
Abstract
Objective:
To improve access to hospital-grade breast pumps for women with infants in the neonatal intensive care unit (NICU) by reducing delays in pump acquisition.
Design:
A quality improvement project using Lean Six Sigma DMAIC (Define–Measure–Analyze–Improve–Control) methodology to identify process gaps and streamline workflows.
Setting/Local Problem:
Level IV NICU at a large academic medical center in the western United States. Women with private or employer-sponsored insurance experienced acquisition delays and out-of-pocket costs compared with women covered by public assistance programs (e.g., Medi-Cal, women, infants, and children [WIC]).
Patients:
Baseline cohort included 39 NICU families (April 2023): 12 with private insurance and 27 with public assistance coverage. During the 12-month follow-up period, 200 admissions were recorded. In addition, 47 staff members participated in the study.
Intervention/Measurements:
Baseline measures included pump ordering timelines, insurance coverage type, and out-of-pocket costs. Interventions included role clarification, durable medical equipment (DME) vendor mapping, standardized communication protocols, staff education, and patient-facing handouts. An onsite WIC pump supply was established. Outcomes were monitored for 12 months.
Results:
At baseline, 92% (11/12) of privately insured women paid out of pocket for hospital-grade pumps, with delays of up to 21 days; women with public assistance coverage obtained pumps within 1–2 business days. After implementation, out-of-pocket rates declined to less than 5%, and median acquisition time decreased to 3.5 days (range: 1–7 days) for privately insured families. Improvements were sustained at 12 months.
Conclusions:
Lean Six Sigma–guided process redesign improved the efficiency and equity of hospital-grade breast pump access in the NICU, reducing delays and financial burden for privately insured families. Persistent payer exclusions highlight insurance-related barriers as a social determinant of lactation support.
Keywords
Human milk is considered a critical component of care because it is associated with lower rates of necrotizing enterocolitis, sepsis, and other prematurity-related morbidities, as well as improved neurodevelopmental outcomes and reduced health care costs.1,2 Despite this evidence, access to hospital-grade breast pumps is not equally distributed. At many institutions, women with infants covered by public assistance programs (e.g., Medi-Cal, WIC) receive relatively timely access to appropriate pumping equipment. In contrast, women with private or employer-sponsored insurance often encounter delays, fragmented communication, and high out-of-pocket costs, reflecting broader disparities in access to maternity and postpartum support services.3,4 These disparities introduce avoidable stress during infants’ neonatal intensive care unit (NICU) stay and may adversely affect lactation outcomes. Despite federal mandates requiring private insurers to cover breast pumps without cost sharing, reimbursement policies and access workflows vary substantially by carrier, leaving individual institutions without standardized processes to bridge this gap.
Problem description
We conducted this quality improvement initiative in a Level IV NICU at a large academic medical center in the western United States, providing complex medical and surgical care to critically ill and premature infants. Within this setting, a long-standing disparity existed in access to hospital-grade breast pumps based on insurance type. Women with infants covered by public assistance programs (e.g., Medi-Cal, WIC) had defined pathways to obtain equipment, while women with private or employer-sponsored insurance were routinely advised to rent pumps out-of-pocket from a local, out-of-network vendor. No standardized institutional process existed to facilitate insurance authorization or DME coordination for these families.
This workflow remained largely unexamined until a clinical case prompted reassessment of existing assumptions. A woman with premature triplets requested assistance obtaining a hospital-grade breast pump through insurance, citing prior coverage during a previous NICU admission at another institution. Direct communication with a regional DME vendor clarified authorization requirements, and the pump was delivered within 24 hours. Subsequent cases involving women with different insurers demonstrated that insurance-covered access was feasible, although timelines varied depending on payer requirements and staff familiarity with DME processes.
These observations revealed that delayed or absent pump access was not primarily driven by insurance policy limitations but by the absence of a standardized, staff-supported workflow and clearly defined process ownership. Reliance on informal guidance and individual knowledge led to inconsistent access, financial burdens for families, and avoidable delays during a critical period of lactation establishment. This identified process gap provided the foundation for the current quality improvement initiative, which aimed to redesign workflows to improve the equity, efficiency, and reliability of hospital-grade breast pump access in the NICU.
