
Abstract
Objectives
Routine imaging modalities combined with state-of-the-art reconstruction software can substantially improve preoperative planning and simplify complex procedure by enhancing the surgeon’s knowledge of the patient’s specific anatomy. The aim of the current study was to demonstrate the feasibility of interactive three-dimensional (3D) computed tomography (CT) reconstructions for preoperative planning and intraoperative guiding in video-assisted thoracoscopic lung surgery (VATS) with 3D vision.
Methods
Twenty-five consecutive patients referred for an anatomic pulmonary resection by a single surgeon were included. Data were collected prospectively. All patients underwent a CT angiography in the diagnostic pathway prior to referral. 3D reconstruction of the pulmonary anatomy was obtained from CT scans with dedicated software. An interactive PDF file of the 3D reconstruction with virtual resection was created, in which all the pulmonary structures could be individually selected. Furthermore, the reconstructions were used for intraoperative guiding on double monitor during VATS with 3D vision.
Results
In total, 26 procedures were performed for 5 benign and 21 malignant conditions. Lobectomy and segmentectomy were performed in 20 (76.9 %) and 6 (23.1%) cases, respectively. In all patients, preoperative 3D reconstruction of pulmonary vessels corresponded with the intraoperative findings. Reconstructions revealed anatomic variations in 4 (15.4%) patients. No conversion to thoracotomy or in-hospital mortality occurred.
Conclusions
Preoperative planning with interactive 3D CT reconstruction is a useful method to enhance the surgeon’s knowledge of the patient’s specific anatomy and to reveal anatomic variations. Intraoperative 3D guiding in VATS with 3D vision is feasible and could contribute to the safety and accuracy of anatomic resection.
Keywords
Introduction
The number of pulmonary resections have increased over recent years and are nowadays included in the standard of care of malignant and benign lesions of the lung. Initially, lung surgery was approached through a conventional thoracotomy; however, the introduction of video-assisted thoracic surgery (VATS) provided a minimally invasive surgical alternative for the treatment of lung cancer, benign tumors, and other lung pathology. In many high-volume centers, VATS has been adopted as the preferred approach over thoracotomy due to favorable morbidity and improved survival rates. In patients with non-small cell lung carcinoma, surgical resection with a systematic mediastinal lymph node dissection remains a cornerstone for treatment. Lobectomy, either through thoracotomy or VATS, constitutes the basis of these surgical resections. 1 However, for patients with early-staged lung cancer, sublobar resections, like segmentectomy, could be considered, especially for patients with impaired pulmonary function.2–4 In comparison with lobectomy, sublobar resections are considered technically more challenging due to their high complexity. Moreover, obtaining an adequate surgical margin in anatomic segmentectomy is crucial for prevention of recurrence. 5
Computed tomography (CT) is still the gold standard for imaging of the chest and is combined with positron emission tomography (PET), a mandatory step in the diagnostic pathway for lung cancer. The use of multiple detector CT angiography in preoperative diagnostics has increased spatial resolution and reduced radiation exposure compared to older CT modalities. Routine imaging modalities combined with state-of-the-art reconstruction software can substantially improve preoperative surgical planning and simplify complex procedure by enhancing the surgeon’s knowledge of the patient’s specific anatomy. 6 In the literature, several anatomic variations in pulmonary arteries, veins, and the bronchial tree are described.7,8 Several studies have indicated that CT pulmonary angiography can correctly identify pulmonary structures with an accuracy up to 98%.9–11 As many variations in pulmonary arteries and veins exist, detailed preoperative understanding of the patient’s specific anatomy could contribute to safely performing lung surgery and could prevent perioperative complications, like intraoperative bleeding. Furthermore, detailed anatomical delineation of the tumor allows surgeons to perform radical resections in anatomic segmentectomy or lobectomy, instead of more invasive pneumonectomy.
The current study demonstrates the feasibility of interactive 3D CT reconstructions for preoperative planning in VATS. Additionally, we provide a surgical setup for intraoperative 3D guiding with the use of 3D vision.
Methods
Patient Selection
The first 25 consecutive patients referred for pulmonary resection were included prospectively. Baseline data, including CT scans with 3D reconstructions, and intraoperative data, including intraoperative video recordings, were collected prospectively. In total, 26 operations for benign and malignant conditions with the use of intraoperative 3D guiding by a single surgeon (PSN) at our tertiary referral center were included. Patients referred for oncologic resection were primarily discussed in our oncologic multidisciplinary team, and in selected patients prior to surgery, mediastinal lymphadenectomy was performed for staging.
