
Abstract
Objective:
This study compared weight trajectories in infants breastfed for at least 1 year, with or without formula supplementation.
Study Design:
A retrospective cohort of 252 infants followed in well-baby clinics. All infants were breastfed ≥12 months and received complementary foods at 4–6 months. Of these, 174 received no formula, and 78 received daily formula supplementation. Anthropometric data were collected from birth to 5 years of age.
Results:
Among males, those breastfed without formula had significantly lower body weight between 13 and 18 months compared with those receiving formula (10.20 kg vs. 10.97 kg, p < 0.001). From 19 months onward, no significant weight differences were observed and trajectories converged through 5 years.
Conclusion:
Prolonged breastfeeding in male infants is associated with lower weight in early toddlerhood; however, differences resolve by age two. These findings suggest early variations may represent physiological patterns. Further controlled studies are needed.
Introduction
Breastfeeding is the gold standard for infant nutrition. 1 The American Academy of Pediatrics recommends exclusive breastfeeding for the first 6 months of life, followed by continued breastfeeding as complementary foods are introduced, with continuation of breastfeeding for two years or longer as mutually desired by mother and infant. 2 Breastfed children have long been recognized to display different weight trajectories than formula-fed infants.3,4 Dewey et al. showed that breastfed infants gain weight more rapidly in the first two months and less rapidly from 3 to 12 months when compared to old WHO/CDC growth charts. 3 The DARLING study followed infants from birth to 18 months and found that, while formula-fed infants maintained weight at or above the National Center for Health Statistics median, breastfed infants’ mean weight fell below the median and remained significantly lower between 6 and 18 months. The growth in length was comparable between groups. 4 As a result, and taken together with breastfeeding being the recommended method of feeding for infants, new growth charts based upon breastfed infants were introduced by the WHO in 2006. 5
Breastfeeding has been associated with numerous health benefits, particularly in early infancy, but data on the potential benefits of prolonged breastfeeding remain limited and inconsistent.6,7–11 While the composition of human milk is well-documented in the first 6 months, studies beyond 1–2 years are scarce.12–15
Although numerous studies have compared weight gain in breast- versus formula-fed infants during the first year of life, data on long-term trajectories—particularly beyond 18 months and up to 5 years—are scarce.3–5,10,16–21 A 2017 study found that formula-fed infants experienced more rapid weight and BMI gain during the first 7 months of life compared to breastfed infants, primarily due to increased lean mass rather than fat mass. 18 Most recently, a 2024 study reported higher weight-for-age Z-scores throughout the first year among exclusively breastfed infants compared to those fed with formula. 19 In this study, we aimed to compare weight trajectories among infants who were breastfed exclusively for a prolonged duration while receiving complementary foods beginning at 4–6 months of age, consistent with global feeding guidelines, with those of infants who were breastfed in combination with infant formula, who likewise received complementary foods at 4–6 months. Our hypothesis was that infants breastfed without formula supplementation would exhibit slightly lower weight patterns during the first year of life, but that these differences would normalize thereafter throughout early childhood.
Materials and Methods
Patient population and study design
This retrospective cohort study was based on data from Israeli well-baby clinics, which provide standardized, government-funded preventive health services delivered by a multidisciplinary team consisting primarily of certified nurses and pediatricians. Children are seen at scheduled intervals—monthly during the first 3 months of life, every 3 months until 2 years of age, every 6 months until 3 years of age, and annually thereafter until 5 years of age.
At each visit, the certified nurse conducts anthropometric measurements (weight and length/height) and systematically assesses feeding and sleep habits. The pediatrician performs a structured developmental evaluation, including a formal developmental examination and targeted clinical questioning. When indicated, infants may be referred for further assessment by a lactation consultant.
Between June 2022 and June 2024, parents of eligible children were contacted by telephone and were informed about the study. Parents who provided verbal informed consent participated in a structured telephone interview that collected demographic and clinical information, as well as data on their child’s dietary habits. After completion of the questionnaire, additional clinical, perinatal, and feeding-related data were retrospectively extracted from each child’s electronic medical record. Longitudinal computerized weight measurements were also retrieved from clinic records, covering a follow-up period of at least 2 years and extending up to 5 years of age.
Inclusion criteria were as follows: delivery at term (gestational age [GA] 37–41 weeks); birth weight appropriate for GA, defined as birth weight between the 10th and 90th percentiles 22 ; and initiation of complementary feeding between 4 and 6 months of age, in accordance with international guidelines; breastfed for at least 12 months, regardless of formula supplementation status.