Rationale
We used Lean Six Sigma, a process improvement framework that combines Lean principles (waste reduction) with Six Sigma strategies (reducing variation).5,6 We selected this methodology for its structured approach to identifying root causes and eliminating non-value-added steps that contribute to delays. We applied the Define–Measure–Analyze–Improve–Control (DMAIC) phases to systematically standardize the pump ordering workflow.
The objective of this quality improvement project was to improve access to hospital-grade breast pumps for women with infants in the NICU by reducing the time between pump request and acquisition.
Methods
Intervention
We designed and reported this quality improvement initiative in accordance with the Standards for QUality Improvement Reporting Excellence (SQUIRE 2.0) guidelines, 7 which provided the reporting framework for this article. Lean Six Sigma DMAIC guided the systematic identification, implementation, and evaluation of process changes. Explicit attention was given to contextual factors influencing pump access, including institutional workflows, interdisciplinary roles, insurance authorization processes, and vendor requirements. The initiative focused on redesigning existing processes to improve the efficiency and equity of hospital-grade breast pump access for NICU families, rather than testing a clinical intervention on individual patients. Root cause analysis using fishbone diagrams and process mapping (Figs. 1 and 2) identified three primary areas for intervention. First, we developed a DME Vendor Matrix, a visual reference tool mapping specific insurance plans (e.g., Blue Cross, Aetna) to their contracted vendors supplying hospital-grade pumps, eliminating the need for staff to research vendors for each patient. Second, we implemented role clarification protocols: bedside nurses and International Board Certified Lactation Consultants (IBCLCs) were designated to identify each family’s need and initiate the order, while case managers were assigned the specific task of transmitting the prescription to the