
Abstract
Objective
The transapical (TA) approach is an alternative access technique for transcatheter aortic valve replacement (TAVR) in patients with symptomatic aortic valve stenosis. The impact of prior coronary artery bypass graft (CABG) surgery and how it affects left ventricular function recovery is not well defined.
Methods
Patients who had TAVR at a single center between June 2012 and December 2016 were reviewed. High-risk patients who underwent the procedure via a TA approach were divided into 2 groups based on their history of CABG surgery. Postoperative outcomes were compared between groups. CABG/TA-TAVR patients were subdivided into 2 per baseline left ventricular ejection fraction (LVEF) <50%. The changes in LVEF and valve function at follow-up (1 to 12 months) were analyzed using paired t-tests.
Results
Of 923 cases in total, 183 (19.8%) were performed via a TA approach. The mean ± SD Society of Thoracic Surgeons risk score of TA patients was 10.2 ± 4.6. Forty-nine (27%) had a surgical history of CABG. Overall all-cause mortality rates at 30 days, 1 year, and 2 years were similar for both groups (P = 0.59, P = 0.64, P = 0.78). Subgrouping of CABG-TAVR patients (n = 49) identified 24 patients (49%) with LVEF ≥50% vs. 25 (51%) with LVEF <50%. At 1-year follow-up, significant improvements in LVEF (low LVEF group) and valve function for both groups were observed. LVEF ≥50% group (LVEF: ∆: −3%, P = 0.878; aortic valve area [AVA]: ∆: 1.3 cm2, P < 0.001; mean gradient: ∆: −38 mmHg, P < 0.001); LVEF <50% group (LVEF: ∆: 10%, P = 0.01; AVA: ∆: 1.3 cm2, P < 0.001; MG: ∆: −31 mmHg, P < 0.001).
Conclusions
TA-TAVR can be safely performed with acceptable postoperative outcomes in patients with a history of CABG surgery. In those with reduced EF, significant improvements in LV and valve functions are seen at 1-year follow-up.
Keywords
Introduction
Transcatheter aortic valve replacement (TAVR) is an accepted treatment option for aortic stenosis (AS) patients deemed high or intermediate risk for conventional surgical AVR. 1 In addition to the noninferior and superior outcomes after TAVR compared to surgical aortic valve replacement (SAVR), several surgical scenarios such as redo surgery have become preferential indications for TAVR. For AS patients with a history of coronary artery bypass graft (CABG) surgery, TAVR will obviate the need for redo-sternotomy.
Previous retrospective studies evaluating the results of TAVR in patients with prior CABG have reported better outcome with transapical TAVR (TA-TAVR) compared with SAVR. 2 -4 Moreover, results from a multicenter Italian registry of TA-TAVR have shown excellent outcomes in several redo scenarios. 3 While a retrograde transfemoral approach in TAVR is often preferred due to its less invasive nature, a TA-TAVR approach is a viable option in patients with inadequate iliofemoral access.
Theoretically, it can be assumed that manipulation of the left ventricular (LV) apex will worsen the functioning of an already suffering LV myocardium especially in AS patients with a history of CABG surgery. Purse-string sutures and perforation of the ventricular wall by the needle and by the device delivery system can lead to myocardial damage, but this degree of myocardial dysfunction may be outweighed by the afterload reduction thus leading to LV function recovery after TA-TAVR. The purpose of the present study is to describe outcomes in patients after a TA-TAVR with a previous CABG surgery, report the incidence of low left ventricular ejection fraction (LVEF), and assess LVEF recovery in those with LV dysfunction.
Methods
A prospectively maintained institutional review board-approved database was queried for data on all patients who had TAVR through a trans-apical approach at a single institution between May 2012 and June 2016. All patients met the criteria for severe AS, as defined by the American College of Cardiology/American Heart Association guidelines. 1 A complete assessment of patients was performed by at least 2 surgeons and an interventional cardiologist independently. Patients who were deemed as noneligible for an SAVR due to their high surgical risk and worse frailty status were recommended a TAVR. A TA approach for TAVR was chosen for patients with inadequate iliofemoral access.
Patients were initially divided into 2 groups based on their history of CABG surgery. Pre and postoperative clinical and echocardiographic data of patients were collected and compared among patient groups. Data collected included baseline clinical and demographics, periprocedural and postoperative follow-up. Patient comorbidities were obtained by using the definitions provided by the Society of Thoracic Surgeons (STS) data collection system. Study participants who had a history of CABG were further categorized based on their baseline LVEF (LVEF <50% vs. LVEF ≥50%).
