
Abstract
Objective:
This study was conducted to evaluate the effects of foot massage applied to the mother in the early postpartum period on breastfeeding success, sleep quality, and newborn stress levels.
Method:
The study was conducted using a parallel-group randomized controlled trial design. The study included 70 primiparous postpartum women who had vaginal deliveries at a public hospital in southern Türkiye between December 2024 and August 2025. Participants were randomized into intervention (n = 35) and control (n = 35) groups. The intervention group received a total of 12 sessions (30 minutes each) of foot massage, three times a week for four weeks, starting from the first week postpartum, in addition to standard postpartum care. The control group received only standard postpartum care. Data were collected using the Personal Information Form, LATCH Breastfeeding Charting System and Documentation Tool, Pittsburgh Sleep Quality Index (PSQI), and the Newborn Stress Scale (NSS). The Mann–Whitney U test, Wilcoxon signed-rank test, and Friedman test were used for data analysis; statistical significance was set at p < 0.05.
Results:
Initially, the groups were similar in sociodemographic and clinical characteristics (p > 0.05). Lactation success (LATCH) scores increased significantly in the intervention group in weekly measurements, and statistically significant differences were found at the 1st, 2nd, and 3rd follow-ups compared with the control group (p < 0.001). Sleep quality (PSQI) scores decreased significantly in the intervention group in the pre-test-post-test comparison (improvement in sleep quality) (p < 0.001). At the same time, no significant change was observed in the control group (p = 0.087). NSS scores decreased more markedly in the intervention group, with significant between-group differences observed at the 2nd and 3rd follow-ups (p < 0.001).
Conclusion:
Foot massage applied to the mother in the postpartum period increases breastfeeding success, improves maternal sleep quality, and reduces newborn stress levels. Foot massage can be considered an effective, safe, and feasible nonpharmacological intervention in postpartum care practices.
Introduction
The postpartum period is an important transitional stage in which mothers experience significant physiological and psychosocial changes and assume responsibility for the care of the newborn. 1 During this period, the mother’s breastfeeding behavior, sleep quality, and stress level play a decisive role in both maternal health and the early development of the newborn.2,3 The World Health Organization recommends initiating breastfeeding within the first hour after birth and ensuring exclusive breastfeeding for the first 6 months. 3 However, conditions such as pain, fatigue, sleep disturbances, and anxiety, which are frequently experienced in the postpartum period, can negatively affect breastfeeding success; they can also reduce milk production and weaken the mother-infant bonding.4,5
It was reported that mothers’ sleep quality decreases significantly in the postpartum period, especially in the first few months. Therefore, ensuring that mothers get sufficient and quality sleep and rest during the postpartum period is critically important for both protecting the mother’s physical and psychological health and for the sustainability of infant care. 6 Sleep, as a fundamental life activity, not only supports the mother’s psychological, physiological, and social health but also makes positive contributions to breastfeeding and infant care.4,5 Conversely, poor sleep quality may lead to postpartum depression, early cessation of breastfeeding, and negative effects on infant development.7,8 Sleep disorders are also a significant source of stress for mothers and may negatively affect hormone secretion, cognitive functions, and mood; breast milk can increase cortisol levels, potentially affecting the neurobiological development of newborns.9,10
For newborns, the postnatal period is a highly sensitive transitional period where adaptation to the external environment begins. The sudden transition from the quiet and protected environment of the intrauterine period to the outside world exposes newborns to stress, particularly due to noise, light, and painful medical procedures in the hospital environment. 11 This stress can negatively impact rapidly developing brain structures; in the short term, it may lead to restlessness, sleep, and feeding problems, and in the long term, to risks in emotional, cognitive, and social development.12,13 Maternal psychological stress has been shown to increase cortisol levels in breast milk and to be associated with negative emotions, such as restlessness, crying, and anxiety, in newborns. 12 These findings reveal that newborn stress is influenced not only by environmental factors but also by maternal biological factors. 12 Therefore, effective stress management in the postpartum period is critical for the physiological maturation and neuropsychological adaptation of the newborn.5,14
In recent years, there has been increased interest in nonpharmacological methods in postpartum care. 15 One of these methods, foot massage, is an effective intervention that supports relaxation and sleep quality by increasing circulation. 16 Foot massage, performed by applying pressure to reflex zones, can also increase breastfeeding motivation by providing relaxation. 17 Previous studies reported that foot massage accelerates breast milk production and supports a successful breastfeeding process.16,18
The current literature has examined the effects of foot massage applied in the postpartum period on pain, fatigue, comfort, mental health, and breastfeeding success; however, studies that comprehensively address these variables and evaluate them in terms of newborn outcomes are quite limited.19–21 Furthermore, although evidence regarding the use of nonpharmacological methods in the postpartum period is increasing, there are no studies specifically investigating the indirect contributions of foot massage to maternal breastfeeding success, sleep quality, and newborn stress.
This study aimed to evaluate the effects of foot massage applied to the mother in the early postpartum period on breastfeeding success, sleep quality, and newborn stress levels. The research aims to be one of the pioneering studies examining the direct and indirect contributions of foot massage to both maternal and newborn health.
Foot massage performed during the postpartum period increases breastfeeding success. Foot massage performed in the postpartum period improves maternal sleep quality. Foot massage performed in the postpartum period reduces stress levels in newborns.
Method
Research design and participants
This study was conducted as a randomized, parallel-group controlled interventional trial. Participants were assigned to the intervention and control groups using a computer-generated random sequence. Due to the nature of the intervention, maternal blinding was not feasible, and no placebo or sham massage was applied. The intervention group received foot massage in addition to standard postpartum care, whereas the control group received only standard postpartum care. Standard postpartum care was provided to both groups in accordance with the routine postnatal care protocol of the hospital before discharge. This care included assessment of maternal vital signs, monitoring of postpartum bleeding and uterine involution, evaluation of pain and general recovery, breastfeeding counseling and support, education on breast care, hygiene, nutrition, rest, newborn care, and warning signs requiring medical consultation. After discharge, study follow-ups were conducted at the participants’ homes for data collection. During home visits, the control group received only follow-up assessments and no massage, reflexology, relaxation exercise, or other complementary intervention. The intervention group received structured foot massage during home visits in addition to standard postpartum care. The only difference between the groups was the structured foot massage intervention applied to the intervention group. The study was conducted on primiparous women who had vaginal deliveries at a public hospital in southern Türkiye.
The study included primiparous mothers aged 18–49 years who were literate, cognitively communicative, had a Pittsburgh Sleep Quality Index (PSQI) global score ≥5, had given birth vaginally after term or singleton pregnancies, had no psychiatric diagnoses, had no health problems that would prevent foot massage, had medically stable newborns, and had no breast problems that would prevent breastfeeding. Only medically stable newborns who stayed with their mothers under routine rooming-in care were included in the study. None of the newborns were admitted to the neonatal intensive care unit during the study period, and no mother–infant separation occurred during follow-up. Newborns who required neonatal intensive care, developed medical problems, or were separated from their mothers during follow-up would have been excluded from the analysis. Therefore, Neonatal Intensive Care Unit (NICU) admission and mother–infant separation were controlled as potential confounding variables in the assessment of newborn stress. Those with chronic/systemic diseases before or during pregnancy, those who experienced complications during delivery, and those with breast problems that would prevent breastfeeding were excluded. During the study, those who wished to withdraw, those with incomplete data forms, those who did not comply with the intervention protocol (those who did not participate in at least three interventions), and those whose newborns developed medical problems were also excluded from the analysis. Mothers who used sleep medications, sedative agents, or pharmacological or herbal galactagogues to improve lactation during the study period were not included in the study. The use of sleep medications, sedative agents, and pharmacological or herbal galactagogues was checked by maternal self-report at baseline and during follow-up assessments. No participant reported using sleep medication, sedative agents, or galactagogues during the study period. Therefore, these factors were controlled as potential confounding variables for sleep quality and breastfeeding outcomes.
