
Abstract
Background:
Breastfeeding has been shown to reduce the risk of several diseases—including those that disproportionately affect Black or African American women and children. Adverse social determinants of health (SDOH) have been associated with a higher prevalence of postpartum depressive symptoms and are negatively associated with breastfeeding outcomes and the timing of solid food introduction. Prior research has focused on each individual SDOH in isolation and has not, to the best of our knowledge, examined the mediating role of depressive symptoms and timing of introduction to solid foods.
Objective:
This study aimed to examine (1) the association between multiple adverse SDOH and timing of breastfeeding cessation and (2) if this relationship is mediated by maternal depressive symptoms and the timing of introduction to solid food.
Materials and Methods:
This secondary data analysis used data from an existing, longitudinal birth cohort study with Black or African American women (n = 242). Multivariable logistic regression and regression-based causal mediation analyses were used to address the objectives of this study.
Results:
Findings showed multiple adverse SDOH were associated with increased odds of stopping breastfeeding at 4 and 6 months of age (4 months: odds ratio [OR] = 3.49, 95% confidence interval [CI]: 1.11, 10.97; 6 months: OR = 5.03, 95% CI: 1.54, 16.47). This relationship was partially mediated by the introduction of solid foods at 4 months of age (indirect effect: OR = 1.53, 95% CI = 1.18, 2.34) but not mediated by maternal depressive symptoms.
Conclusions:
Multiple adverse SDOH demonstrated relationships with the timing of both breastfeeding cessation and introduction to solid foods.
Introduction
Breastfeeding has been associated with several health advantages—including a reduced risk of diseases, such as cardiovascular disease (CVD) 1 and asthma. 2 CVD and asthma disproportionately affect Black or African American women and children.3,4 In the United States, breastfeeding initiation rates are the lowest (74.5%) among Black or African American mother–infant dyads. 5 Other racial subgroups below the national prevalence rate (84.0%) include American Indian or Alaskan Native (77.7%) and Other Pacific Islanders (79.4%). 5 Breastfeeding initiation rates for Asian (90.1%) and White (85.9%) racial subgroupings exhibited among the highest rates and were both above the national prevalence rate. 5 Similarly, duration rates of breastfeeding at 3 and 6 months of age were lower among Black infants (3 months: 58.0%; 6 months: 44.7%) compared with White infants (3 months: 72.7%; 6 months: 62.0%), respectively. 6
Social determinants of health (SDOH) are defined as “the conditions in the environment in which people are born, live, learn, work, play, worship, and age” that influence quality of life and health outcomes. 7 Adverse SDOH, such as lower levels of income or maternal education, have been negatively associated with breastfeeding outcomes 8 and with the introduction of solid food prior to 4 months of age.9,10 The American Academy of Pediatrics (AAP) and the Centers for Disease Control and Prevention (CDC) recommend introducing solid foods at approximately 6 months of age, which aligns with the recommendation for approximately 6 months of exclusive breastfeeding.11,12 In the Early Childhood Nutrition Report, the CDC additionally deemed the introduction of solid foods before 4 months as “too early.” 11 The AAP recommendations also acknowledged that many families introduce solid foods around 3–4 months of age. 12
Black or African American dyads exhibited higher rates of adverse SDOH and prevalence of “early” introduction to solid foods.13–15 Recent research guided by Restoring Our Own Through Transformation, a theoretical framework designed to identify the structural and SDOH relating to maternal-infant health inequities, corroborated key SDOH, such as education level and current living situation (e.g., housing) as influential for maternal-infant health.13–16 A study using U.S. National Survey of Children’s Health data identified an increased prevalence of “early” introduction to solid foods among Black children (overall prevalence: 10.7%; Black children: 21.0%). 15 Adverse SDOH, such as lower levels of education or living at or below the federal poverty level (FPL), have also been associated with a higher prevalence of postpartum depressive symptoms.17,18 Differences in the prevalence of postpartum depressive symptoms or diagnosis among Black or African American women vary across studies. A 2025 study using Pregnancy Risk Assessment Monitoring System data found Black women were more likely to experience postpartum depressive symptoms. 19 Whereas, a 2024 study did not find significant differences in the diagnosis of perinatal mood and anxiety disorders (PMAD) across racial or ethnic subgroups. 20
Existing research examining the association between adverse SDOH and breastfeeding outcomes has predominantly focused on each individual SDOH in isolation8,21–23 and, to the best of our knowledge, has not yet examined if this relationship is mediated by maternal depressive symptoms and the timing of introduction to solid foods. Given Black or African American mother–infant dyads exhibit among the lowest rates of U.S. breastfeeding initiation and duration5,6 and demonstrate among the highest prevalence of health conditions known to have a reduced risk among breastfeeding dyads,1,2 this study aims to (1) examine the association between multiple adverse SDOH and breastfeeding duration among Black or African American women and (2) determine if the association between multiple adverse SDOH and breastfeeding duration is mediated by the timing of introduction to solid foods and maternal depressive symptoms within this critically important population.
