
Abstract
Purpose:
The purpose of the current study was to assess the effect of couple counseling on maternal distraction and attention levels during breastfeeding and nonfeeding childcare in mothers experiencing distractions in Hamadan, western Iran.
Methods:
In this randomized controlled trial, mothers attending comprehensive health centers for routine postpartum care who reported distraction during breastfeeding were enrolled. Participants were assigned via block randomization to an intervention group (standard care plus couple-centered counseling) or a control group (standard care alone). The maternal distraction was measured using the maternal distraction questionnaire at baseline, immediately post-intervention, and at two-, three-, and 4-month follow-ups.
Results:
The analysis included 64 participants in each group. At 4 months, 40.6% more mothers in the intervention group than in the control group reported not being at all distracted during breastfeeding, with a 36% difference in favor of the intervention group for very high attention. Corresponding figures during childcare were 42.2% and 37.5%, respectively. A significant interaction between time and group was observed for both maternal distraction during breastfeeding and during childcare (p < 0.001). In the intervention group, maternal distraction during breastfeeding decreased from 17.89 ± 2.53 at baseline to 8.31 ± 1.27 at 4 months, and during childcare from 18.03 ± 1.94 to 8.98 ± 2.06. In the control group, these scores decreased only slightly, from 16.84 ± 2.50 to 15.52 ± 2.37 for breastfeeding and from 17.84 ± 2.44 to 15.19 ± 2.29 for childcare.
Conclusion:
Our study showed that a couple-centered counseling intervention significantly reduced maternal distraction and improved attention during breastfeeding and childcare.
Keywords
Introduction
Women face many challenges in initiating and continuing breastfeeding. 1 Child nutrition in the first years of life, particularly during infancy, is critically issue. 2 Proper nutrition ensures the healthy and appropriate growth of the child, and the positive effect of breast milk on the growth and development is well established. 3 In Iran, only 56% of infants are exclusively breastfed until 4 months of age, and 28% until 6 months. 4 According to the World Health Organization, almost all mothers are able to breastfeed their infants. 5 However, in 2011, 38% of the world’s infants younger than 6 months had exclusive breastfeeding. A more recent global study of low- and middle-income countries from 2010 to 2018 reported rate of 45.7% exclusive breastfeeding. 6
Factors that contribute to higher breastfeeding rates include maternal knowledge, support networks, socioeconomic status, and self-efficacy.7,8 Other key factors are environmental, such as family functioning, sociocultural norms, and marital satisfaction. 9 The lack of spousal support is shown by some mothers as a reason for discontinuing exclusive breastfeeding. 10 In addition, targeted education to correct false beliefs, combined with active family support, is shown to improve the continuation of exclusive breastfeeding. 11
Today, media technologies are integrated into everyday life, providing individuals with information, entertainment, and opportunities for social engagement. 12 In Iran, more than 88% of people aged 10 to 65 use social media. These platforms are used for reasons of connecting with others (48.9%), getting news (40.7%), and browsing the internet in general (40.6%). 13 The advantages of utilizing smartphones and mobile applications have been demonstrated in various studies to promote health, exchange health information, and support patient screening, monitoring, and management. 14 However, long-term use of smartphones can have an adverse effect on physical health and psychosocial well-being and lead to addictive and dependent behavioral patterns. 15 The increasing integration of technology into daily life carries risks. For new mothers, higher levels of parenting stress are associated with increased social media use. 16 Feedings were classified as distracted when mothers reported engaging in activities other than feeding or interacting with the infant. 17 Accumulating evidence suggests that maternal distraction (e.g., watching television or using a mobile device) may influence infant feeding interactions and subsequent outcomes.17,18 A study by Arezi et al. (2024) investigated the effect of family-centered counseling on breastfeeding continuation among mothers experiencing distraction. Their results indicated that this intervention successfully reduced maternal distractions during both breastfeeding and other activities. 19 Building on this evidence for the importance of support-based interventions, the purpose of the current study was to assess the effect of couple counseling on maternal distraction and attention levels during breastfeeding and nonfeeding childcare in mothers experiencing distractions in Hamadan, western Iran.
Materials and Methods
Study design and setting
This randomized controlled trial (RCT) was performed in Hamadan City, western Iran. Hamadan is 1850 meters above sea level and located approximately 360 km southwest of Tehran. The study period spanned from October 15 to December 30, 2025.
Ethical
Before enrolment, written informed consent was given by all breastfeeding women. Ethical approval was obtained by the Ethics Committee of Hamadan University of Medical Sciences (Registration ID: IR.UMSHA.REC.1404.240) and the Iranian Registry of Clinical Trials (Code: IRCT20180707040370N14).
Inclusion and exclusion criteria
Inclusion criteria were distraction during breastfeeding based on the maternal distraction questionnaire (MDQ), age greater than 18 years, 2–6 weeks postpartum, exclusive breastfeeding or mixed feeding (breast milk and formula), and having a healthy, full-term singleton infant. Exclusion criteria were breast anomalies and incomplete completion of the questionnaire.
