
Abstract
Objective:
This study aimed to identify factors influencing the frequency of fresh mother’s own milk feeding during the first 7 days of life in very low birth weight infants (VLBWIs), in order to inform evidence-based nursing interventions.
Methods:
A retrospective case-control study was conducted. A total of 917 VLBWIs admitted to the neonatal intensive care unit of a tertiary maternity hospital in Zhejiang Province, China, between January 2020 and December 2023, were enrolled using convenience sampling. Based on the number of adequate fresh mother’s own milk feedings, infants were categorized into three ordinal groups: 0 times, 1–13 times, and ≥14 times. Univariate ordinal logistic regression was used to screen for statistically significant variables, which were subsequently included in a multivariate ordinal logistic regression model to adjust for confounders and identify independent factors.
Results:
Multivariate analysis identified multiple gestation (odds ratio [OR] = 0.66, 95% confidence interval [CI]: 0.50–0.87) and higher CRIB-II score (OR = 0.90, 95% CI: 0.81–0.99) as significant risk factors for reduced feeding frequency. In contrast, several protective factors were confirmed: two or more telephone follow-ups (OR = 1.68, 95% CI: 1.27–2.23), parental participation in offline professional educational sessions (OR = 2.78, 95% CI: 1.63–4.77), father as primary milk transporter (OR = 1.96, 95% CI: 1.25–3.09), higher paternal education level (OR = 3.03, 95% CI: 1.30–10.58), and cesarean delivery (OR = 1.96, 95% CI: 1.44–2.68).
Conclusion:
The frequency of early fresh mother’s own milk feeding in VLBWIs is influenced by a constellation of neonatal, interventional, and familial factors. To effectively promote feeding practices, clinical care should implement an integrated model that encompasses risk assessment (e.g., for multiples and infants with high illness severity), systematic nursing interventions (including structured follow-up and parent education), and enhanced family support, with a particular emphasis on paternal engagement.
Statement of Significance
Problem or Issue: Promoting fresh mother’s own milk feeding for very low birth weight (VLBW) infants during the critical first week of life remains a significant clinical challenge.
What is Already Known: Clinical risks such as neonatal illness severity are known barriers to establishing early milk feeding.
What This Paper Adds: This study quantifies the strong protective effect of paternal engagement and identifies structured nursing interventions (e.g., ≥2 follow-ups) as key facilitators. It uniquely highlights the need for tailored post-discharge support for families after vaginal birth. The findings provide an evidence base for an integrated, family-centered clinical care model.
Keywords
Introduction
Fresh mother’s own milk, defined as unpreserved milk fed to infants within 4 hours of expression, is critically important for vulnerable neonates.1,2 For very low birth weights (VLBWs) (defined as infants weighing < 1,500 g at birth), particularly in the first week of life, fresh milk serves as a personalized medicine, rich in immunologically active components that confer significant benefits for immune development and reduction of complications.1,3–5 Consequently, both international and national guidelines strongly advocate for the preferential use of fresh mother’s own milk in the care of preterm and high-risk infants.6,7 However, the establishment and maintenance of fresh mother’s own milk feeding for very low birth weight infants (VLBWIs) face substantial systemic barriers. Following birth, infants are admitted to a closed Neonatal Intensive Care Unit (NICU), resulting in maternal separation. This situation necessitates that mothers express breast milk and transport it to the NICU promptly, often requiring deliveries every 3 hours—a process that presents a formidable challenge for families. 8 These challenges contribute to the persistently low rates of fresh mother’s own milk feeding in domestic settings. 9 Therefore, promoting fresh mother’s own milk feeding for VLBWIs in the NICU has become a key focus and a critical challenge in recent research. However, evidence regarding the factors influencing its feeding frequency during the very first days of life, particularly from a multidimensional perspective, remains limited. 9 Our institution hosts the first human milk bank in Zhejiang Province and has implemented several innovative support measures, including doorstep milk collection and dedicated courier services. To inform the development of more precise clinical interventions, this study aims to retrospectively analyze the key factors associated with the feeding frequency of fresh mother’s own milk during the first 7 days of life in VLBWIs.
Methods
Study design and participants
This retrospective case-control study was conducted in the NICU of a tertiary maternity hospital in Zhejiang Province, China. A convenience sample of 917 VLBWIs born and admitted to the NICU between January 2020 and December 2023 was enrolled.
Inclusion criteria were: (1) gestational age < 32 weeks and birth weight ≤ 1,500 g; (2) direct admission to the NICU after birth; and (3) initiation of enteral nutrition within 12–24 hours of birth. Exclusion criteria were: (1) documented medical contraindications to fresh mother’s own milk feeding and (2) hospital stay of less than 7 days; and (3) severe congenital malformations or death unrelated to breastfeeding. The study was approved by the hospital’s Institutional Review Board (Approval No: IRB-20240072-R).