Methods
Data source and participants
This secondary data analysis used data from the Infant Growth and Microbiome (IGRAM) Study, a prospective, longitudinal birth cohort study of 300 Black or African American women and their infants. 24 Women with normal weight (body mass index [BMI] between 18.5 and 24.9 kg/m2) and obesity (BMI equal to or greater than 30.0 kg/m2) were included in the IGRAM study. The main exclusion criteria for infants in the IGRAM study included delivery at a hospital outside of the study area, premature birth, intrauterine growth restriction at less than the fifth percentile, chromosomal abnormality, or significant illness known to impact growth and development. 24 A more detailed description of the parent study can be found in Benitez et al. 24 In the present analysis, participants who did not provide information on breastfeeding practices were also excluded. Of the 300 participants in the full cohort, a subsample of 242 mother–infant dyads had breastfeeding data and consented to secondary analysis of their data. Written informed consent was obtained from all participants. This study was approved by the Institutional Review Boards (IRB) of the University of Pennsylvania and the Children’s Hospital of Philadelphia (CHOP).
Social determinants of health
The approach used by Javed et al. 25 informed the operationalization of the exposure variables. Each individual SDOH was dichotomized into adverse (assigned a value of “1”) or favorable (assigned a value of “0”) (Table 1). All SDOH exposure variables were collapsed into two categories: “One or no adverse SDOH (≤1 SDOH)” was assigned a value of “0,” and “Two or more adverse SDOH (≥2 SDOH)” was assigned a value of “1.” A minimum threshold of at least two or more was used to define the term “multiple” in this study.
Operationalization of Social Determinants of Health Variables
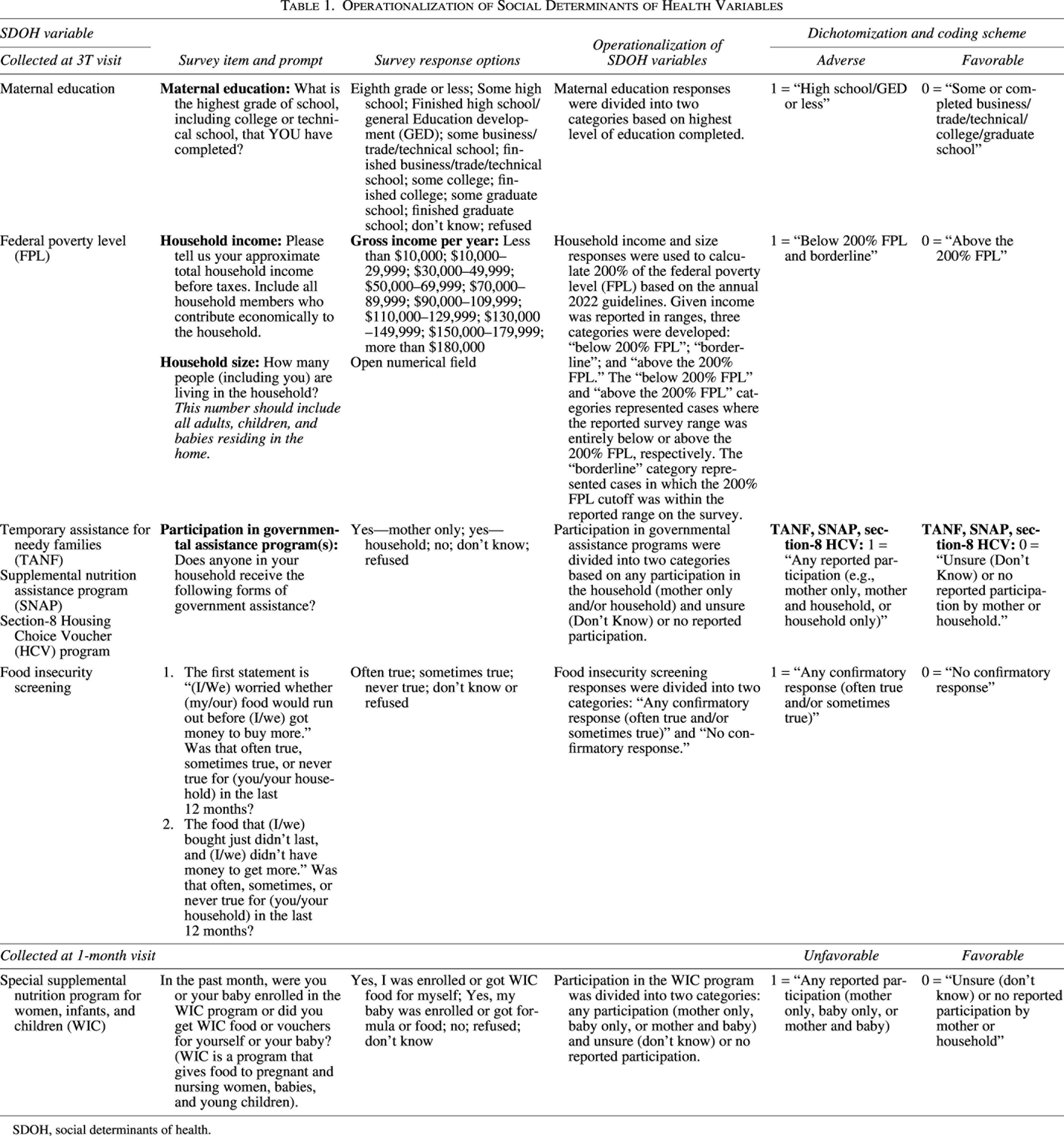
SDOH, social determinants of health.
