
Abstract
Objective:
This study aimed to be the first to quantify dimethyl sulfoxide (DMSO) concentrations in human milk after the maternal dosing and estimate the relative infant dose (RID) to assess potential safety concerns.
Methods:
Human milk samples were obtained at different time points after the mother had received one Rimso-50 treatment. The concentrations of DMSO were then quantified at each time interval by a liquid chromatography-mass spectrometry.
Results:
The maximum concentration (Cmax) was observed to be 34.5 μg/mL at hour 5 post-treatment. The RID was calculated to be 0.45%, while the estimated infant dose was found to be 2 mg/kg/day.
Conclusion:
The findings of the study demonstrate that DMSO’s transfer into human milk is minimal. Additionally, the study provides the first quantification of DMSO in human milk.
Interstitial cystitis/bladder pain syndrome (IC/BPS) is defined by the Society for Urodynamics and Female Urology 2008, as “An unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than 6 weeks duration, in the absence of infection or other identifiable causes.” 1 These painful symptoms often lead to sleep disruption, affecting day-to-day activities, and all together reducing the quality of life for these women. 2 Although the exact number of this disorder is unknown due to the difficulty in making a definitive diagnosis, it is believed that 3.3–7.9 million of women over the age of 18 in the United States are impacted. 3 The etiology of the disorder is not fully understood, but IC/BPS is thought to occur as either a primary or secondary disorder to another underlying cause. 1 Due to IC/BPS’s lack of universal diagnostic criteria and unknown etiology, diagnosing remains difficult. 4 Theories point toward the upregulation of inflammatory genes, glycosaminoglycans causing frequent urination; a damaged urothelium activating mast cells; and/or increased levels of nerve growth factor. 5 First-line available options are behavior/nonpharmacological therapies such as: stress and/or pain management, behavior modification, and physical therapy. Second-line therapies include oral medications and intravesical instillations. 6
Dimethyl sulfoxide (DMSO) has been used to treat IC/BPS since before it was approved by the FDA in 1978. 7 While the precise mechanism of action of DMSO in this syndrome remains unknown, intravesical DMSO therapy is known to have anti-inflammatory properties, as it scavenges for free radicals and inhibits fibroblast proliferation, among other properties that may explain the effectiveness of the medication. 7 Once DMSO is metabolized in the liver, DMSO and its active metabolite, dimethyl sulfone (DMSO2) are mainly excreted via the urine. 8 However, another small fraction of DMSO is reduced to dimethyl sulfide (DMS), which is eliminated via skin and lungs and responsible for the distinctive garlic smell. 9 One of the primary challenges in conducting placebo-controlled trials with DMSO is the garlic smell it produces compared to an unscented placebo. It remains evident from the literature that more guidance and criteria are needed to conduct research on the effectiveness of both the treatment and diagnosis of IC/BPS. 6
DMSO demonstrates exceptional permeability across biological membranes and is known to rapidly diffuse into soft tissues; because of this, its administration raises concern for lactating mothers for potential transfer to breast milk. 10 To help address this concern, a 37-year-old female (61.2 kg), diagnosed with interstitial cystitis/bladder pain syndrome received a single intravesical instillation of Rimso-50 (50/50 dilution of DMSO, 50 mL; 0.54 g/mL; 27 g total). The medication was instilled into the bladder, retained in for 15 minutes, and subsequently voided. After obtaining the mother’s consent, she provided breast milk samples to evaluate DMSO’s transfer into milk. Milk samples were obtained at 5, 11, 19, 24, 27, 32, and 36 hours post Rimso-50 treatment as well as the milk sample just before taking the treatment. At each time point, both the breasts were fully emptied, and milk was mixed to ensure homogeneity. The samples were shipped frozen and stored at −80°C until analysis. A self-reported health information from mother–infant dyad was also provided.
