to the experiences of racism and resource deprivation (e.g., stress, social support, occupation, and employment status) may be directly or indirectly on the pathway to lower rates of breastfeeding initiation, exclusivity, and duration. 9 For example, individuals with higher educational attainment are more likely to work professional office jobs that may offer more paid leave time, schedule flexibility, or time to express breast milk during work, improving one’s chances of meeting their breastfeeding goals, compared with those in hourly positions who have little or no paid leave or protected pumping time.10–13 Racial disparities based on employment type are prevalent. White women are more likely to hold managerial/professional positions compared with Black women, and Black women are more likely to work in service and transportation occupations. 14 Black women and other POC may be at an increased risk of suboptimal breastfeeding outcomes based on job discrimination and racial discrimination. Research aiming to address breastfeeding outcomes based on professional occupation often overlooks the discrimination experienced by Women of Color in the professional workforce. In addition, sociology provides substantial context for the differences experienced between white and Women of Color in raising their infants. In her book Mothering While Black, Dawn Doe proposes her Market Family Matrix Theory, which argues that familial and work responsibilities offer a potentially beneficial relationship for Women of Color. 15 The theory proposes that being employed versus non-employed increases access to maternal resources such as supportive leave, increased income, and breastfeeding policies in the work place. 15
This paper hypothesizes stress as a mediator for breastfeeding outcomes and race/ethnicity and educational attainment. Isiguzo and colleagues found that higher prenatal anxiety, also measured with the Cohen Perceived Stress Scale (PSS), was associated with decreased odds (OR 0.88, 95% CI: 0.83–0.92) of exclusive breastfeeding. 16 Research supports that navigation of lower SES and experiences of racism and discrimination are linked to elevated psychosocial stress, which is associated with reduced breastfeeding intensity and duration, potentially resulting from behavioral (i.e., formula may be logistically easier) and physiological (i.e., inflammation can inhibit lactogenesis) pathways.17–19
Increased social support may serve as a buffer against challenges experienced by individuals with lower SES and/or identifying as racially and ethnically underrepresented populations, providing practical support with infant care and relieving stress to improve breastfeeding outcomes. A longitudinal study of 251 participants in Southwestern Pennsylvania found participants who were provided with help or support from a person, group, or organization to continue breastfeeding were more likely to exclusively breastfeeding their infant (OR 2.30, 95% CI: 1.52–3.49) compared with those who did not. 16 Focus groups of African American women identified barriers to breastfeeding specific to their lived experiences, such as lack of access to practical and emotional breastfeeding support delivered by their health care providers, 20 and a general distrust in the provided information. 21 Previous literature identified that providers’ unconscious bias toward African American mothers’ fitness to breastfeed their infants harmfully translates into the perception of differential treatment, as well as a lack of culturally relevant education that inadequately addresses the support needs of African American mothers in their breastfeeding journeys.22,23 Finally, evidence indicates that POC are less likely to receive provider support with breastfeeding resulting from systemic racism in health care. 20 Thus, differential support for lactation inside and outside of the health care setting may drive racial and socioeconomic breastfeeding disparities. We aimed to identify patterns in breastfeeding outcomes at the intersection of race/ethnicity and SES and to examine how social support, employment status, and perceived prenatal stress might mediate breastfeeding disparities.
Methods
The Measurement of Maternal Stress study was an observational cohort study designed to examine maternal stress, biomarkers, and birth outcomes at four sites across the country: Northwestern University in Chicago, Illinois; University of Texas Health Science Center in San Antonio, Texas; University of Pittsburgh, Pennsylvania; and Children’s Hospital of Philadelphia in Schuylkill County, Pennsylvania. In total, 744 English-speaking participants with singleton pregnancies were recruited prior to 21 weeks of gestation. Individuals were ineligible if they were under the age of 18, had major fetal congenital anomalies or chromosomal anomalies, were receiving progesterone treatment, or were undergoing chronic corticosteroid treatment. Participants completed extensive surveys and interviews during the second and third trimesters of pregnancy. After delivery, participant medical records were abstracted for birth outcomes by trained research staff. The study received approval from Institutional Review Boards at all four sites, and all participants were appropriately consented to the study.