identified vendor. Third, we established a dedicated on-site WIC pump supply, allowing immediate distribution of pumps to women whose infants were covered by WIC. This WIC closet operated by maintaining a standing inventory of hospital-grade loaner pumps provided by the local WIC agency; eligible women were identified at admission and issued a pump directly from the unit, typically within the first 24 hours. This intervention did not reduce access for WIC-eligible families; rather, it streamlined their pathway and simultaneously freed case management resources to address the more complex private-insurance authorization process. We organized standardized training sessions to familiarize staff with all new workflows.
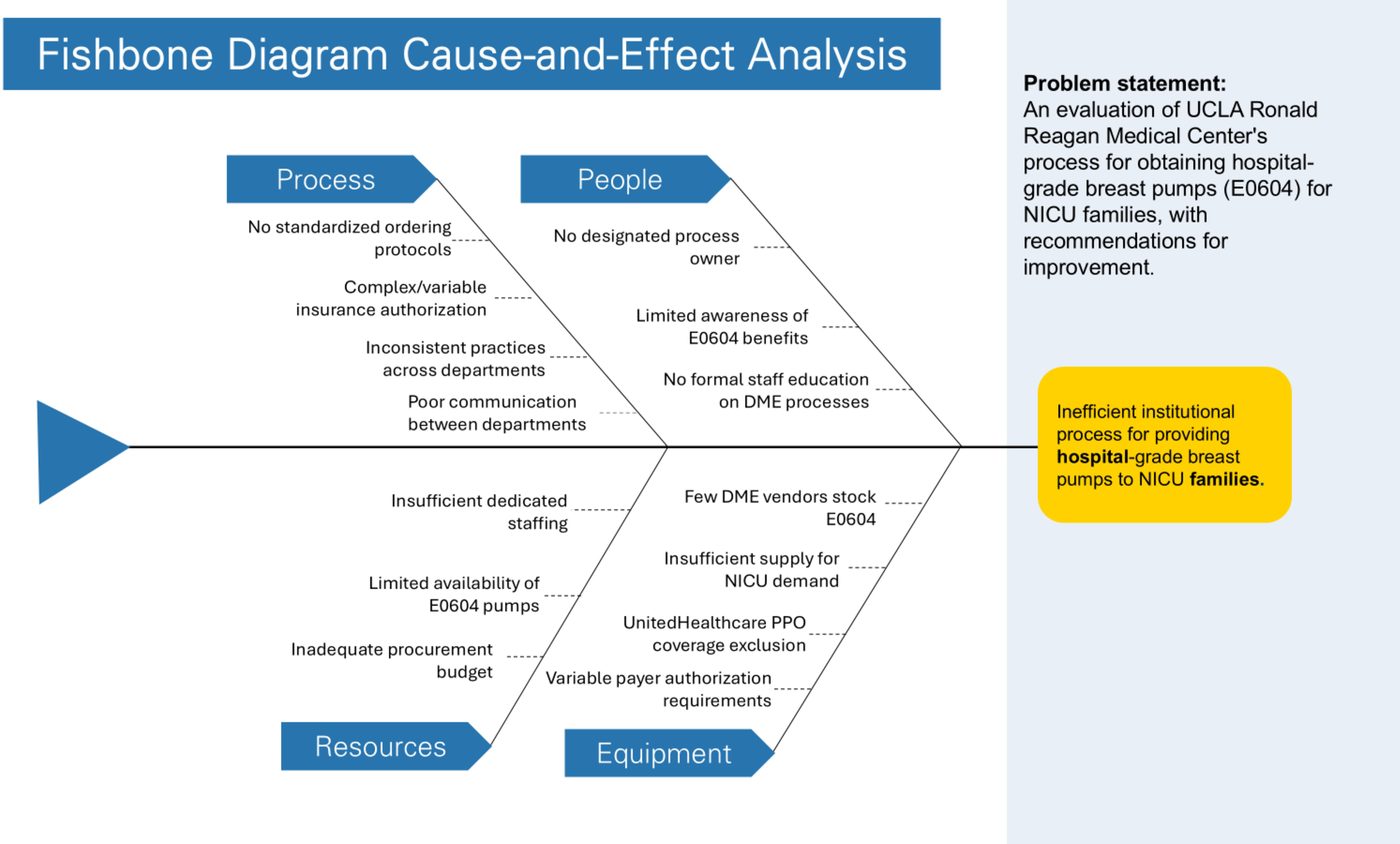
Fishbone diagram: Barriers to hospital-grade breast pump access for privately insured NICU families. This fishbone diagram illustrates the key barriers identified during the Analyze phase of the DMAIC process, including communication, vendor knowledge, insurance processes, and workflow standardization. DMAIC, Define–Measure–Analyze–Improve–Control; NICU, neonatal intensive care unit.
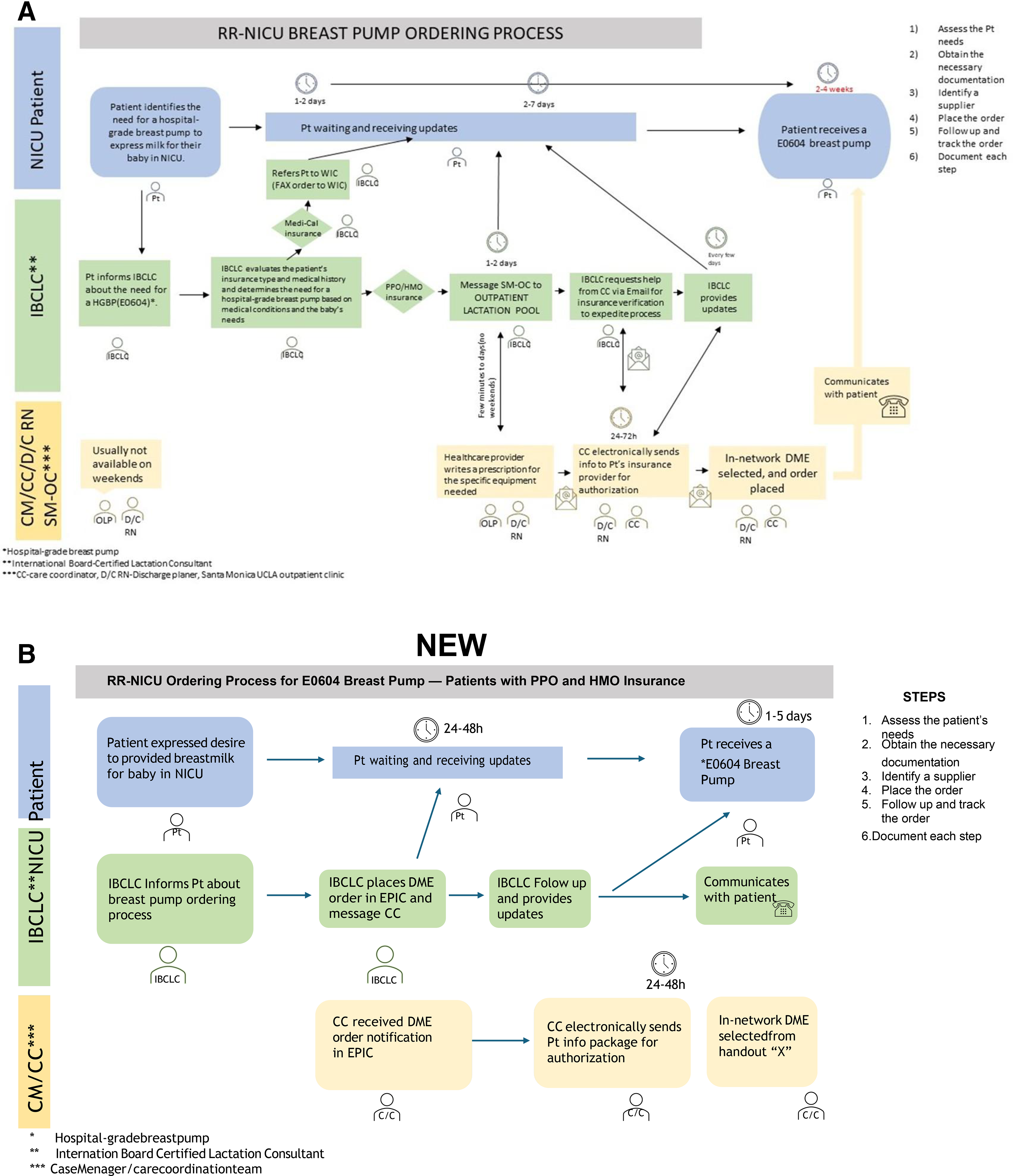
Process map: Hospital-grade breast pump ordering workflow before
Context
We conducted this initiative in a Level IV NICU at a large academic medical center. Stakeholders included lactation consultants, NICU nurses, case managers, discharge planners, social workers, and DME vendors. DME vendors were engaged during the Analyze phase to map authorization requirements by payer and confirm equipment availability and during the Improve phase to establish direct ordering pathways. The project lead, an IBCLC with extensive NICU experience, facilitated data collection and coordinated interdisciplinary input.
Measures