Sample size
The sample size was determined based on the findings of Arezi et al., which reported a large effect size (Cohen’s d = 0.80) 19 for family-centered counseling on reducing distraction in breastfeeding women. Using a conservative effect size of 0.30, a power of 80%, a two-sided alpha of 0.05, and an assumed intracorrelation of 0.50 between repeated measures, the sample size calculation determined a requirement of 58 participants per group. Considering an estimated 10% attrition rate, the sample size was increased to 64 participants per group.
Measurement tools
Demographic characteristics
Demographic characteristics were including husband’s age, maternal occupation, maternal education, husband’s education, husband’s occupation, household income, child’s sex, number of children, and mode of delivery.
Maternal Distraction Questionnaire
The MDQ, a 14-item self-report instrument developed by Ventura, 20 encompasses a range of activities in which mothers may engage during interactions with their infants. The 10 items in the first section measure how often mothers engage in activities (e.g., watching television, using a phone, or reading) while feeding or caring for their infants. Responses are recorded on a 5-point Likert scale (1 = never to 5 = always). Section two comprises four items that measure the mother’s overall level of attentiveness while interacting with her infant, which are rated on a 5-point scale from 1 (not at all distracted/very high attention) to 5 (very distracted/very low attention). Accordingly, higher scores denote higher levels of distraction and lower levels of attention, whereas lower scores denote lower levels of distraction and higher levels of attention. The questionnaire has been evaluated for validity and reliability by Ventura et al., 20 with Cronbach’s alpha of 0.86 for technological activities and 0.95 for non-technological activities. For use in the Iranian context, Arezi et al., 21 confirmed the questionnaire’s validity and reported an overall Cronbach’s alpha of 0.75 for reliability.
Sampling
Sampling was performed from five comprehensive urban health centers (five geographical regions: center, north, south, west, and east). Following enrollment during postpartum visits, participants were randomly allocated to two groups using block randomization (block size of four). The randomization sequence (e.g., AABB, ABAB, and BAAB) was generated with a fixed allocation ratio of 1:1. Each block of four participants contained two assignments to the intervention group (A) and two to the control group (B). Randomization was performed by a member of the research team (M.B.) who had no role in participant recruitment or intervention implementation. The randomization sequence was generated using a random number table to create blocks of four, ensuring balanced group sizes. To ensure allocation concealment, the randomization sequence was prepared by an independent person not involved in recruitment or intervention. They generated random blocks, wrote each assignment on a card, and placed it in a sequentially numbered, opaque envelope before sealing it. The sealed envelopes were stored together in a box. During enrollment, the researcher opened the next consecutive envelope to reveal the participant’s group.