The sample size was calculated using the G*Power 3.1.9.7 program, based on Cohen’s d = 0.82 effect size obtained from a previous randomized controlled trial. Assuming α = 0.05 and power (1–β) = 0.95, it was determined that at least 33 participants were needed for each group; considering potential dropouts, 72 participants were planned, and the study was completed with a total of 70 participants: 35 in the experimental group and 35 in the control group.
Participants were randomly assigned to the intervention and control groups using a computer-generated random allocation sequence with a 1:1 allocation ratio. Simple randomization was performed before participant recruitment by an independent researcher who was not involved in recruitment, intervention delivery, outcome assessment, or data analysis. No block randomization or stratification was used. Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes prepared according to the randomization list. Each envelope contained the participant’s group assignment and was opened sequentially only after eligibility confirmation, written informed consent, enrollment, and completion of the baseline assessment. This procedure prevented the researcher responsible for recruitment and baseline data collection from foreseeing the upcoming assignment.
Due to the nature of the intervention, participant blinding was not feasible, and no placebo or sham massage was applied. However, allocation concealment was maintained until the completion of eligibility confirmation, informed consent, enrollment, and baseline assessment.
Of the 120 women assessed for eligibility, 70 met the inclusion criteria and were randomized. Participant flow was prepared according to the CONSORT guidelines and is presented in Figure 1. Reasons for exclusion were not meeting the inclusion criteria (n = 10), refusing to participate (n = 14), lack of spousal consent (n = 21), and change of residence (n = 5). Analyses were performed on all 70 randomized participants.
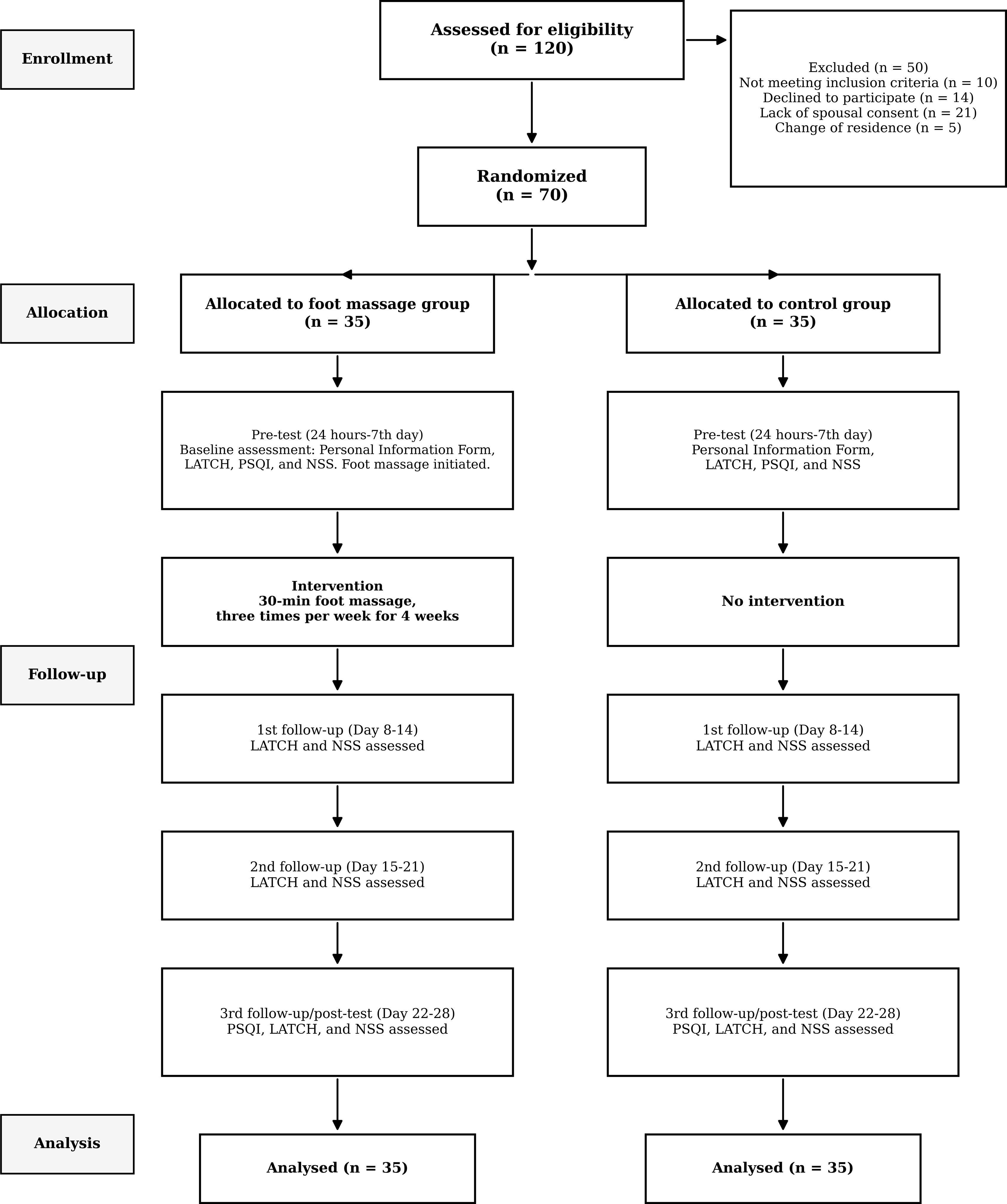
CONSORT flow diagram of the study.
Data collection
The data were collected using the Personal Information Form, LATCH Breastfeeding Charting System and Documentation Tool, PSQI, and Newborn Stress Scale (NSS).
Personal information form
This form was prepared by researchers through a literature review to determine some demographic characteristics (age, family type, educational level, etc.) and obstetric characteristics (number of pregnancies, number of births, number of living children, etc.) of mothers.16,22
LATCH breastfeeding charting system and documentation tool
The LATCH Breastfeeding Charting System and Documentation Tool, developed in 1986, like the APGAR scoring system, is a practical scale that enables objective assessment of breastfeeding and identification of problems. 23 The LATCH Breastfeeding Charting System and Documentation Tool was adapted into Turkish by Yenal and Okumuş (2003), and its reliability and validity study was conducted. 24 The LATCH is an abbreviation consisting of the first letters of five English components. Each item is evaluated between 0 and 2 points, and the total score that can be obtained from the scale ranges from 0 to 10. Higher scores indicate high breastfeeding success. The Cronbach’s alpha internal consistency coefficient of the LATCH scale was found to be 0.95. In this study, it was found to be 0.76.
Pittsburgh sleep quality index
The PSQI was developed by Buysse et al. (1989) to comprehensively assess the sleep quality, type, and severity of sleep disorders in individuals. This index, consisting of 24 items, includes 19 items answered by the individual through self-report, while the remaining 5 items are completed by the individual’s spouse. 25 The Turkish adaptation and validity-reliability study of the index was conducted by Ağargün et al. (1996). The index consists of seven subscales: “Subjective sleep quality,” “Sleep latency,” “Sleep duration,” “Habitual sleep efficiency,” “Sleep disturbances,” “Use of sleep medication,” and “Daytime dysfunction.” The sum of the scores obtained from each subscale constitutes the global score (total sleep quality index). The global score ranges from 0 to 21, with higher scores indicating lower sleep quality. A total score above 5 indicates impaired sleep quality. This suggests that the individual has significant problems in at least two areas or mild to moderate difficulties in three or more areas. In analyses conducted to determine the internal consistency of the scale, the Cronbach’s alpha coefficient was found to be 0.80. 26 In this study, the Cronbach’s alpha coefficient was found to be 0.72.
Newborn stress scale
Developed by Ceylan and Bolışık, the scale consists of 24 items in total, using a 3-point Likert scale. The scale includes 8 subgroups: facial expression, body color, respiration, activity level, soothability, muscle tone, extremities, and posture. Each subgroup is evaluated between 0 and 2 points, with a minimum score of 0 and a maximum score of 16. As the score increases, the stress level of the newborn increases. 27 In the study by Ceylan and Bolışık (2017), the α value was 0.65–0.81. In this study, the reliability coefficient was determined as 0.92.