CT and 3D Reconstruction
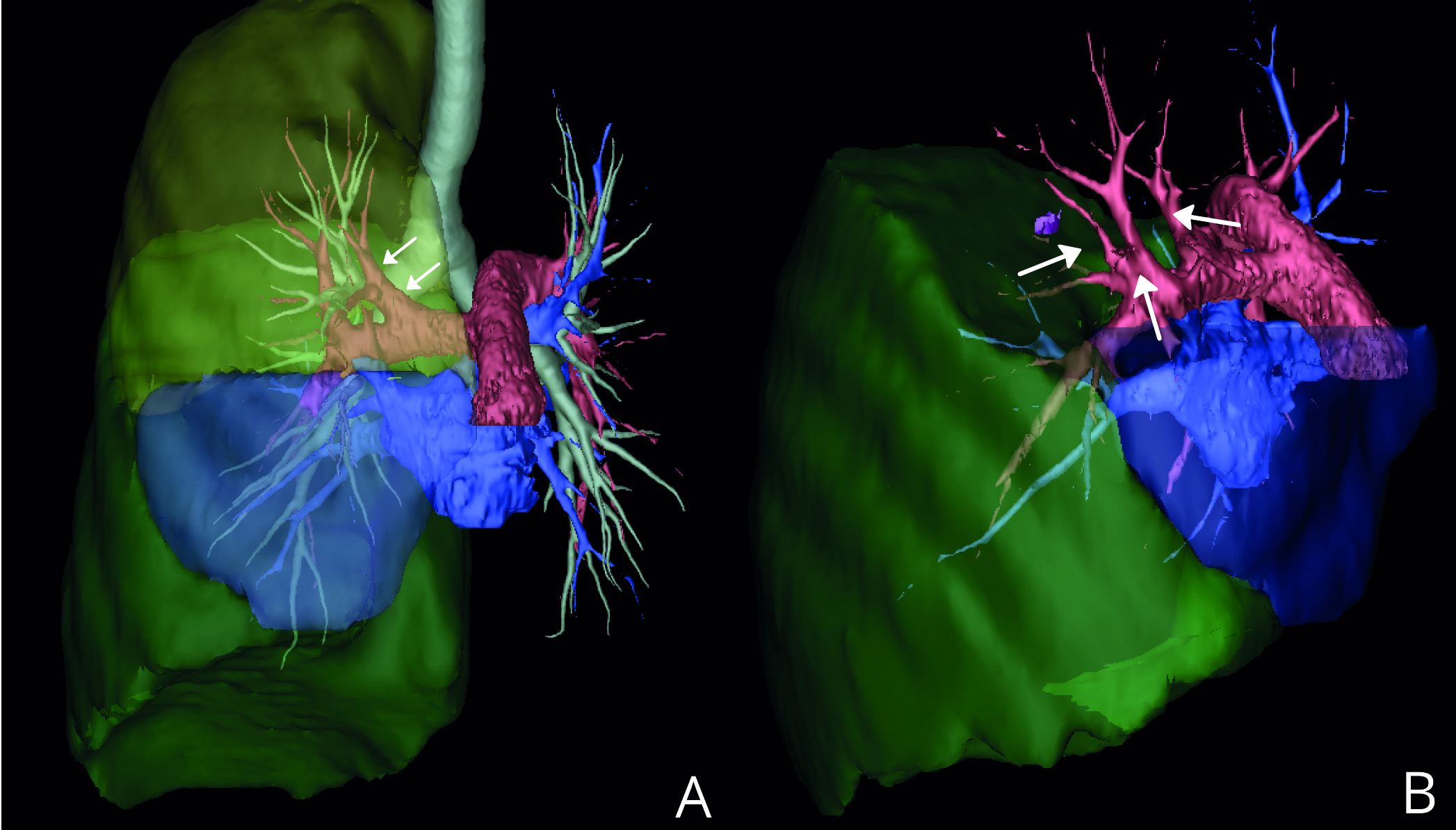
In all patients, multidetector CT angiography during the preoperative diagnostic pathway was realized using a third-generation dual source CT scanner (Somatom Force, Siemens Healthineers, Forchheim, Germany) and iopromide as contrast agent (300-mg iodine/mL, Ultravist, Bayer, Berlin, Germany). Primary indication for chest CT were suspected lesions on chest X-ray in 11 patients, hemoptysis in 1 patient, and to rule out pulmonary embolism in 2 patients. In 3 patients, a chest CT was made during follow-up of other treated malignancies. A total of 6 patients were known with lung pathology requiring follow-up with CT. In 2 patients, a contrast-enhanced chest CT was made for other thoracic disease, with an incidental finding of a suspected lesion. In none of the patients, an additional CT, with solely the goal of preoperative planning, was made. Digital Imaging and Communications in Medicine (DICOM) data were transferred to a dedicated workstation. Based on contrast-enhanced CT images, 3D volume rendering was performed using Fujifilm Synapse Vincent system (Fujifilm Corporation, Tokyo, Japan). For 3D reconstructions, contrast-enhanced CT images with a slice thickness of 2 mm or less were used for optimal results. Lung reconstruction was performed by extracting and segmenting the territories of pulmonary vessels and bronchi. 12 The use of contrast agent, in combination with the right timing of the contrast, allows the system to automatically perform 3D reconstructions of the pulmonary arteries and veins (Fig. 1). Additionally, an extraction of the tumor with volume calculation, thoracic cage, and virtual simulation of pulmonary resections were performed to visualize the resection surface and the extent of the surgical margin (Supplemental Video 1). For each patient the 3D reconstruction and virtual simulation of the resection was saved onto an interactive PDF file, in which all the pulmonary structures could be individually selected (Fig. 2). All the reconstructions were performed by the operating surgeon and took between 5 and 10 minutes to construct.