Breastfeeding duration
Data on infant feeding practices (e.g., breastfeeding duration) included survey prompts to address when breastfeeding or pumping was completely stopped. To capture the duration of any breastfeeding for the first 12 months of life, measured in days, a new variable was created. This variable was then converted into months and dichotomized into still offering any breast milk/breastfeeding (“0”) and stopped offering any breast milk/not breastfeeding (“1”) at 4 and 6 months of age. These timepoints were selected based on national recommendations and common practices of solid food introduction.11,12
Timing of introduction to solid foods
Data on the introduction to solid foods included questions to address the first time the infant was introduced to solid foods and the frequency of adding cereal or baby food to the bottle. A new variable was created to capture the first introduction to solid foods, regardless of the feeding vessel (e.g., via a spoon, cereal in a bottle). Variables were dichotomized, and “early” introduction to solid foods was defined as at or before 3 months of age and at or before 4 months of age (assigned a value of “1”).
Maternal depression
Maternal depressive symptoms were measured using the 20-item Center for Epidemiology Studies—Depression Scale (CES-D) at the third trimester (3T), 2-month, 6-month, and 12-month visits. 26 The CES-D is designed to screen for depressive symptoms, such as feelings of guilt and worthlessness or depressed mood. 26 The screening tool is not diagnostic; however, scores of 16 or greater have been used as a cut-off score to identify individuals at a higher risk for clinical depression. 26 To examine if maternal depressive symptoms measured at 2 months postpartum served as a mediating variable, the CES-D score was used as a continuous variable.
Covariates
Covariate selection included variables within the IGRAM dataset with an established association with the variables (exposure, outcome, and mediator) used in this study.21,22,27–30 These variables included: birth delivery mode (e.g., cesarean section), maternal age, parity (primiparous), BMI (equal to or greater than 30 kg/m2), smoking status (e.g., smoker), and Medicaid enrollment status, measured via self-report.
Statistical analysis
Descriptive statistics were used to summarize and describe the sample characteristics. Multicollinearity was examined using variance inflation factor calculations for all independent variables (exposure and covariate). All values were below 1.5, indicating that multicollinearity was negligible. Missing data across the outcome, mediator, and independent variables ranged from 0.83% to 4.04%. Bivariate analyses, using Fisher’s exact tests for binary variables and t tests for continuous variables, found no statistically significant associations. All covariates were included due to their potential confounding effects, supported by the established literature. 31
For all analyses, statistical significance was defined as an alpha level of ≤0.05. Descriptive statistics and complete-case multivariable regression analyses were conducted using SAS software (Version 9.4; Copyright 2025 SAS Institute Inc.). All sensitivity analyses using multiple imputation by chained equations (MICE) were conducted using R Studio (Version 2025.5.1.513; Posit Software 2025, PBC, Boston, MA). 32 The mediation analyses were performed using the CMAverse package in RStudio software (Version 2025.5.1.513; Posit Software 2025, PBC, Boston, MA). 33
In this secondary data analysis, missing data were addressed using two methods: complete case analysis (n = 213) and, as a sensitivity analysis, MICE (number of imputations = 10). 32 Multivariable logistic regression analyses were then performed to examine the relationship between breastfeeding cessation measured at 4 and 6 months of age (outcome) and adverse SDOH measured during pregnancy and the first month postpartum (exposure), adjusted for all covariates (Aim 1). To determine if symptoms of maternal depression and the ‘early’ introduction of solid foods were potential mediating variables, a regression-based causal mediation analysis was used (Aim 2).34,35
Sensitivity analysis
MICE was employed for all variables (e.g., outcome, exposure, mediator, and covariates). Multivariable logistic regression analyses were then performed to examine the relationships between variables in Aims 1 and 2. Confidence interval (CI) estimation was based on 1,000 bootstrap analysis iterations.
Exploratory analysis
Exploratory analyses were conducted to examine the individual contribution, or the salience, of each adverse SDOH to breastfeeding cessation. Multiple logistic regression models, utilizing both complete case analysis and multiple imputation, were employed. Results were reported in the log odds scale and converted to the odds ratio (OR) scale.
Results
Sample description
Participants engaged in any breastfeeding for an average of 148.8 ± 204 days (median: 57.5 days). Table 2 presents the demographic characteristics of the sample. Table 3 shows the distribution of adverse SDOH among the sample.