Data collection process
The data were collected between December 2024 and August 2025 through face-to-face interviews conducted by the researcher at the hospital and during home baseline assessments were conducted within the first postpartum week, between 24 hours and the 7th postnatal day. The same baseline assessment window was used for both the intervention and control groups. Subsequent follow-ups were conducted within predefined weekly postpartum intervals.
Baseline assessment/Pre-test (24 hours–7th postnatal day)
The first meeting took place at the hospital. The Personal Information Form, PSQI, LATCH, and NSS were completed. In the intervention group, the first foot massage session was performed at the hospital, and two additional foot massage sessions were conducted at home during the same week. Each massage session lasted 30 minutes.Participants’ contact and address details were collected to plan future follow-ups.
1st follow-up (days 8–14)
Three foot massage sessions were administered to the intervention group during this week. At the end of the follow-up, the LATCH and NSS were administered.
2nd follow-up (days 15–21)
Three foot massage sessions were administered to the intervention group during this week. At the end of the follow-up, the LATCH and NSS were re-administered.
3rd follow-up/post-test (days 22–28)
Three foot massage sessions were administered to the intervention group during the final week. At the end of the follow-up, the PSQI, LATCH, and NSS were administered as post-tests.
Control group
Baseline assessment/Pre-test (24 hours–7th postnatal day): The first post-natal encounter took place at the hospital. The Personal Information Form, PSQI, LATCH, and NSS were administered. Participants’ contact and address details were collected to plan for subsequent follow-ups. No intervention was applied to the control group. Data were collected face-to-face at the participants’ homes.
1st Follow-up (days 8–14): Assessments were conducted using the LATCH and NSS.
2nd Follow-up (days 15–21): The LATCH and NSS were re-administered.
3rd Follow-up/Post-test (days 22–28): Last week, the PSQI, LATCH, and NSS were administered as post-tests. Figure 1.
Midwifery intervention
Foot massage was planned as a midwifery care intervention in this study and was administered by a single researcher midwife (M.K.), who had completed a 16-hour internationally certified training program on foot massage/reflexology techniques. The training program was intended to provide theoretical and practical competence in the safe and standardized application of foot massage, including foot anatomy, reflex zones, massage techniques, appropriate pressure and rhythm, hygiene principles, contraindications, and monitoring for discomfort or adverse effects. No other researcher or health care professional delivered the foot massage intervention.
Each foot massage session lasted 30 minutes and was performed according to a standardized protocol developed based on the intervention protocol used in the study and supported by previous foot massage/reflexology practices in postpartum and complementary care interventions.16,18,20,28–30 The session consisted of general bilateral preparation, right foot massage, left foot massage, and bilateral closing movements. The protocol was organized as approximately 3 minutes of general preparation, 12 minutes for the right foot, 12 minutes for the left foot, and 3 minutes of closing movements. The same sequence, duration, and repetition numbers were maintained across all sessions to ensure intervention fidelity and reproducibility.16,28
Before the massage, the room temperature was maintained between 23°C and 26°C, and a quiet, softly lit, and hygienic environment was provided. The mother was placed in the supine position, with her head supported by a pillow and a soft roll or small pillow placed under the knees.16,28 Foot hygiene was checked before the procedure. The practitioner washed and warmed her hands and applied a small amount of petroleum jelly or baby oil to both feet to provide lubrication. 29 During the procedure, pressure, rhythm, and intensity were adjusted according to the mother’s individual tolerance. Continuous hand contact was maintained throughout the massage. If the mother reported pain, discomfort, or any adverse effect, the intervention was stopped immediately.16,28,29
During the preparation phase, both feet were stroked simultaneously with slow effleurage movements; both lower limbs were gently lifted, shaken, and stretched; and circular thumb rubbing was applied over the solar plexus reflex area of both feet. The single-foot massage sequence was first applied to the right foot and then repeated on the left foot. This sequence included upward and downward effleurage with both hands 5 times; paired circular rubbing with both thumbs on the plantar surface 5 times and on the dorsal surface 5 times; pressured sliding between the toes 5 times; gliding vibration on the dorsum of the foot 3 times; medial foot effleurage/friction 5 times; lateral foot effleurage/friction 5 times; each toe was rotated 5 times in each direction; the ankle was rotated 5 times in each direction; downward and upward stretching from the ankle 5 times; cross-compression and twisting stretch movements 5 times in each direction; pressured sliding and petrissage on all surfaces of each toe 3 times; circular or pressured sliding on the medial surface of the foot 5 times; and circular friction or pressured sliding on the lateral surface of the foot 5 times. Light tapping on the plantar surface and relaxing effleurage over the entire foot and lower leg were then applied continuously. At the end of the session, simultaneous stretching, gentle traction, and relaxing effleurage were applied to both feet.16,18,20,28–30
Ethics
Ethical approval was obtained from the XXX University’s Research Ethics Committee (22.05.2024-2024/68). Following ethical committee approval, institutional permission was granted by the Kahramanmaraş Provincial Health Directorate (10.07.2024; E-72307149-604) to conduct the research. Written informed consent was obtained from participants before registration. The study was conducted in accordance with the Helsinki Declaration. Participant confidentiality and data security were strictly protected. The study is registered on ClinicalTrials.gov (NCT06786481). Permission was obtained from the original authors for the use of the scales utilized in the study.
Data analysis
In this study, the assumption of normal distribution of continuous dependent variables was evaluated using the Kolmogorov-Smirnov normality test. According to the normality test results, the assumption of normal distribution was not met for the majority of variables (p < 0.05). Based on these findings, nonparametric statistical analyses were used in the study. Descriptive statistics included arithmetic mean and standard deviation, median and interquartile range for continuous variables, and frequency and percentage distributions (n, %) for categorical variables. The chi-square test and Fisher’s exact test were applied to assess group homogeneity in terms of sociodemographic and clinical characteristics for categorical variables. The Mann–Whitney U test was used for intergroup comparisons. The repeated measures Friedman test was used to evaluate changes between weekly measurements within groups, and the Wilcoxon signed-rank test was applied for within-group pre-test-post-test comparisons of the PSQI. All statistical analyses were performed using the SPSS 25.0 software package. The statistical significance level was accepted as p < 0.05.
Results
Table 1 shows the distribution of participants’ sociodemographic characteristics. No statistically significant differences were found between groups in age, educational level, age of the spouse, educational level of the spouse, income, place of residence, marriage duration, and smoking (p > 0.05). Based on these findings, the distribution of sociodemographic characteristics across groups was homogeneous.