Standards were prepared from DMSO (99%; density 1.1 g/mL). Using the composite density equation: (
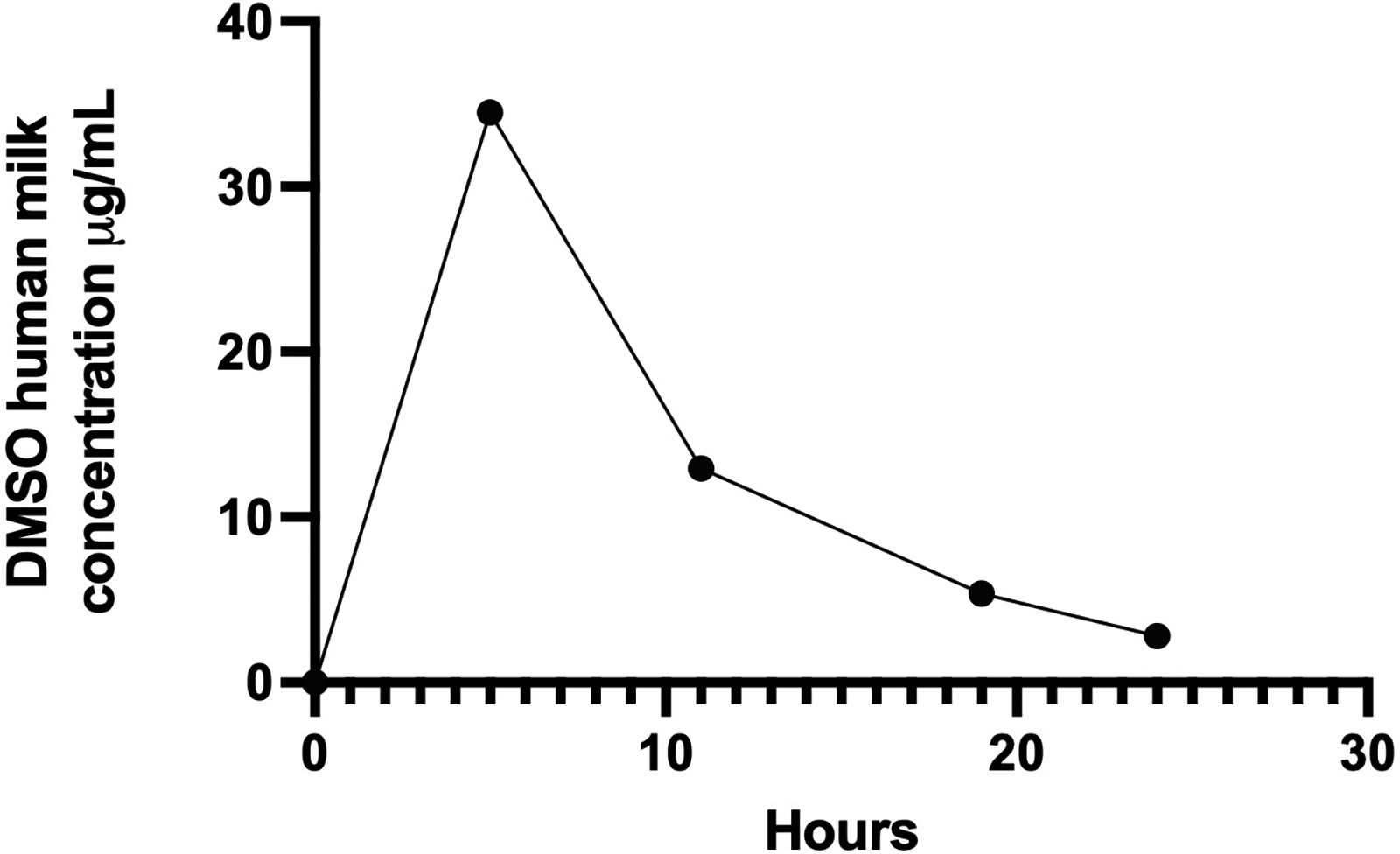
Concentration-time profile of DMSO in human milk following bladder instillation.
In our study the RID was calculated to be 0.45% for a 27 g treatment of DMSO. The estimated infant dose was determined to be 2 mg/kg/day. Although a large portion of the administered dose is not systemically absorbed, the RID was calculated using a 24-hour period to provide a standardized estimate of infant exposure. While milk samples were available at later timepoints, the 24-hour calculation was selected to represent a conservative, “worst-case” (maximal exposure) scenario for estimating drug transfer into milk. The pharmacokinetic parameters derived for DMSO and the graph representing milk levels of DMSO as a function of time are shown in Table 1.
