
Abstract
Background:
Painful procedures are frequently performed in neonatal care, yet their repeated exposure is associated with adverse short- and long-term neurodevelopmental outcomes. Nonpharmacological, physiological, and parent-involved interventions such as breastfeeding and breast milk sensory stimuli have emerged as promising strategies for procedural pain management.
Objective:
This umbrella review and meta-analytic reanalysis aimed to synthesize the evidence from systematic reviews and meta-analyses evaluating the analgesic effects of breastfeeding, breast milk odor, and breast milk taste during painful procedures in term and preterm infants.
Methods:
A comprehensive umbrella review approach was applied, and the methodological quality of all included reviews was assessed using the Assessment of Multiple Systematic Reviews-2 tool. Effect sizes from existing meta-analyses were reanalyzed using random-effects models, incorporating heterogeneity, prediction intervals, and clinical variation across interventions and populations.
Results:
Breastfeeding demonstrated the strongest analgesic effect, with large reductions in pain scores, crying duration, and heart rate during procedural pain. Breast milk odor and taste also reduced behavioral and physiological pain indicators, particularly among preterm infants, though with smaller effect sizes compared with direct breastfeeding. Despite generally consistent effect directions, substantial heterogeneity was observed across meta-analyses due to variation in populations, procedures, intervention timing, and outcome measures. High-quality Cochrane reviews contributed the strongest evidence base, while non-Cochrane reviews showed moderate-to-low methodological confidence due to limitations such as lack of protocol registration or incomplete reporting.
Conclusions:
Breastfeeding and breast milk–related sensory interventions are effective, feasible, and safe nonpharmacological strategies for managing procedural pain in neonates. These findings support the integration of breastfeeding or maternal milk sensory exposure as first-line approaches in neonatal pain management protocols. Further research is needed to clarify optimal timing, dosing, and combinations with other nonpharmacological interventions.
Introduction
Infants admitted to the neonatal intensive care unit (NICU) are exposed to numerous painful procedures and the stress these procedures generate throughout their hospital stay. In particular, premature newborns have been reported to undergo more than 100 painful interventions during hospitalization. Procedure-related pain has been associated with hormonal imbalances, alterations in growth hormone and glucocorticoid levels, disruptions in metabolic and immune system functions, and various behavioral problems. As a result of these painful experiences, infants may develop a range of physiological and behavioral difficulties later in life. In this context, the accurate assessment and effective management of pain in newborns are of critical importance.1–4
Nonpharmacological methods are frequently preferred in neonatal pain management due to their low cost, ease of application, and absence of adverse effects. However, the effectiveness of these interventions may be influenced by various factors, including the infant’s age, coping abilities, and cultural background. Therefore, identifying the most effective approach is not always straightforward. In recent years, breastfeeding, as well as the smell and taste of breast milk, have emerged as simple, feasible, and potentially effective nonpharmacological strategies.5–10
The taste and smell of breast milk represent not only a source of nutrition for infants but also an important sensory experience that provides comfort, security, and analgesia. Studies have shown that infants exposed to stimuli containing their mother’s scent exhibit calmer behaviors and demonstrate fewer signs of stress during painful procedures. These findings suggest that the taste and smell of breast milk may serve as effective supportive interventions in neonatal pain management.8,11–14
There is a substantial body of meta-analytic research in the literature evaluating the effects of breastfeeding and the taste and smell of breast milk on pain in newborns. However, no study has comprehensively examined the collective strength of this evidence or assessed the overall level of certainty across these meta-analyses. The present study aims to integrate the findings of existing meta-analyses in this field and thereby provide a high-level synthesis of the available evidence. In addition, through reanalysis of the existing meta-analytic datasets, this review seeks to quantitatively reassess the effects of breast milk-related sensory stimuli (taste, smell, and breastfeeding) on pain scores during various clinical procedures (e.g., heel lance, injection, venipuncture).
Methods
Literature search and data extraction
This umbrella review was designed to include all existing meta-analyses examining the effects of breast milk taste, breast milk odor, and breastfeeding on pain reduction in newborns. A systematic search of the PubMed, Cochrane Database of Systematic Reviews, and Web of Science databases was conducted for meta-analyses published between 2010 and 2025, using the following keywords: “breastfeeding,” “breast milk,” “taste,” “smell,” “odor,” “infant,” “newborn,” “pain,” “pain management,” “meta-analysis,” and “systematic review.”
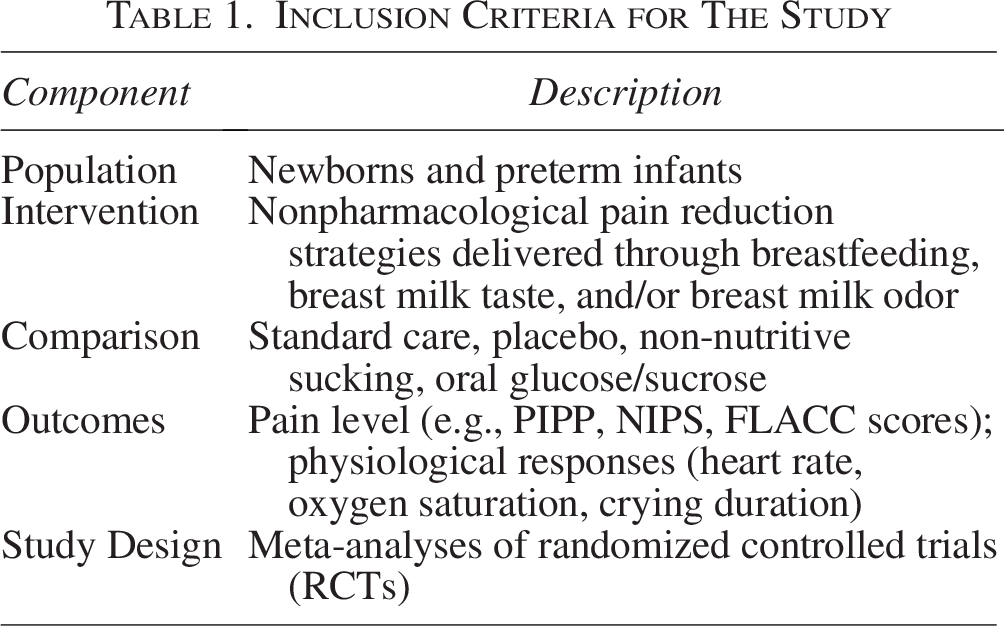
In addition, the reference lists of all included meta-analyses were manually screened to identify any additional relevant studies. The search was restricted to articles published in English. Meta-analyses that met the eligibility criteria were reviewed to synthesize and reanalyze the available evidence regarding the effects of breast milk taste, smell, and breastfeeding on pain scores during invasive procedures (e.g., heel lance, injection, venipuncture) in newborns (Table 1).