Interventions
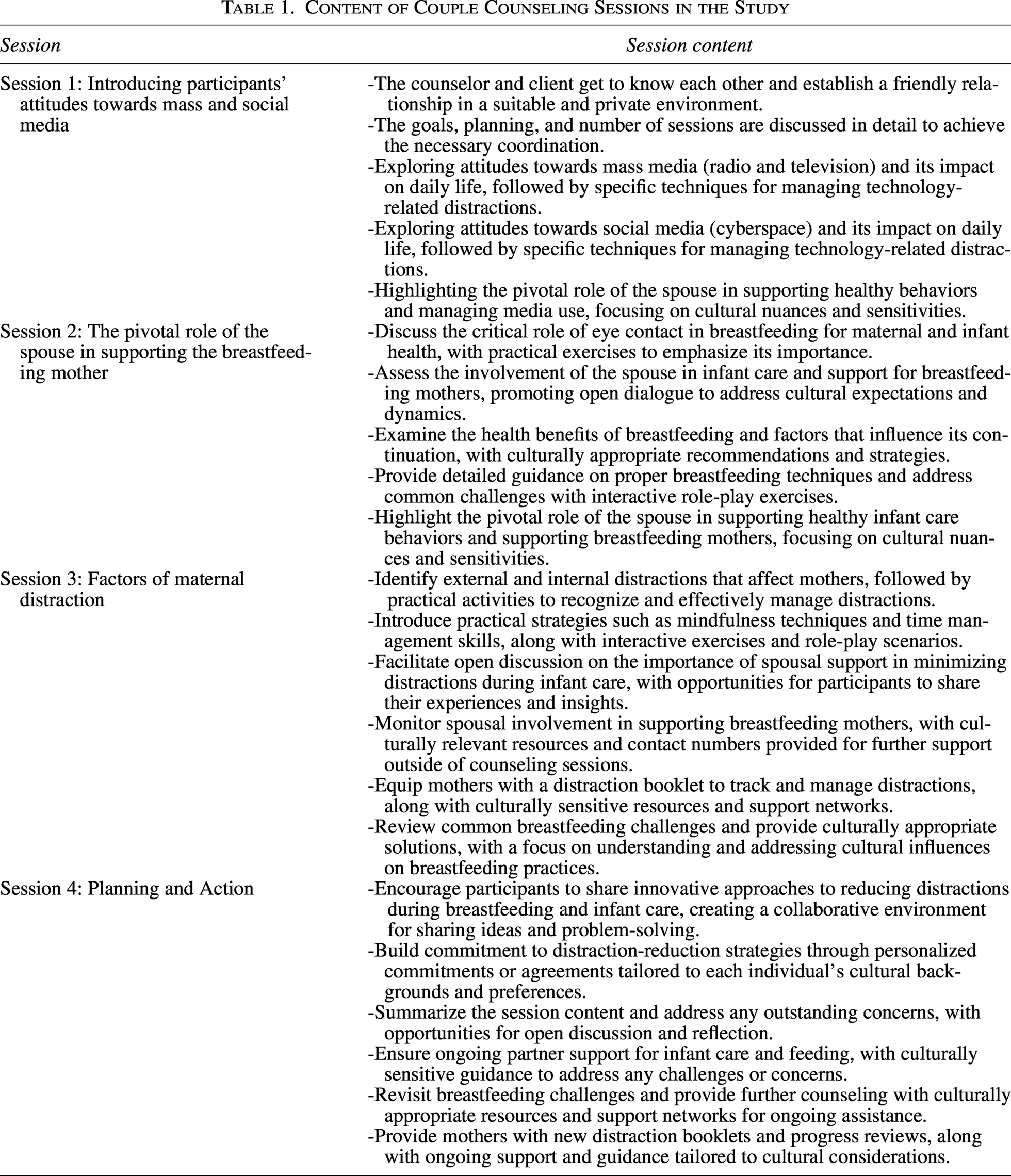
Participants in the control group received the standard postpartum care protocol. This protocol begins with breastfeeding education in the hospital immediately after delivery and includes three scheduled visits at comprehensive health centers (days 3, 15, and 40). Standard counseling during these visits was the following topics: Personal hygiene, breastfeeding, infant vaccinations and care, vitamin use, screening for postpartum complications (hemorrhage/infection), family planning, and nutrition. In addition to standard care, the intervention group received, for 4 weeks, face-to-face couple counseling sessions (45–60 minutes each) involving the mother and her spouse, based on established protocols.19,22 It was conducted by a PhD candidate in midwifery. All mothers completed the questionnaires and were asked to attend the educational sessions together with their husbands to enhance the effectiveness of the intervention. The intervention was designed with a focus on spousal support to reduce maternal distraction. This was achieved by providing a calm environment for feeding (such as managing noise and designating a quiet space), sharing household responsibilities, providing emotional encouragement to limit smartphone use, and strengthening parent-infant bonding. Outcomes were measured at the following time points: Pre-intervention, after the completion of the fourth session, and at follow-ups during the second, third, and fourth months postpartum. The content of couple counseling sessions is presented in Table 1. Due to the educational nature of the study, blinding was not performed.
Content of Couple Counseling Sessions in the Study
Statistical analyses
The distribution of baseline demographics between the two study groups was tested using the chi-square test. This test was also used to compare the distribution of maternal distraction and attention levels during breastfeeding and childcare across follow-up times. The normality of the data was checked at each time point using the Shapiro–Wilk test. The repeated measures ANOVA test was employed to assess the effect of the intervention on the studied outcomes. To assess the robustness of the findings against potential violations of normality, the Friedman test (a nonparametric alternative) was also conducted as a sensitivity analysis for each outcome variable separately. A p value of less than 0.05 was considered statistically significant. All data analyses were performed using IBM SPSS Statistics, version 27.
Results
Of the 203 breastfeeding women assessed for eligibility, 59 did not satisfy the predefined inclusion criteria (one woman aged <18 years, 47 who used bottle feeding, 6 with a chronic medical condition, 3 with preterm birth, and 2 with multiple gestation), and an additional 16 declined to participate. Thus, 128 women were randomly assigned to the intervention (n = 64) or control (n = 64) group. No loss to follow-up occurred; therefore, 64 participants from each group were included in the final analysis (Fig. 1).