Distribution of the Sociodemographic Characteristics of Participants (n = 70)
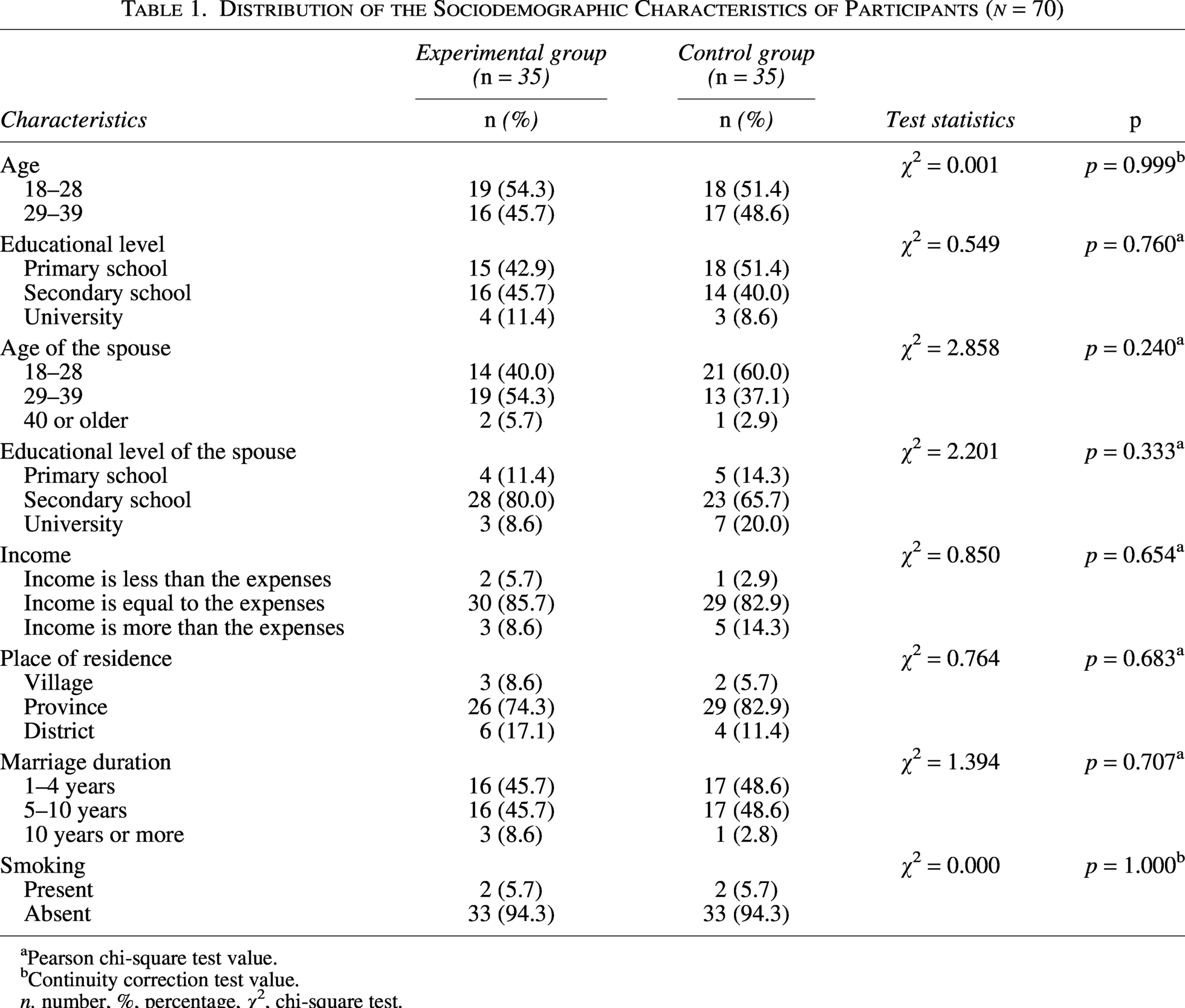
Pearson chi-square test value.
Continuity correction test value.
n, number, %, percentage, χ2, chi-square test.
Table 2 shows the distribution of breastfeeding- and sleep-related characteristics of participants (n = 70). No statistically significant differences were found between groups in terms of breastfeeding duration, receiving breastfeeding education, breastfeeding adequacy, and sleep problems before pregnancy (p > 0.05). Based on these findings, the distribution of breastfeeding- and sleep-related characteristics was homogeneous between the groups. None of the mothers in either group reported using sleep medications, sedative agents, or pharmacological or herbal galactagogues during the study period.
Distribution of Breastfeeding- and Sleep-Related Characteristics of Participants (n = 70)
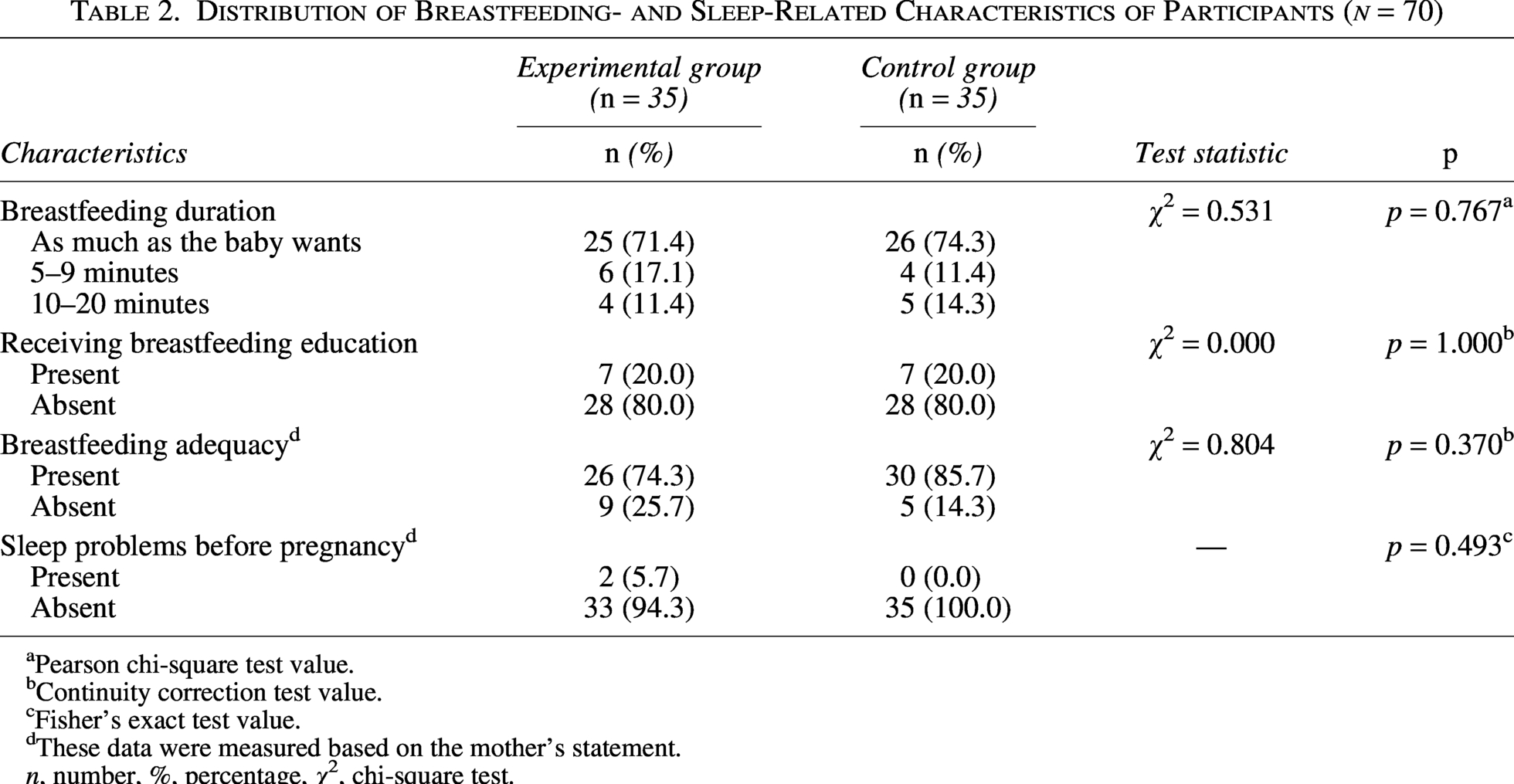
Pearson chi-square test value.
Continuity correction test value.
Fisher’s exact test value.
These data were measured based on the mother’s statement.
n, number, %, percentage, χ2, chi-square test.
Table 3 shows the comparison of the within-group and between-group LATCH mean scores of participants.