Process measures included time from pump request to delivery (in days), stratified by insurance type (private versus public assistance), and the proportion of privately insured families successfully obtaining pumps through insurance coverage. Outcome measures included the proportion of families incurring out-of-pocket costs for pump rental and the average monthly out-of-pocket cost per family. A balancing measure tracked whether the WIC closet intervention affected pump access for WIC-eligible families; specifically, we monitored whether acquisition times for WIC-covered women changed following implementation. A voluntary electronic survey administered to the interdisciplinary NICU team (N = 47) assessed staff knowledge across three domains: perceived importance of timely pump access, familiarity with the pump ordering process, and awareness of private payer coverage for hospital-grade pump rentals. This survey served as the primary diagnostic tool for identifying root causes of the process failure. Baseline process data for April 2023 admissions (n = 39) were tracked in a spreadsheet documenting insurance type, pump delivery status, and acquisition delays by payer. Descriptive statistics were used to summarize all baseline and postimplementation measures.
Results
Among 39 NICU admissions in April 2023, 27 (69%) were covered by Medi-Cal or WIC and 12 (31%) by private or employer-sponsored insurance. Women with Medi-Cal or WIC coverage obtained hospital-grade breast pumps within a median of 1–2 business days through established agency pathways. Among the 12 privately insured families, only 3 (25%) successfully obtained pumps through insurance during the baseline period. Despite this, 11 out of 12 families (92%) incurred out-of-pocket rental costs because several families rented pumps temporarily while awaiting insurance authorization and later transitioned to insurance-covered equipment. Two privately insured families experienced acquisition delays of 14 and 21 days, respectively, and several rented pumps at an average cost of $145 per month. Families were often required to travel more than 25 minutes to the nearest DME vendor to obtain equipment. Kaiser-covered families demonstrated the shortest acquisition times among privately insured families, typically within 24 hours, due to an existing vendor relationship.