Inclusion Criteria for The Study
All study selection and data extraction processes were conducted independently by two reviewers, and any disagreements were resolved through consultation with a third reviewer. The reliability and methodological quality of the included studies were assessed using the Assessment of Multiple Systematic Reviews-2 (AMSTAR-2) criteria; the included meta-analyses were compared qualitatively, and the overall level of evidence was reinterpreted accordingly. This review was conducted in accordance with the PRISMA and Joanna Briggs Institute guidelines recommended for umbrella reviews, and all methodological steps were reported transparently.15,16
For each included meta-analysis, data on sample size, effect sizes, 95% confidence intervals (CI), and the quality or risk-of-bias assessments of the primary studies (Jadad or Cochrane ROB2) were recorded. Heterogeneity was evaluated using the I2 statistic, and caution was exercised when interpreting findings from meta-analyses with substantial heterogeneity. Furthermore, prediction intervals and publication bias (Egger’s test) were intended to be reported; however, these values were available in only one study, and no publication bias assessments were provided in the remaining meta-analyses.
Inclusion and exclusion criteria
Inclusion criteria
Studies examining the effects of breastfeeding, breast milk taste, or breast milk odor on pain management in newborn and preterm infants. Full-text, peer-reviewed publications. Meta-analyses that include data exclusively from randomized controlled trials (RCTs). Studies published in English.
Exclusion criteria
Studies not conducted in a NICU setting. Studies in which the invasive procedure was performed on infants with specific medical conditions (e.g., burns, surgery, cancer). Studies that do not report pooled or summary meta-analytic results. Meta-analyses evaluating breastfeeding, breast milk odor, or taste in combination with additional nonpharmacological interventions.
Types of interventions and outcomes considered
The interventions included nonpharmacological pain management methods involving the taste and/or smell of breast milk and breastfeeding. All types of painful procedures (such as heel lance, venipuncture, intravenous intervention, cannulation, and lumbar puncture) were accepted as outcome-relevant events. The primary outcomes consisted of neonatal pain levels and physiological/behavioral responses (heart rate, oxygen saturation, crying duration).
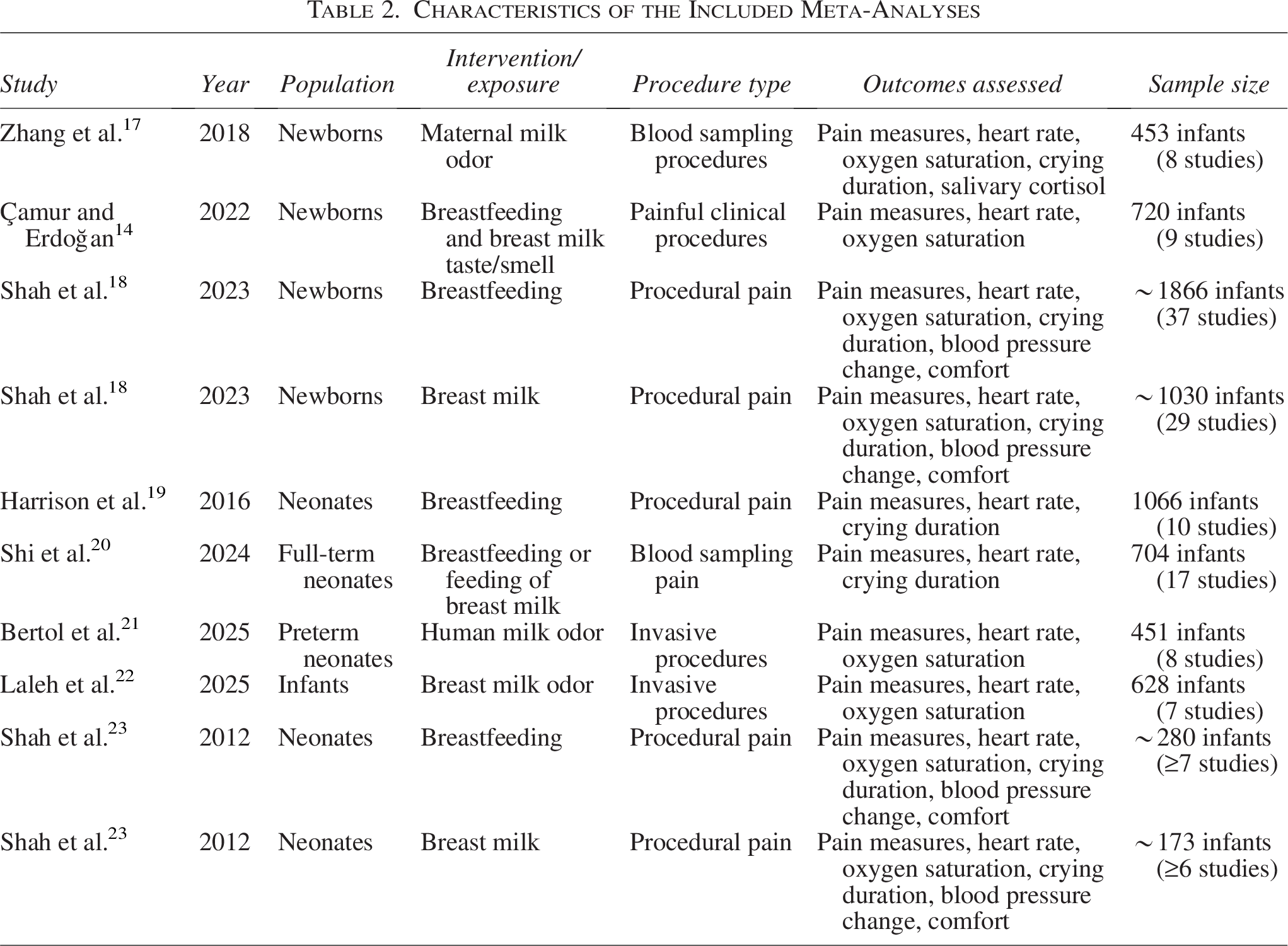
All interventions and evaluated outcome measures are presented in detail in Table 2, and the effect sizes (standardized mean differences [SMD]) obtained from each meta-analysis were standardized to allow for direct comparison across studies.
Characteristics of the Included Meta-Analyses
Assessment of summary effects and heterogeneity
In this study, the summary effect sizes reported in each included meta-analysis were examined descriptively. To evaluate differences across meta-analyses, sample characteristics, types of interventions, and outcome measures were compared. The I2 statistic was used to determine the extent to which between-study variation was attributable to true heterogeneity rather than chance. In accordance with commonly accepted standards, I2 values were interpreted as low (∼25%), moderate (∼50%), and high (≥75%) heterogeneity.
Since prediction intervals were not reported in the majority of the included meta-analyses, it was not possible to generate an estimated range representing the potential effect sizes that the same intervention might yield in future studies. Therefore, the current findings were evaluated solely based on the reported effect sizes and heterogeneity statistics.
Evaluation of small-study effects and excess statistical significance
The included meta-analyses were examined to determine whether smaller-sample studies tended to report larger effect sizes and whether commonly used tests for excess statistical significance had been applied. Within this umbrella review, findings related to Egger’s test and excess statistical significance tests were reported only to a limited extent in the majority of the meta-analyses. Consequently, it was not possible to directly and quantitatively assess the presence of small-study effects or excess statistical significance.