Comparison of the within-Group and Between-Group LATCH Mean Scores of Participants (n = 70)
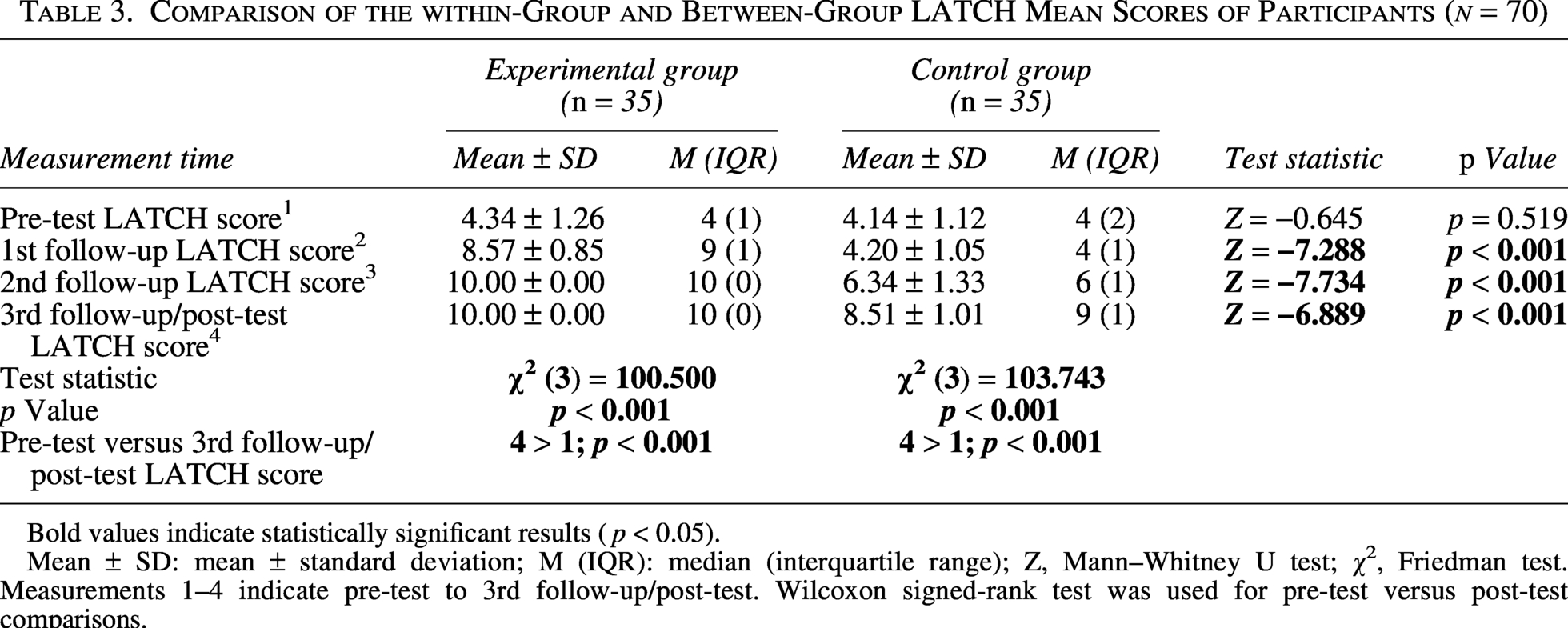
Bold values indicate statistically significant results (p < 0.05).
Mean ± SD: mean ± standard deviation; M (IQR): median (interquartile range); Z, Mann–Whitney U test; χ², Friedman test. Measurements 1–4 indicate pre-test to 3rd follow-up/post-test. Wilcoxon signed-rank test was used for pre-test versus post-test comparisons.
The LATCH mean scores of the participants in the intervention group were 4.34 ± 1.26 at the pre-test, 8.57 ± 0.85 at the 1st follow-up, 10.00 ± 0.00 at the 2nd follow-up, and 10.00 ± 0.00 at the 3rd follow-up/post-test. In the control group, the LATCH mean scores were 4.14 ± 1.12 at the pre-test, 4.20 ± 1.05 at the 1st follow-up, 6.34 ± 1.33 at the 2nd follow-up, and 8.51 ± 1.01 at the 3rd follow-up/post-test. In the between-group comparison, no statistically significant difference was found in LATCH mean scores at the pre-test before the intervention (p = 0.519), whereas statistically significant differences were found in favor of the intervention group at the 1st, 2nd, and 3rd follow-ups after the intervention (p < 0.001, p < 0.001, and p < 0.001, respectively). In the within-group comparison, statistically significant differences were found between measurement times in both the intervention and control groups (p < 0.001 for both groups). In the pairwise within-group pre-test/post-test comparison, LATCH scores increased significantly from pre-test to the 3rd follow-up/post-test in both groups (4 > 1; p < 0.001 for both groups). The increase of + 4.23 points from the pre-test to the 1st follow-up suggests that breastfeeding performance improved markedly in the early postpartum period in the intervention group. The +1.49-point difference between the groups at the 3rd follow-up/post-test suggests that foot massage may provide additional support for breastfeeding success beyond standard postpartum care (Table 3, Fig. 2).
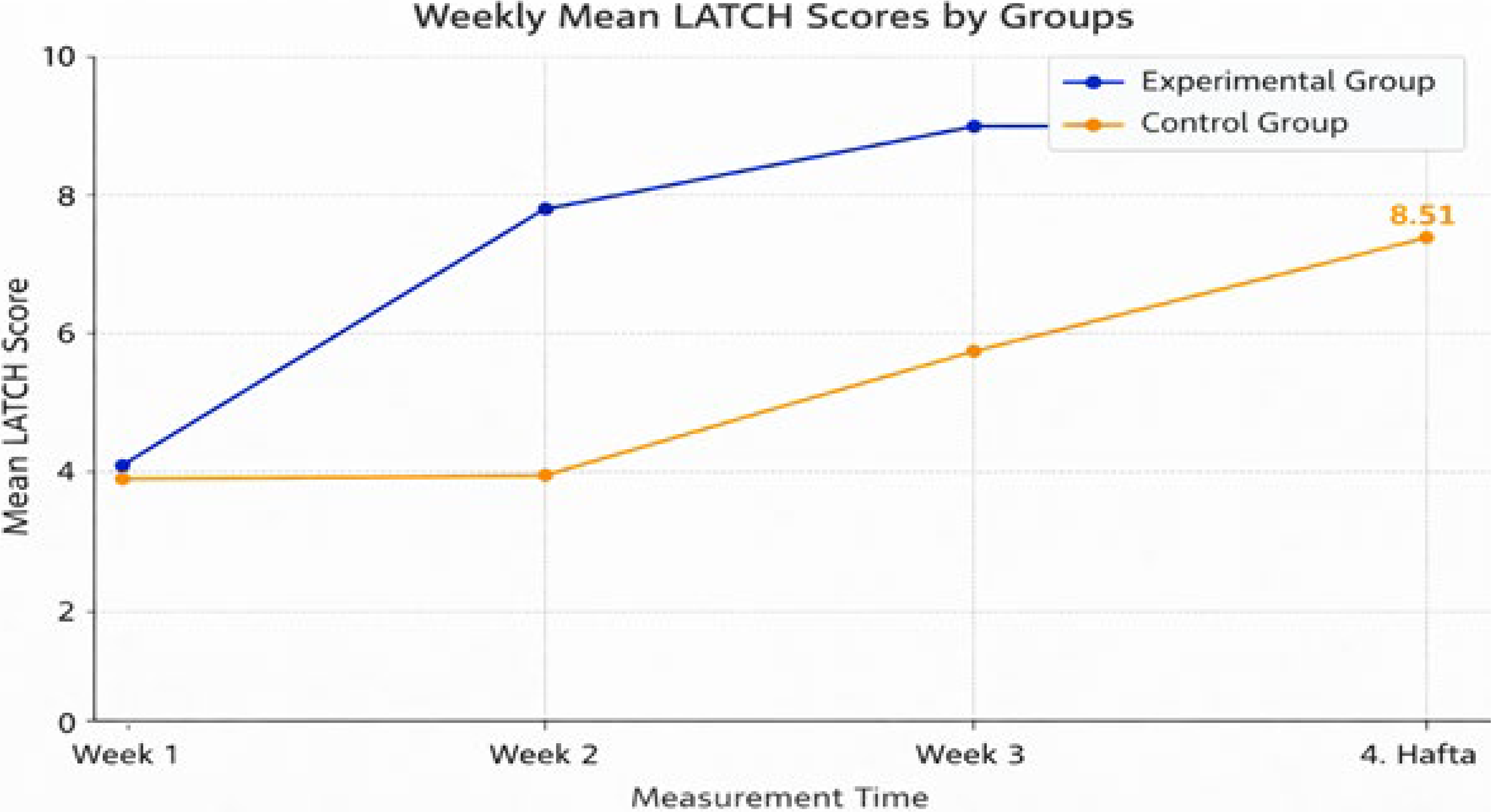
Weekly LATCH mean scores of the groups.
Table 4 shows the comparison of the within-group and between-group PSQI mean scores of participants.