SES was ascertained by educational attainment, which was available for 99.6% of respondents and correlated highly (correlation coefficient = 0.68) with self-reported income. 8 SES was reported as the highest degree completed and categorized as low-SES (high school education or less), mod-SES (some college/associate’s degree), or high-SES (bachelor’s degree or more). We used educational attainment as a proxy for SES and found a high correlation between education and income in this sample and therefore felt comfortable using education as a proxy for SES [Supplementary Tables S1 and Table S2]. Self-reported income was not consistently reported (10.2% missing data) in the study sample.
Race/ethnicity was self-reported from a list of 14 racial and 5 ethnic identities. For this analysis we included participants who identified as white, Black, or Hispanic/Latine. Race/ethnicity was dichotomized to non-Hispanic/Latine white (white) or Person of Color (POC).
Race/SES was created to examine the intersection of SES and race/ethnicity. We crossed the three SES groups with the two race/ethnicity groups (low-SES POC, low-SES white, mod-SES POC, mod-SES white, high-SES POC, high-SES white) to create a six-category variable.
Hours worked outside the home was used to approximate employment status. Participants reported the number of hours they typically worked each week, which was used as a continuous variable in regression models.
Breast milk feeding at discharge was abstracted from medical records by trained research staff and defined as any breast milk feedings within the last 24 hours of the delivery admission.
Social support was measured using the Social Support Questionnaire (SSQ). The SSQ was administered by an interviewer, and participants were asked to rate the different types of support they received throughout their lives. 24 Nineteen items were used to assess various forms of support present during the participant’s pregnancy. Possible participant scores ranged from the lowest, 0, to the highest, 100, which corresponds with possessing greater varieties of support.
Perceived prenatal stress was measured by the 10-item Cohen’s PSS administered by the interviewer at two timepoint(s) prenatally, between 12–30 and 32–35 weeks gestational age. The survey includes 10 questions asking participants to numerically rate on a scale how often they experienced feelings or thoughts regarding difficulties that may have occurred during the past month. 25 Participant scores may range from 0 to 40.
Covariates included factors known to be associated with race/ethnicity, SES, and breastfeeding outcomes. These included the study sites, participant age, parity, smoking, prepregnancy body-mass-index, hypertensive disorders of pregnancy, diabetes, mode of delivery, and infant neonatal intensive care unit admission.
Statistical analysis
Logistic regressions were used to model the relationships between race/ethnicity, SES, and race/SES; perceived stress; hours worked; and social support with any breast milk feeding at discharge. Models were adjusted for all covariates. Analyses were conducted using IBM SPSS statistics for MAC, Version 26 (Armonk, NY, USA: IBM Corp). In the event of significant associations between potential mediators and breastfeeding at discharge, mediation analyses were planned using the PROVESS macro model 4.
Results
This analysis included 636 participants, 62% of whom identified as non-Hispanic/Latine white, and 37% who identified as a POC (Table 1). 26.4% were low-SES, 35.5% were mod-SES, and the remaining 38.0% were high-SES. The majority of participants provided breast milk to their infants at discharge (76.5%).