The sample size was calculated based on 5–10 times the number of independent variables (n = 29), 10 plus an additional 10–20% to account for potential invalid cases, and then divided by the rate of colostrum feeding in the NICU (43.95%). This yielded a minimum sample size of 792. A total of 917 infants were ultimately included to enhance the statistical power, given the uncertain rate of exclusive fresh mother’s own milk feeding in this population.
Grouping criteria
Based on the clinical practice of preterm infant feeding at our center, an “adequate” fresh mother’s own milk feeding was defined as follows: a feeding was counted as adequate only if the nurse documented that the milk administered consisted of 100% fresh mother’s own milk and the administered volume met the full volume prescribed by the physician for that specific feeding. Verification of feeding adequacy was based on the recorded volume in the nursing charts.
Based on previous studies,3,11,12 infants were categorized into three ordinal groups according to the number of adequate fresh mother’s own milk feedings received within the first 7 days of life: the nonfeeding group (0 times), the low-frequency feeding group (1–13 times), and the high-frequency feeding group (≥14 times).
Standardized clinical education and support protocol (routine care)
The following procedures represent the standard of care provided to all families following infant admission to the NICU, rather than an experimental intervention. They were implemented consistently throughout the study period.
After the infant’s admission to the NICU, a structured face-to-face education session was conducted with the father. This session detailed the critical importance of fresh milk, provided instruction on specific expression techniques, and outlined proper handling procedures, after which informed consent was secured. To reinforce this foundational instruction, targeted educational materials on breastfeeding management were subsequently disseminated via a cloud-based follow-up system.
The dedicated breastfeeding management team conducted telephone-based knowledge assessments to verify comprehension, identified the designated primary milk transporter (the family member responsible for delivering fresh milk to the NICU), collected supplementary paternal information, and delivered additional telephone follow-ups as needed. Maternity ward nurses provided hands-on instruction and assistance with initial milk expression using breast pumps. All expressed milk was collected in standardized containers with patient identification labels.
Based on the half-life of fresh mother’s own milk and to ensure its quality, a logistical protocol required that the milk be delivered to the NICU every 3 hours. Transportation was undertaken by the infant’s father, grandparents, or a nanny (including family nanny or postpartum caregiver). In addition, the hospital’s human milk bank conducted weekly offline professional educational sessions to provide ongoing education and support to families.
Impact of the COVID-19 pandemic on study procedures
The study period (January 2020 to December 2023) overlapped with the COVID-19 pandemic. Our hospital was not a designated COVID-19 referral center; infected or suspected patients were transferred elsewhere. Rigorous screening was applied to all maternity admissions. For nearly the entire study period, no confirmed COVID-19 cases were identified among obstetric patients, and standard protocols for fresh mother’s own milk (receipt, handling, and feeding) remained unchanged.
A brief exception occurred during the peak outbreak: the NICU temporarily suspended acceptance of fresh milk for several weeks starting December 18, 2022. However, according to our enrollment records, no VLBWI meeting the inclusion criteria was born between November 2, 2022, and the end of that year. Thus, this temporary measure did not affect any included infant, and the pandemic had no substantive impact on the study findings.
Data collection and instruments
Data were collected using a standardized form developed after a comprehensive review of the literature (CNKI, WanFang, VIP, PubMed) and consultation with clinical experts. The finalized form comprised six sections:
Demographics: Infant characteristics (sex, gestational age, birth weight, Apgar scores at 1 and 5 minutes, CRIB-II score) and parental profiles (parental age, education level, employment status, residence). Maternal delivery data: Steroid exposure, mode of delivery, gravidity, parity, plurality, membrane rupture type, and amniotic fluid characteristics. Maternal health status: Postpartum maternal health, adverse obstetric history, histological chorioamnionitis, and pregnancy comorbidities (e.g., hypertension, diabetes, heart disease, depression), with the presence of any such condition classified as a maternal health issue. Systematic interventions: Number of telephone follow-ups, parental participation in offline professional courses, and telephone knowledge test score. Family support: Identity of the primary milk transporter. Feeding outcome: Adequate fresh mother’s own milk feedings frequency within the first 7 days of life.
Quality control
Two trained research nurses collected data strictly in accordance with the inclusion and exclusion criteria. Both nurses had ≥10 years of experience in the NICU and had completed an initial 18-hour breastfeeding training course, followed by annual 3-hour refresher training thereafter. Data were obtained from three sources: the electronic medical record system (infant and maternal characteristics), the breastfeeding support team’s records (intervention details, including telephone follow-ups and course participation), and NICU nursing notes (feeding records). All data were double-checked for accuracy prior to entry into an Excel database. A dedicated data analyst was part of the study team to ensure the accuracy of the statistical analyses.