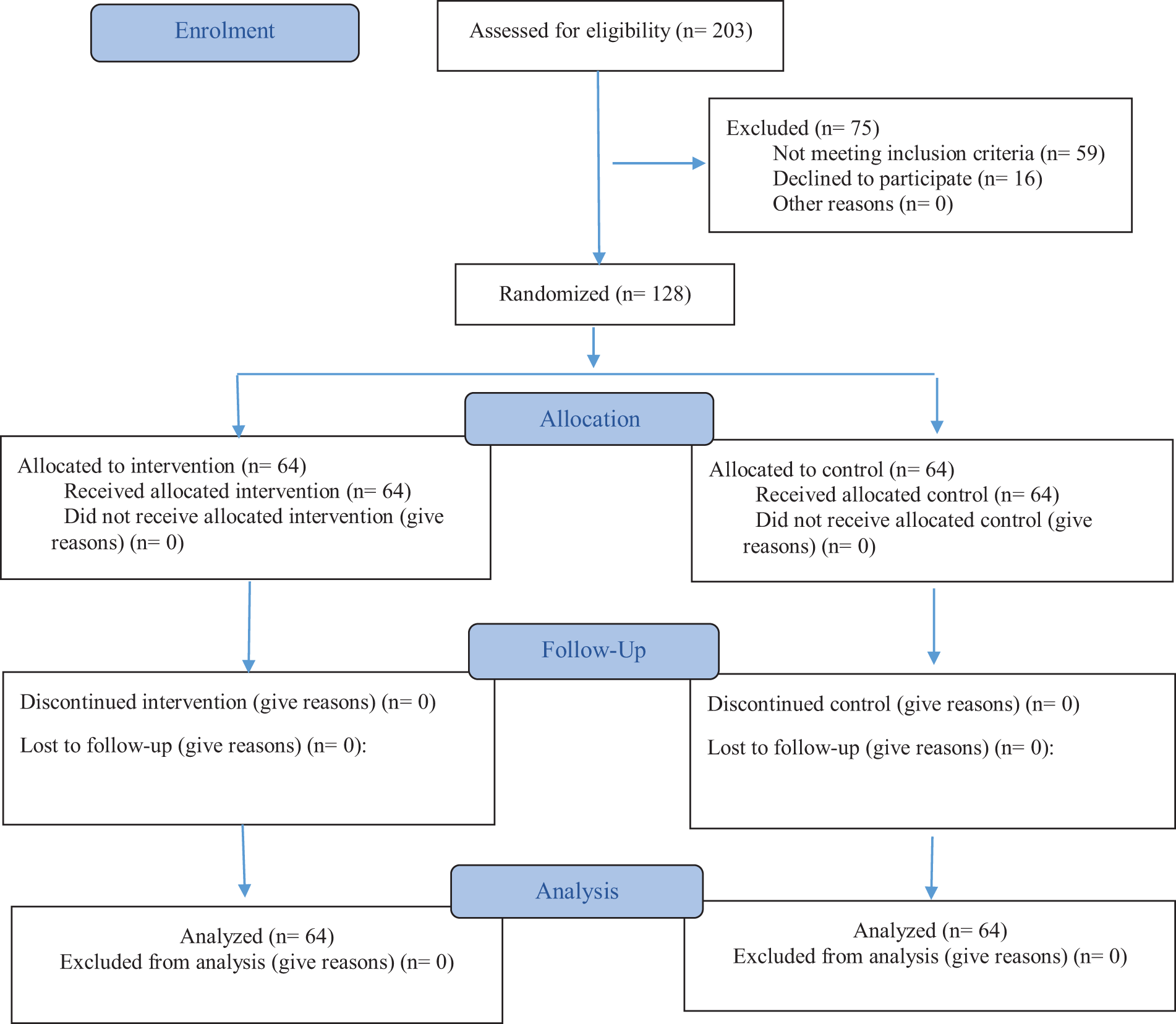
CONsolidated Standards Of Reporting Trials (CONSORT) flow diagram.
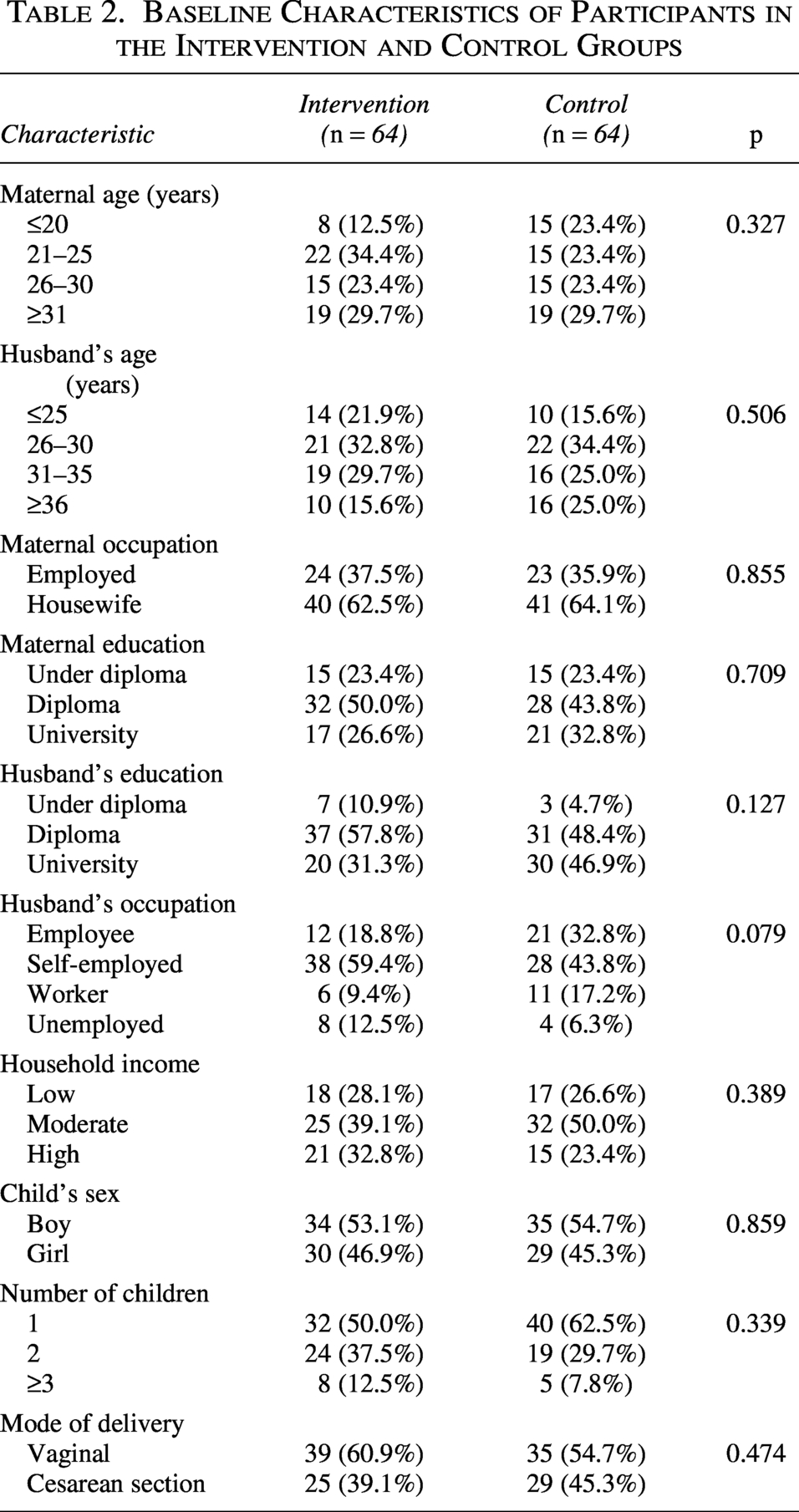
The two groups did not differ in terms of maternal age, husband’s age, maternal and husband’s education and occupation, household income, child’s sex, number of children, or mode of delivery (p > 0.05; Table 2).
Baseline Characteristics of Participants in the Intervention and Control Groups
The results in Table 3 demonstrate a different pattern of maternal distraction and attention during breastfeeding between the intervention and control groups over time. At baseline, the two groups were comparable, with most mothers in both groups reporting moderate-to-high distraction and correspondingly low-to-moderate attention during feeding. Following the intervention, a significant change was observed in the intervention group towards lower distraction and higher attention. By the 4-month follow-up, 98.4% of mothers in the intervention group