Characteristics of the MOMS Study Sample
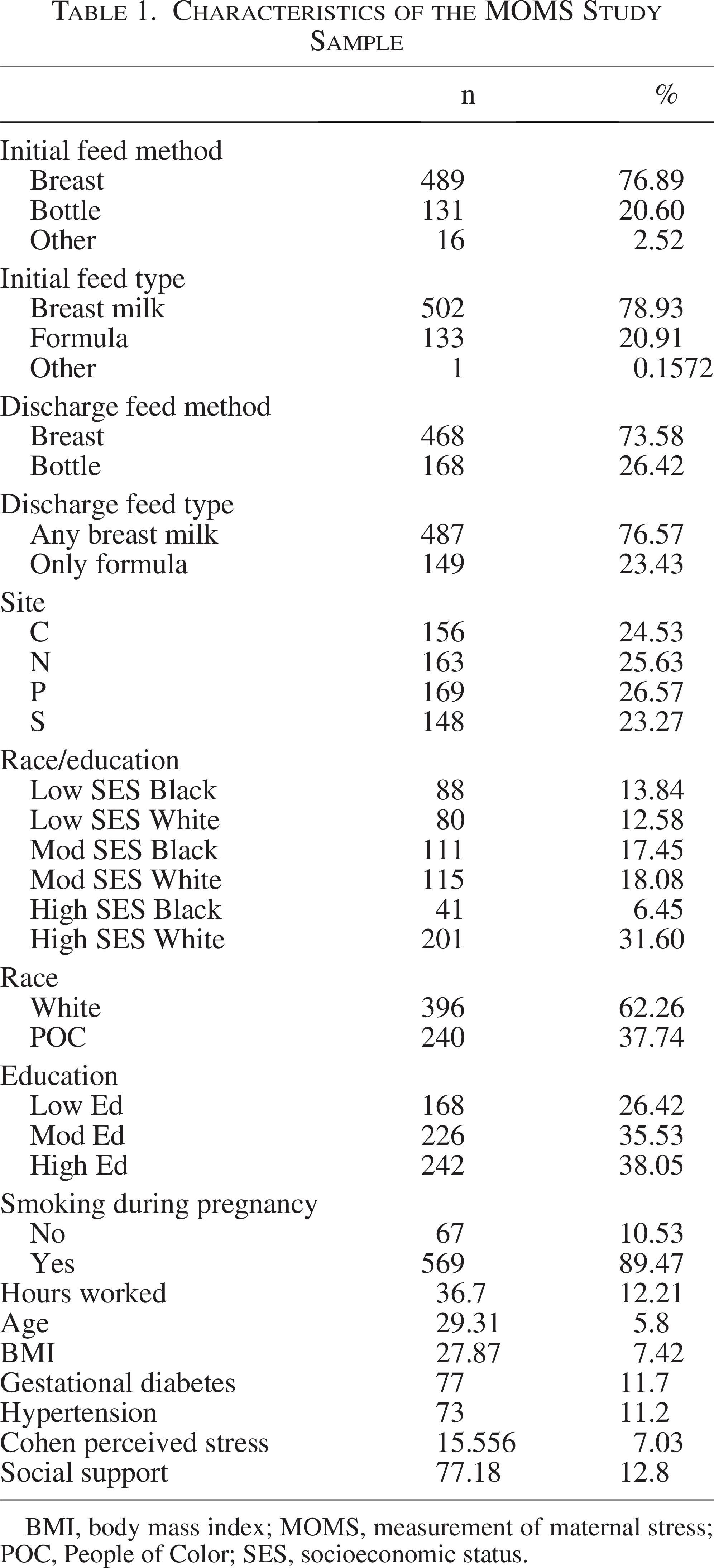
BMI, body mass index; MOMS, measurement of maternal stress; POC, People of Color; SES, socioeconomic status.
Race/SES and any breast milk feedings at discharge
The interaction model for race/ethnicity and educational attainment was conducted, revealing educational attainment was primarily driving breastfeeding rates at discharge. High-SES white participants had the highest rate of breastfeeding at discharge (92%), and low-SES white had the lowest rate at 54% (Table 2). There was a strong pattern by SES, with 58% breastfeeding among low-SES POC, 73% among mod-SES white, 79% among mod-SES POC, and 91% among high-SES POC (Table 2). The stepwise pattern was reflected in adjusted regressions, with low-SES POC participants having the lowest odds of breast milk feeding at discharge compared with high-SES white participants (adjusted odds ratio (aOR): 0.10, 95% CI: 0.04, 0.23) (Tables 3 and 4).