Outcome measures consisted of variables defined by the Valve Academic Research Consortium-2 criteria. 5 Operative outcomes were compared between those with a history of CABG and those with none and also for patients with a history of CABG surgery stratified by LVEF. Among those with a history of CABG, the outcomes of interest were the change in LVEF and valve function post-implant and at follow-up.
Statistical Analysis
For clinical data, continuous variables were reported as mean ± SD and compared by using analysis of variance or the Wilcoxon rank sum test when noted. Categorical variables were reported as percentages and numbers and compared using the chi-squared or Fisher’s exact test. Baseline and postoperative 30-day echocardiographic parameters within each group were compared by using paired Student’s t-tests.
For survival analysis, all-cause mortality was the primary outcome of interest. All patients, including those lost to follow-up or alive at last follow-up, were censored on the day of last known follow-up. The incidence rate of death was calculated at assigned time intervals (30 days, 1 year, and 2 years). Kaplan-Meier survival curves and the log-rank tests were used to estimate and compare survival between patient groups. All statistical analyses were performed using the JMP Version 10.0 software (SAS Institute, Inc., Cary, NC, USA). A 2-sided P-value less than 0.05 was considered as statistically significant.
Results
During the study period, 183 patients (female = 99 [54%]) had TAVR via a TA approach at a single center. Forty-nine patients (27%) had a history of CABG. The mean STS score for the entire cohort was 9.6 ± 5.9 and similar across both patient groups.