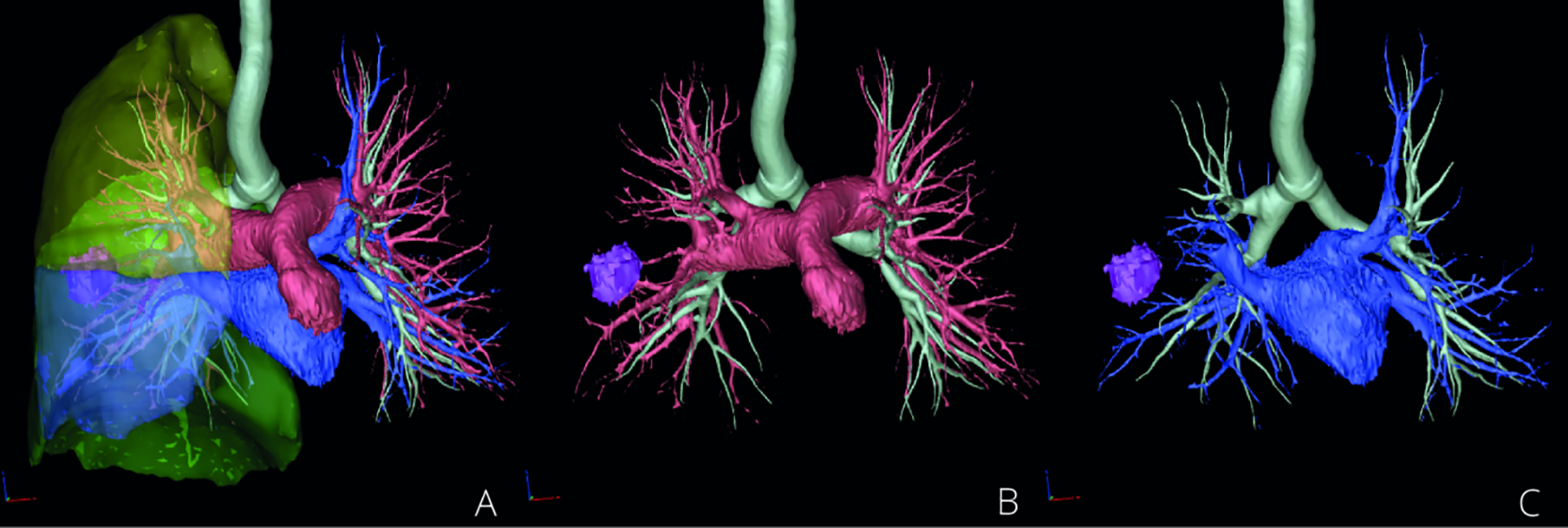
(a) Three-dimensional (3D) lung reconstruction. (b) Visualization of the arterial vessels. (c) Visualization of venous system.