Statistical analysis
Analyses were performed using R software (version 4.3.1). Continuous variables are presented as mean ± standard deviation if normally distributed (compared using t-tests) or as median and interquartile range if non-normally distributed (compared using the Mann–Whitney U or Kruskal–Wallis H test). Categorical data were presented as counts and percentages and compared using the chi-square test. Variables with statistical significance in univariate ordinal logistic regression were included in a multivariate ordinal logistic regression model to identify independent protective and risk factors associated with fresh mother’s own milk feeding frequency. A two-sided p value <0.05 was considered statistically significant.
Results
Participant characteristics and flow
From an initial cohort of 1,313 VLBWIs, 917 were included in the final analysis after applying exclusion criteria (343 with hospital stays < 7 days, 2 deaths, and 51 with congenital anomalies). Eleven infants transferred for surgery (primarily for necrotizing enterocolitis) were retained in the primary analysis. Missing data were handled using multiple imputation.
The 917 VLBWIs were categorized into three ordinal groups based on the frequency of adequate fresh mother’s own milk feeding during the first 7 days of life: no feeding (0 times, n = 410), low-frequency feeding (1–13 times, n = 321), and high-frequency feeding (≥14 times, n = 186).
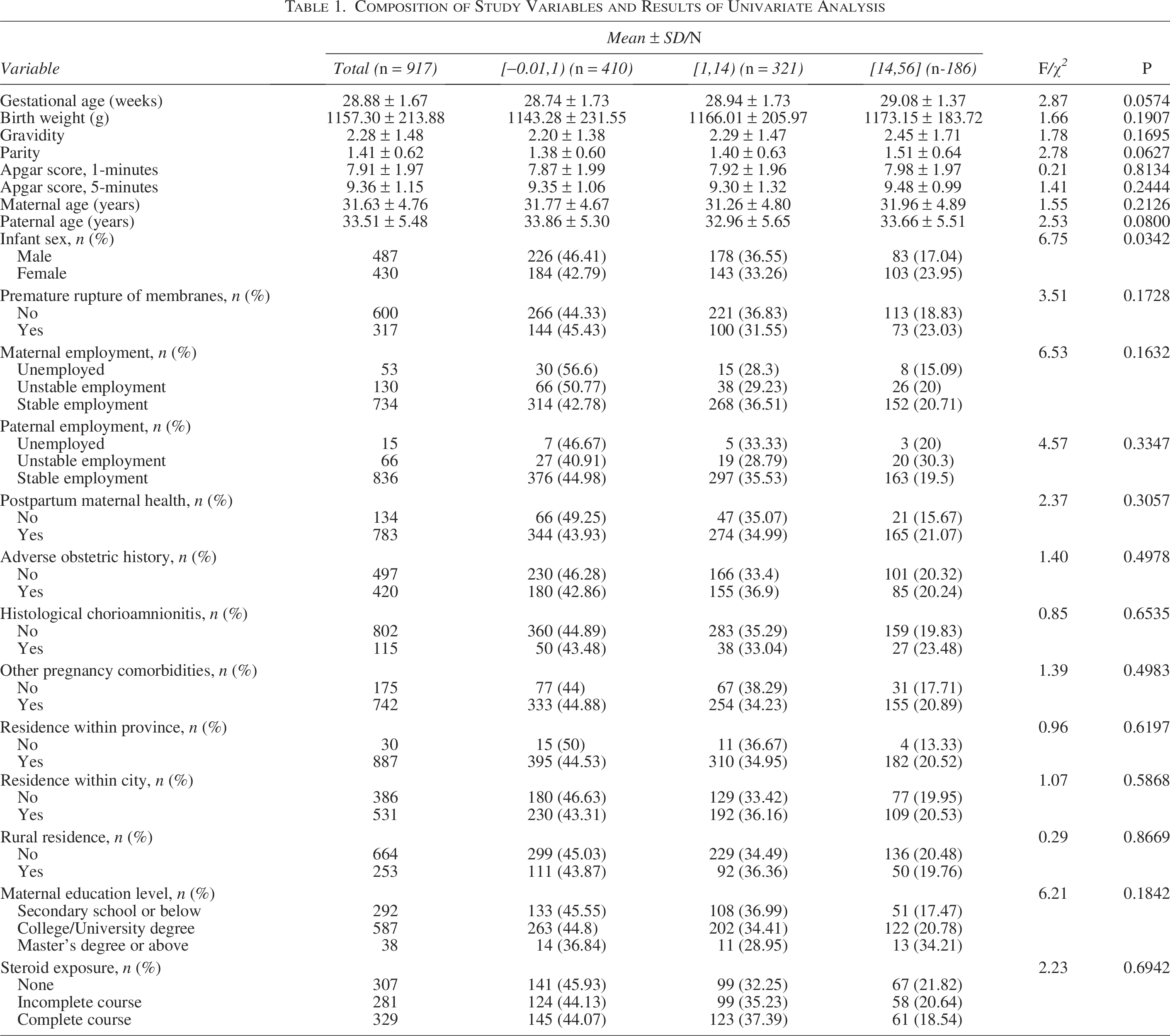
Comparison of baseline demographic and clinical characteristics revealed a statistically significant difference in infant sex distribution across groups (p = 0.034). Specifically, female infants constituted a higher proportion in the high-frequency feeding group (≥14 feedings) than male infants (23.95% vs. 17.04%), whereas male infants were more prevalent in the non-feeding group (0 feedings) (46.41% vs. 42.79%). No significant differences were observed in other variables, including gestational age, birth weight, parental age, gravidity, parity, amniotic fluid contamination, premature rupture of membranes, histological chorioamnionitis, other maternal comorbidities during pregnancy, postpartum maternal health status, adverse obstetric history, or steroid exposure (all p > 0.05), as detailed in Table 1.