Exclusion criteria included: breastfeeding for <12 months, gestational diabetes mellitus; maternal smoking during pregnancy; preterm (GA < 37 weeks) or postterm (GA > 41 weeks) delivery; birth weight classified as small for GA (SGA) or large for GA; presence of chronic diseases in the infant and any cases of repeated parental reports of difficulties establishing solid food intake.
Feeding patterns were classified into two clearly defined groups:
Breastfeeding without formula supplementation These infants received exclusive breastfeeding for the first 6 months, followed by breastfeeding combined with complementary foods, with no formula supplementation at any time. All the infants received breast milk exclusively through direct breastfeeding, without any supplemental expressed breast milk by bottle. Breastfeeding continued for at least 12 months. After the age of 12 months, transition to whole cow’s milk occurred according to standard national guidelines (typically between 12 and 18 months), and no formula was introduced at any point. Breastfeeding with formula supplementation Infants in this group received breastmilk alongside infant formula. Formula supplementation was defined as daily and consistent exposure to infant formula during the first 12 months of life. Infants who received formula but did not meet this criterion were not included in the study. The duration of supplementation varied among infants, but all had sustained daily formula exposure.
Complementary feeding
In both groups, complementary foods were introduced between 4 and 6 months of age in accordance with international complementary feeding guidelines. By 6 months, infants were expected to establish at least one solid meal per day, progressing to two meals by approximately 7–8 months, and to three meals per day by 9 months of age. As they advanced through infancy and toddlerhood, additional snacks were gradually introduced according to developmental readiness and appetite cues.
Group allocation (breastfeeding without formula vs. breastfeeding with formula supplementation) was determined based on documented feeding patterns extracted from the electronic medical record.
The study was approved by the Institutional Review Board of the Tel Aviv Medical Center (Protocol No. TLV-0308-19). All the recorded data were handled in accordance with the principles of Good Clinical Practice certification. All parents provided verbally informed consent to participate in the study.
Data acquisition
The information retrieved from the electronic medical record and the telephone questionnaire included:
Sociodemographic characteristics: infant’s age and sex, number of people living in the household, number of rooms in the household, maternal years of formal education, number of the infant’s siblings. Perinatal data: birthweight, GA, delivery mode, Apgar scores, perinatal complications. Feeding history: breastfeeding duration, formula use, age of complementary feeding initiation. Maternal history: pregnancy complications, maternal health conditions, restrictive diets, and relevant medication. Anthropometric data: weight-for-age from birth to 5 years were extracted from the electronic medical record.
Statistical analysis
Growth patterns based on weight were evaluated separately for males and females. Weight-for-age Z-scores were calculated monthly according to WHO reference standards. Continuous variables were summarized as means with 95% confidence intervals (CI), and categorical variables as counts and percentages. Group comparisons were conducted using chi-square or Fisher’s exact test, as appropriate.
Sample size calculation indicated that 170 participants (with a 1:3 allocation ratio) were required to detect a 0.5 difference in weight-for-age Z-scores between groups, assuming a two-sided α of 0.05 and a power of 80%.
A p value of <0.05 was considered statistically significant. Given the number of comparisons performed, a Bonferroni correction was applied, yielding an adjusted significance threshold of p < 0.001 (0.05/44). All analyses were performed using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 400 parents to 400 infants were approached for participation. Of these, 133 did not meet the inclusion criteria: 25 due to infant chronic disease, 43 due to SGA weight, and 65 due to insufficient breastfeeding duration. Of the 267 eligible participants, 252 (94.4%) were enrolled in the final analysis; 15 were excluded due to insufficient anthropometric data in the well-baby clinic records Figure 1. Among the final cohort, 252 infants who were breastfed for at least 1 year, 174 infants were breastfed for at least 1 year without formula supplementation (92 males and 82 females) and 78 infants were breastfed for at least 1 year with formula supplementation (40 males and 38 females), which was introduced at the median (IQR) age of 6.00 (4.00, 9.00) months. Table 1 lists the demographics, relevant medical history, and overall diet of the infants and mothers who participated in this study.