Participants Characteristics, n = 242
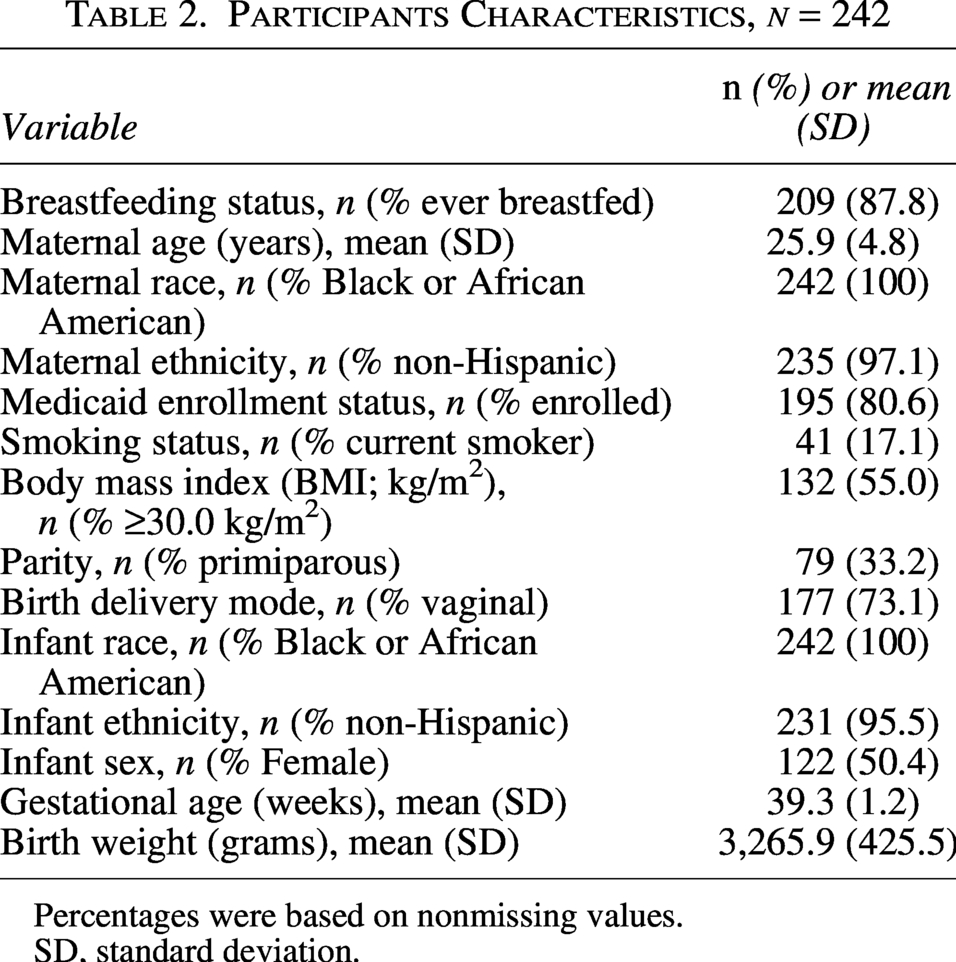
Percentages were based on nonmissing values.
SD, standard deviation.
Percent of Sample with Adverse Social Determinants of Health, n = 242
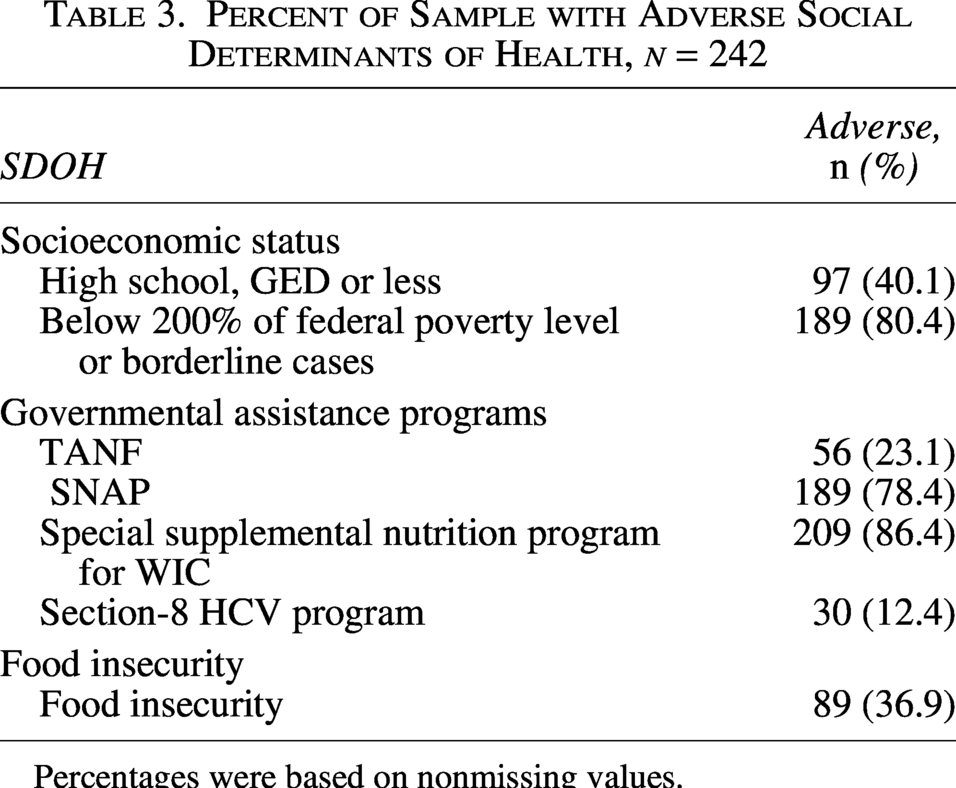
Percentages were based on nonmissing values.
Odds of stopping any breastfeeding
Approximately two-thirds of the sample (n = 160) and three-fourths of the sample (n = 178) stopped breastfeeding at 4 and 6 months of age, respectively. A total of 29 participants reported never breastfeeding. After adjusting for all covariates, the odds of breastfeeding cessation at 4 and 6 months of age were significantly higher among women with ≥2 SDOH compared with women with ≤1 SDOH (4 months: OR = 3.49, 95% CI: 1.11, 10.97; 6 months: OR = 5.03, 95% CI: 1.54, 16.47) (Table 4). Similar estimates were observed in the sensitivity analysis, which utilized MICE (4 months: OR = 3.38, 95% CI: 1.07, 10.68; 6 months: OR = 4.81, 95% CI: 1.46, 15.87).