Composition of Study Variables and Results of Univariate Analysis
Factors associated with feeding frequency
Univariate ordinal logistic regression analysis
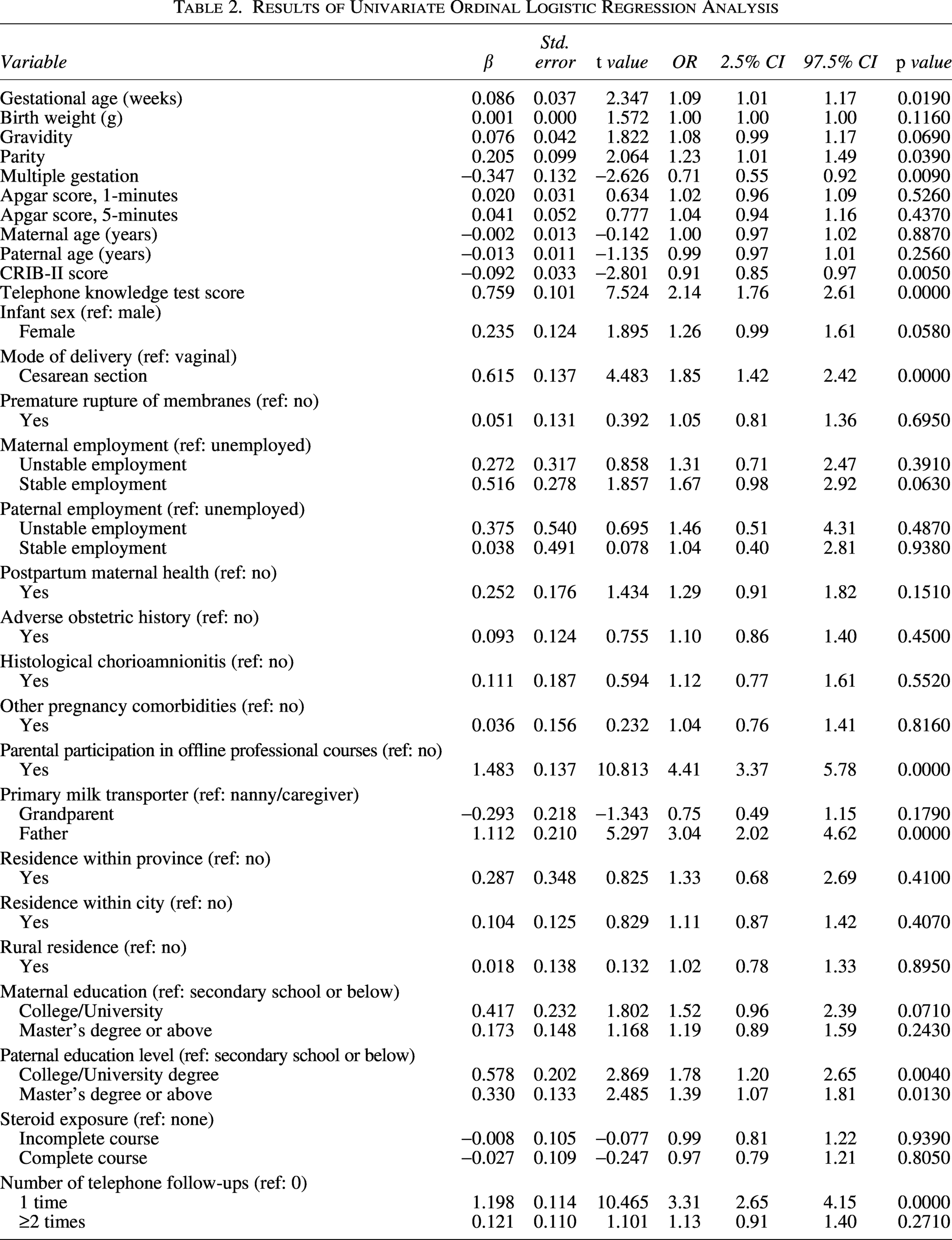
Univariate analysis was conducted using a significance threshold of p < 0.10 to identify candidate variables for the multivariate model. The following variables met this criterion: gestational age, parity, gravidity, multiple gestation, CRIB-II score, infant sex, mode of delivery, number of telephone follow-ups, telephone knowledge test score, participation in offline professional courses, primary milk transporter, stable maternal employment (vs. unemployed), maternal education (college/university degree), and paternal education level (college/university degree and master’s degree or above). These results are shown in Table 2.