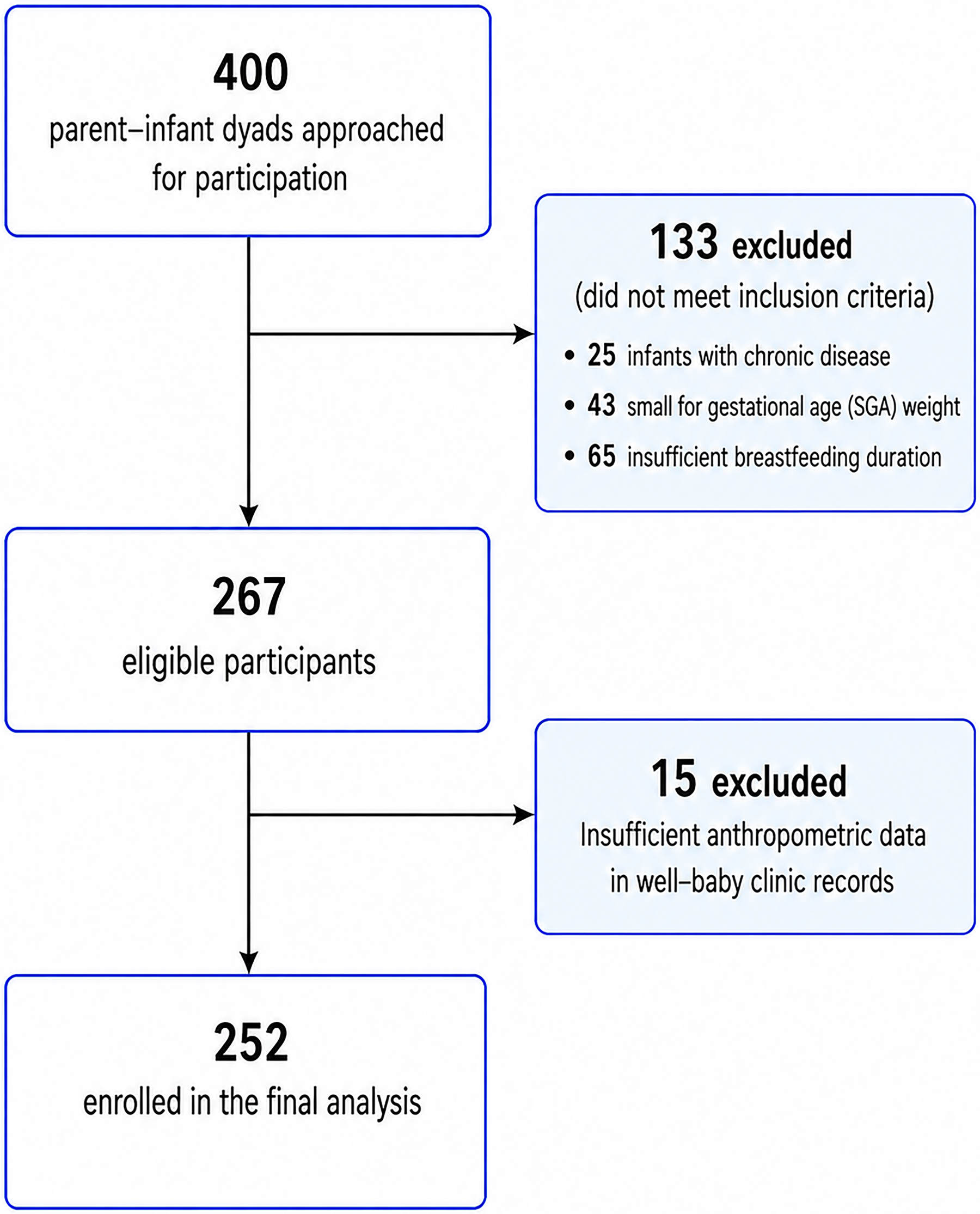
Study participant flowchart diagram.
Demographics, Medical History, and Overall Diet of Infants and Mothers
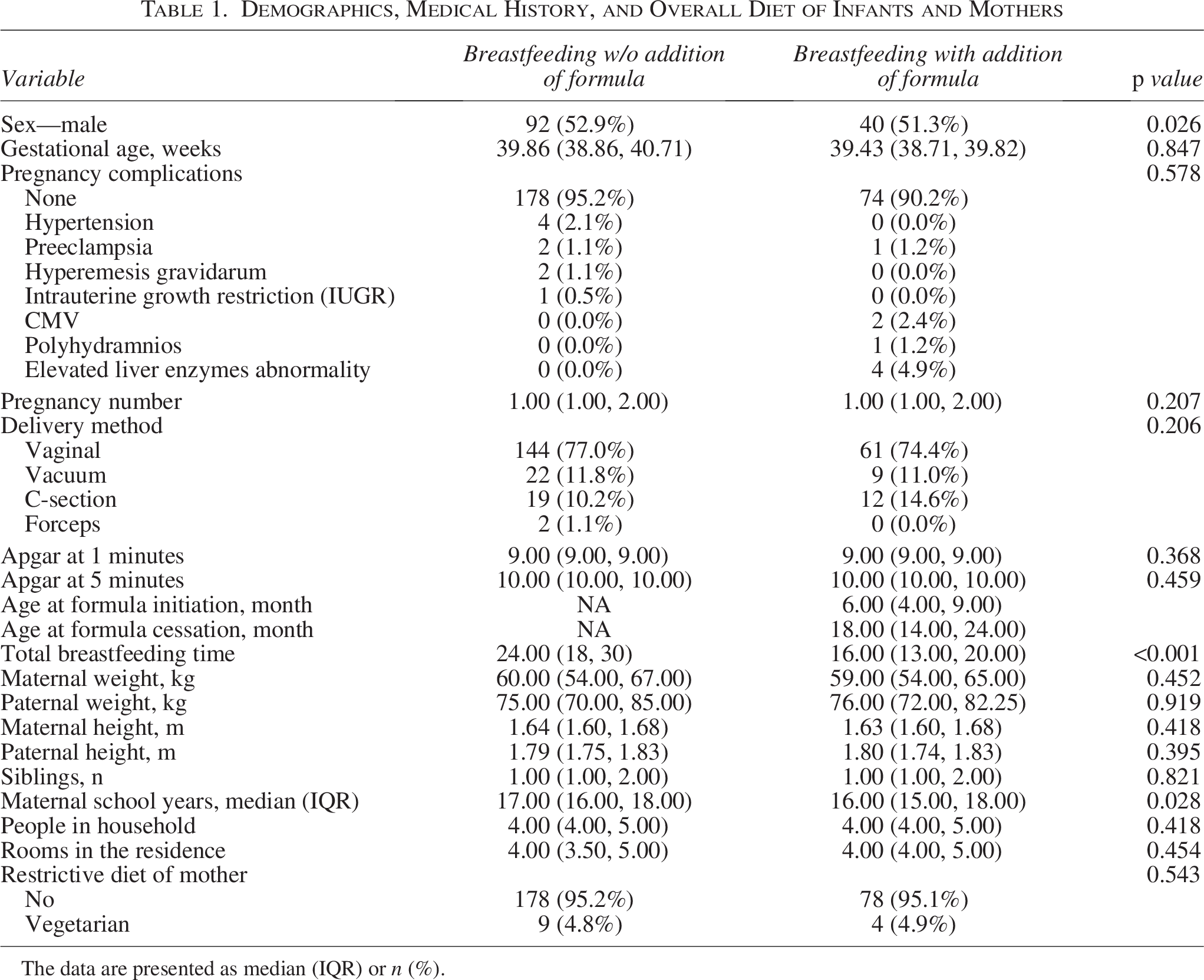
The data are presented as median (IQR) or n (%).
The pregnancy of most participating mothers was free of complications (93.7%), and most were vaginal deliveries (76.2%). The number of years of education was higher among mothers whose infants were breastfed without formula supplementation compared to those whose infants also received formula supplementation (17 [16–18] vs. 16 [15–18], respectively, p = 0.03). No significant difference was found in GA between the groups (39.86 [38.86–40.71] weeks vs. 39.43 [38.71–39.82] weeks, p = 0.847). Importantly, breastfeeding duration was significantly longer among infants who were breastfed without formula supplementation compared to those who also received formula (24 vs. 16 months, p < 0.001). There were no significant differences in the number of pregnancies, maternal/paternal weight, number of siblings, or number of rooms in the house, nor in the Apgar score at 1 minute/5 minute after birth.
Table 2 presents the comparison between breastfed infants with and without formula supplementation in periodic measures conducted from birth until 60 months of age. No significant difference was found in the body weight between infants with and those without formula supplementation from birth up to 12 months old. However, between 13 and 18 months, the median body weight of the male infants without formula supplementation was significantly lower compared to the median weight of the male infants with formula supplementation (10.20 kg [9.46–11.00] vs. 10.97 kg [10.35–11.90], Z score −0.276 [−1.018, 0.340] vs. 0.436 [−0.402, 0.845] respectively, p < 0.001). Importantly, these findings were remained significant after Bonferroni correction was applied (p < 0.001). There was a similar trend among female infants, but it did not reach a level of significance (9.765 kg [9.284–10.70] vs. 10.30 kg [9.52–11.00], Z score 0.100 [−0.490, 0.490] vs. 0.287 [−0.255, 0.917], p = 0.08). There were no significant group differences in body weight from 19 months of age onward.