Adjusted Logistic Regression Estimates Between Adverse Social Determinants of Health and Breastfeeding Cessation in the IGRAM Study, n = 213
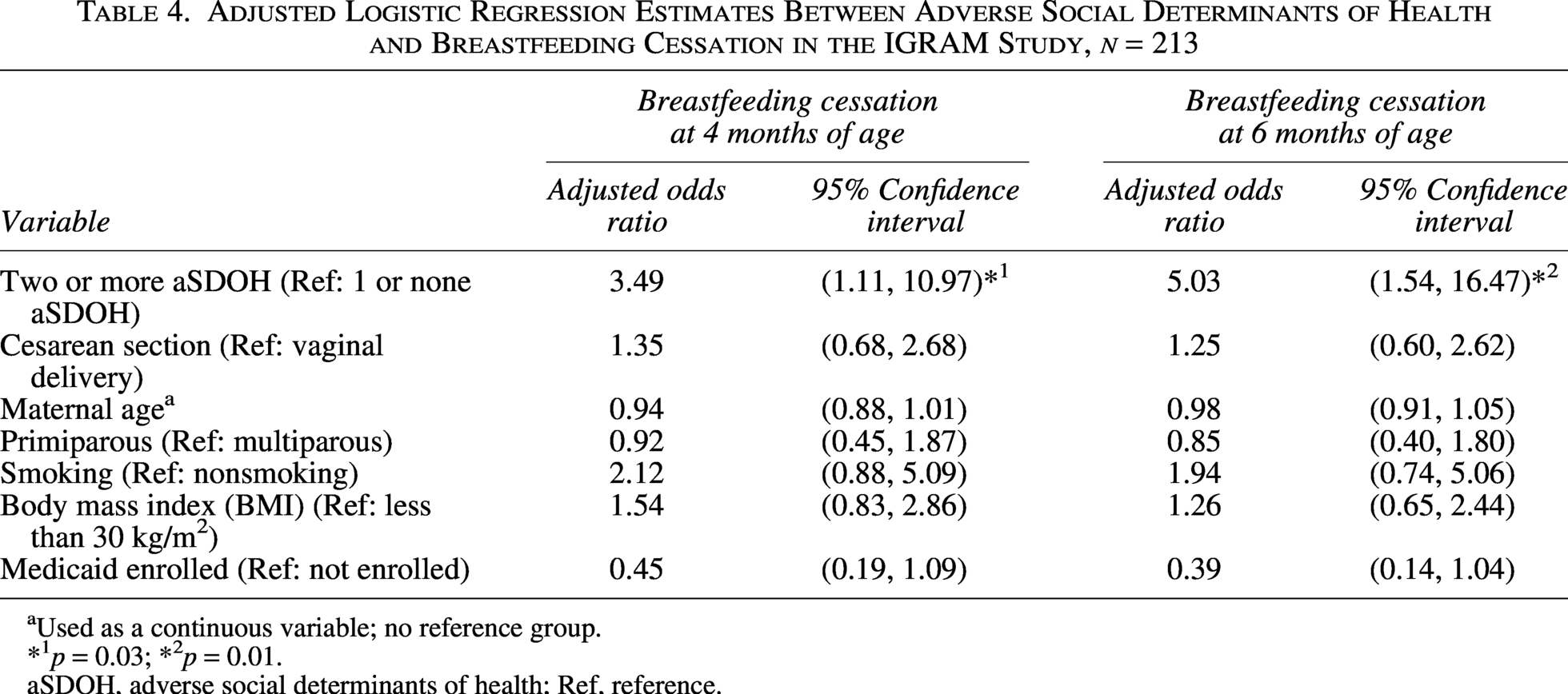
Used as a continuous variable; no reference group.
*1p = 0.03; *2p = 0.01.
aSDOH, adverse social determinants of health; Ref, reference.
Salience of adverse SDOH
In exploratory analyses, the odds of stopping breastfeeding at 4 and 6 months of age were significantly higher among participants who self-reported participation (mother, infant, or both) in the Special Program for Women, Infants, and Children (WIC) program at 1 month of age compared with those who did not (4 months: OR = 3.00, 95% CI: 1.27, 7.10; 6 months: OR = 2.96, 95% CI: 1.22, 7.21) and among women with a high school or general education development (GED) education or less as compared with those with higher education (4 months: OR = 2.33, 95% CI: 1.21, 4.51; 6 months: OR = 3.24, 95% CI: 1.52, 6.87). In the multiple imputation sensitivity analysis, the odds of stopping breastfeeding at 4 and 6 months of age were significantly higher among participants who self-reported participation in the WIC program at 1 month of age as compared to those who did not (4 months: OR = 3.11, 95% CI: 1.30, 7.41; 6 months: OR = 3.23, 95% CI: 1.32, 7.89) and among women with a high school (or GED) education or less as compared with those with higher education (4 months: OR = 2.12, 95% CI: 1.11, 4.03; 6 months: OR = 2.77, 95% CI: 1.33, 5.74).
Maternal depressive symptoms
Less than one-fifth (18.7%) of the present sample had CES-D scores of 16 or higher. In adjusted mediation models, maternal depressive symptoms measured at 2 months postpartum were not found to mediate the relationship between multiple adverse SDOH and breastfeeding cessation at 4 or 6 months of age (women with ≥2 SDOH compared with women with ≤1 SDOH; 4 months: OR = 1.01, 95% CI: 0.84, 1.26; 6 months: OR = 0.94, 95% CI: 0.77, 1.19) (Table 5). Similar results were observed in the multiple imputation models (sensitivity analyses) (4 months: OR = 1.01, 95% CI: 0.84, 1.27; 6 months: OR = 0.94, 95% CI: 0.77, 1.20).