Evaluations of publication bias and small-study effects were therefore based solely on the qualitative assessment of methodological quality according to the AMSTAR criteria, and thus could be interpreted only to a limited degree (Table 3).24,25
Methodological Quality Assessment of the Included Meta-Analyses According to the AMSTAR-2 Criteria

Quality of the included studies
The methodological quality of the included meta-analyses was assessed using the AMSTAR tool. Each meta-analysis was evaluated based on the number of AMSTAR criteria it fulfilled. In addition, available information regarding the quality assessments of the primary studies and their potential risk of bias was also recorded (Table 3).24,25
Assessment of the level of evidence
In some of the included meta-analyses, the level of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach. However, within the scope of this umbrella review, no additional GRADE rating was performed; instead, the strength of the evidence was interpreted based on the overall methodological quality of the meta-analyses. Accordingly, the methodological rigor of all included meta-analyses was re-evaluated using the AMSTAR (A Measurement Tool to Assess Systematic Reviews) criteria.
Statistical analysis
For each included meta-analysis, random-effects summary effect sizes calculated using the DerSimonian and Laird (DL) method, along with their corresponding 95% confidence intervals (CI), heterogeneity levels (I2), and p values, were recorded (DerSimonian and Laird, 1986). Since all meta-analyses included five or more primary studies, the Hartung–Knapp–Sidik–Jonkman (HKSJ) adjustment—typically recommended for small-sample meta-analyses (i.e., those including fewer than five studies)—was not required. 26 When available, 95% prediction intervals (PI) were intended to be extracted to indicate the expected range of effects in future studies; however, these data were not reported in the included articles.26,27 Heterogeneity was assessed using the I2 statistic, and I2 values of <25%, 25–50%, and >50% were interpreted as low, moderate, and high heterogeneity, respectively. 28
Although the application of Egger’s regression asymmetry test was planned to assess publication bias, this analysis could not be performed because the necessary data were available in only one article, and individual study-level data were not accessible within the scope of this umbrella review. Furthermore, it is well known that publication bias analyses are not recommended in meta-analyses including fewer than 10 studies, as is the case for many of the included reviews. However, because a low number of studies increases the risk of bias in such analyses, caution is warranted when interpreting the findings. 29 All p values were reported as two-tailed, and all analyses were conducted using Stata statistical software (StataCorp, College Station, TX; version 16.0).
Results
Results—literature review
The database search identified a total of 360 records across PubMed, Web of Science, and the Cochrane Database of Systematic Reviews. After removing duplicates, 146 studies remained for screening. Based on title and abstract review, 130 studies were excluded due to nonrelevant populations (i.e., not involving newborn or preterm infants), lack of relevance to pain management, or not being in a meta-analytic format.
Of the 16 studies retrieved for full-text assessment, 8 did not meet the inclusion criteria. Reasons for exclusion included lack of meta-analytic methodology, inclusion of observational studies only, absence of breastfeeding or breast milk taste/odor interventions, and failure to report outcomes related to painful procedures.
Ultimately, eight meta-analyses were included in this umbrella review. However, two of these meta-analyses presented breastfeeding and breast milk outcomes separately; therefore, these were evaluated independently, resulting in a total of 10 meta-analytic datasets.
Collectively, these meta-analyses synthesized the findings of more than 138 randomized controlled trials involving over 7,371 newborn and preterm infants. All included meta-analyses evaluated the effects of nonpharmacological interventions—specifically breastfeeding, breast milk taste, and/or breast milk odor—on procedure-related pain in neonates. The study selection process followed PRISMA 2020 guidelines and is presented as a flow diagram in Figure 1.
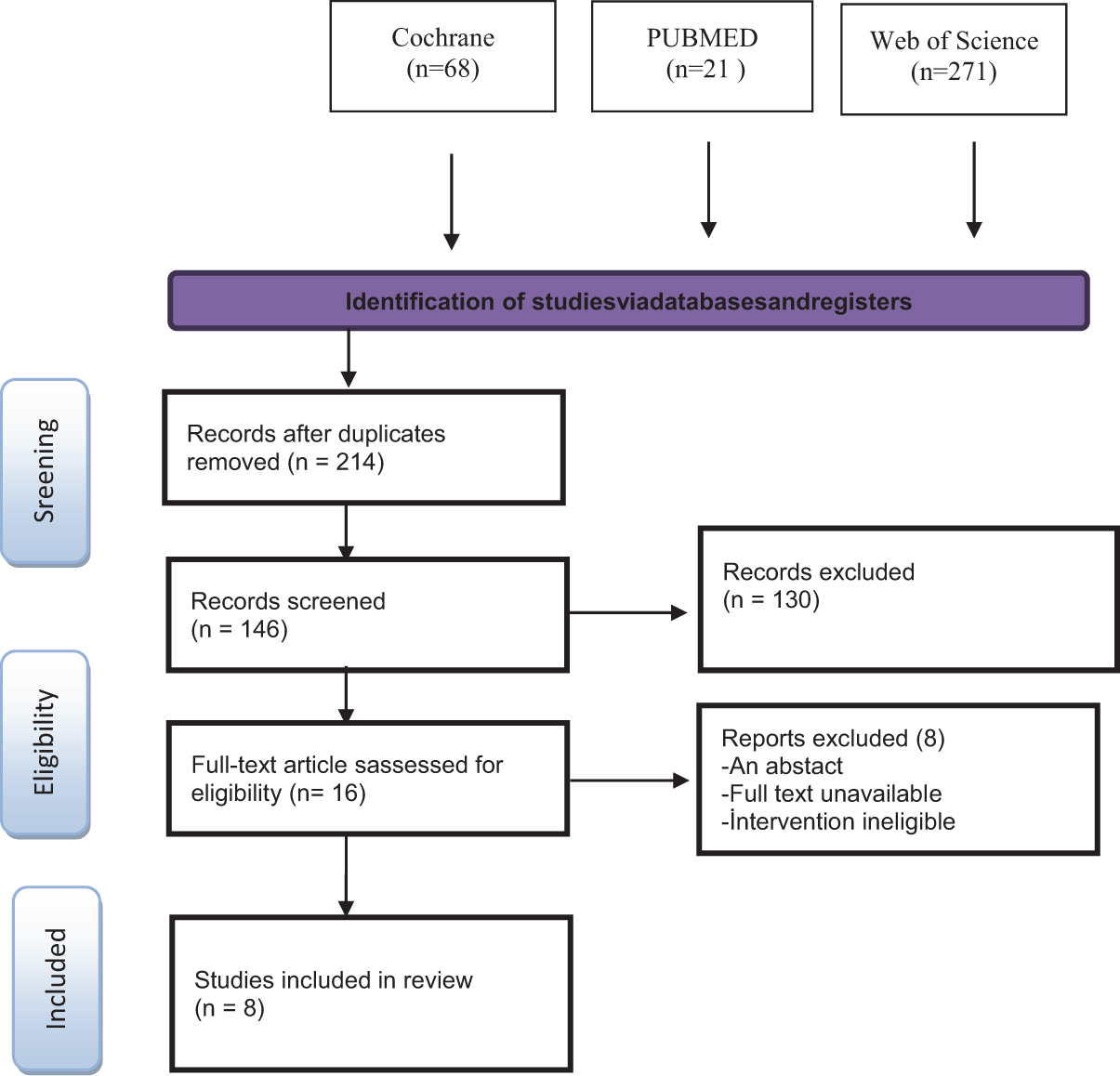
Flow diagram of study retention process for the meta-analysis and systematic review.
Meta-analyses of RCTs
In the RCT–based meta-analyses included in this umbrella review, breastfeeding, breast milk taste, and breast milk odor interventions were compared with standard care, placebo, or no-intervention controls. Across the included meta-analyses, the median number of RCTs per review was approximately 13.8 (IQR: 7–37). The mean total sample size was estimated to be around 737.1 infants (IQR: 137–1,866).