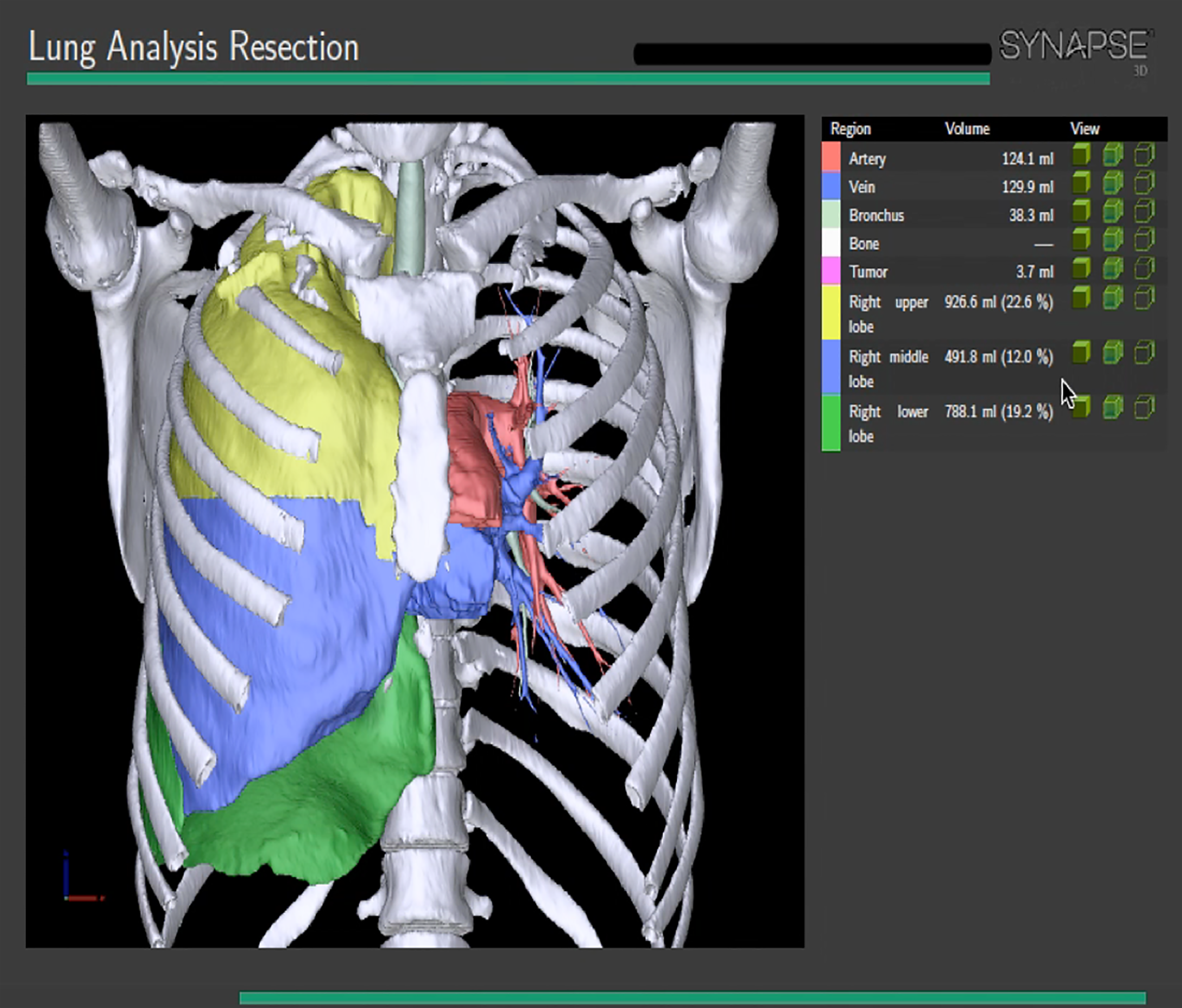
Interactive PDF file of three-dimensional (3D) lung reconstruction.
Surgical Approach
Patients underwent surgery under general anesthesia with single-lung ventilation with the patients in lateral decubitus. For all patients two ports were used, one working port of 3 to 4 cm and one 10-mm camera port for 3D endoscopic camera. Based on CT reconstruction and depending on tumor location, the utilization port was made in most cases in the anterior axillary line of the fourth or fifth intercostal space. Only a soft tissue retractor was used. For lobectomy, the anterior approach was used. Two monitors were placed in front of the surgeon displaying the intraoperative video on one screen and the interactive preoperative 3D reconstruction on the other (Fig. 3). To enable in-depth vision, surgeons wore polarized 3D glasses. The pulmonary arteries, veins, and the bronchus are individually dissected and ligated with the use of automated staplers. In patients operated for lung cancer, a systematic lymph node dissection was performed.

Intraoperative setup with dual monitors. The left monitor displays the preoperative three-dimensional (3D) reconstruction. The right monitor displays the intraoperative 3D imaging. Surgeon wears 3D glasses for in-depth visualization.
Endpoints and Statistics
The current prospective single-center, single-arm study focuses on preoperative planning to safely perform VATS and optimize surgical results. Endpoints for procedural results were defined as radical resection, number of lymph nodes dissected, and procedural time. Endpoints for surgical safety were defined as adverse events grade ≤2 prior to discharge according to the Clavien–Dindo classification. 13 Summary statistics were obtained using SPSS 24.0 for Macintosh (SPSS Inc., Chicago, IL, USA). Frequencies are presented as absolute numbers and percentages. Continuous data are presented as mean with standard deviation and nonparametric data as median with interquartile range.
Results
Baseline Characteristics
A total of 26 operations, performed in 25 patients, were included. In 1 patient, an anatomic segmentectomy was performed in staged fashion at right and left lung. Median age was 62.5 [57.8, 70.0] and 15 patients (57.7 %) were female. Mean body mass index was 23.6 ± 3.4. In 2 patients (7.6%), World Health Organization performance score was ≥2. Mean forced expiratory volume in 1 second was 2.5 ± .8 L. Further characteristics are depicted in Table 1.