Adjusted Mediation of Early Introduction to Solid Foods and Maternal Postpartum Depressive Symptoms in the Relationship Between Multiple, Adverse Social Determinants of Health and Breastfeeding Cessation, in the IGRAM Study, n = 213
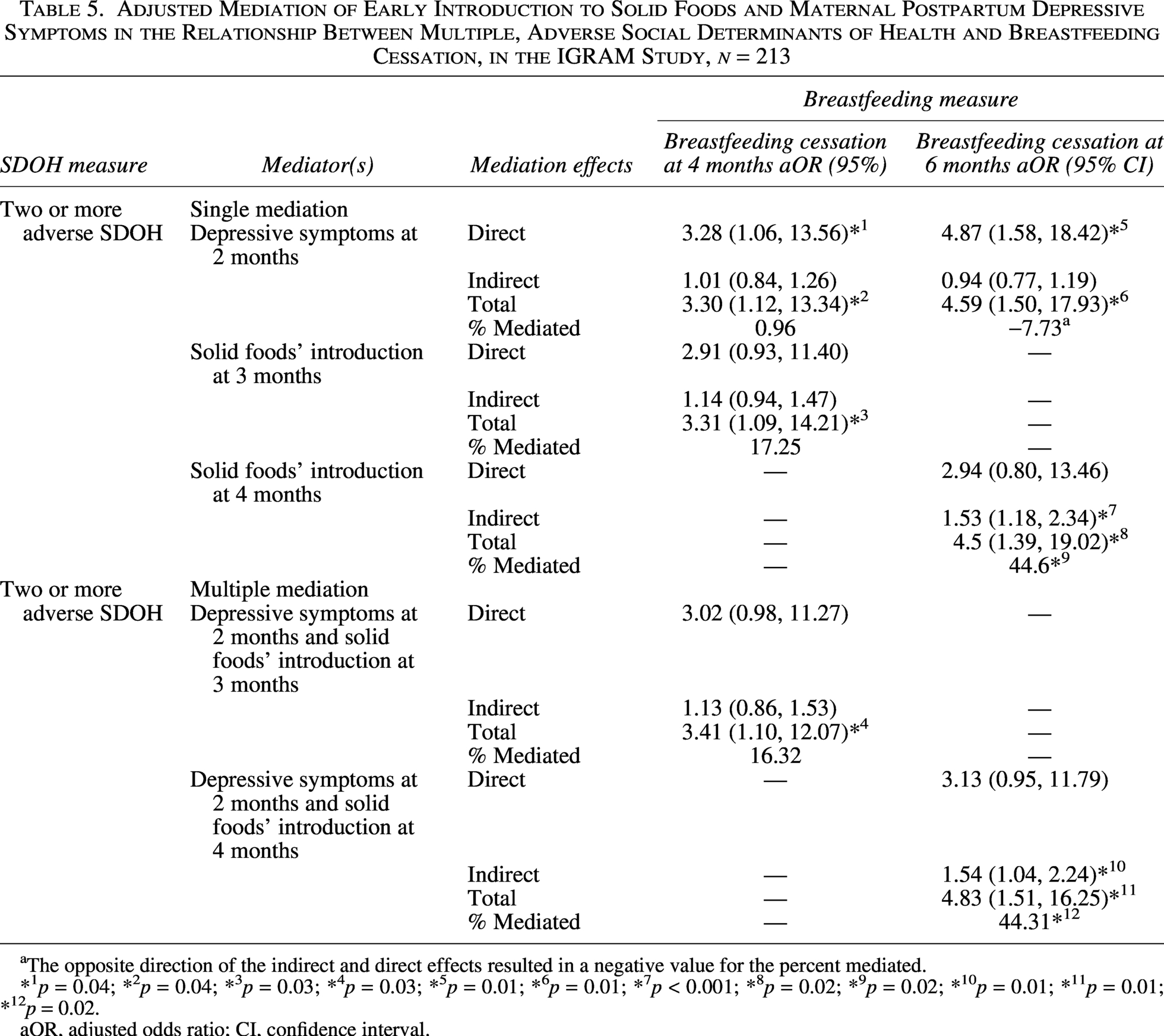
The opposite direction of the indirect and direct effects resulted in a negative value for the percent mediated.
*1p = 0.04; *2p = 0.04; *3p = 0.03; *4p = 0.03; *5p = 0.01; *6p = 0.01; *7p < 0.001; *8p = 0.02; *9p = 0.02; *10p = 0.01; *11p = 0.01; *12p = 0.02.
aOR, adjusted odds ratio; CI, confidence interval.
Early introduction to solid foods
Approximately one-third (n = 80) and roughly half (n = 130) of the sample introduced solid foods at 3 and 4 months of age, respectively. In adjusted mediation models, the introduction of solid foods at 4 months of age mediated 44.6% of the total effect of multiple adverse SDOH on breastfeeding cessation at 6 months of age (indirect effect: women with ≥2 SDOH compared with women with ≤1 SDOH OR = 1.53, 95% CI = 1.18, 2.34) (Table 5). In contrast, the introduction to solid foods at 3 months of age was not found to mediate the relationship in adjusted models (indirect effect: OR = 1.14, 95% CI = 0.94, 1.47). Similar to the results observed in the complete case analysis, in the adjusted multiple imputation models, the introduction of solid foods at 4 months of age mediated 40.9% of the total effect of multiple adverse SDOH on breastfeeding cessation at 6 months of age (indirect effect: OR = 1.47, 95% CI = 1.14, 1.95).