reported low distraction levels (“Not at all” to “Rarely” distracted), in contrast to only 31.3% of mothers in the control group. Concurrently, the pattern for attention reversed in alignment with this change so that 87.5% of the intervention group reported high attention (“Very high” to “High” attention) at 4 months, compared to 39.0% in the control group.
Distribution of Maternal Distraction and Attention Levels During Breastfeeding Across Follow-up Periods
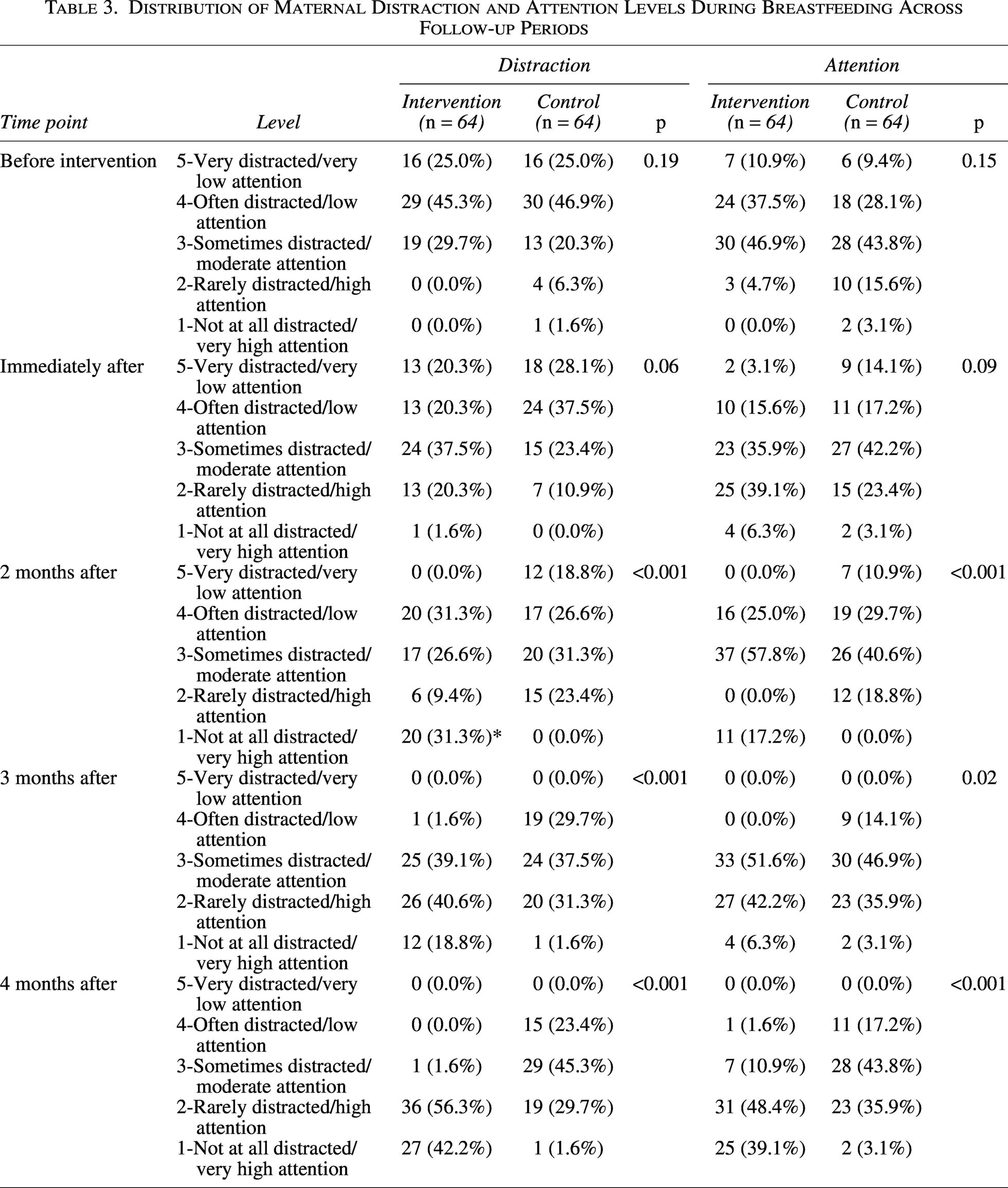
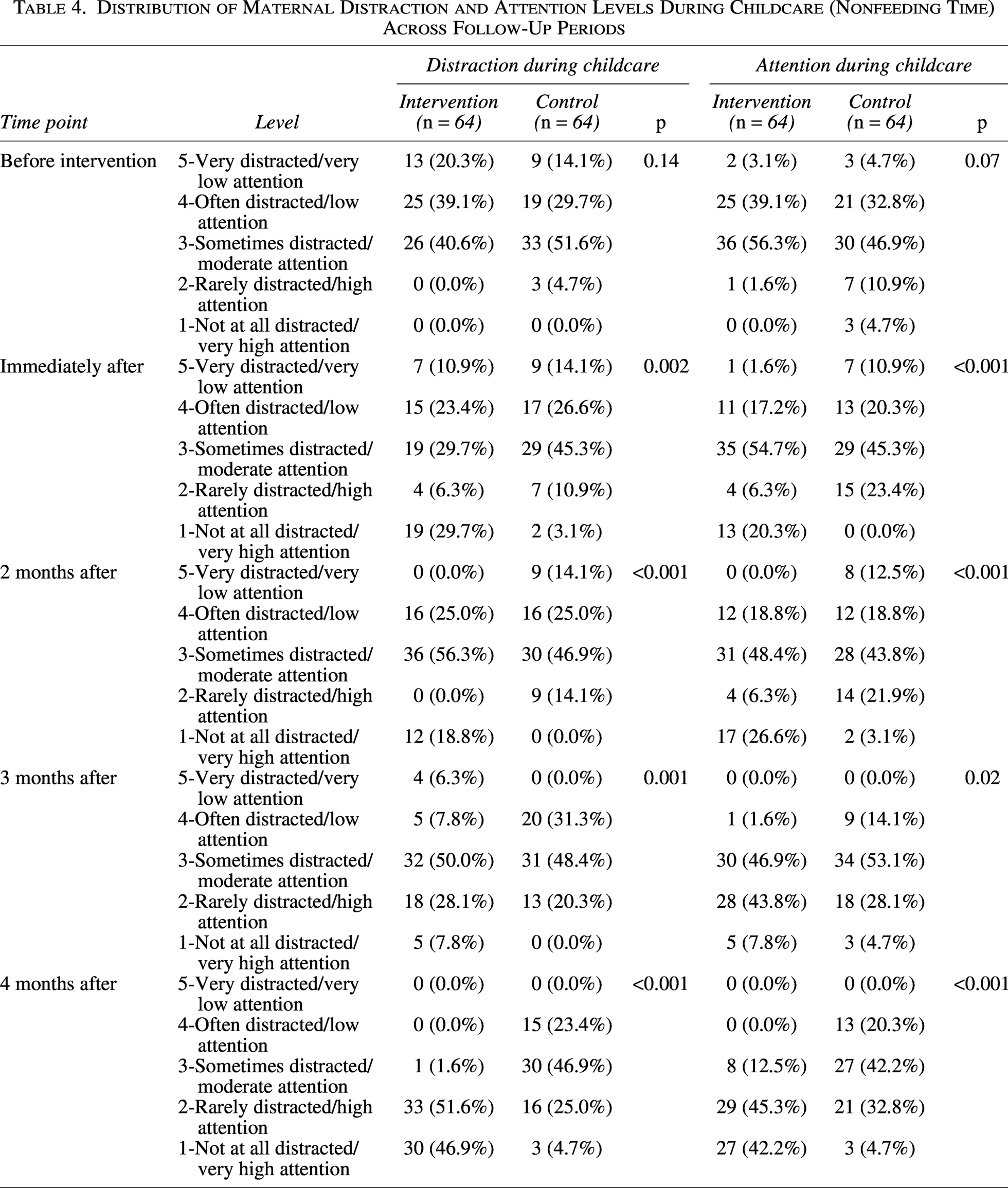
Two groups were comparable in terms of distraction and attention before the intervention phase; however, in the other four phases, the distribution of distraction and attention was significantly different between the two groups. Immediately after the intervention, 29.7% of those in the intervention group reported being “Not at all distracted,” while this figure in the control group was 3.1%. By 4-month follow-up, 46.9% of mothers in the intervention