Comparison of Weight Gain of Breastfed Infants with and without Formula Supplementation
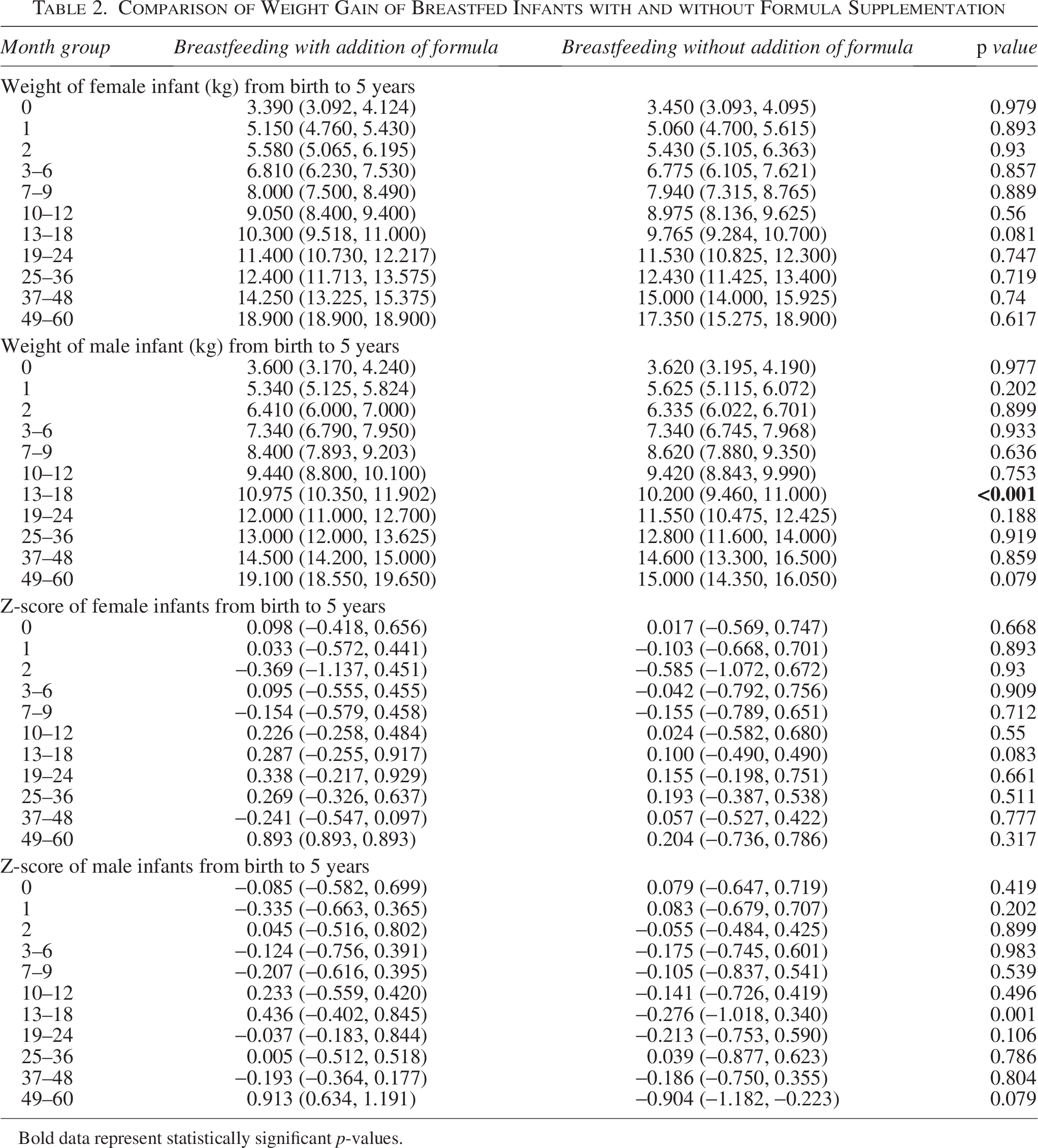
Bold data represent statistically significant p-values.
The body weight curves of breastfed infants with and without formula supplementation over time are presented in Figure 2 and 3. The curves for males and females from birth to 5 years of age are depicted in percentiles and Z-scores (Fig. 2a–2d). The curves for males and females from birth to 12 months of age are also shown in percentiles and Z-scores (Fig. 3a–3d).