The most frequently examined outcome measures were pain scores (n = 10), heart rate (n = 9), oxygen saturation (n = 7), and crying duration (n = 7). The majority of meta-analyses focused on commonly performed painful procedures in newborns, including heel lance, venipuncture, injection/vaccination, and intravenous catheter placement.
The summarized meta-analytic findings indicate that breast milk-related sensory interventions provide clinically meaningful and consistent reductions in procedure-related pain among neonates. Breastfeeding demonstrated the strongest analgesic effect among the evaluated interventions, with most meta-analyses reporting moderate to large effect sizes. Interventions involving breast milk taste and odor yielded small to moderate improvements, particularly in physiological stress responses and behavioral indicators. Overall, the findings of this umbrella review suggest that breast milk-based interventions are safe, feasible, and effective methods for reducing pain in newborns.
A substantial proportion of the included meta-analyses reported strong and clinically significant effects of breastfeeding, breast milk taste, or breast milk odor on neonatal pain outcomes. SMD, based on the extracted Excel dataset, ranged from –0.79 to –4.70, with >70% of analyses showing effect sizes of –0.80 or larger in magnitude. These values indicate that breast milk-related sensory stimuli produce medium to very large analgesic effects in newborns.
However, heterogeneity levels varied considerably across meta-analyses. In most reviews, I2 values ranged between 66% and 98%, with approximately 66% of analyses exhibiting high heterogeneity (I2 ≥ 75%). This substantial variability may be attributed to differences in population characteristics, the pain assessment tools used, the types of procedures examined (heel lance, venipuncture, injection), and the nature of the interventions (breastfeeding, breast milk odor, breast milk taste).
Conversely, the lowest observed heterogeneity value was 47%, indicating greater consistency in effect direction and magnitude among studies in those analyses. This finding suggests that in certain procedure types or more methodologically homogeneous subgroups, breast milk-based interventions may yield more stable and predictable analgesic effects.
A more homogeneous set of results was reported in the meta-analysis by Zhang et al. (2018), which demonstrated that breast milk odor provides a moderate and statistically reliable analgesic effect (SMD = –0.8; I2 = 47%). This lower level of heterogeneity indicates greater consistency across studies in terms of effect direction and supports the notion that sensory stimulus-based interventions can produce predictable and stable analgesic effects in specific procedural contexts. When these findings are considered alongside the larger effect sizes observed in other meta-analyses within the dataset, it becomes evident that breast milk taste, breast milk odor, and breastfeeding interventions consistently reduce pain across diverse clinical settings.
Regarding publication bias, only one meta-analysis 14 reported Egger’s test results, yielding a p value of approximately 0.05. No other meta-analyses provided assessments of small-study effects or publication bias. Therefore, conclusions about publication bias remain limited; however, the available evidence suggests a moderate level of reliability, indicating that findings should be interpreted with caution but with reasonable confidence in their validity.
The meta-analytic reanalysis of pain outcomes revealed that breast milk–based sensory interventions produce a marked and clinically significant reduction in procedure-related pain among newborns. Although effect sizes varied across individual studies, the overall random-effects model confirmed a strong analgesic effect (SMD = –1.62; 95% CI: –2.25 to –1.00). The high level of heterogeneity (I2 = 88.41%) reflects variability likely attributable to differences in clinical settings and intervention protocols (Fig. 2).
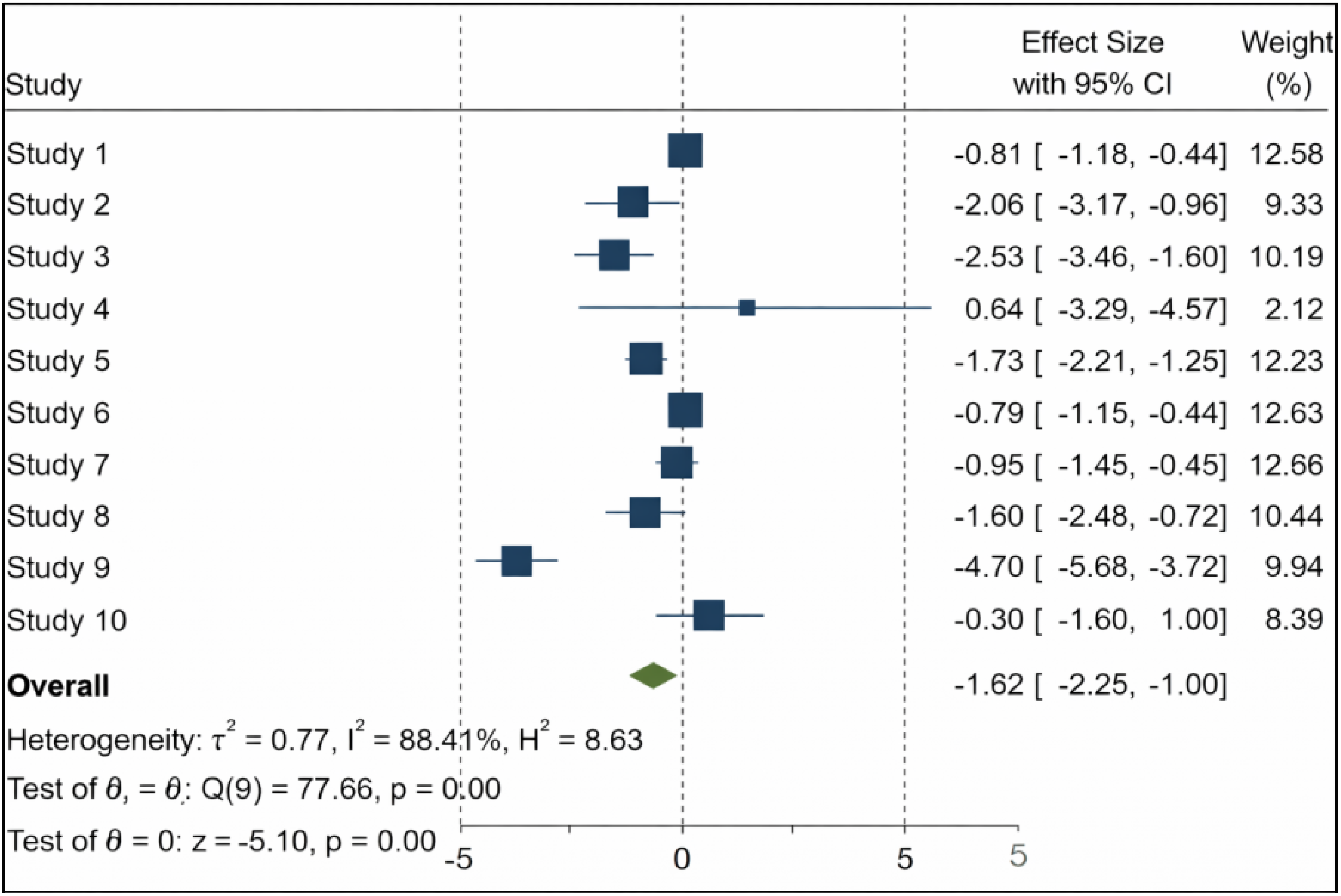
Forest plot comparing pain levels between intervention and control groups based on random-effects meta-analysis.