Staff survey results (N = 47) indicated that 98% of respondents (46/47) rated timely, insurance-covered pump access as very important for NICU families, yet 70% reported receiving no formal education or having limited awareness of a standardized pump-ordering process. A significant proportion were also unaware that private payers typically cover hospital-grade pump rentals (HCPCS code E0604) for women with infants in the NICU, identifying gaps in staff knowledge about available insurance benefits as a primary driver of the process failure.
Postintervention outcomes
During the 12-month follow-up period, more than 200 NICU admissions occurred. Thirty privately insured families requiring access to hospital-grade pumps were identified and tracked for outcome analysis. Follow-up data collected from May 2023 through April 2024 demonstrated improvements in pump access for privately insured families. The proportion of privately insured families obtaining hospital-grade pumps through insurance increased from 25% (3/12) at baseline to 60% (18/30) postimplementation. Median time to pump acquisition for privately insured families decreased from up to 21 days at baseline to 3.5 days postimplementation (range: 1–7 days). Out-of-pocket rental rates for privately insured families decreased from 92% (11/12) at baseline to less than 5% postimplementation. For comparison, women with public assistance coverage maintained consistent access throughout, with pump acquisition times remaining at 1–2 business days (Fig. 3). Remaining coverage exclusions were limited to a single insurance carrier (UnitedHealthcare PPO). The on-site WIC pump supply and the lactation documentation tab in the electronic health record were both sustained through the 12-month follow-up period.
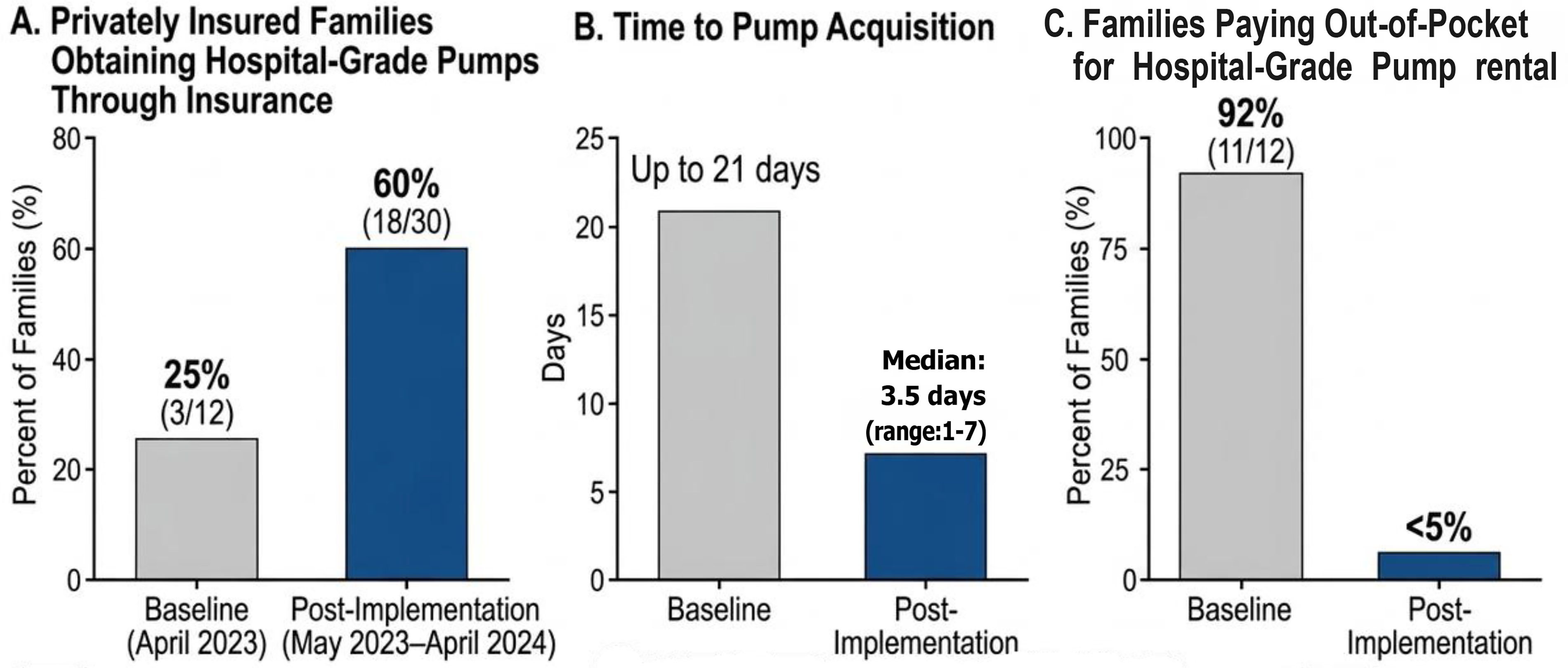
Pre- and postintervention outcomes among privately insured NICU families.