Distribution of Feeding Type at Discharge by Race/Education, Race and Education
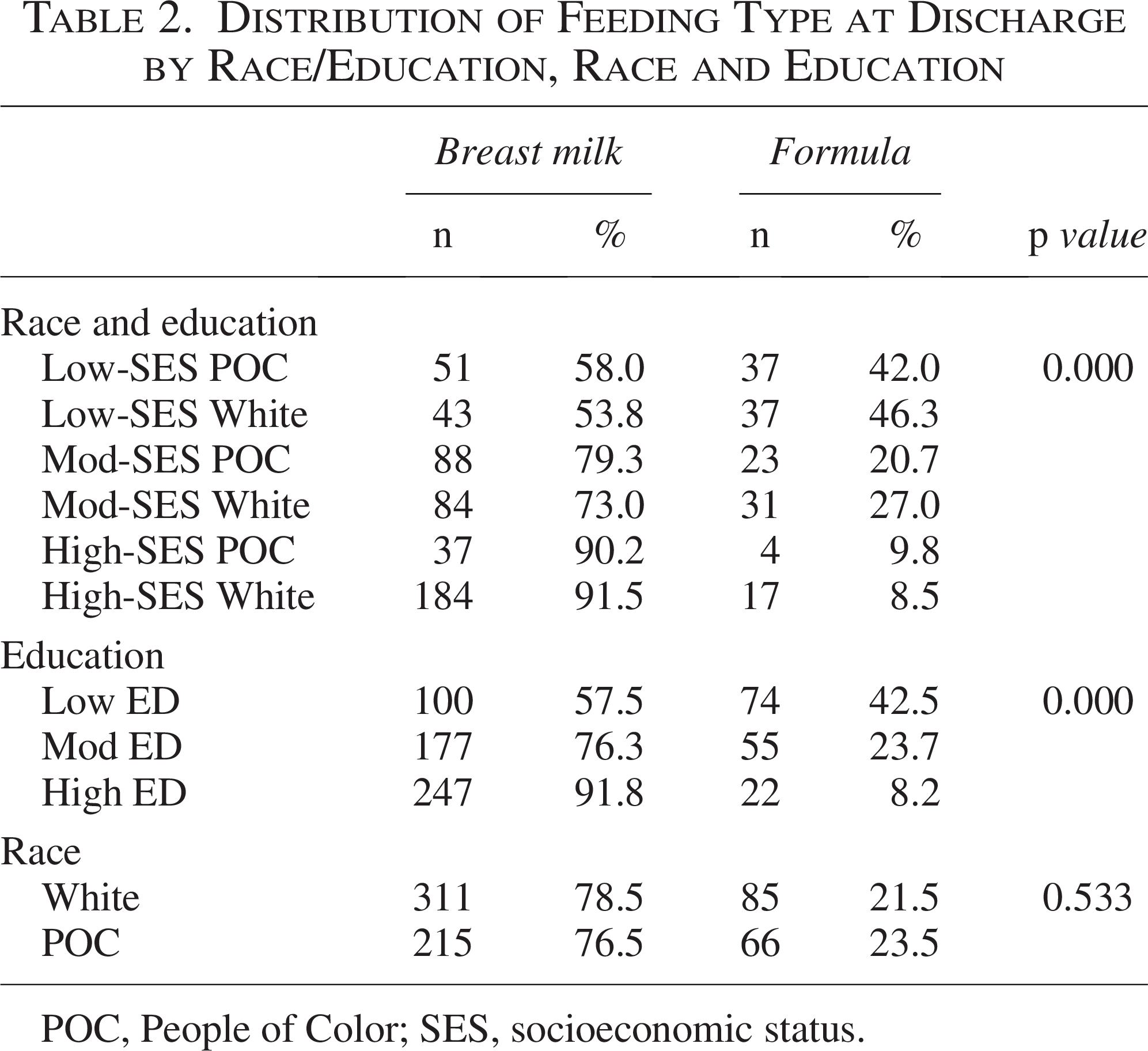
POC, People of Color; SES, socioeconomic status.