The funnel plot demonstrated notable asymmetry across studies. Specifically, a leftward shift and broader dispersion in the lower portion of the plot indicate a tendency for smaller-sample studies to report larger effect sizes (Fig. 3).
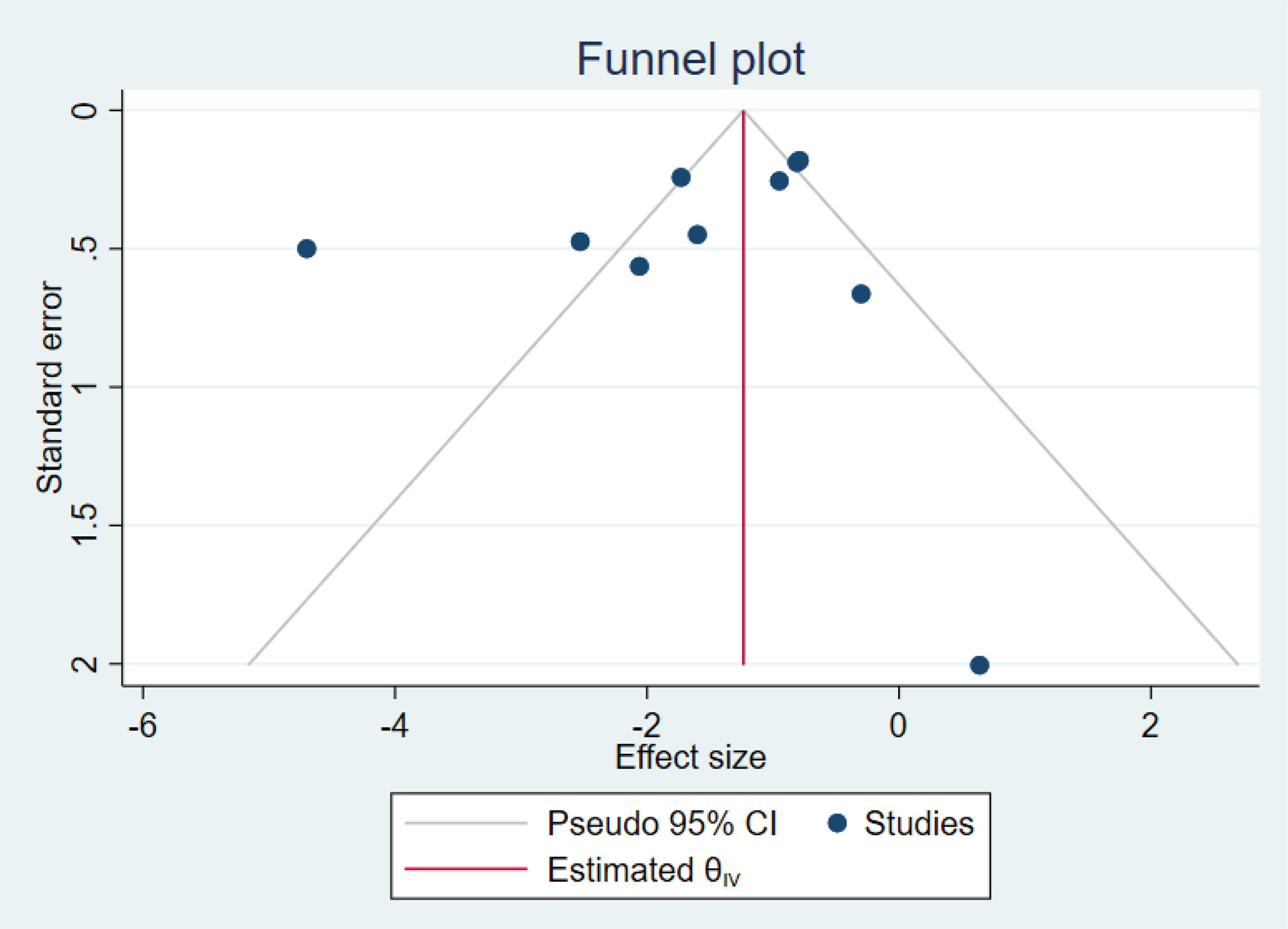
Funnel plot assessing potential publication bias for pain outcomes in the included meta-analytic studies.
Meta-analytic findings regarding crying duration indicate that breast milk-related sensory interventions significantly reduce infants’ behavioral stress responses during painful procedures. The pooled effect size obtained from the reanalysis demonstrated a substantial reduction in crying duration associated with these interventions (SMD = –18.64; 95% CI: –33.15 to –4.14; p = 0.01). Owing to considerable variation across individual studies, heterogeneity was found to be extremely high (I2 = 92.52%), suggesting that differences in procedure type, population characteristics, and intervention modalities may influence the effectiveness of these approaches on crying outcomes (Fig. 4).
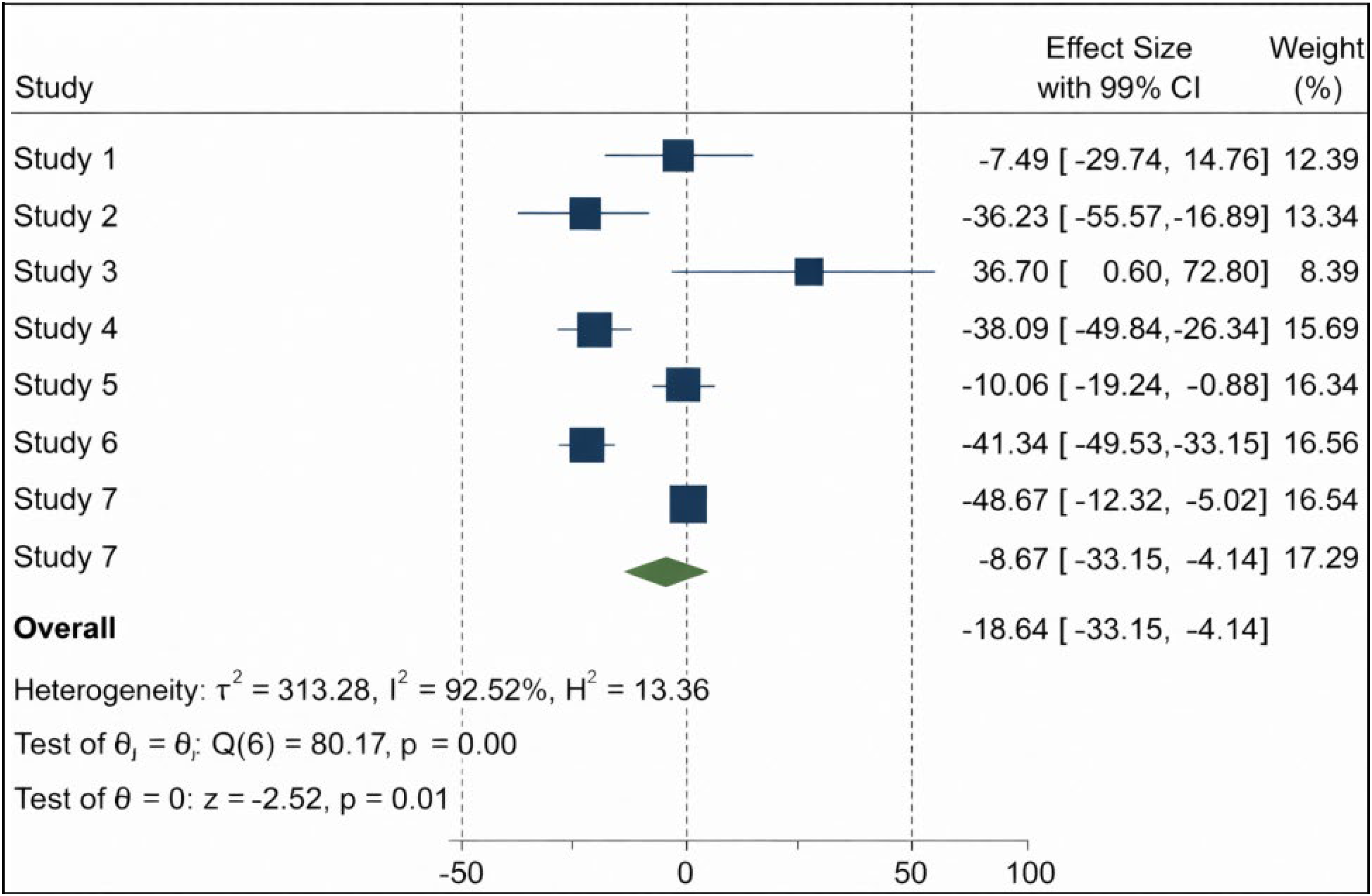
Forest plot comparing crying duration between intervention and control groups based on random-effects meta-analysis.