Preoperative Baseline Characteristics and Comorbidities.
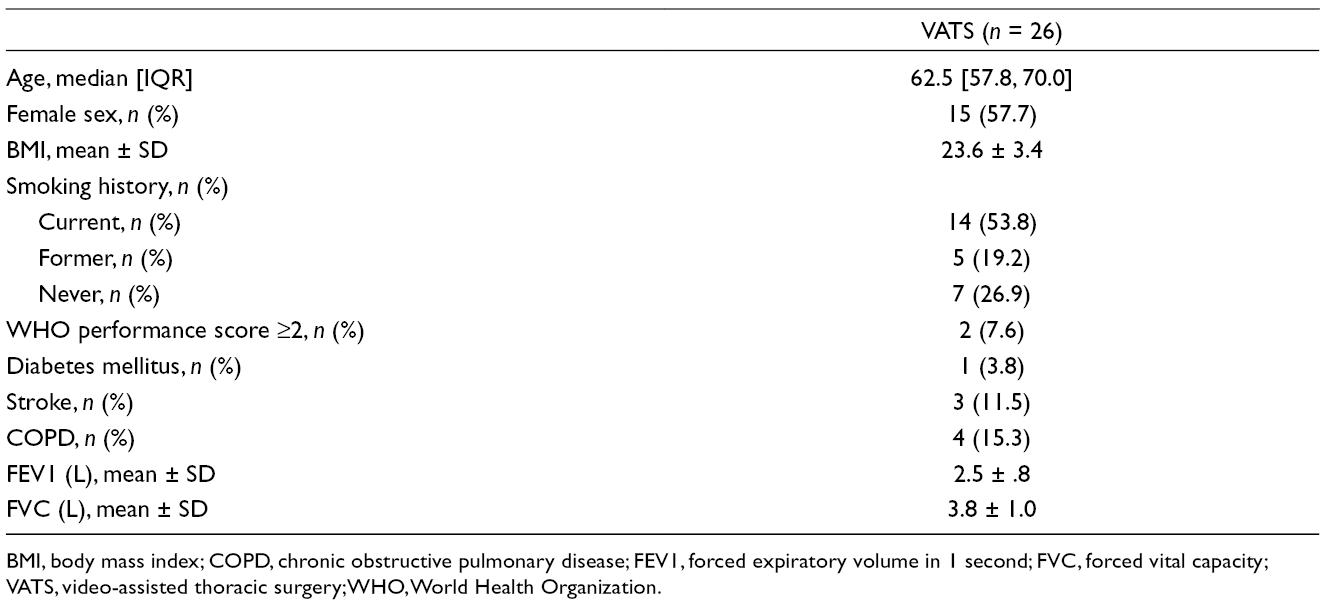
BMI, body mass index; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; VATS, video-assisted thoracic surgery; WHO, World Health Organization.
Surgical Procedure
Indication for surgery were emphysema (n = 1), bronchiectasis (n = 1), primary ciliary dyskinesia (n = 1), and suspected malignant lesions (n = 23). In total, 16 patients were operated for right-sided lung pathology, 8 for left-sided pathology, and 1 patient was operated for both left- and right-sided pathology as mentioned earlier. Lobectomy was performed in 19 (73.1 %) cases, bilobectomy in 1 (3.8%) case, and anatomic segmentectomy in 6 (23.1%) cases. Mean procedural time was 218 ± 56 minutes. In oncologic resection, median number of dissected lymph node stations was 65,6 with a mean number of 8 ± 3 lymph nodes per patient. Surgical procedural details are depicted in Table 2.
Perioperative Data.