group reported being “not at all distracted”; however, 4.7% of those in the control group reported this level of distraction. Concurrently, by 4-month follow-up, the very high attention in the intervention and control groups was 42.2% and 4.7%, respectively (Table 4).
Distribution of Maternal Distraction and Attention Levels During Childcare (Nonfeeding Time) Across Follow-Up Periods
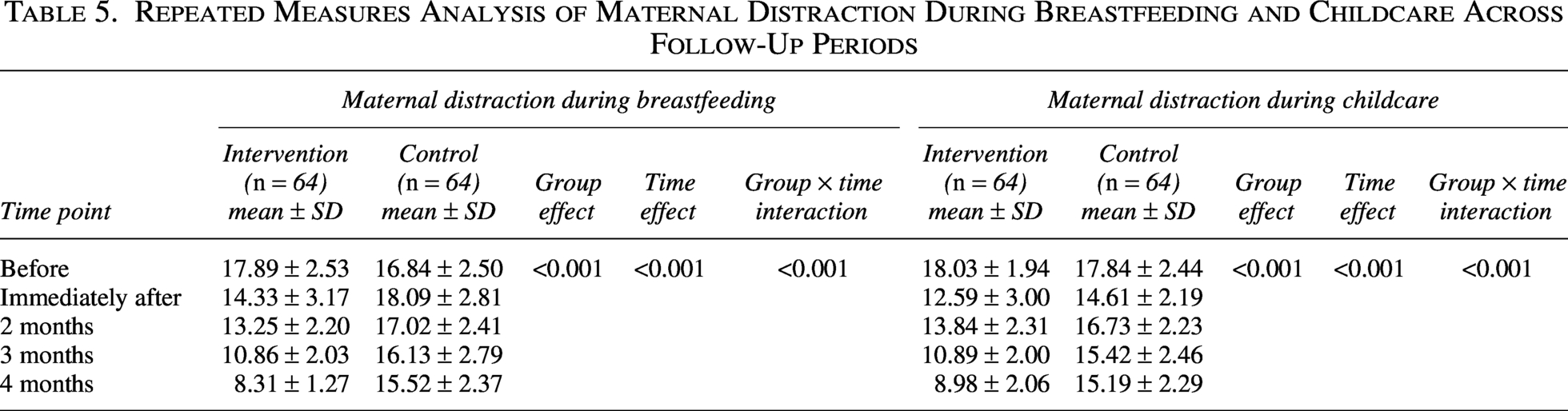
The repeated measures analysis presented in Table 5 provides evidence regarding the effect of intervention on maternal distraction during breastfeeding and childcare. A significant Group × Time interaction (p < 0.001) was found for both breastfeeding and childcare distraction scores, demonstrating that the score of the distraction is a function of the study groups. The intervention group exhibited a linear declined in mean distraction scores from baseline to the 4-month follow-up. The score of maternal distraction during breastfeeding decreased from 17.89 ± 2.53 to 8.31 ± 1.27. Also, the score of maternal distraction during childcare decline from 18.03 ± 1.94 to 8.98 ± 2.06. In contrast, the control group’s scores remained persistently elevated. For breastfeeding, their mean score decreased from 16.84 ± 2.50 to 15.52 ± 2.37, and also there was a modest decline from 17.84 ± 2.44 to 15.19 ± 2.29 for childcare. Although the Shapiro–Wilk test showed some moderate deviations from normality at certain time points, we conducted the Friedman test as a nonparametric sensitivity analysis to verify the robustness of the findings. For maternal distraction during breastfeeding, the Friedman test revealed a significant change over time (χ2 = 229.136, df = 4, p < 0.001), with mean ranks decreasing from 4.02 at baseline to 1.57 at 4 months. For maternal distraction during childcare, the Friedman test also showed a significant change over time (χ2 = 274.776, df = 4, p < 0.001), with mean ranks decreasing from 4.67 at baseline to 1.90 at 4 months.