Results of Univariate Ordinal Logistic Regression Analysis
Multivariate ordinal logistic regression analysis
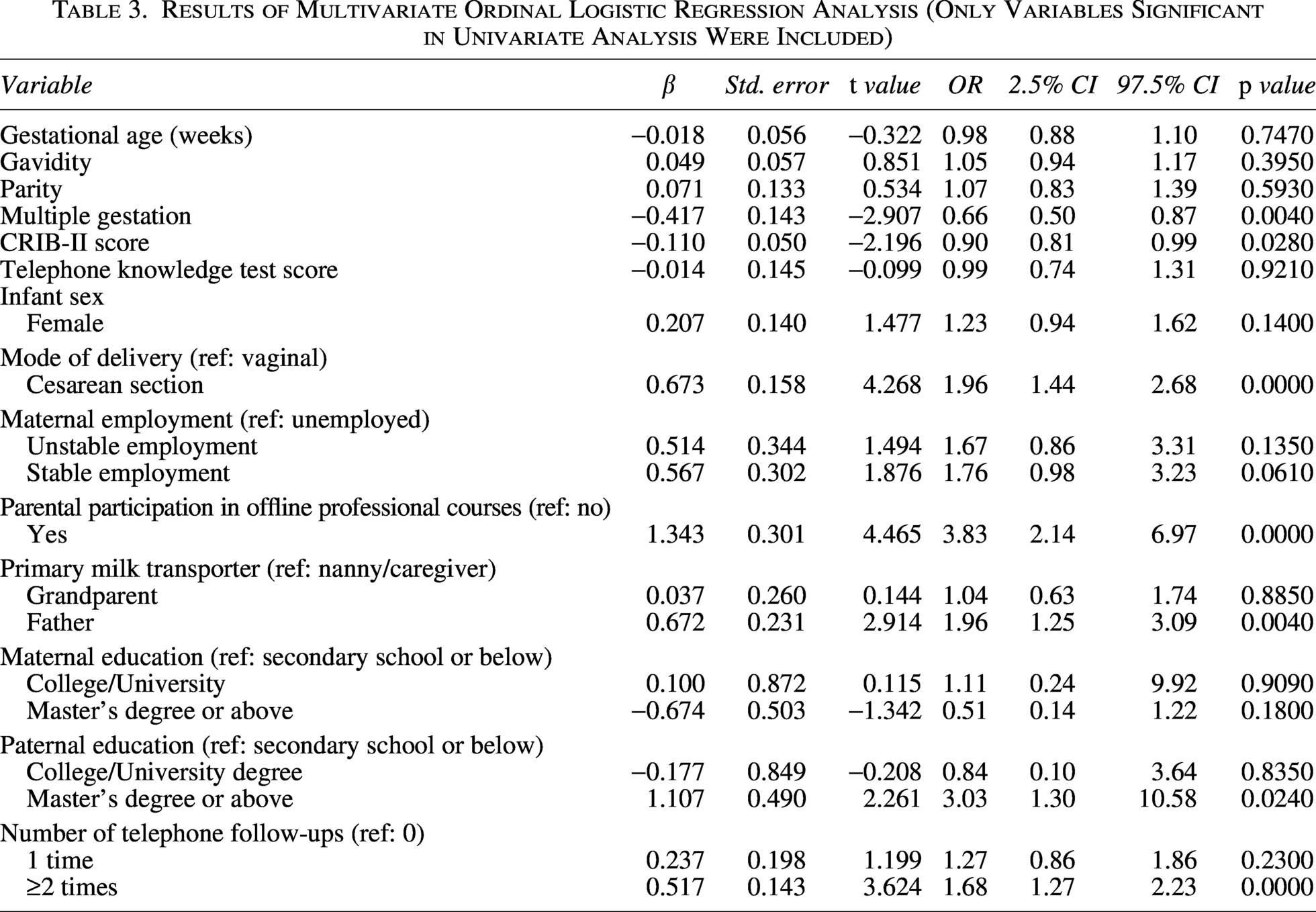
Variables identified as significant in the univariate analysis were incorporated into a multivariate ordinal logistic regression model to identify independent factors influencing the frequency of fresh mother’s own milk feeding during the first 7 days of life (Table 3). Figure 1 provides a forest plot of the independent factors identified in the multivariate analysis (Table 3). The figure visually compares the odds ratios and 95% confidence intervals across neonatal, health care system, and familial factors.