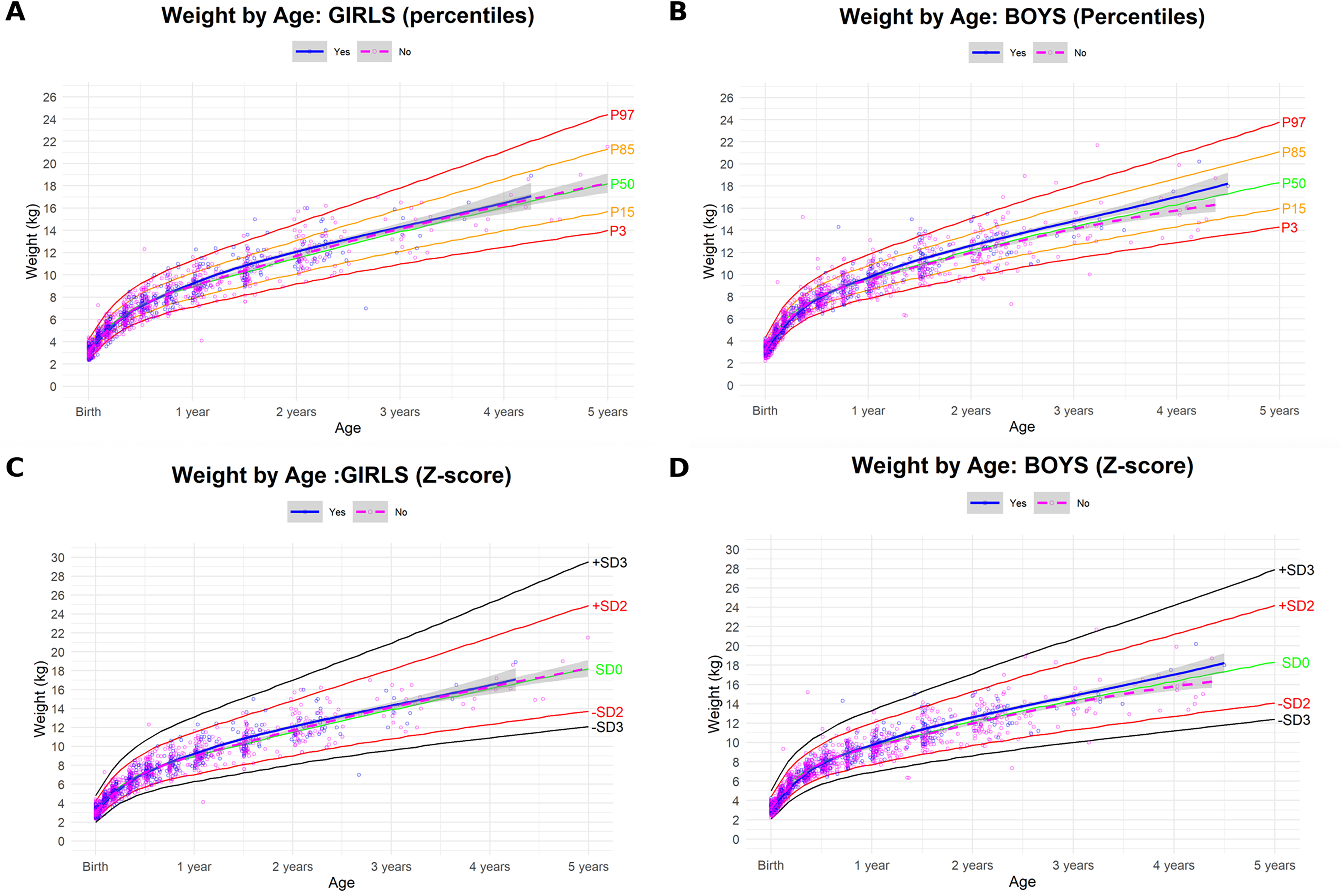
Weight-for-age curves of breastfed infants with and without addition of formula, from birth to 5 years.