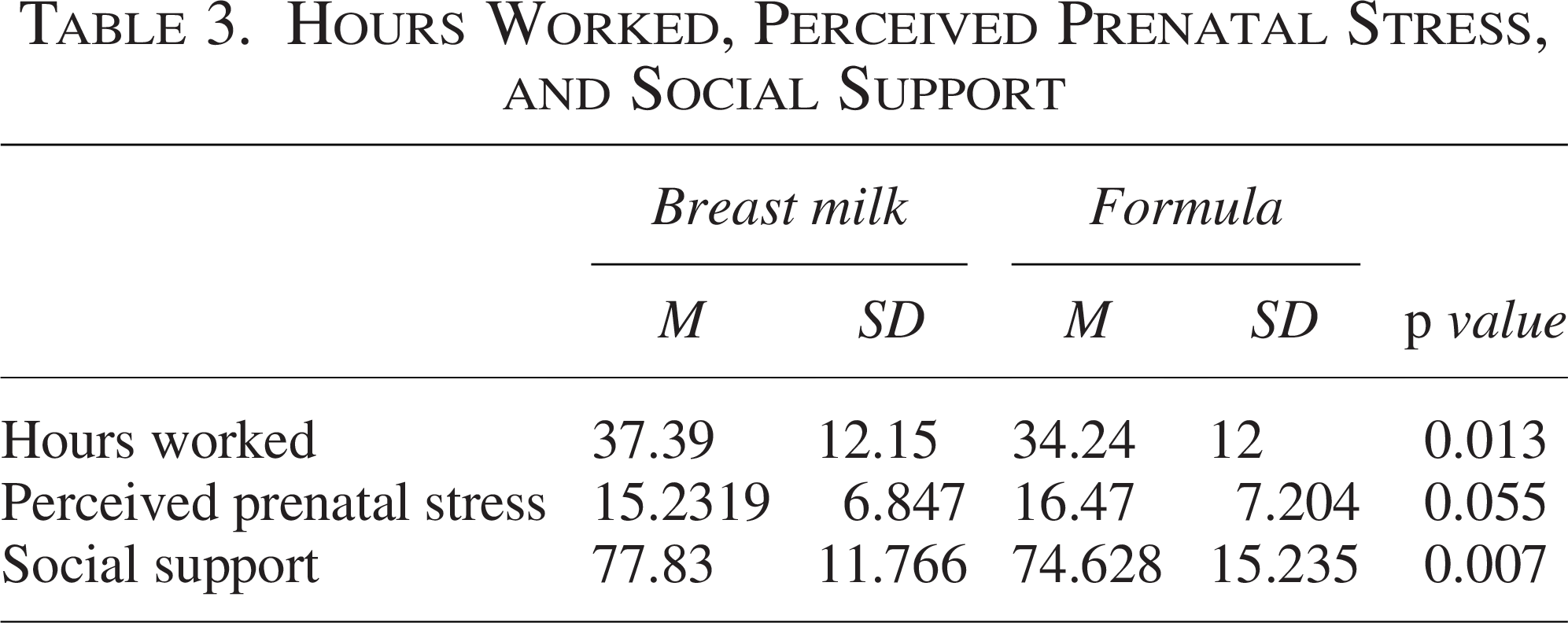
Hours Worked, Perceived Prenatal Stress, and Social Support
Adjusted Odds of Breast Milk Feeding in the 24 Hours Prior to Hospital Discharge by Race/Education, Hours Worked, Perceived Stress, and Social Support
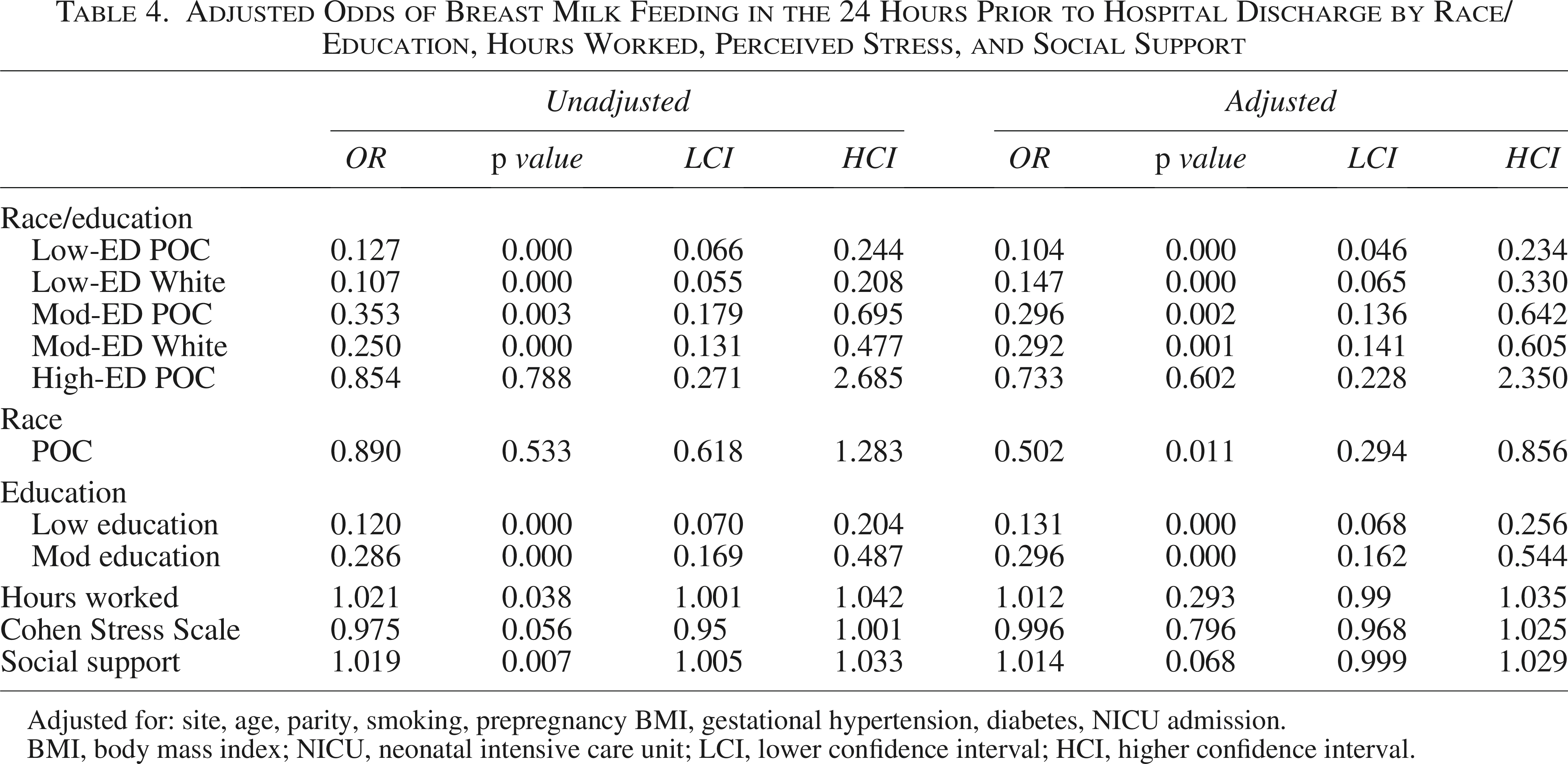
Adjusted for: site, age, parity, smoking, prepregnancy BMI, gestational hypertension, diabetes, NICU admission.
BMI, body mass index; NICU, neonatal intensive care unit; LCI, lower confidence interval; HCI, higher confidence interval.
Employment
Approximately 66% of the sample worked full-time during their enrollment in the study, and the average hours worked outside the home per week were 36.83 ± 12.12 (Table 1). Full-time work is patterned significantly by SES and race, with full-time work occurring among 85% of high-SES white, 73% of high-SES POC, 71% of mod-SES white, 59% of mod-SES POC, 47% of low-SES white, and 42% of low-SES POC. Low-SES white participants worked the fewest number of hours (32.83; SD: 11.11), while high-SES white participants worked the greatest number of hours (40.50; SD: 12.00). In unadjusted models, participants who worked more hours were more likely to feed their infants any breast milk at discharge (OR: 1.021, 95% CI: 1.001, 1.042); however, this relationship was attenuated in adjusted models (Tables 3 and 4), thus no mediation testing was performed.
Social support
Participants had an average social support score of 76.9 (SD: 12.99), with high-SES white participants having the highest scores (mean: 80.02, SD: 9.5) and low-SES POC having the lowest (mean: 72.60, SD: 14.25). Increased social support was significantly associated with breast milk feeding at discharge in the unadjusted model (OR: 1.019, 95% CI: 1.005, 1.033), but the result was attenuated when adjusted (aOR: 1.014, 95% CI: 0.999, 1.029) (Tables 3 and 4); thus, no mediation testing was performed.
Perceived prenatal stress
The average PSS score for participants was 15.77 (SD: 7.07). The highest level of perceived prenatal stress occurred among low-SES POC participants (mean: 19.03, SD: 6.86) and the lowest levels among high-SES white participants (mean: 13.55, SD: 6.01). Neither unadjusted nor adjusted models indicated a relationship between perceived stress and breast milk feedings (Tables 3 and 4); thus, no mediation testing was performed.