Results of Multivariate Ordinal Logistic Regression Analysis (Only Variables Significant in Univariate Analysis Were Included)
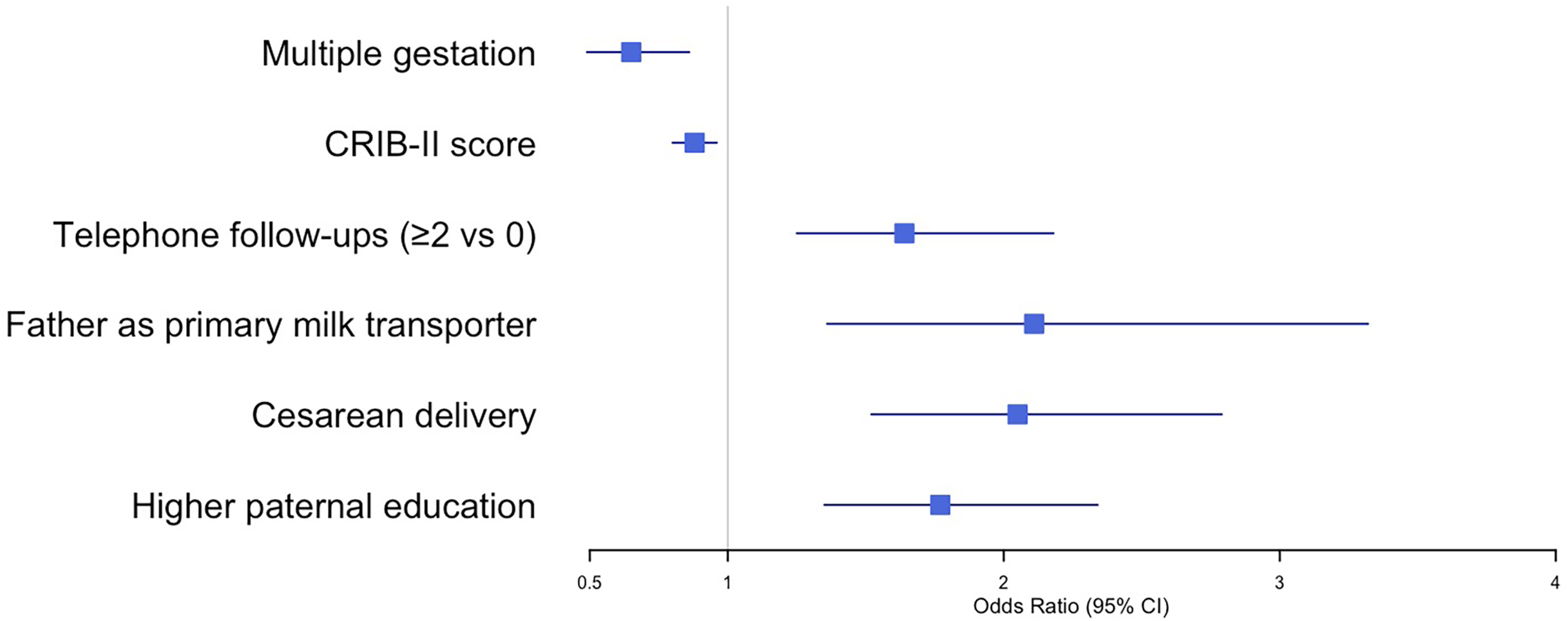
Forest plot of independent factors associated with fresh mother’s own milk feeding frequency (derived from the multivariate ordinal logistic regression model in Table 3). The solid vertical line at OR = 1 indicates the reference line; horizontal lines represent 95% confidence intervals.
Neonatal factors: Multiple gestation was identified as a significant risk factor for reduced feeding frequency (OR = 0.66, 95% CI: 0.50–0.87, p = 0.004). Similarly, a higher CRIB-II score, indicating greater initial illness severity, was independently associated with decreased feeding frequency of fresh mother’s own milk (OR = 0.90, 95% CI: 0.81–0.99, p = 0.028).
Health care system and interventional factors: Structured health care support demonstrated significant protective effects. Participation of both parents in offline professional courses was a strong protective factor (OR = 3.83, 95% CI: 2.14–6.97, p < 0.001). Telephone follow-ups exhibited a clear pattern of benefit: compared with no follow-ups, two or more telephone follow-ups were associated with significantly increased odds of higher feeding frequency (OR = 1.68, 95% CI: 1.27–2.23, p < 0.001).