Shown in Table 1 is a comparison of baseline clinical and echocardiographic characteristics of patients stratified according to a history of CABG. Except for a higher incidence of dyslipidemia among the groups with a history of CABG, all other baseline characteristics were comparable. The mean LVEF of the group with a history of CABG was 48% compared to a mean LVEF of 52% in the group with no history of CABG. Among CABG patients with EF <50%, the distribution was as follows: EF 40% to 50% (n = 9), EF 30% to 39% (n = 10), and EF <30% (n = 6), respectively. Although the incidence of postoperative complications in the group with no history of CABG was higher, these differences did not reach statistical significance (Table 2). Overall all-cause mortality rates at 30 days, 1 year, and 2 years were similar for both groups (P = 0.59, P = 0.64, P = 0.78) (Table 2). After a median follow-up of 25 months, survival was comparable in both groups (Fig. 1) (log-rank test: P = 0.495).
Baseline Clinical and Demographic Characteristics of Transapical Transcatheter Aortic Valve Replacement Patients Based on a History of CABG.
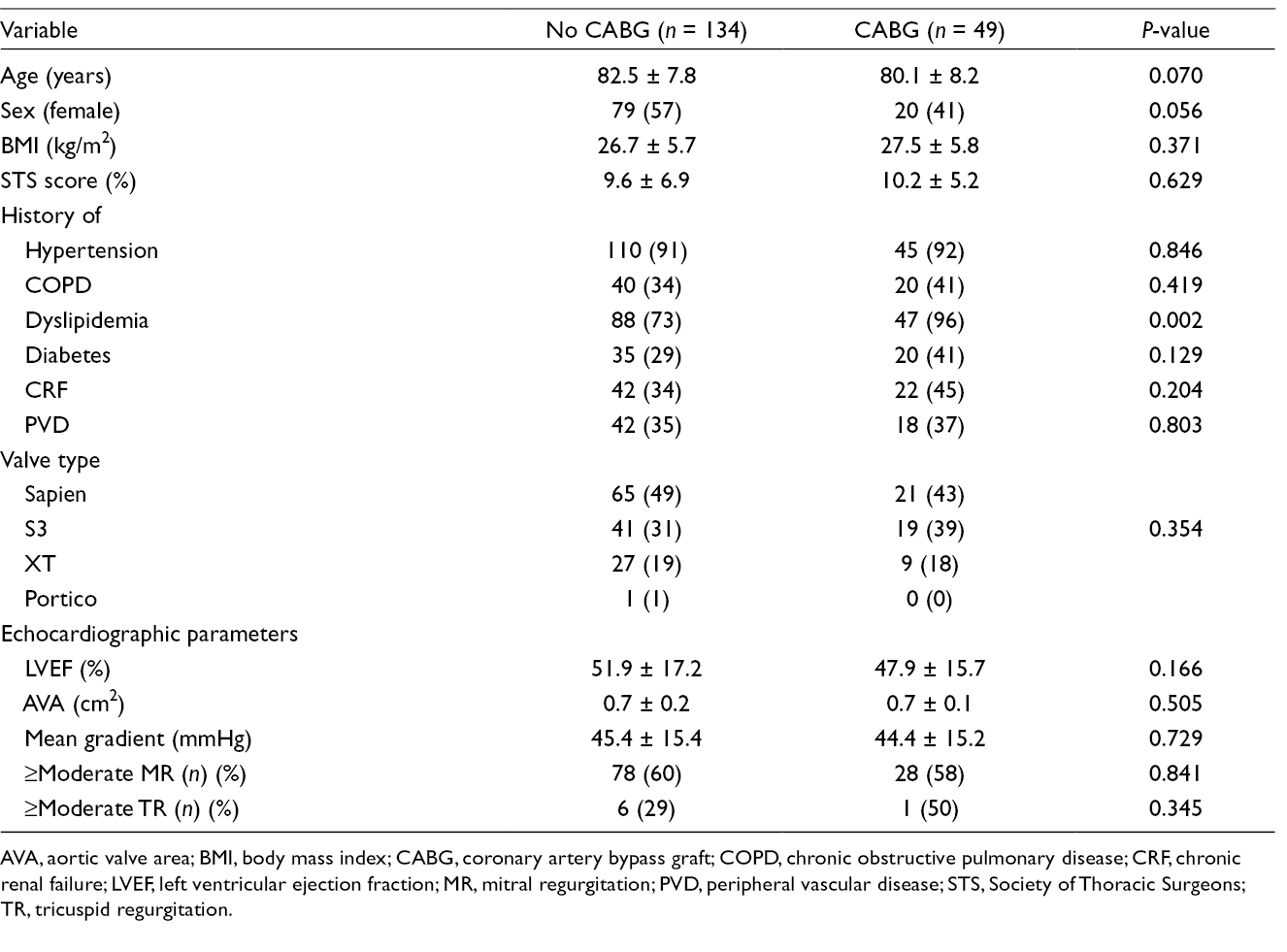
AVA, aortic valve area; BMI, body mass index; CABG, coronary artery bypass graft; COPD, chronic obstructive pulmonary disease; CRF, chronic renal failure; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; PVD, peripheral vascular disease; STS, Society of Thoracic Surgeons; TR, tricuspid regurgitation.
Operative Outcomes After Transapical Transcatheter Aortic Valve Replacement.
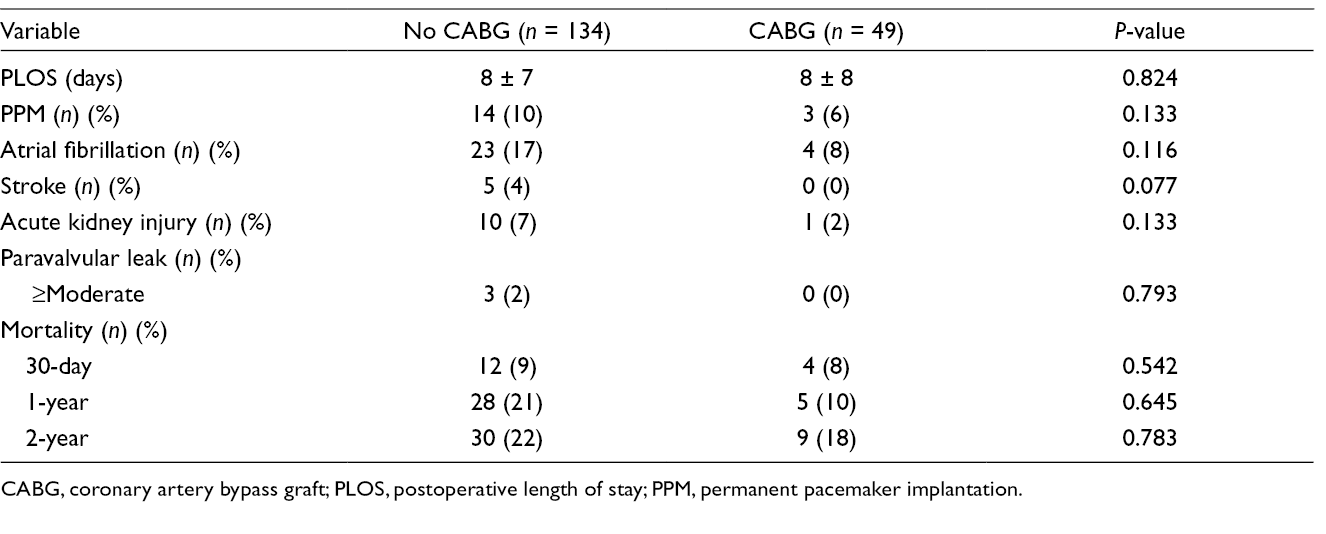
CABG, coronary artery bypass graft; PLOS, postoperative length of stay; PPM, permanent pacemaker implantation.