Discussion
In this secondary data analysis of mother–infant dyads from the IGRAM cohort study, we showed that experiencing multiple adverse SDOH was associated with increased odds of stopping breastfeeding at both 4 and 6 months of age. This analysis also demonstrated that the introduction of solid foods at 4 months of age partially mediated the total effect of multiple adverse SDOH on breastfeeding cessation at 6 months of age. Maternal depressive symptoms were not found to mediate the relationship at 4 or 6 months of age. In addition, in the exploratory analysis, participation in WIC and maternal education (i.e., mothers with a high school diploma or less) were associated with higher odds of stopping breastfeeding at 4 and 6 months of age. These findings collectively suggest that the presence of multiple adverse SDOH may increase the odds of stopping any breastfeeding among Black or African American mother–infant dyads.
Multiple adverse SDOH and odds of breastfeeding
In the current analysis, the odds of stopping any breastfeeding at 4 and 6 months of age were higher among Black or African American women with ≥2 SDOH compared with women with ≤1 SDOH. This result aligns with the study conducted by Newhook et al., 36 which compared multiple adverse versus favorable SDOH, specifically socioeconomically marginalized groups to socioeconomically privileged groups, and found that more women in the socioeconomically marginalized group (24.7%) stopped breastfeeding at one month compared with the socioeconomically privileged group (6.9%). Overall, the current findings are novel as this study, to the best of our knowledge, is among the first to concurrently examine the impact of experiencing multiple adverse SDOH on the timing of breastfeeding cessation among Black or African American mother–infant dyads.
Salience of adverse SDOH
In our exploratory analysis examining the individual contributions of each adverse SDOH, we found that mother–infant dyad participation in the WIC program (compared with those who did not participate) and women with a high school (or GED) education or less (compared with those with higher education) had higher odds of stopping breastfeeding at 4 and 6 months of age. The results regarding the association between maternal education and breastfeeding duration are consistent with the well-established link between maternal educational attainment and breastfeeding, with higher levels of education being associated with longer breastfeeding durations.21,37 Prior literature examining the association between WIC participation and breastfeeding duration has found mixed results, ranging from shorter to longer breastfeeding durations among WIC participants.38,39 One potential underlying explanation for these discrepancies could be the differences in the budget allotments for formula and breastfeeding within the WIC programs. A 2013 study found that WIC spends 25 times more on formula compared with its breastfeeding services, 40 which could shorten breastfeeding duration and exclusivity. The remaining exposure variables that we examined (Federal Poverty Level, participation in other governmental assistance programs, and food insecurity) were not associated with an increased odds of stopping breastfeeding at 4 or 6 months of age. Aranda et al. 41 found that individuals with housing insecurity had lower rates of exclusive breastfeeding at 6 months of age compared with those with secure housing. However, it is possible that being below 200% of the federal poverty level or participating in other governmental assistance programs may have increased access to needed supports, such as safe, clean, or secure housing that provides less crowded or private spaces for breastfeeding through the Section-8 Housing Choice Voucher program. There are conflicting findings within the published literature on the relationship between food insecurity and breastfeeding duration. Specifically, some studies have found shorter durations of breastfeeding among individuals who screened positive for food insecurity. 23 Whereas, other studies have found no association between this relationship.42,43 The food insecurity screening tool in this study assessed for having sufficient funds to purchase food. 44 Thus, it is plausible breastfeeding may have been used as a method to reduce food costs (e.g., formula), which may explain why food insecurity was not found to be significantly associated with breastfeeding duration in this study. Motivating factors to breastfeed (e.g., to save money or not buy formula) are beyond the scope of this study but highlight an important area of future study.
Maternal depressive symptoms
Despite the increased risk of depression associated with adverse SDOH, maternal depressive symptoms did not mediate the relationship between multiple adverse SDOH and the timing of breastfeeding cessation in the present analysis (4 months: OR = 1.01, 95% CI: 0.84, 1.27; 6 months: OR = 0.94, 95% CI: 0.77, 1.19). 17 Less than one-fifth (18.2%) of the present sample had CES-D scores of 16 or higher. This may be why, in this study, maternal depressive symptoms alone, without a clinical diagnosis of depression, did not mediate the relationship between multiple adverse SDOH and breastfeeding cessation. Data collected in the IGRAM study on depression treatments were focused on the use of tricyclic antidepressants. Thus, it is possible that maternal depressive symptoms were not identified as a mediator in this analysis, as mothers experienced improvement in depressive symptoms, following either treatment for depressive symptoms using other forms of treatment (e.g., selective serotonin reuptake inhibitors, cognitive behavioral therapy) or the birth of their infant. Future research needs to examine the mediating role of clinically diagnosed depression and other mental health conditions, such as anxiety, to better understand the role of PMADs in the relationship between multiple adverse SDOH and breastfeeding duration. Future research will also need to investigate the mediating effects of depressive symptoms in the relationship between multiple adverse SDOH and breastfeeding duration among mothers who received other forms (e.g., not tricyclic antidepressants) of treatment for depressive symptoms.