Discussion
We found breastfeeding outcomes among racial/ethnic groups were driven by educational attainment, echoing prior findings from an earlier analysis of National Immunization Study data where we found that both longer breastfeeding durations and breastfeeding exclusively were most strongly influenced by educational attainment and patterned by race/ethnicity. 8 Here, we found disparities in breastfeeding at discharge patterned in a stepwise fashion, driven by educational attainment, with the highest odds of breast milk feeding at discharge among high-SES white participants and the lowest odds among low-SES POC participants. While our prior analysis and other research consistently show Black individuals have the lowest rates of breastfeeding initiation in the United States,26–29 we saw that POC individuals in both the low (53% versus 58%) and mod (73% versus 79%) SES groups had slightly higher rates of breastfeeding at delivery compared with white individuals in similar SES strata, and rates were near comparable among those with high-SES (91% white versus 90% POC). In this analysis, Black and Hispanic/Latine individuals were both categorized as POC, though Hispanic/Latine dyads tend to have the highest rates of breast milk initiation across the United States30,31, so our findings likely reflect both national and regional trends.
We anticipated that hours worked, social support, and perceived stress might explain the relationships between SES and race/ethnicity and breastfeeding at discharge; however, none of these factors were independently associated in adjusted models. It is noteworthy that the majority of breastfeeding literature focuses on breastfeeding duration and not initiation. The possible mediators in this paper may have greater influence on one’s ability to maintain breastfeeding, as opposed to breastfeeding initiation within the hospital. Prior studies have contributed mixed findings regarding the relationship between breastfeeding prior to hospital discharge and our potential mediators.
Published literature reports mixed findings on the effect of employment hours worked and breastfeeding initiation, with the majority focusing on breastfeeding duration. An analysis of 817 individuals in Minnesota who were majority (86%) white and mostly (46%) working in a professional field similarly did not find that hours worked during pregnancy predicted breastfeeding initiation. 12 In another study of 1,498 birthing people, with 42% employed full-time, 41% unemployed and 68.4% white, employment status did not predict breastfeeding intention. However, the authors did find that compared with no employment, full-time employment decreased the odds of exclusive breastfeeding at 1-week postpartum [OR = 0.48]. 32 These findings support that the number of hours worked may be driving one’s ability to maintain breastfeeding versus one’s ability to initiate breastfeeding following delivery. In contrast, another study of 185 African American women found full- and part-time employment during pregnancy was associated with higher odds of breastfeeding at 1-week postpartum compared with nonemployment during pregnancy [OR = 2.25]. 33 A nationally representative study at the University of Michigan studied postpartum occupation and breastfeeding duration among 970 mothers. 13 The majority (70%) of participants identified as white, 13% as Black, and 17% as other race. Black and other race mothers working a managerial/professional occupation breastfed for a longer duration (4.68 months) compared with service/labor (3.11 months) and non-employed (2.97 months). The relationship was reversed for white mothers, as those who were non-employed breastfed for the longest duration (5.94 months). 13 These results are consistent with the previously mentioned Family Matrix Theory by Dawn Doe. 15 These conflicting results also suggest that simple approximations of employment status, like hours worked, may be insufficient for understanding how employment contributes to racial and SES disparities in breastfeeding in the United States. To develop an accurate picture of maternal employments effect on breastfeeding behaviors, other racially divided differences (job safety, paid leave) should be considered.
Our finding that social support did not predict breastfeeding outcomes is inconsistent with prior findings. Quintero and colleagues measured several forms of social support received by participants while pregnant, including breastfeeding-specific support received from a doctor, support groups, and/or friends and family. They concluded that support from any of these groups was associated with significantly increased breastfeeding rates across all racial/ethnic groups. 34 Notably, the association between social support and breastfeeding was weaker for Alaska Native, Hispanic, and Black participants in their sample, potentially indicating different racial/ethnic groups may benefit differentially from similar types of breastfeeding support. 34 This suggests the need for culturally salient, tailored support models. To that end, Carlin and colleagues asked 402 participants, the majority of whom were Black, college educated, with 42% WIC participation, about their social support network and breastfeeding behaviors, categorizing family-centered social support networks as “exclusive” and nonfamily-centered social support networks as “expansive.” Their findings suggested that white mothers with expansive social networks were more likely to exclusively breastfeed their infants, while Black mothers with exclusive social networks were more likely to exclusively breastfeed and/or mixed-feed their infants. 35 Taken together, this research suggests that social support and lactation support play different roles across racial/ethnic groups. In addition, our measure of social support may not be inclusive of various support networks, as participants were asked about social support in the context of partner support. Future investigation into support models designed to reduce breastfeeding disparities must consider the differential social and cultural traditions and perceptions around breastfeeding possessed by each racial/ethnic group.