Comparison of the within-Group and Between-Group PSQI Mean Scores of Participants (n = 70)
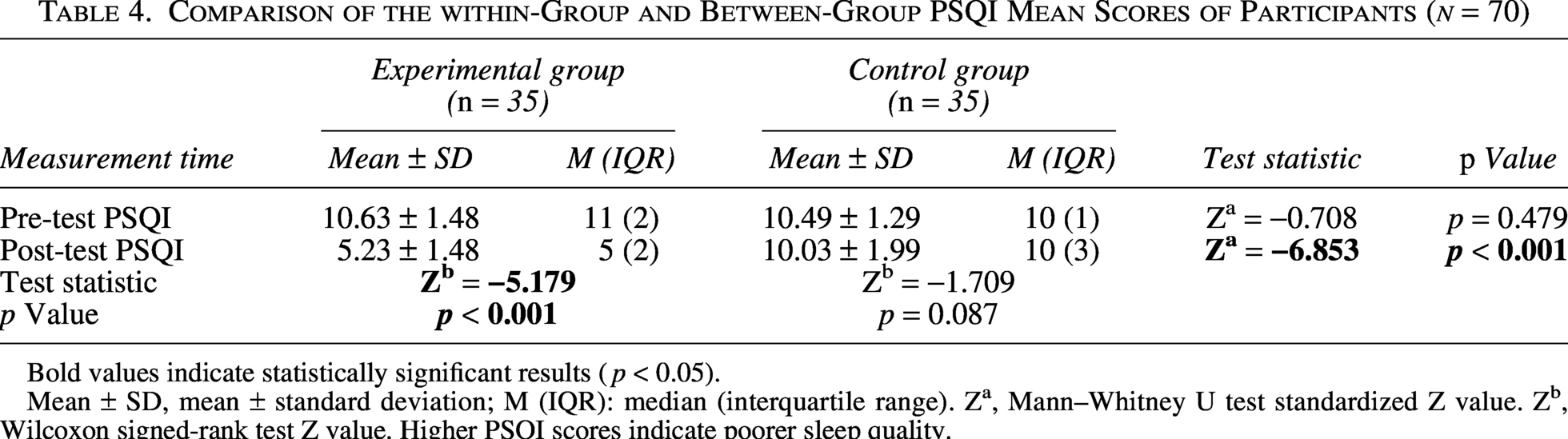
Bold values indicate statistically significant results (p < 0.05).
Mean ± SD, mean ± standard deviation; M (IQR): median (interquartile range). Za, Mann–Whitney U test standardized Z value. Zb, Wilcoxon signed-rank test Z value. Higher PSQI scores indicate poorer sleep quality.
The PSQI mean score of participants in the experimental group was found to be 10.63 ± 1.48 in the pre-test and 5.23 ± 1.48 in the post-test. In the control group, the PSQI mean score was 10.49 ± 1.29 in the pre-test and 10.03 ± 1.99 in the post-test. In the between-group comparison, no statistically significant difference was found in the PSQI mean scores in the pre-test (p = 0.479), while a statistically significant difference was found in favor of the experimental group in the post-test (p < 0.001). In the within-group comparison, a statistically significant difference was found between the pre-test and post-test scores in the experimental group (p < 0.001). No significant difference was found in the control group (p = 0.087). In the experimental group, a decrease of −5.40 points was recorded in PSQI scores between the pre-test and post-test, suggesting a significant improvement in parameters such as time to fall asleep, frequency of nocturnal awakenings, and overall feeling of rest. In contrast, only a minimal change of −0.46 points was observed in the control group, and this change was considered clinically insignificant. The difference between the groups being −4.94 points indicates that foot massage may have a direct and strong effect, especially on sleep quality (Table 4, Fig. 3).
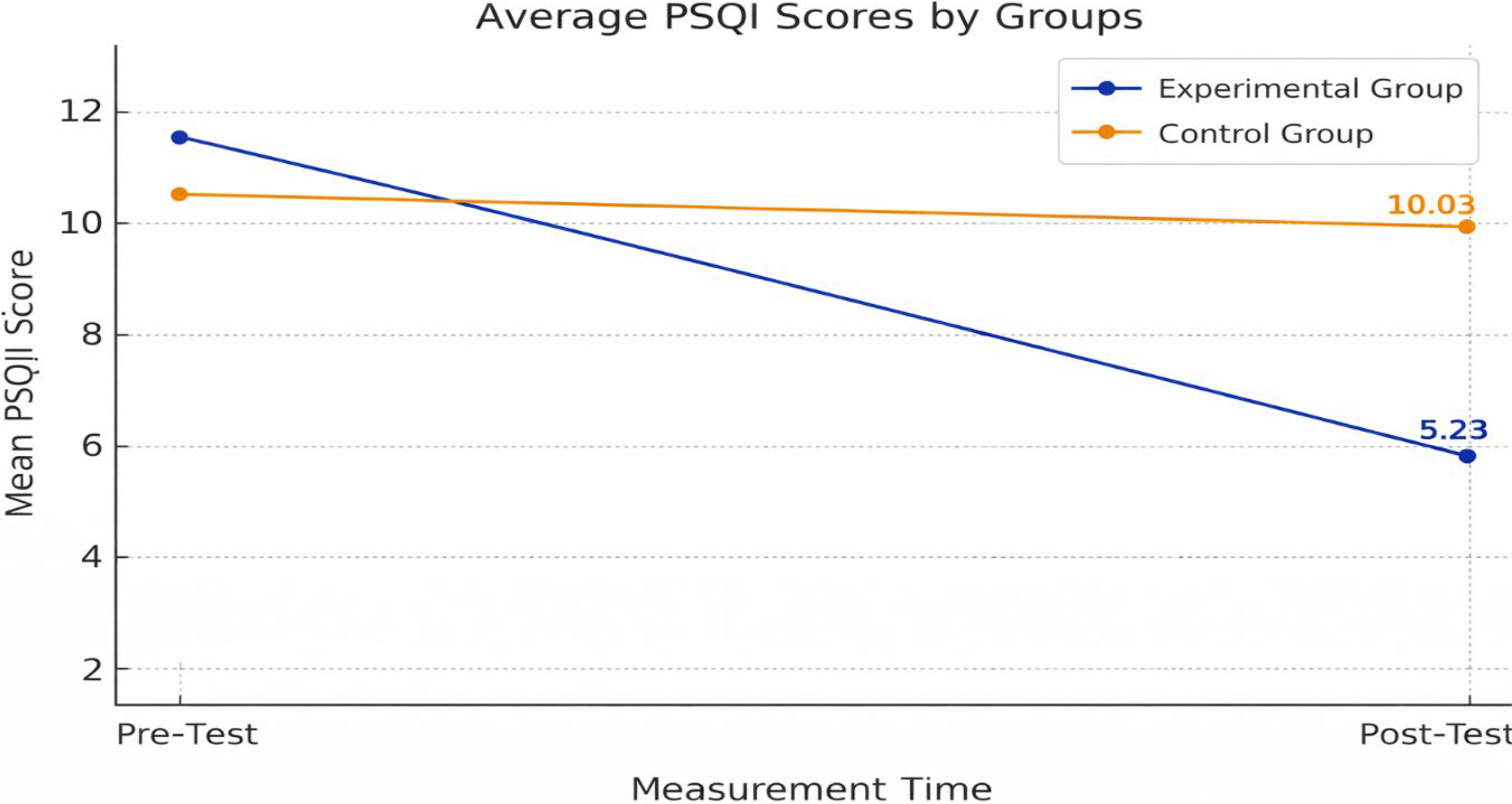
Weekly PSQI mean scores of the groups.
Table 5 shows the comparison of the within-group and between-group NSS mean scores of participants.