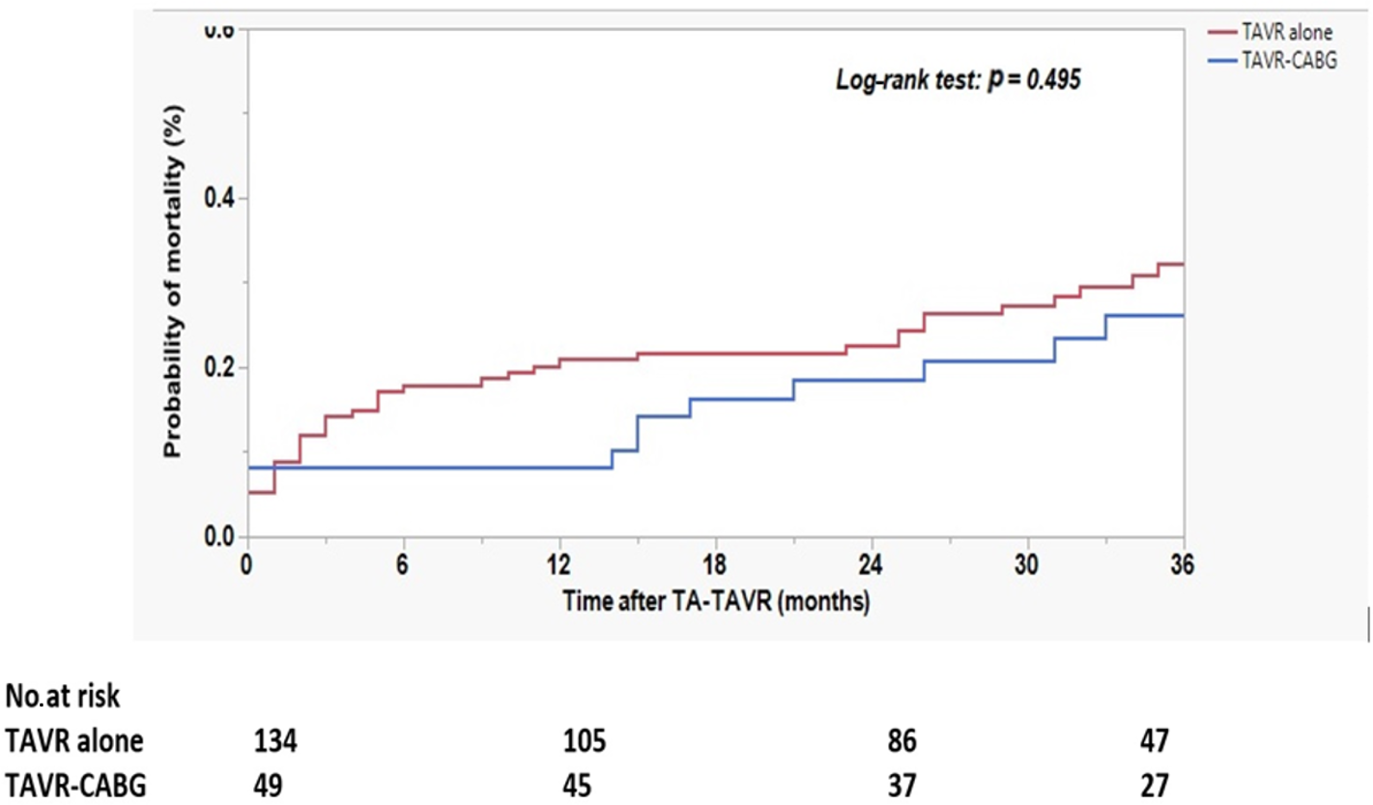
Kaplan-Meier survival curves comparing survival in patients with a history of CABG to those with no prior CABG. CABG, coronary artery bypass graft; TA-TAVR, transapical transcatheter aortic valve replacement.
Out of the 49 TAVR-CABG patients, 25 (51%) had a baseline LVEF <50% while an LVEF of ≥50% was seen in 24 (49%). Both groups had similar baseline clinical characteristics, and their mean aortic valve areas (AVAs) and degree of mitral regurgitation were similar. The mean EF of the low EF group was 35% compared with a mean EF of 61% in the normal of high EF group (P < 0.001) (Table 3). Complete postimplant and (30-day to 1-year) follow-up echocardiography was available for all patients. At 1-year follow-up, significant improvements in LVEF in the LVEF <50% group and valve function for both groups were observed. LVEF ≥50% group (LVEF: ∆: −3%, P = 0.878; AVA: ∆: 1.3 cm2, P < 0.001; mean gradient: ∆: −38 mmHg, P < 0.001); LVEF <50% group (LVEF: ∆: 10%, P < 0.001; AVA: ∆: 1.3 cm2, P < 0.001; MG: ∆: −31 mmHg, P < 0.001; Fig. 2).