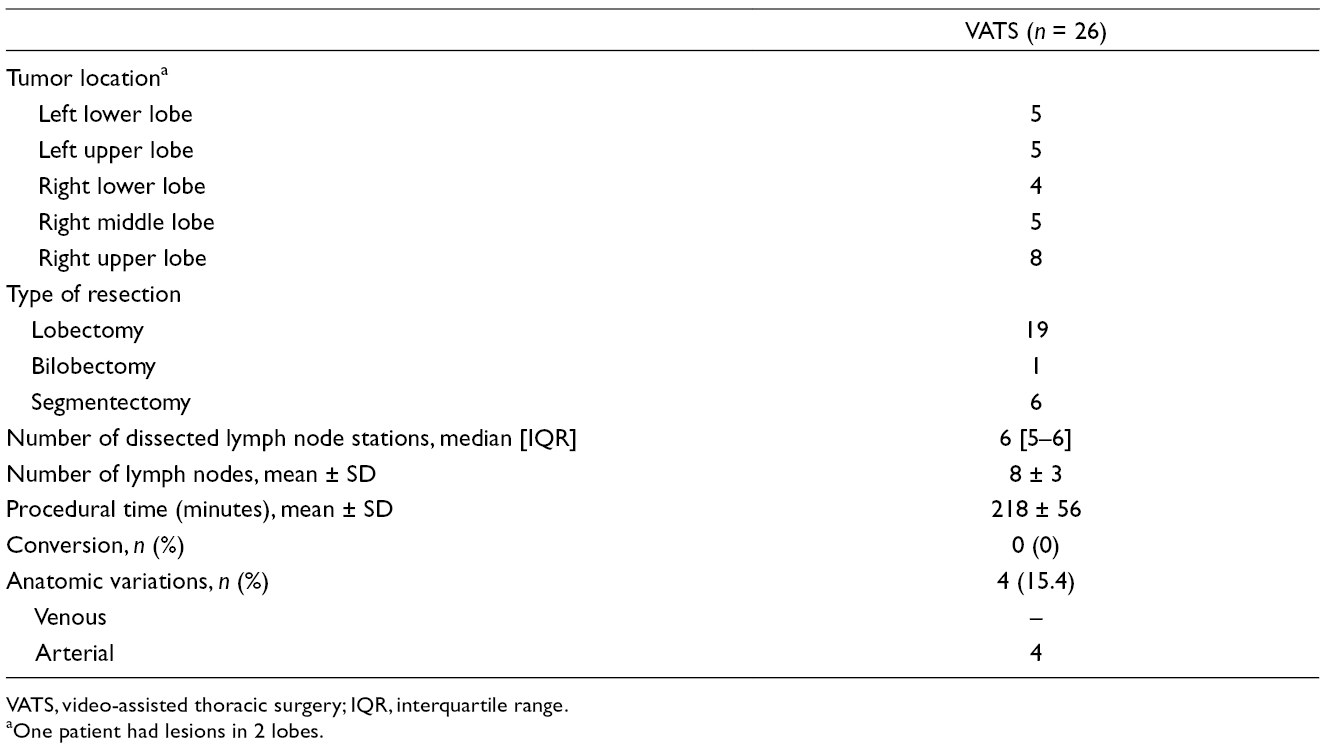
VATS, video-assisted thoracic surgery; IQR, interquartile range.
Pathology
Benign lung pathology was found in 5 patients, including 1 patient referred for a suspected lesion in the right upper lobe. Preoperative diagnostic pathway suspected a malignant lesion, but because of deep tumor location, no histologic confirmation could be realized; therefore, a resection of the suspected lesion was performed. Postoperative pathological examination revealed no malignant disease. In 21 patients, non-small cell lung carcinoma was found, and pathological examination revealed adenocarcinoma in 17 patients and squamous cell carcinoma in 3 patients. In 1 patient, a carcinoid tumor was found. Median tumor size was 27 mm [15–45]. In 8 patients (38.1%), pleural invasion was present. In all patients, a complete (R0) resection was performed. Postoperative staging was performed according to the eighth edition of the TNM Classification of Malignant Tumours and is depicted in Table 3. 14
Pathology.
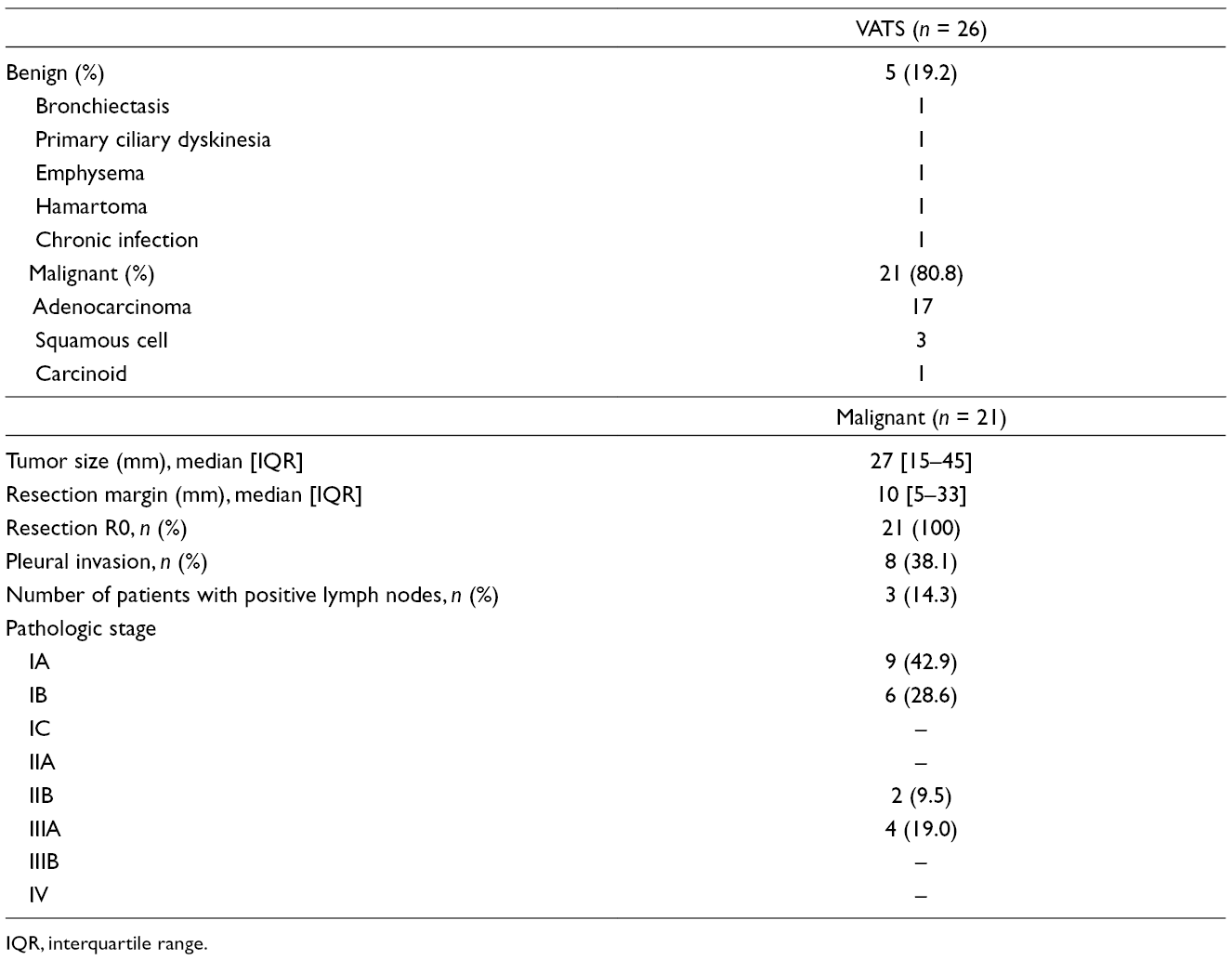
IQR, interquartile range.
Postoperative Complications
Postprocedural complications were grade ≤2 in 96.2% of patients. Only 1 patient had grade IVa complication due to ischemic stroke. Outpatient clinical follow-up at 5 months revealed full recovery. Prolonged air leak without indication for intervention was found in 4 patients and hospital-acquired pneumonia occurred in 6 patients. Clinical postoperative data are summarized in Table 4.
Postoperative Data.
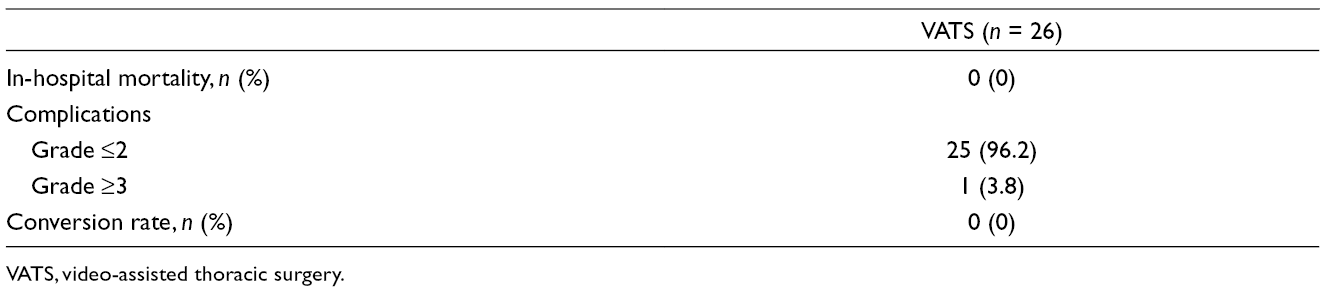
VATS, video-assisted thoracic surgery.