Comparison of the within-Group and Between-Group NSS Mean Scores of Participants (n = 70)
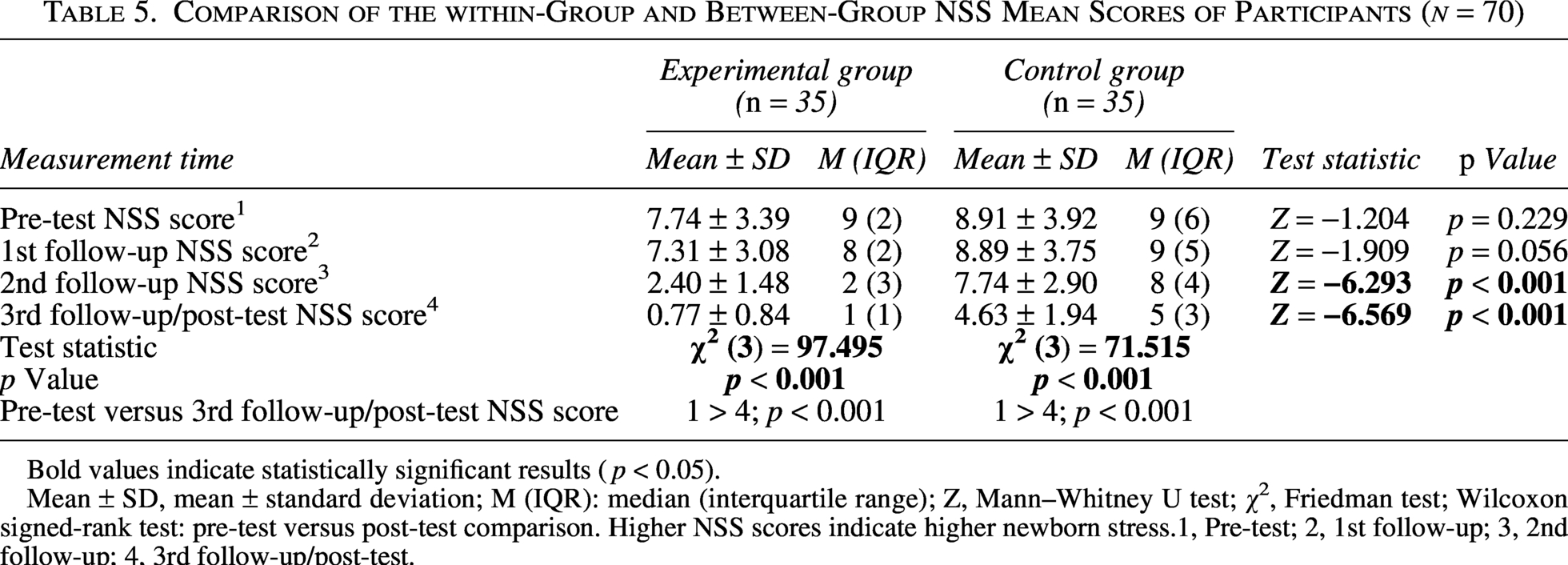
Bold values indicate statistically significant results (p < 0.05).
Mean ± SD, mean ± standard deviation; M (IQR): median (interquartile range); Z, Mann–Whitney U test; χ², Friedman test; Wilcoxon signed-rank test: pre-test versus post-test comparison. Higher NSS scores indicate higher newborn stress.1, Pre-test; 2, 1st follow-up; 3, 2nd follow-up; 4, 3rd follow-up/post-test.
The NSS mean scores of the participants in the experimental group were 7.74 ± 3.39 at the pre-test, 7.31 ± 3.08 at the 1st follow-up, 2.40 ± 1.48 at the 2nd follow-up, and 0.77 ± 0.84 at the 3rd follow-up/post-test. In the control group, the NSS mean scores were 8.91 ± 3.92 at the pre-test, 8.89 ± 3.75 at the 1st follow-up, 7.74 ± 2.90 at the 2nd follow-up, and 4.63 ± 1.94 at the 3rd follow-up/post-test.
In the between-group comparison, no statistically significant differences were found in NSS mean scores at the pre-test and at the 1st follow-up before the effect of the intervention became evident (p = 0.229 and p = 0.056, respectively). However, statistically significant differences were found in favor of the intervention group at the 2nd and 3rd follow-ups (p < 0.001 and p < 0.001, respectively). In the within-group comparison, statistically significant differences were found between measurement times in both the intervention group (p < 0.001) and the control group (p < 0.001). In the pairwise within-group pre-test/post-test comparison, NSS scores decreased significantly from pre-test to the 3rd follow-up/post-test in both the intervention group and the control group (1 > 4; p < 0.001 for both groups). A gradual decrease in NSS scores was observed in the intervention group, reaching almost a minimum level at the 3rd follow-up/post-test, with a total decrease of 6.97 points from pre-test. In contrast, the decrease in the control group was more limited, with a total decrease of 4.28 points. These findings suggest that foot massage applied to mothers may indirectly contribute to reducing newborn stress levels by supporting maternal relaxation and mother–infant interaction (Table 5, Fig. 4).
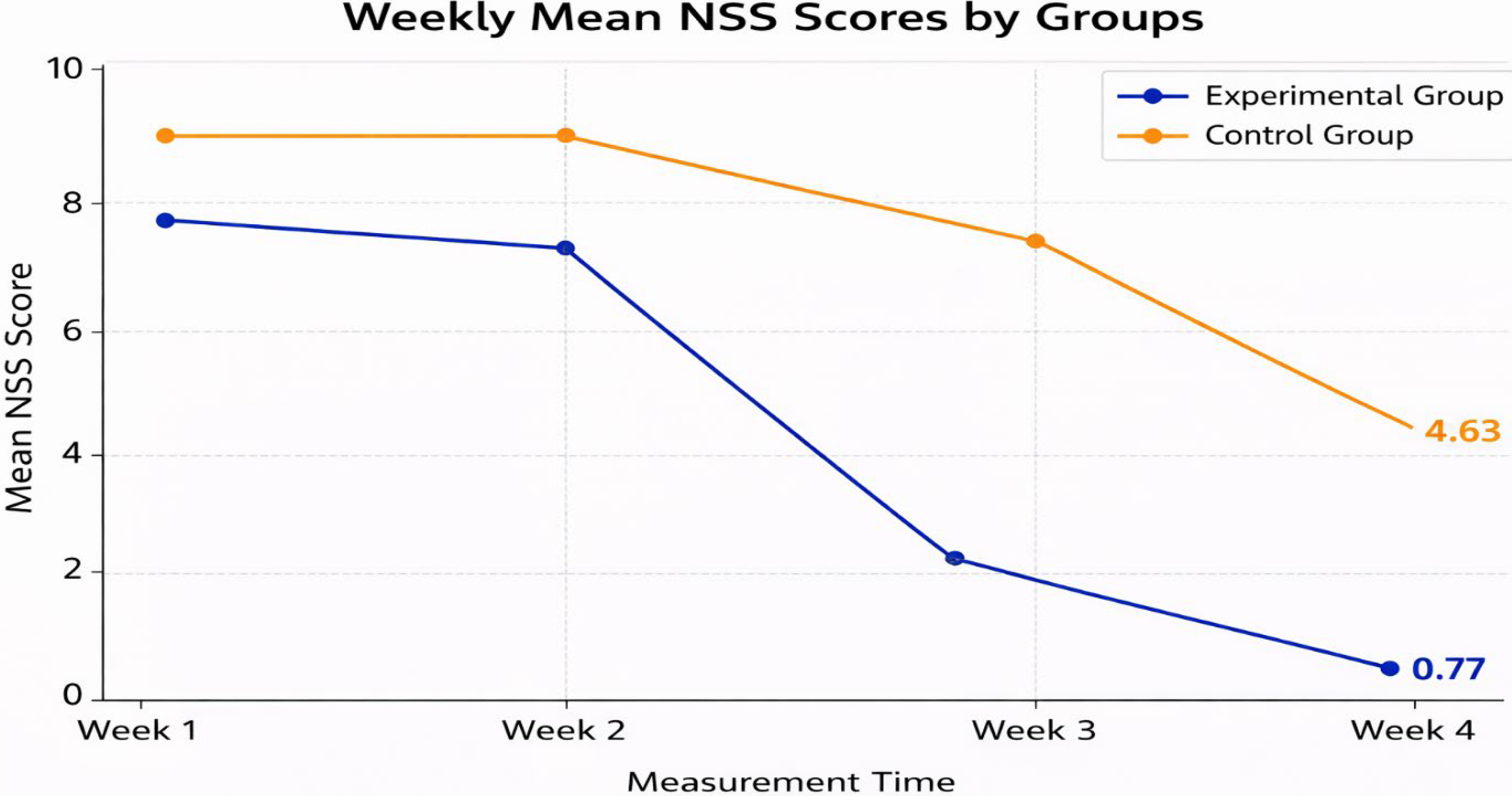
Weekly NSS mean scores of the groups.