Social and familial factors: Paternal involvement demonstrated substantial protective effects. When the infant’s father served as the primary milk transporter, compared with a nanny or caregiver, the odds of higher feeding frequency significantly increased (OR = 1.96, 95% CI: 1.25–3.09, p = 0.004). Moreover, a higher paternal education level (Master’s degree or above) was also a significant protective factor compared with secondary education or below (OR = 3.03, 95% CI: 1.30–10.58, p = 0.024).
Delivery-related factors: Cesarean delivery was significantly associated with increased feeding frequency compared with vaginal delivery (OR = 1.96, 95% CI: 1.44–2.68, p < 0.001).
In contrast, gestational age, parity, knowledge test score, primary milk transporter being a nanny/caregiver, and paternal education level (college/university degree) did not demonstrate statistical significance in the final multivariate model (all p > 0.05).
Variable coding
Categorical independent variables were coded as follows: Infant sex (male = 1, female = 2); paternal education level (high school/vocational school or below = 1, college/university degree = 2, master’s degree or above = 3); mode of delivery (vaginal = 1, cesarean section = 2); premature rupture of membranes (no = 0, yes = 1); histological chorioamnionitis (no = 0, yes = 1); other diseases during pregnancy (no = 0, yes = 1); postpartum maternal health (no issues = 0, issues = 1); primary milk transporter (nanny/caregiver = 0, grandparent = 1, father = 2); participation in offline professional courses (no = 0, yes = 1); residence within the province (no = 0, yes = 1); residence within the city (no = 0, yes = 1); rural residence (no = 0, yes = 1); telephone follow-up sessions (0 sessions = 0, 1 session = 1, ≥2 sessions = 2). Continuous variables were entered as their original values.
Discussion
This study provides comprehensive evidence regarding the multidimensional factors influencing the frequency of fresh mother’s own milk feeding in VLBWIs during the critical early postnatal period through multivariate ordinal logistic regression analysis. Our findings not only confirm the significant impact of neonatal biological factors such as illness severity but also highlight the crucial roles of health care system support and paternal involvement in promoting the fresh mother’s own milk feeding. These results offer a robust evidence base for developing precise and systematic nursing intervention strategies.
Neonatal illness severity and multiple gestation as barrier factors
This study identified a higher CRIB-II score and multiple gestation as independent risk factors impeding the achievement of higher feeding frequency of fresh mother’s own milk in VLBWIs, a finding consistent with previous domestic and international research.13,14 The CRIB-II score, an objective indicator of initial illness severity after birth, signifies greater physiological instability and poorer tolerance to early enteral feeding in neonates with higher scores. Furthermore, the closed management model of the NICU prolongs mother–infant separation, directly disrupting key lactation-promoting practices such as early skin-to-skin contact and regular suckling.15,16 Mothers of multiples face higher risks of perinatal complications, earlier delivery, and greater postpartum challenges—including feeding multiple infants and managing time and energy—resulting in significantly increased recovery burden, fatigue, and mother–infant separation stress compared with mothers of singletons.9,17,18 International studies also identify multiples as a high-risk factor for early breastfeeding failure, necessitating more support, which is often not adequately addressed in standard health education programs typically designed for singleton pregnancies.19–22 This underscores the need for clinical nurses to identify mothers of multiples and preterm infants with high CRIB-II scores as high-risk populations, warranting earlier, more proactive breastfeeding support and priority access to a family-integrated NICU environment.
Health care system support as a facilitator
Our results demonstrate that professional nursing interventions and systematic health education function as crucial facilitating factors. Specifically, telephone follow-ups and participation in offline professional courses were strong protective factors associated with increased fresh mother’s own milk feeding. Telephone follow-up, a core component of transitional care, provides timely resolution of family queries, ongoing technical guidance, and emotional support, thereby effectively enhancing parental confidence and capacity to persist with fresh mother’s own milk provision.9,23 Offline professional courses deliver structured, systematic health education, transferring essential knowledge and skills. This format is more effective than fragmented knowledge dissemination. Through hands-on learning and practice, parents can develop a deeper understanding of the importance of early fresh mother’s own milk and master correct expression and storage techniques.24–27 Therefore, clinical nursing practice should prioritize the optimization of health education delivery and content quality, developing well-structured and engaging educational programs that promote active family engagement.
The paternal role in the support system
The familial support system, particularly the role of fathers, warrants greater recognition. This study identified the infant’s father serving as the primary milk transporter and a higher paternal education level as significant protective factors for the mother’s own milk feeding frequency. Active involvement of the father can alleviate maternal caregiving burden and ensure the timely delivery of milk.9,28 Moreover, higher paternal education may be associated with greater receptivity to evidence-based parenting practices, more positive attitudes toward fresh mother’s own milk feeding, and enhanced capacity to provide informed decision-making and practical assistance. 29 Collectively, these efforts contribute to cultivating a family-centered environment that supports the sustained provision of fresh mother’s own milk.