Discussion
This project demonstrates that Lean Six Sigma methodology can successfully improve the efficiency and equity of hospital-grade pump access in the NICU. Using DMAIC tools, we identified key bottlenecks including fragmented communication, unclear interdisciplinary roles, and gaps in staff knowledge about DME vendors and insurance authorization processes (Fig. 1). Standardized communication protocols and vendor mapping reduced ordering delays and financial burdens. Sustained improvements at 12 months confirm the effectiveness of these interventions in reducing access inequities. The success of this intervention suggests that perceived access barriers are often, fundamentally, process barriers: Although both the necessary equipment and insurance coverage were in place, the mechanism for linking them was dysfunctional. By establishing clear vendor pathways and defining staff roles, we bridged this operational gap. Implementing these changes required alignment across clinical and administrative stakeholders. Initial perspectives framed pump access delays as external insurance-related barriers; however, baseline data demonstrated that internal workflow redesign could meaningfully improve access and equity. By quantifying the disparity and framing it as a solvable workflow gap rather than an intractable payer issue, we secured the necessary leadership support to restructure the ordering process.
The persistent gap among families covered by UnitedHealthcare PPO plans indicates that insurance policies remain a critical determinant of access, forcing some families to continue renting pumps out of pocket. This exemplifies how inequity in health care is linked to social determinants of health, with insurance carriers’ policies dictating lactation support options.3,4 While the Affordable Care Act required private insurers to cover breast pumps without cost sharing beginning in 2012, reimbursement policies vary substantially by carrier; evidence demonstrates that reductions in insurer reimbursement thresholds risk shifting women toward lower-quality devices with diminished milk output and reduced breastfeeding duration.8,9 In this context, inequity refers to disparities in access to medical care based on payer type: the process failure forced privately insured families to face barriers that publicly insured families did not, regardless of socioeconomic status. Notably, the WIC closet intervention did not diminish access for women with public assistance coverage; access times for WIC-eligible women remained stable at 1–2 business days throughout the follow-up period, confirming that the balancing measure was preserved. The planned hospital-managed loaner pump program could further address disparities by providing immediate equipment to families awaiting prior authorization or during periods when case management support is limited. The addition of a lactation documentation tab in the electronic health record represents a durable systems–level change, reducing reliance on ad hoc workflows and ensuring long-term sustainability.
Our findings align with previous studies demonstrating that pump-dependent mothers without access to hospital-grade equipment may produce approximately half the cumulative milk volume of those with appropriate pump access, a deficit that may not fully resolve even after proper equipment subsequently becomes available,10–12 and that inadequate access to equipment and lactation support increases maternal anxiety and reduces mothers’ own milk provision in the NICU.13,14 These findings reflect broader racial and socioeconomic disparities in breast milk feedings documented across U.S. NICUs, in which maternal pump rental costs and the opportunity costs of sustained pumping have been identified as primary mediators of the racial gap in mother’s own milk provision at NICU discharge, with Black very low birth weight infants substantially less likely than non-Black infants to receive mother’s own milk through discharge.3,15,16 Our project extends this literature by identifying insurance type, independent of race or income, as an additional, addressable determinant of access.
Long-term recommendations include establishing an in-house DME provider and creating a hospital-managed pump loan program, an intervention for which evidence from similar NICU populations demonstrates improved human milk feeding rates at discharge and beyond.16–19 The recently implemented lactation tab within epic reflects the sustainability principles of the Control phase of DMAIC and can serve as a model for replication in other NICU settings.