Anatomic Variation
The preoperative 3D reconstruction of pulmonary vessels and intraoperative guiding corresponded to intraoperative findings in 100% of cases. In 4 (15.4%) patients, anatomic variations were found on preoperative 3D reconstruction and were confirmed intraoperative. Variations included four arterial anomalies. In 3 patients, an early debranching of the truncus superior was found (Fig. 4a). Additionally, in 1 of these patients, an additional right posterior segment artery was found (Fig. 4b). Furthermore, in 1 patient, an additional left anterior basal segmental artery was found. An example of anatomic variation is displayed in Supplemental Video 2.
(a) Early debranching of the truncus superior. (b) Duplicate right posterior segment artery.
Discussion
In this preliminary study, we present our method of preoperative planning and the feasibility of intraoperative guiding based on high-quality 3D lung reconstructions. All reconstructions were made from conventional diagnostic CT images with the use of dedicated reconstruction software. The 3D reconstructions were used in various settings for planning of both benign and (suspected) malignant resections. All patients were operated through two-port VATS with 3D vision without conversion to thoracotomy. In all patients operated for lung cancer, a radical resection with full systematic resection of all associated lymph node stations was performed. In the operating room, two monitors allowed the surgeon to review the vascularity and bronchial tree intraoperative in 360° next to the intraoperative imaging.