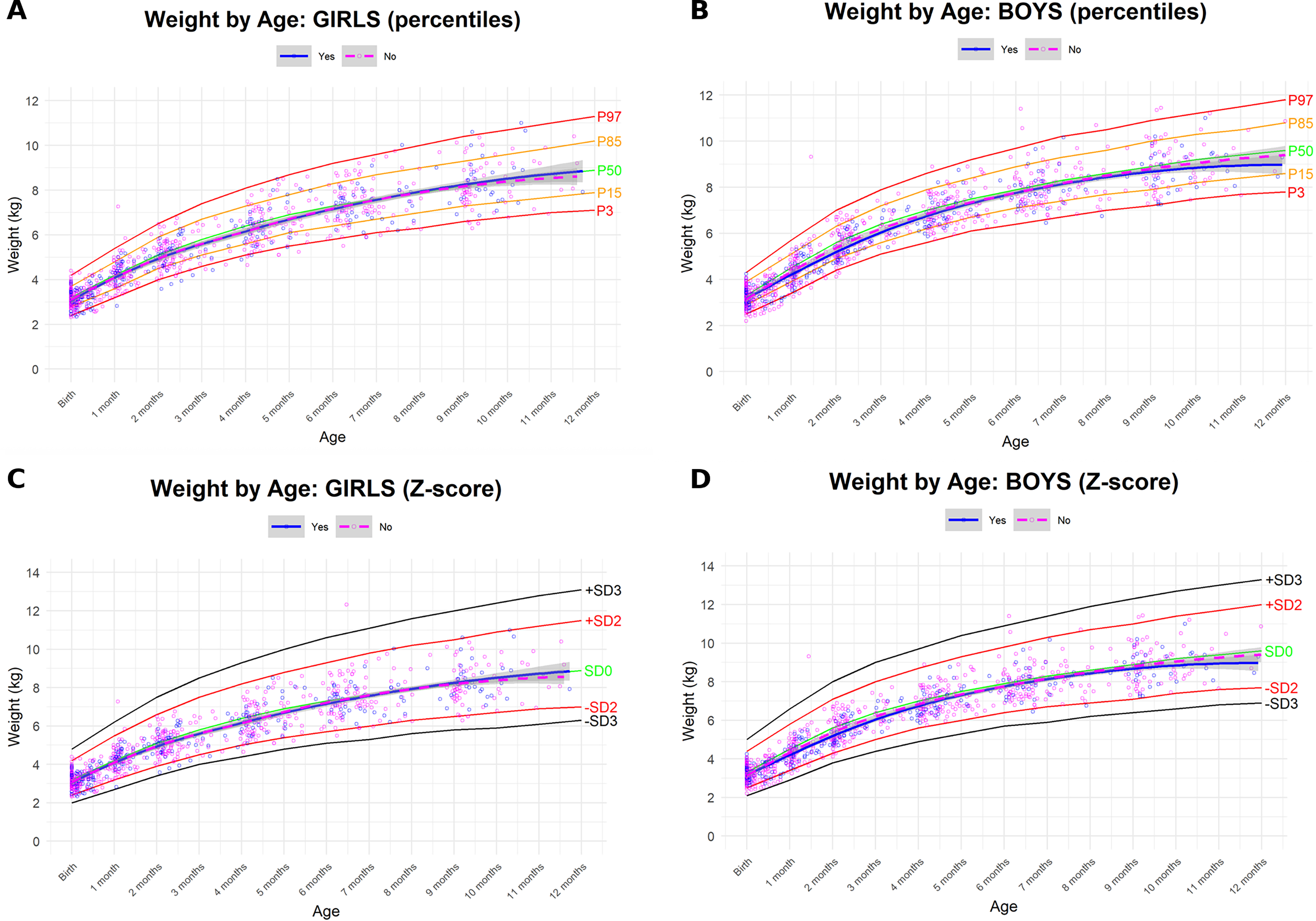
Weight-for-age curves of breastfed infants with and without addition of formula, from birth to 1 year.
Discussion
The influence of formula supplementation to the weight trajectories of infants who are breastfed for 1 year or more has not been investigated in depth. The finding of the current study supported our hypothesis that infants who are breastfed for a prolonged time without the addition of formula exhibited slower weight gain than formula-supplemented breastfed infants, especially among males, and that the gap tended to be reduced by the age of 2 years and no significant differences persisted through early childhood.
Several studies have shown that breastfed infants may gain weight more rapidly in the first 2–3 months, but thereafter, formula-fed infants tend to gain weight at a faster rate, resulting in higher mean weights for formula-fed infants from around 4–6 months onward.3,4,21 There may be several reasons why the weight increase rate of exclusively breastfed infants is slower compared to formula-fed infants. First, breastfed infants can self-regulate their milk intake. Breastfeeding, when delivered directly from the breast, allows infants to learn to regulate their energy intake based upon internal cues of hunger and satiety, in contrast to formula bottle-feeding, which may encourage overfeeding.23–25 Since parents can visually monitor the amount of milk remaining in a bottle, they may be more likely to encourage the infant to finish the entire quantity, even if the infant is already satiated. In contrast, during breastfeeding, the mother cannot precisely measure the amount of milk consumed, allowing the infant’s intake to be naturally adjusted to their physiological hunger needs.23–25 Additionally, the dynamic composition of breast milk may contribute to the slower rate of body weight observed in exclusively breastfed infants compared to exclusively formula-fed infants. It is well established that the composition of breast milk changes over time.12–14,26,27 This factor may also play a role in the differences observed between the weight-gaining curves of breastfed and formula-fed infants, since formula maintains a fixed composition that does not adjust to the infant’s changing requirements while breast milk does. Furthermore, the distinct nutritional composition of infant formula may also contribute to greater weight gain in formula-supplemented infants, in addition to feeding mode. 28
In the present study, no significant weight differences were observed between the groups during the first 12 months of life. This is consistent with the fact that all infants were exclusively breastfed until a median age of 6 months, precluding any feeding-related differences in early infancy. Previous observations have shown that weight differences between breastfed and formula-fed infants tend to emerge and consolidate over time, 4 suggesting that the lack of difference between 6 and 12 months may reflect a developmental window during which the cumulative effects of early milk nutrition have yet to fully manifest in growth trajectories. Of note, as both groups in the present study received breast milk, the between-group feeding differences were more subtle than in studies comparing exclusive breastfeeding with exclusive formula feeding, which may have further contributed to the delayed emergence of weight differences.