Meta-analytic reanalysis of heart rate outcomes demonstrated that breast milk-related sensory interventions significantly reduce infants’ physiological stress responses during painful procedures. According to the random-effects model, the pooled effect size indicated a significant decrease in heart rate associated with these interventions (SMD = –5.49; 95% CI: –7.92 to –3.07; p < 0.001). This finding suggests that the taste and smell of breast milk, as well as breastfeeding, are effective in modulating physiological stress responses. The heterogeneity level was moderate to high (I2 = 70.19), indicating considerable variability across studies. This variability may be attributable to differences in procedure types, newborn characteristics (term vs. preterm), pain intensity, and the nature of the interventions employed (Fig. 5).
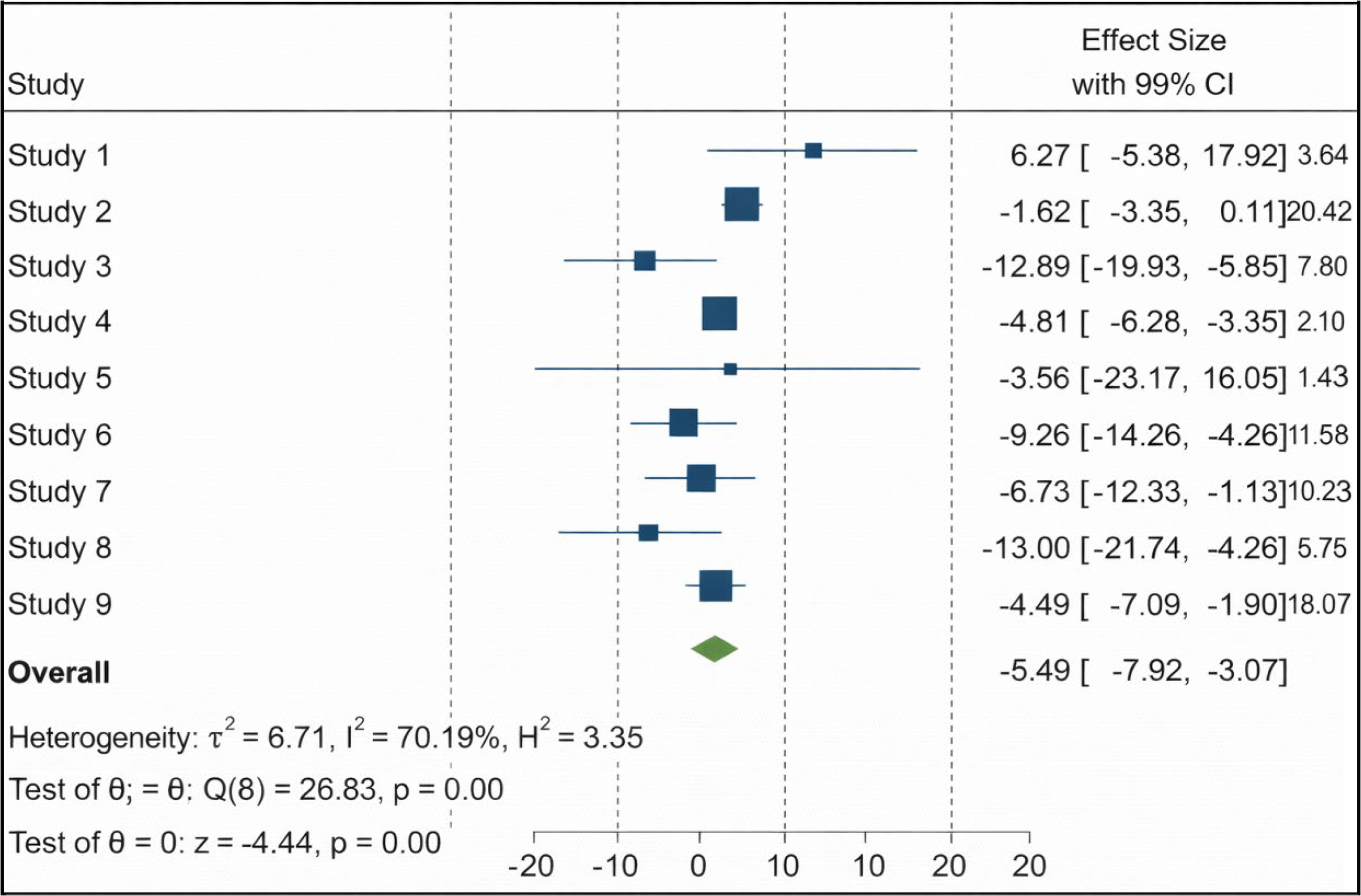
Forest plot comparing heart rate between intervention and control groups based on random-effects meta-analysis.
Meta-analytic reanalysis of SpO2 outcomes showed that breast milk-related sensory interventions have an overall positive effect on oxygen saturation; however, this effect did not reach statistical significance (SMD = 1.36; 95% CI: –0.12 to 2.83; p = 0.07). Although the direction of the effect suggests a potential clinical improvement, the confidence interval crossing zero limits the interpretation of this finding as a definitive indicator of an analgesic physiological response. Heterogeneity was extremely high (I2 = 89.13), suggesting that the variability across studies likely reflects true differences rather than random error. Variations in intervention type (breastfeeding, breast milk odor/taste), gestational age of the infants, the types of procedures performed, and differences in measurement protocols are probable contributors to the high heterogeneity observed (Fig. 6).