Repeated Measures Analysis of Maternal Distraction During Breastfeeding and Childcare Across Follow-Up Periods
Discussion
Compared to the control group, the intervention group showed significantly lower distraction and higher attention levels across all follow-up time points. At 4 months, mothers in the intervention group were much less distracted while breastfeeding. Specifically, 40.6% more of them said they were “not at all distracted,” and the rate of those with “very high attention” was 36% higher compared to the other group.
The finding of the present study was in line with another study from Iran that showed structured counseling may be related to improved breastfeeding outcomes. For instance, Azizi et al. 23 have demonstrated that prenatal stress management counseling significantly enhanced maternal self-efficacy and exclusive breastfeeding rates at 4 months postpartum. Similarly, an RCT by Arezi et al. 19 provided evidence for the efficacy of family-oriented counseling in promoting exclusive breastfeeding and reducing maternal distraction. Our study extends this evidence by specifically highlighting the potent role of couple-centered counseling, which yielded an even more substantial reduction in distraction scores. This finding is strongly supported by a recent qualitative meta-synthesis, which synthesized that fathers influence breastfeeding continuity both directly and indirectly, yet they often lack the knowledge, attitude, and practice to participate effectively, which shows why such interventions like couple counseling are needed. 24
The importance of structured, interactive interventions such as education and counseling is further supported by studies conducted in diverse populations. For instance, an RCT among adolescent mothers demonstrated that an education and counseling intervention delivered by a lactation consultant-peer counselor team significantly increased breastfeeding duration. 25 This suggests that actively involving the spouse as a targeted support unit within the family system may be a particularly effective strategy for enhancing maternal distraction and attention. These findings underscore that family-oriented counseling plays a more significant role in supporting maternal breastfeeding and childcare than information-based approaches like Short Message Service (SMS) reminders. 26 The likely mechanisms may involve strengthened spousal support, enhanced parental awareness, and an improved caregiving environment that can address the underlying causes of distraction, whereas passive information delivery does not. The superiority of the interactive approach over passive methods is best understood by considering the nature of the problem. Distraction during feeding, often driven by smartphone use, has been shown to directly impair specific, sensitive maternal behaviors like visual responsiveness to the infant. 27 The critical need for such targeted interventions, for example, couple counseling is further highlighted by recent cross-sectional studies from Iran, which found that the use of smartphones use was reported as the most frequent source of distraction for breastfeeding mothers.21,28 Our findings are consistent with interventions aimed at enhancing the quality of feeding interactions between mothers and infants. For example, an RCT in China evaluating a responsive breastfeeding intervention program demonstrated that such an intervention is associated with increased maternal enjoyment, self-efficacy, and exclusive breastfeeding rates, while also reducing perceived pressure from significant others. 29 Although we evaluated a different method such as counseling couples instead of coaching mothers directly, it seems both interventions work in a similar way. They are likely to contribute to creating a more supportive and less stressful caregiving environment, thereby enabling the mother to devote greater mental capacity to being attentive and responsive during feeding.
This RCT has several limitations. First, the educational nature of the intervention prevented blinding of both participants and counselors, and the reliance on self-administered questionnaires may have introduced measurement bias. Second, the long-term sustainability of the intervention’s effects beyond the 4-month follow-up period remains unknown. Despite these limitations, the novelty of the present study lies in its focus on reducing maternal distraction and increasing maternal attention through structured educational sessions. To the best of our knowledge, studies in this area are very limited, and this study addresses a significant gap in existing literature, which represents a key strength of our research.
Conclusion
This RCT shows that couple counseling intervention may be related to reducing maternal distraction and enhancing attention during both breastfeeding and childcare among mothers experiencing distractions in Hamadan, Iran. These findings highlight the importance of actively engaging the spouse to provide a supportive environment along with practical and emotional support. However, the effect of the couple-centered counseling intervention still needs to be evaluated when integrated with other educational and counseling approaches and over longer follow-up periods.
Authors’ Contributions
E.J., E.A., and S.F.: Conceptualization, methodology, investigation, data curation, writing—original draft preparation, review and editing, and visualization. M.B.A.: Conceptualization, data collection, investigation, data curation, writing—original draft preparation, review and editing, and visualization.
Footnotes
Acknowledgments
During the preparation of this article, the authors used ChatGPT for language editing and grammar improvement. After its use, the authors thoroughly reviewed, verified, and revised all AI-assisted content to ensure accuracy and originality. The authors take full responsibility for the integrity and final content of the published article.
Disclosure Statement
The authors declare no competing interests.
Funding Information
Financial support for this research was provided by Hamadan University of Medical Sciences (Grant No: 140404032867).