Limitations
This quality improvement project was conducted at a single academic medical center within the United States, which may limit generalizability to health care systems with different reimbursement structures, equipment procurement processes, or universal health care coverage. The baseline observation period was limited to one month of admissions, potentially limiting representation of seasonal variation in patient volume or case mix. In addition, manual data collection may have introduced reporting inconsistencies, and survey responses may be subject to self-report bias. Finally, this initiative focused on process outcomes and did not evaluate downstream clinical outcomes such as milk production, breastfeeding duration, mother’s own milk feeding rates, or neonatal health outcomes. Future studies should examine whether improved pump access translates into measurable benefits for lactation and infant health.
Implications for practice
Health care institutions should systematically evaluate and address barriers to hospital-grade breast pump access for NICU families. Lean Six Sigma provides a structured framework for identifying and resolving process inefficiencies that create inequitable access. Nurses, lactation consultants, and case managers should be educated about insurance coverage variations and equipped with standardized protocols to facilitate timely pump orders. Integration of lactation support documentation into electronic health record systems can improve communication and workflow efficiency. Establishing loaner pump programs can provide immediate access to families facing authorization delays or coverage gaps; institutional loaning programs in comparable preterm populations have demonstrated sustained improvements in human milk feeding rates through NICU discharge and at 6 months’ postpartum. 19 Health care providers should advocate for insurance policy changes that ensure equitable access to hospital-grade breast pumps for all NICU families, recognizing that insurance coverage is a social determinant of health that affects lactation outcomes. Finally, leadership should recognize that quality improvement is often driven by individual staff members’ passion. Encouraging these efforts does more than fix workflows; it motivates the entire interdisciplinary team to believe that they can, and should, challenge inefficiencies to make a tangible difference in patient care.
Conclusion
The application of Lean Six Sigma methodology streamlined the process for securing hospital-grade breast pumps in the NICU, improving equity and reducing the financial burden for families. Standardizing communication, clarifying roles, and leveraging technology represent actionable strategies to sustain improvement. Furthermore, this initiative serves as a testament to the power of frontline providers in identifying hidden systemic barriers. By recognizing a lack of process and acting upon it, a single health care provider can drive significant equity improvements. Ultimately, the goal of disseminating this work is to motivate other clinicians to look beyond the “status quo.” We hope this project demonstrates that individual staff members, regardless of administrative rank, possess the agency to dismantle complex barriers and make a profound difference in the lives of the families they serve. Broader implementation of these methods could reduce disparities in lactation support nationwide. Persistent insurance coverage gaps underscore the need for continued advocacy to address insurance as a social determinant of health affecting lactation support for NICU families.
Author’s Contributions
M.J.O.: Conceptualization, data collection, formal analysis, methodology, project administration, writing—original draft, and writing—review and editing.
Ethical Considerations
This project was designed and conducted as a quality improvement initiative with the primary aim of improving internal workflows and hospital-grade breast pump access at a single institution. As a quality improvement project, it does not constitute human subjects research as defined under 45 CFR 46.102(d) and did not require IRB review or approval. The staff knowledge survey was administered solely to identify internal process failures driving the workflow gap and to guide targeted interventions—not to generate or test hypotheses intended for generalization beyond this institution. The intent to disseminate findings to motivate similar institutional improvements does not alter this classification, as the primary goal remains process improvement rather than the production of generalizable knowledge.
Consent to Participate
Not applicable. This quality improvement project did not involve individual human subjects research.
Data Availability
The data supporting this quality improvement project are not publicly available due to institutional patient privacy policies but are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The author thanks the NICU staff, case managers, discharge planners, and lactation team at UCLA Ronald Reagan Medical Center for their support and collaboration in this quality improvement initiative. The author also gratefully acknowledges Laura Erskine, PhD, Faculty, UCLA Fielding School of Public Health, for her mentorship and guidance as faculty advisor during the MHA capstone project from which this work originated. The author thanks the NICU staff, case managers, discharge planners, faculty advisor for my MHA capstone project, and lactation team at the study institution for their support and collaboration in this quality improvement initiative. The author used artificial intelligence-assisted writing tools (Claude, Anthropic) for article editing, specifically grammar and spelling, and reference formatting.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this project.