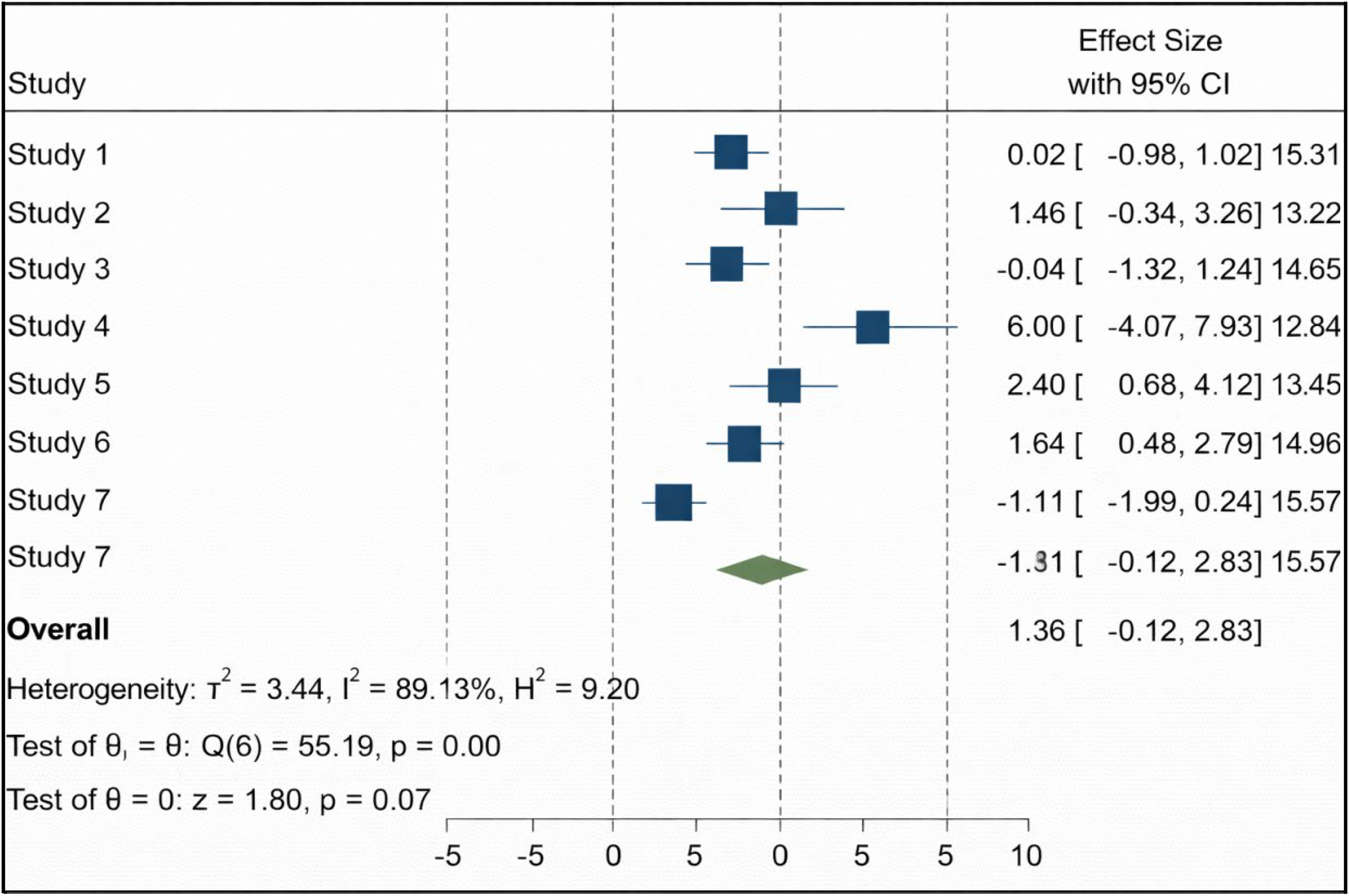
Forest plot comparing SpO2 levels between intervention and control groups based on random-effects meta-analysis.
Overlap among meta-analyses
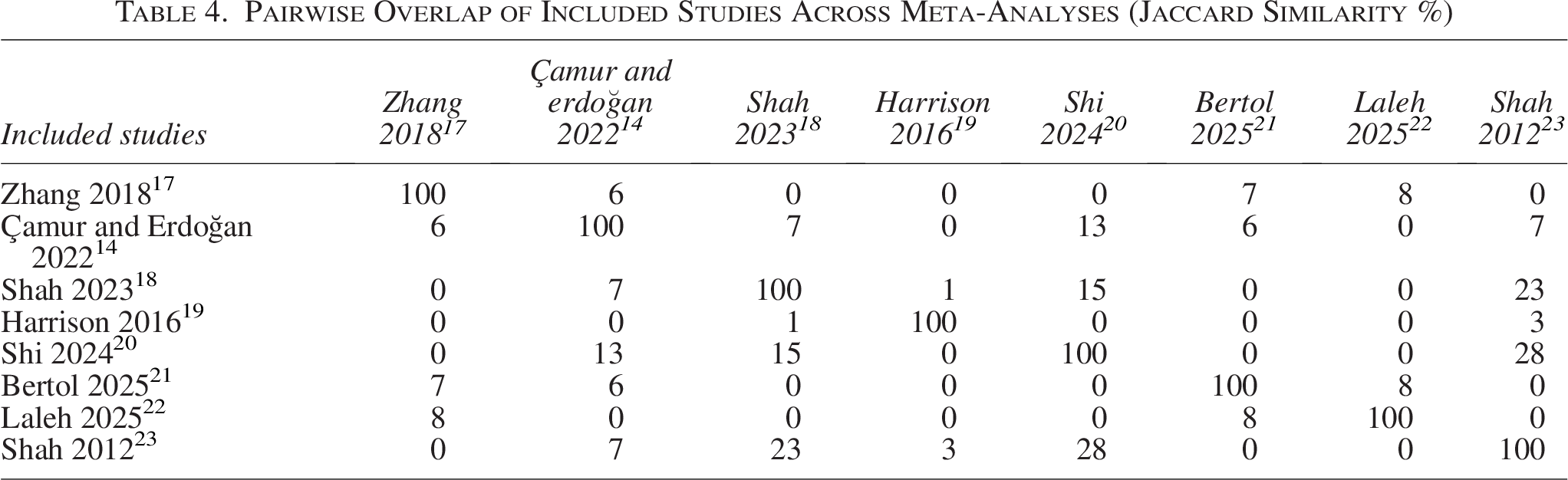
Because the meta-analyses included in this umbrella review examined similar populations (newborn and preterm infants), similar interventions (breastfeeding, breast milk odor, and/or taste), and largely overlapping outcome measures (pain scores, heart rate, oxygen saturation, crying duration), a certain degree of methodological and clinical overlap was observed. Most meta-analyses drew upon different combinations of the same primary randomized controlled trials, reflecting a common methodological challenge in umbrella reviews known as “overlap.” The degree of study-level overlap among the eight included meta-analyses was assessed using the Jaccard similarity coefficient. The results indicated that overall overlap across meta-analyses was low. The highest overlap was observed between Shah et al. (2012) 23 and Shi et al. (2024), 20 with a Jaccard index of 28%. This was followed by a 23% overlap between Shah et al. (2023) 18 and Shah et al. (2012). 23 Most other pairwise comparisons fell within the 0–15% range, with particularly low overlap observed for the meta-analyses by Harrison (2016), 19 Laleh (2025), 22 and Zhang (2018). 17
The presence of only a limited number of shared RCTs across studies indicates that the included meta-analyses vary methodologically and focus on different populations, intervention characteristics, or procedural contexts. These findings suggest that the present umbrella review integrates largely independent and non-redundant bodies of evidence, thereby minimizing the risk of bias from double-counting or duplicated data (Table 4).