Early introduction to solid foods
Introduction to solid foods at 4 months, but not 3 months of age, was found to mediate the relationship between multiple adverse SDOH and breastfeeding cessation at 6 months. However, the same was not true for the relationship between multiple adverse SDOH and breastfeeding cessation at 4 months. Stern et al. 9 found that the earlier infants were introduced to solid foods, the earlier they consumed larger portions of solid foods. The early introduction of solid foods has also been shown to replace breast milk feedings. 45 Thus, one possible mechanism for the mediation of solid foods at 4 months, rather than at 3 months, is that the 2 months between the timing of introduction to solid foods and the subsequent timing of breastfeeding cessation was sufficient time for the infant to consume larger volumes of solid foods and replace enough breast milk feedings (at the breast or expressed) to cause secondary lactation failure. Another possible mechanism is that the 3-month model may have been underpowered to evaluate the mediation of introduction to solid foods at 3 months of age (n = 80). Conducting future research studies that examine the gap between the timing of introduction to solid foods, the number and/or quantity of solid foods consumed, and the feeding methods used (e.g., self-led weaning) is a critical next step in understanding the results of this study.
Study Strengths and Limitations
To the best of our knowledge, this study is among the first to examine the association between experiencing multiple adverse SDOH and the timing of breastfeeding cessation among Black or African American mother–infant dyads, and to investigate if this relationship was mediated by maternal depressive symptoms or the early introduction to solid foods.
Areas of limitation in this study include unmeasured confounding, such as marital or employment status, social support, or breastfeeding self-efficacy, which can increase the risk of biased estimates.21,46–49 Variables related to marital status, social support, and breastfeeding self-efficacy were not collected in the parent study. The employment variables had up to 74% missing data, as these questions were added to the questionnaire later in the parent study. Thus, future research should examine the relationship between experiencing multiple adverse SDOH and the timing of breastfeeding cessation, controlling for key covariates unavailable in the present analysis. The results of this study exhibited wide CIs, which may be a result of unmeasured confounding or small sample sizes in specific covariates and outcome variables (e.g., current smoking status, BMI). The included covariates are established influential factors affecting breastfeeding duration.21,47,50 In the current analysis, some of the covariates had a low prevalence. For example, only 17.1% of the sample reported current smoking, and 33.2% reported primiparity. The lower prevalence of known influential factors associated with shorter breastfeeding duration may have accounted for the wide CIs observed in the results. Similarly, overweight and obesity are known to be influential factors associated with shorter breastfeeding durations or early breastfeeding cessation.21,50 Maternal BMI equal to or greater than 30 kg/m2 was not associated with the odds of stopping breastfeeding in the current study. The parent study only included women with a healthy weight or obesity; thus, the exclusion of participants with overweight may have also contributed to the wide CIs observed in the present study. Lastly, although the selected adverse SDOH variables have established negative relationships with breastfeeding duration in the literature, the results from this secondary data analysis should be interpreted with caution as it was beyond the scope of this study to examine why these SDOH affected breastfeeding practices (e.g., duration or initiation). It is critical that future research examines the relationship between experiencing multiple adverse SDOH and the timing of breastfeeding cessation in larger samples and addresses covariates that were unavailable in this study.
Conclusions
The current study demonstrated increased odds of breastfeeding cessation at both 4 and 6 months of age among Black or African American mother–infant dyads with multiple adverse SDOH compared with dyads with one or no adverse SDOH. The relationship found between multiple adverse SDOH and breastfeeding cessation in this study underscores the need for interventions and policy changes that simultaneously address a combination of adverse SDOH to best support pregnant or breastfeeding Black or African American women. The finding that the introduction of solid foods at 4 months partially mediated the total effect of multiple adverse SDOH on breastfeeding cessation at 6 months of age underscores a critical target for anticipatory guidance and intervention in both clinical settings (e.g., primary care) and among federal assistance programs (e.g., WIC). The findings from this secondary data analysis provide key areas for future research including further examination of (1) adverse SDOH not included in the present study (e.g., employment) in the relationship between multiple adverse SDOH and the timing of breastfeeding cessation; (2) the additive effects of adverse SDOH on the timing of breastfeeding cessation; (3) the gap between the timing of introduction to solid foods and breastfeeding cessation; and (4) the role of diagnosed PMADs in the relationship between multiple adverse SDOH and breastfeeding duration.
Authors’ Contributions
C.N.S. contributed to conceptualization, data analysis, writing the original draft, and editing. L.H., B.S.Z., and T.V.E.K. contributed to data analysis. All authors contributed to the conceptualization and were involved in the review and editing of this work. All authors approved the final version of this article and took responsibility for its content.
Footnotes
Acknowledgments
Eileen Ford served as the program manager for the IGRAM project (parent study). Eileen made significant contributions to the design and implementation of the IGRAM study (parent study). Eileen was a driving force behind data collection and the design of the data collection forms.
Ethical Considerations
This study received ethical approval from the IRB of the University of Pennsylvania (approval no. 856339) on July 2, 2024, and the CHOP (approval no. 24-022656) on October 11, 2024.
Consent to Participate
Written informed consent was obtained from all participants in the parent study. Participants included in this study consented to secondary analysis of their data.
Consent for Publication
This study was included in the dissertation of Courtney Slater submitted in partial fulfillment of the requirements for the Doctor of Philosophy program at the University of Pennsylvania School of Nursing in 2025 and published on ProQuest and Scholarly Commons under embargo.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
Research reported in this publication was supported by the