The importance of post-discharge fresh mother’s own milk support
Cesarean delivery emerged as a significant positive factor associated with increased feeding frequency. The underlying mechanism may be attributed to the typically longer postpartum hospitalization following cesarean sections compared with vaginal births, which facilitates more direct and manageable milk transportation logistics during the critical early postnatal period. Notably, residence distance from the hospital demonstrated no statistically significant association with feeding frequency in our analysis, contrasting with some previous findings. 30 This may be explained by our center’s downtown location in Hangzhou, the city’s efficient public transport (including an expanding subway system), and the fact that most mothers were local or long-term residents. Notably, although our center established the first human milk bank in Zhejiang Province in 2016 and offers SF Express courier and volunteer-assisted collection, these services have been limited to refrigerated mother’s own milk (restricted to Zhejiang, Jiangsu, Shanghai, and Anhui) and were not used for fresh milk delivery during the study period. Extending such services to fresh milk in the future could provide additional convenience. These findings collectively highlight the vulnerability of mothers experiencing vaginal birth, who typically face earlier discharge, to disruptions in sustained fresh milk provision. This evidence underscores the urgent need to develop comprehensive support strategies specifically tailored for early-discharged mothers to maintain fresh mother’s own milk feeding.
Limitations and Future Directions
This study has several limitations that should be acknowledged. First, some maternal factors, such as lactational capacity (i.e., the mother’s physiological ability to produce sufficient milk volume to meet the infant’s nutritional needs) and psychological status, were not included in the analysis, which may influence feeding initiation and continuation. Second, while our study focused on the frequency and adequacy of fresh mother’s own milk feedings, we did not analyze the energy content or nutritional composition of the milk provided, which represents an important dimension of infant nutrition. Furthermore, the retrospective design and single-center nature of this research, while providing valuable insights, inherently limit causal inference and generalizability. Future investigations would benefit from prospective multicenter cohort studies incorporating mixed-methods approaches, including qualitative interviews, to explore the complex biological, psychological, and social dimensions of fresh mother’s own milk feeding practices.
Conclusion
This study, utilizing multivariate ordinal logistic regression analysis, has identified key protective and risk factors associated with the frequency of fresh mother’s own milk feeding in VLBWIs during the first critical week of life. The findings demonstrate that:
Multiple gestation and higher CRIB-II scores represent significant barriers to achieving frequent feedings; Telephone follow-ups and structured, offline professional courses are independent and potent protective factors, underscoring the vital importance of specialized, continuous nursing support; Higher paternal education level and active involvement in milk transportation are crucial familial factors supporting the sustained provision of fresh mother’s own milk.
Consequently, we recommend the clinical implementation of an integrated care model founded on risk assessment, driven by systematic intervention, and secured by family support. This model should facilitate the accurate identification of high-risk dyads (e.g., multiples, infants with high illness severity), strengthen the continuity between in-hospital education and post-discharge follow-up, and proactively engage fathers of preterm infants as core participants in health education initiatives. Such a multidimensional approach is essential for effectively promoting the successful establishment and maintenance of fresh mother’s own milk feeding in this vulnerable population.
Authors’ Contributions
H.D. and L.Z.: Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; H.D.: Involved in drafting the article or revising it critically for important intellectual content; H.D., L.Z., W.Z., and Q.L.: Given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content; H.D., L.Z., W.Z., and Q.L.: Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data Availability Statement
The data are available on reasonable request from the corresponding author.
Ethics Approval Statement
Ethical approval was obtained from the Ethics Committee of Women’s Hospital, School of Medicine, Zhejiang University (Approval No.: IRB-20240072-R). All methods that we used adhered to the accepted guidelines for ethical reporting.
Declarations
There is a statistician on the author team, Longfei Zhang. The authors confirm that the data analysis methods were appropriate for their study design and context and that the statistical findings were properly implemented and interpreted. Each author has read and approved the final version submitted.
Footnotes
Acknowledgments
We sincerely acknowledge the Medical Records and Informatics Department of Zhejiang University Women’s Hospital for their expert data stewardship. We also appreciate the support of the funds. We extend gratitude to the critical contribution of anonymized clinical data that enabled this analysis while ensuring patient confidentiality.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The project was supported by Scientific Research Fund of Zhejiang Provincial Education Department (Grant No. Y202454811) and Zhejiang Provincial Hospital Sustainable Development Yangtze River Research Project (Grant No. 2024ZHA-YZJ211), Zhejiang Provincial Disease Control Science and Technology Plan (2025JK223), and the Open Research Fund of Zhejiang Key Laboratory of Maternal and Infant Health, Women’s Hospital, Zhejiang University School of Medicine (Project Title: Detection of Organic Pesticide Residues in Breast Milk and Risk Assessment of Infant Exposure in Zhejiang Province).