Pairwise Overlap of Included Studies Across Meta-Analyses (Jaccard Similarity %)
Quality assessment
According to the AMSTAR-2 assessment, the methodological quality of the included meta-analyses was generally rated as moderate to high. These findings indicate that interventions involving breast milk and breastfeeding provide a moderate-to-high level of evidence supporting their effectiveness in reducing needle-related pain in infants (Table 3). The Cochrane-origin meta-analyses18,19 demonstrated high methodological confidence, meeting all critical AMSTAR-2 domains; these studies fulfilled requirements for protocol registration, comprehensive search strategies, dual screening and data extraction, detailed lists of excluded studies, appropriate risk-of-bias assessments, and complete evaluations of publication bias. The study by Shi et al. (2024) 20 also achieved a high-quality rating, satisfying most critical criteria.
In contrast, the meta-analyses by Zhang et al. (2018) 17 and Çamur and Erdoğan (2022) 14 were rated as low in methodological confidence due to deficiencies in critical AMSTAR-2 domains, such as lack of protocol registration, failure to report excluded studies, and absence of publication bias analyses. The meta-analyses by Bertol et al. (2025), 21 Laleh et al. (2025), 22 and Shah et al. (2012) 23 provided a moderate level of confidence, largely owing to limitations in critical areas such as protocol registration and assessment of publication bias. Common shortcomings across several studies included inadequate reporting of funding sources, lack of justification for excluded studies, and failure to conduct publication bias assessments.
Discussion
The findings of this umbrella review and the accompanying meta-analytic reanalysis demonstrate that breastfeeding, as well as sensory interventions based on the taste and smell of breast milk, exert clinically meaningful and consistent analgesic effects in newborn and preterm infants undergoing procedural pain. The reanalyzed meta-analytic data revealed moderate to very large analgesic effects, particularly on pain scores and behavioral indicators such as crying duration. The fact that most SMDs were below –0.80 suggests that breast milk-related sensory stimuli provide not only statistically significant but also clinically potent soothing and analgesic benefits. This reinforces the importance of nonpharmacological, physiologically grounded, and family-centered pain management strategies during the neonatal period.
The meta-analytic reanalyses further identify breastfeeding as the most effective analgesic intervention among those examined. The pooled effect size for neonatal pain scores (SMD = –1.62; 95% CI: –2.25 to –1.00) demonstrates that breastfeeding substantially reduces procedure-related pain. Similarly, the findings related to crying duration (SMD = –18.64; 95% CI: –33.15 to –4.14) indicate that breastfeeding and breast milk-based interventions markedly attenuate behavioral stress responses. The reduction in heart rate (SMD = –5.49; 95% CI: –7.92 to –3.07) further suggests that these interventions modulate physiological stress responses by decreasing procedure-induced autonomic activation. Although the effect direction for oxygen saturation was positive (SMD = 1.36; 95% CI: –0.12 to 2.83), it did not reach statistical significance; this may indicate that SpO2 is more sensitive-to-severe clinical stressors and may show limited variability during brief, mild-to-moderate procedural stimuli.
Interventions based on the smell and taste of breast milk, while not as potent as direct breastfeeding, still produced small-to-moderate improvements in physiological parameters and behavioral indicators. This finding suggests that sensory stimulation with breast milk represents a valuable alternative in clinical scenarios where direct breastfeeding is not feasible (e.g., intubated preterm infants, infants with restricted oral intake, maternal contraindications). Notably, studies focusing on preterm populations (e.g., Bertol 2025 21 and Laleh 2025) demonstrated meaningful improvements, supporting the notion that the developing neurosensory system responds robustly to mother-specific and breast-milk-specific stimuli.
However, the substantial heterogeneity observed across the included meta-analyses indicates that the findings should be interpreted with caution. A considerable portion of this heterogeneity is likely attributable to differences in procedure types (heel lance, venipuncture, injection, intravenous cannulation), population characteristics (term vs. preterm status, clinical stability), intervention formats (direct breastfeeding, breast milk odor, breast milk taste, duration and timing of the intervention), and the pain assessment tools employed (e.g., PIPP, NIPS, FLACC, NFCS). Moreover, limited sample sizes in some meta-analyses and variability in study design and methodological quality contributed to wide confidence intervals around the effect estimates. Nevertheless, the consistent direction of effects favoring breast milk–based interventions across the majority of analyses supports the robustness of the analgesic benefit despite heterogeneity.
From a methodological standpoint, the AMSTAR-2 appraisal revealed a broad quality spectrum across the included meta-analyses. Cochrane-origin reviews and several high-quality meta-analyses demonstrated strong methodological rigor, including protocol registration, systematic and comprehensive search strategies, dual independent screening and data extraction, integration of risk-of-bias assessments into synthesis, and appropriate evaluation of publication bias. In contrast, several reviews lacked protocol registration, did not report excluded studies with reasons, provided insufficient information regarding funding sources of included RCTs, or omitted publication bias testing—all of which reduced the overall certainty of evidence to a “moderate” level for those analyses. Furthermore, the limited reporting of advanced small-study effect assessments, such as Egger’s regression or excess significance testing, introduces uncertainty regarding the extent of potential asymmetry and positive-result bias.
One of the key strengths of this umbrella review is its exclusive inclusion of RCT-based meta-analyses and its focused examination of sensory interventions involving breastfeeding, breast milk taste, and breast milk odor. This approach enabled the synthesis of a comprehensive, high-level evidence framework demonstrating the analgesic value of breast milk-based nonpharmacological modalities across various invasive procedures in both term and preterm infants. Additionally, the assessment of overlap across meta-analyses using Jaccard similarity indices confirmed that the evidence base exhibited minimal redundancy, indicating that the pooled findings were derived from largely independent sets of RCTs—thereby minimizing the risk of double-counting at the umbrella review level.
This study also presents several important limitations that warrant consideration. First, most of the included meta-analyses did not report prediction intervals or statistical tests for small-study effects, which limited the ability to quantitatively assess the expected range of true effects in future studies or the magnitude of potential publication bias. Second, the substantial heterogeneity observed across analyses could only be interpreted at a methodological and clinical level due to the absence of individual patient data for detailed subgroup exploration. This limitation restricts the ability to determine with precision the specific clinical scenarios in which these interventions exert their strongest analgesic effects.
Conclusion
In conclusion, this umbrella review and meta-analytic reanalysis demonstrate that interventions based on breast milk smell, taste, and breastfeeding are safe, feasible, and effective strategies for reducing procedure-related pain in neonates. Beyond their analgesic benefits, these approaches are inexpensive, easy to implement, and may reduce the need for pharmacological analgesia. Despite the existing methodological limitations, the overall direction and magnitude of the evidence strongly support the integration of breast milk-based interventions into routine clinical practice for neonatal pain management.
Authors’ Contributions
Ç.G. and P.K.: Conceptualization, methodology, investigation, formal analysis, data curation, writing—original draft, writing—review and editing, visualization, supervision, and project administration. Both authors contributed equally to all aspects of the work.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.