Finally, while we saw differences in perceived stress between racial/ethnic and SES groups consistent with other studies, we did not observe independent effects of perceived stress on breastfeeding, and thus our findings contribute to the heterogeneity of the stress and health outcomes literature. It is possible that anxiety, rather than generalized stress, is more strongly predictive of breastfeeding behavior; it may also be the case that stress measures more accurately predict breastfeeding duration, rather than initiation, which we were not able to assess with our study design. Findings from Dozier and colleagues further suggest particular types of prenatal stress matter more than others for breastfeeding outcomes. 19 Using the Moods and Feelings during Pregnancy Life Events Self-Evaluation, they found partner-related stress, traumatic stress, and financial stress, but not emotional stress, were associated with early cessation of breastfeeding before 4 weeks postpartum. 19 Studies of stress as a mediator of breastfeeding disparities remain rare but necessary. Dhaurali and colleagues evaluated a nationally representative sample of 95,820 birthing parents, finding lower odds of breastfeeding among Black individuals experiencing more stress. 31 Taken together, these findings highlight the ongoing challenge in the stress and disparities literature to develop generalizable measures of psychological burden that may underlie health disparities.
That none of our expected predictors were independently associated with, and thus able to mediate, the relationships between race/SES and breastfeeding underlines the complexity of breastfeeding behavior and the extent to which we still lack understanding of critical pathways and interventions to address breastfeeding inequities. Our results suggest socioeconomic interventions that impact education and/or occupational factors may have the greatest impact upon early breastfeeding outcomes, but such interventions may not be sufficient if they do not also address the complex social and cultural needs of diverse pregnant and parenting populations. It is imperative that future efforts to address breastfeeding disparities acknowledge the impact of intersectionality on health outcomes and provide support.
Strengths and limitations
Strengths of our study include a diverse cohort that included 4 geographically distinct sites in the United States. The study also had well-characterized measures of perceived stress and participant demographics, allowing the examination of multiple potential mediators of breastfeeding disparities. Furthermore, we used an intersectional approach to examine racial/ethnic and socioeconomic disparities simultaneously, which was more informative of breastfeeding patterns than conventional approaches of statistical adjustment. Limitations include our use of a binary race variable, which allowed our analyses to have better power but prevented granular understanding of differences in breastfeeding experiences shaped by racial/ethnic identity, which has been well-documented, with Hispanic/Latine individuals having better early breastfeeding outcomes than Black individuals.30,31 We chose not to include income as a component of SES in this analysis, as income was not reported in 10.2% of the sample. Moreover, cost-of-living differences across geographic regions make income less comparable across distinct regions. Education level is easily comparable across geographic regions regardless of cost-of-living differences and therefore was a more appropriate SES measure in this study. Finally, we were unable to account for occupation type, which is an important avenue for future research.
Conclusions
Our findings indicate that breastfeeding initiation rates in this sample were driven by both educational attainment and race/ethnicity, and that social support, stress, and employment status did not explain differences in breastfeeding outcomes prior to delivery discharge. Our results highlight the importance of considering the combined effect of race/ethnicity and educational attainment to address breastfeeding disparities and the need for more research investigating strategies to achieve breastfeeding equity.
Authors’ Contributions
B.P.S.: Conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing. M.S.B.: Conceptualization; methodology, formal analysis, and writing—review and editing. J.F.: Writing—original draft and writing—review and editing. W.G.: Writing—review and editing. H.S.: Writing—review and editing. P.W.: Writing—review and editing. A.E.B.B.: Funding acquisition and writing—review and editing. L.S.K.-D.: Conceptualization, supervision, and writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding support for this research provided by the following sources: Funding for this study was provided by: HHSN275201200007I-HHSN27500005. Patient Centered Outcomes Research Institute contract #AD-2020C3-21231 (Borders).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.