The safety and efficacy of CT angiography for preoperative assessment for thoracic surgery has already been described.15,16 All patients underwent CT imaging of the chest during initial preoperative diagnostic evaluation before referral for surgery. As all reconstructions were based on diagnostic CT images, no additional CT scanning solely for preoperative planning was necessary. As a result, unnecessary exposure to radiation and the risk of contrast-induced nephropathy was ruled out. Furthermore, additional health-care costs could be avoided.
The possibility to depict a patient’s individual pulmonary anatomy with high accuracy will greatly contribute to the safety and accuracy of lung surgery, especially in sublobar resections. Within minutes, the dedicated software automatically generates a 3D reconstruction of the pulmonary structures for surgical simulation. The 3D reconstructions can be transferred to an interactive PDF file for use in the operating room for intraoperative guiding. Additionally, 3D guiding intraoperative will be helpful to obtain an adequate margin as the distance between the tumor and surgical resection can be calculated. A possible disadvantage of automatically generated 3D image reconstructions could be potential identification of nonexisting structures owing to complex anatomical overlap. However, previous studies have demonstrated an excellent accuracy of CT and use in preoperative planning.
Conversion rates for VATS to thoracotomy for anatomical resection vary in worldwide literature between 7.0% and 10.3%.17,18 The Dutch Lung Surgery Audit from 2013 to 2015 reported a conversion rate between 8.8% and 10.9%. 19 In most cases bleeding from main pulmonary vessels is the main reason for conversion with rates up to 29%. 20 Additionally, bleeding after VATS is also of clinical importance with an incidence between 0.5% and 1.9%.21,22 As many variations in pulmonary anatomy exist, preoperative knowledge could prevent intraoperative bleeding complications with the necessity for conversion. Furthermore, we found a high percentage of anatomic variations in line with variations described in literature.
Multidisciplinary care teams have already proved their survival benefit for patients with cancer.23,24 However, the evidence for a survival benefit from multidisciplinary care teams in lung cancer is limited. 25 Preoperative depiction of patients’ individual anatomy, tumor size, and tumor location could be beneficial for assessment of surgical resectability in clinical multidisciplinary decision making in oncologic teams and could help improve patient survival rates. Additionally, 3D reconstructions can help residents and medical students to study lung anatomy.
Preoperative planning could play an important role in reducing intraoperative complications. Additionally, for the preoperative planning, we adapted our surgical setup with dual monitors, with one screen displaying the intraoperative 3D video and the other screen, the 3D reconstruction. In the literature, shorter operation times, less blood loss, and shorter postoperative drainage times have all been attributed to the use of 3D vision in VATS. In the current study both novelties were introduced; therefore, the true effect of preoperative planning could not be investigated. We can only postulate that both technologies, in combination, could be beneficial for patients. Currently, our operational setup requires an assistant to manually rotate the reconstruction in three dimensions on the computer connected to the screen in front of the surgeon. In the future, a possible solution could be the use of virtual navigation based on anatomical landmarks recognized by the system with automatic rotation in real time with movement of the instruments, like in neuro-navigation. Furthermore, in robotic surgery, the TilePro display, displaying the 3D surgical navigation, could be helpful to surgeons and could overcome the need for an assistant.
We recognize the relatively small sample size in our current study. However, the objective of the study was only to investigate the feasibility of advanced imagining techniques and the study was not designed to compare the use of intraoperative 3D guiding with the conventional approach. However, the currently study shows the possibilities of the system in different lung pathologies and pulmonary resections, both in malignant and nonmalignant disease. Further studies are warranted to determine whether preoperative 3D reconstruction and intraoperative 3D guiding have an objective effect on short-term and long-term morbidity and mortality.
Conclusions
The current study demonstrates the feasibility of preoperative planning for VATS lung surgery using CT-based 3D reconstructions for the assessment of pulmonary anatomy. Additionally, a new surgical setup with intraoperative 3D guiding with 3D vision was demonstrated for anatomic lobar and sublobar pulmonary resections. The use of intraoperative 3D guiding could contribute to the safety and accuracy of anatomical resections through VATS by enhancing the surgeon’s knowledge on the patient’s individual lung anatomy. Further studies are warranted to investigate the role of intraoperative 3D guiding for prevention of complications and improvement of complete resections in lung cancer, especially in sublobar resections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peyman Sardari Nia, MD, PhD, is a consultant to Fujifilm Corp., Tokyo, Japan, Jules R Olsthoorn, BSc, Samuel Heuts, MD, and Jos G. Maessen, MD, PhD, have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.