Discussion
This randomized controlled trial demonstrated that structured foot massage applied during the first 4 weeks postpartum increased breastfeeding success, improved maternal sleep quality, and reduced newborn stress levels. The initial homogeneity of the intervention and control groups supports attributing the observed differences to the intervention and strengthens the internal validity of the study. The findings suggest that non-pharmacological and holistic approaches in postpartum care may have multifaceted effects on maternal and newborn outcomes.
The significant increase in breastfeeding success observed in mothers who received foot massage indicates a strong clinical effect, not only in terms of statistical significance. The rapid increase in LATCH scores in the early period and their maintenance at a maximum level in the following weeks suggest that the intervention not only accelerates breastfeeding adaptation but also stabilizes performance. In contrast, the more gradual improvement observed in the control group suggests that standard postpartum care alone may be less effective in optimizing early breastfeeding adaptation. The breastfeeding findings of the present study are consistent with previous studies reporting positive effects of foot massage or reflexology on lactation-related outcomes. Kiliçli and Zeyneloglu reported that reflexology improved lactation outcomes in postpartum primiparous women after cesarean delivery, while Çankaya and Ratwisch found that reflexology positively affected lactation and postpartum comfort in primiparous mothers after cesarean delivery. Similarly, Mirzaie et al. reported that foot reflexology massage increased breast milk volume in mothers of premature infants. Although these studies differed from the present study in terms of delivery type, sample characteristics, and lactation outcome measures, their findings support the present result that foot massage may facilitate breastfeeding adaptation and improve breastfeeding performance in the early postpartum period.16,18,30
The underlying mechanisms of this effect can be explained by neurophysiological and psychobiological processes. Massage is known to suppress the stress response by increasing parasympathetic activity and promoting oxytocin release. Oxytocin, in addition to being the primary regulator of the milk let-down reflex, plays a critical role in maternal emotional regulation and bonding processes. Therefore, foot massage may not only directly support lactation physiology but also holistically influence breastfeeding performance by reducing maternal stress and increasing caregiving sensitivity. These findings are consistent with studies reporting positive effects of foot massage and reflexology on lactation initiation and milk production.16,18,30
Sleep quality in the postpartum period is a critical determinant of physiological recovery, emotional balance, and caregiving capacity. In this study, clinically significant improvement in sleep quality was observed in mothers who received foot massages. The minimal change observed in the control group suggests that this improvement may be due to intervention rather than natural adaptation.
The improvement in maternal sleep quality observed in the present study is supported by previous research. Kiliçli and Zeyneloglu found that reflexology improved sleep quality in postpartum women, and Mardasi et al. reported that foot massage reduced sleep disorders during the postpartum period. Similar to these studies, the present study showed a marked improvement in sleep quality among mothers who received foot massage. This consistency suggests that foot massage may improve postpartum sleep quality by promoting relaxation, reducing physiological arousal, and supporting maternal recovery.16,31
Massage techniques have been shown to suppress sympathetic activity, increase parasympathetic response, reduce cortisol levels, and promote neuromuscular relaxation. These mechanisms may improve sleep continuity by reducing hyperarousal, which is frequently experienced in the postpartum period. Improved sleep quality may also indirectly contribute to maternal caregiving behaviors by strengthening stress tolerance, emotional regulation, and physical recovery.
One of the most original findings of this study is that maternal foot massage was associated with a significant reduction in newborn stress levels. The decrease, which became more evident from the second follow-up onward, suggests that the intervention may have an indirect but systemic effect on newborn stress regulation. The more limited decrease observed in the control group indicates that the natural adaptation process alone may not fully explain this change.
Direct studies examining the effect of foot massage applied to mothers on newborn stress levels are limited; therefore, comparison with previous findings should be interpreted cautiously. However, the reduction in newborn stress observed in the present study is indirectly supported by studies showing that maternal psychological state and postpartum stress are associated with infant behavioral and developmental outcomes. Previous evidence indicates that maternal psychological distress may affect breast milk cortisol levels and infant emotional responses, and postpartum stress may influence infant regulation and development. In this context, the present study extends previous evidence by suggesting that a maternal relaxation-based intervention, such as foot massage, may indirectly contribute to newborn stress regulation through improved maternal well-being, sleep quality, and mother–infant interaction.11–13
This result can be interpreted within the framework of the biopsychosocial interaction model between mother and newborn. A decrease in maternal stress may support regulation of the newborn’s autonomic nervous system through increased caregiving sensitivity, strengthened emotional synchronization, and improved quality of physical contact. Maternal psychological state can also influence biological components of breast milk, which may be related to infant behavior. In this context, foot massage may modulate newborn stress responses through both behavioral and potential biological pathways via improved maternal relaxation and sleep quality. 12
When the findings are considered together, foot massage appears to provide not only symptomatic relief in the postpartum period but also an interactive improvement pattern between lactation performance, maternal sleep, and newborn stress regulation. This supports the need to address postpartum care within a biopsychosocial framework. As a low-cost and non-pharmacological intervention, integrating structured foot massage into midwifery care models may be clinically valuable.
Taken together, these findings suggest that integrating structured foot massage into postpartum care may provide a simple, low-cost, and non-pharmacological strategy to support maternal well-being, optimize early breastfeeding outcomes, improve maternal sleep quality, and contribute indirectly to newborn stress regulation.
Limitations
Due to the nature of the intervention, maternal blinding was not feasible, and no placebo or sham massage was used in the control group. This should be considered when interpreting the findings.
Another limitation of this study is that baseline assessments were conducted within a time window ranging from 24 hours to the 7th postnatal day. Since breastfeeding adaptation, maternal sleep quality, and newborn stress may change rapidly during the early postpartum period, this variation in baseline assessment timing may have introduced methodological bias. Although the same assessment window was applied to both groups, this issue should be considered when interpreting the findings.
Conclusion
This randomized controlled trial determined that foot massage applied to mothers in the postpartum period had significant and positive effects on breastfeeding success, sleep quality, and newborn stress levels. Foot massage supported both the physiological and psychological well-being of the mother; this effect was indirectly reflected in the newborn’s stress level. These findings provide unique contributions to the literature on the clinical effectiveness of non-pharmacological interventions in midwifery care.
It is recommended that evidence-based non-pharmacological practices, such as foot massage, be integrated into postpartum care protocols. Theoretical and practical training on foot massage should be included in midwifery education programs. In-service training for health care professionals, especially midwives, should address the physiological and psychological effects of foot massage in light of current scientific evidence. Informative content on the benefits of foot massage should be added to prenatal education programs. It is recommended that foot massage be included as a complementary care practice in national postpartum care guidelines. Further studies examining the effects of foot massage on different age groups and long-term maternal and infant outcomes should be planned.
Authors’ Contributions
Conceptualization and design: M.N.K. and H.G.Ö.; Material preparation, data collection and analysis: The first draft of the article: H.G.Ö. and M.N.K.; Writing—review and editing: H.G.Ö. and M.N.K.; All authors read and approved the final version of the article.
Ethical Aspects of the Study
Ethical approval was obtained from the XXX University’s Research Ethics Committee (22.05.2024-2024/68). Following ethical committee approval, institutional permission was granted by the Kahramanmaraş Provincial Health Directorate (10.07.2024; E-72307149-604) to conduct the research. Written informed consent was obtained from participants before registration. The study was conducted in accordance with the Helsinki Declaration. Participant confidentiality and data security were strictly protected. The study is registered on ClinicalTrials.gov (NCT06786481). Permission was obtained from the original authors for the use of the scales utilized in the study.
Footnotes
Acknowledgments
The authors would like to thank all women who participated in this research.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.