Calculated Pharmacokinetic Parameters of DMSO in Breast Milk after Bladder Instillation
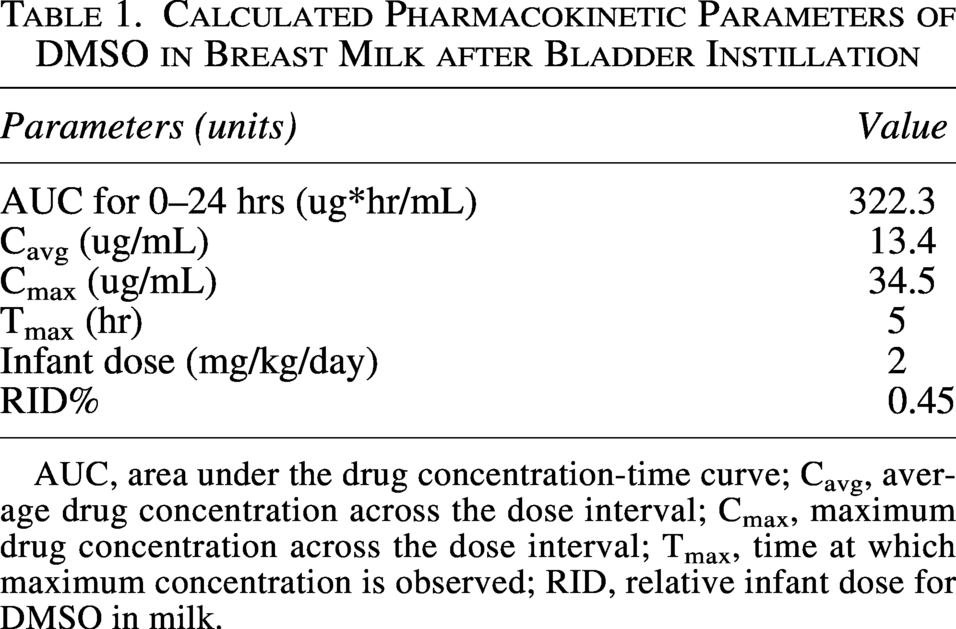
AUC, area under the drug concentration-time curve; Cavg, average drug concentration across the dose interval; Cmax, maximum drug concentration across the dose interval; Tmax, time at which maximum concentration is observed; RID, relative infant dose for DMSO in milk.
Currently, there are no published studies evaluating the transfer of DMSO into human milk. Given DMSO’s characteristic garlic-like odor, it is also unknown whether its presence in breast milk may alter milk palatability, which may influence an infant’s desire to nurse. In this case report, we demonstrate that DMSO is detectable in human milk following intravesical instillation but at minimal concentrations. The calculated RID is below the theoretical value of concern of 10%, suggesting low risk of clinically significant exposure to the breastfed infant. 11 This study has its limitations, including the single-patient design and limited postinstillation milk sampling. Future studies should incorporate more frequent milk collection time points (hourly) over a 24-hour period, a large participant cohort, and systematic infant monitoring and evaluation of repeated DMSO instillations to better define its pharmacokinetics. Additionally, the study did not analyze DMSO2. In future investigations of DMSO, DMSO2 should be measured because of the molecule’s longer persistence in the body. 8 To our knowledge, this is the first reported case of DMSO transfer into human milk following treatment for interstitial cystitis. These preliminary findings provide clinically relevant information for health care providers and lactating women. Future studies are warranted to confirm these findings, further elucidate the pharmacokinetics and safety of DMSO exposure during lactation, and assess any potential effects on an infant.
Footnotes
Acknowledgments
The authors would like to thank the volunteer for donating milk samples, without which this study would not have been possible. This case report involves a single individual and is exempt from Institutional Review Board review in accordance with institutional guidelines. However, the volunteer gave her consent for publication purposes. The authors would like to sincerely thank Dr Thomas Hale for his valuable support and guidance throughout this work. We also extend our gratitude to Kathleen Felkins for her assistance with the analysis.
Disclosure Statement
No competing financial interests exist.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.