Our second hypothesis, suggesting that the weight difference between groups would diminish before the age of 2 years, was also supported. Among males, no significant difference between the groups was observed from 19 months of age onward. This pattern appeared to persist up to the age of 5 years. These findings may indicate that, in cases of mild weight maintenance decline, and under appropriate medical supervision ensuring adequate intake and absence of malabsorption, additional nutritional supplementation might not be necessary.
The observed sex-specific difference in weight trajectories may reflect a sexually dimorphic response to infant feeding mode. Cheng et al. demonstrated that boys showed a greater response to feeding mode than girls in terms of linear growth during infancy, suggesting that male infants may be more sensitive to differences in nutritional intake. 29 This greater sensitivity in males may similarly account for the significant weight difference observed between groups in male but not female infants in the present study, though further investigation is warranted.
Importantly, several studies, including the present study, have shown that the introduction of formula to infants who are breastfed is associated with shorter breastfeeding duration.30–34 Beyond the known benefits of breastfeeding and breast milk, exclusive breastfeeding was found to have advantages over combined breastfeeding and formula. Observational studies have also reported that infants exclusively breastfed exhibit lower incidences of lower respiratory tract infections in infancy and reduced risks of asthma and allergic rhinitis in childhood.35,36Although reverse causation cannot be excluded in observational designs, these longitudinal, real-world data can aid clinicians and parents in making informed, evidence-based decisions about infant feeding that fully consider both its benefits and potential drawbacks.
While our study showed that breastfed infants without formula supplementation attained median weights comparable to those of breastfed infants with supplemental formula by two years of age, those receiving formula demonstrated a steeper early weight‐gain trajectory. Accelerated weight gain during infancy has been linked prospectively to later overweight and obesity across varied settings and birth‐weight categories.20,37–42 Notably, however, the largest randomized promotion of breastfeeding study—the PROBIT trial—did not demonstrate a reduction in overweight or obesity at 6.5 years among children whose mothers received the intervention. 43
The contribution of the current study is the characterization and understanding of the weight patterns of breastfed infants over a prolonged period. The direct comparison of infants’ weight with and without the addition of formulas can help guide pediatricians in clinical decision-making. The current findings expand previous literature on breastfed infants’ weight gain by monitoring them for up to the age of 5 years.
This study has several limitations that should be acknowledged. First, its retrospective design inherently limits the ability to collect detailed quantitative information regarding the exact amounts of infant formula consumed, and infants with varying levels of formula supplementation were grouped together. Moreover, individual maternal milk production was not measured, as this is not routinely assessed in clinical practice. Nevertheless, as all infants were followed in well-baby clinics with standardized and frequent weight monitoring, cases of inadequate growth due to insufficient milk supply would likely have been identified and managed clinically, thereby reducing, to some extent, the likelihood that such cases remained in the breastfeeding-only group. Furthermore, as the feeding history data were collected via parental recall, recall bias cannot be excluded. However, previous studies have demonstrated that maternal recall of breastfeeding duration and practices is valid and reliable, even years after childbirth.44–45 Additionally, where available, parental recall data were cross-referenced with documented records in the electronic medical record.
In conclusion, the findings of the present study demonstrated that the weight gain of male infants who were breastfed for at least 1 year alongside complementary feed introduction was significantly lower than that of breastfed male infants who received formula supplementation between 13 and 18 months. A similar trend was observed among female infants. No significant differences in weight gain were observed between the two groups after 18 months, and this trend persisted up to 5 years. If confirmed in additional prospective studies, these findings could assist in making better-informed nutritional decisions for breastfed infants.
Authors’ Contributions
R.K.D. and R.L. contributed equally to the study conceptualization and design, developed the methodology, and performed data collection and curation. H.M.L. performed the formal statistical analyses, led the interpretation of the results, and drafted the original article. D.M. contributed to interpretation of the findings, and critically revised the article for important intellectual content. All authors participated in writing—review and editing of the article, approved the final version for submission, and agree to be accountable for all aspects of the work.
Ethical Approval
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Helsinki ethics committee. Verbal informed consent was obtained from all parents.
Footnotes
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
No funding was received.