Comparison of Baseline Clinical Characteristics in CABG Patients Stratified by LVEF.
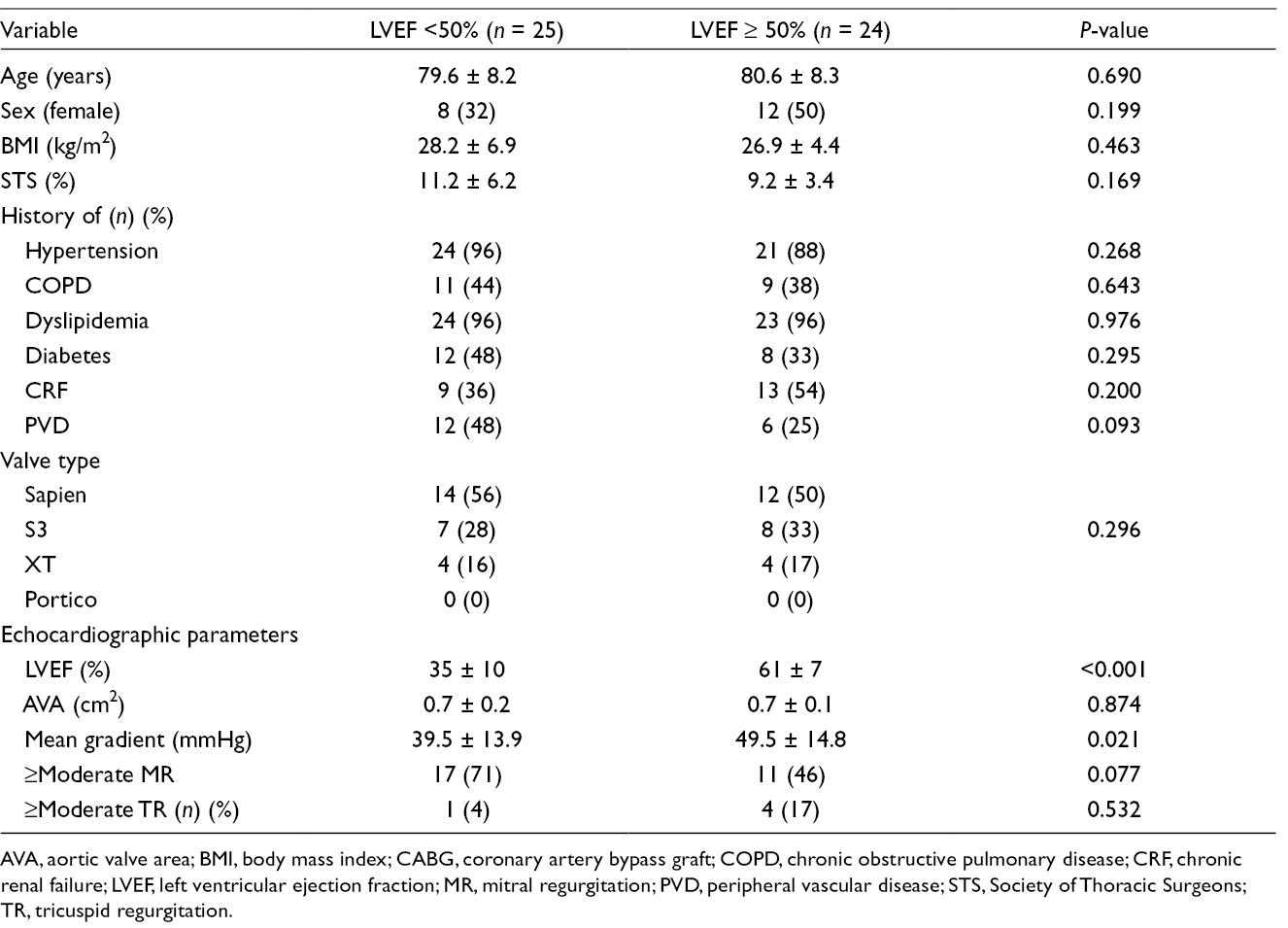
AVA, aortic valve area; BMI, body mass index; CABG, coronary artery bypass graft; COPD, chronic obstructive pulmonary disease; CRF, chronic renal failure; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; PVD, peripheral vascular disease; STS, Society of Thoracic Surgeons; TR, tricuspid regurgitation.
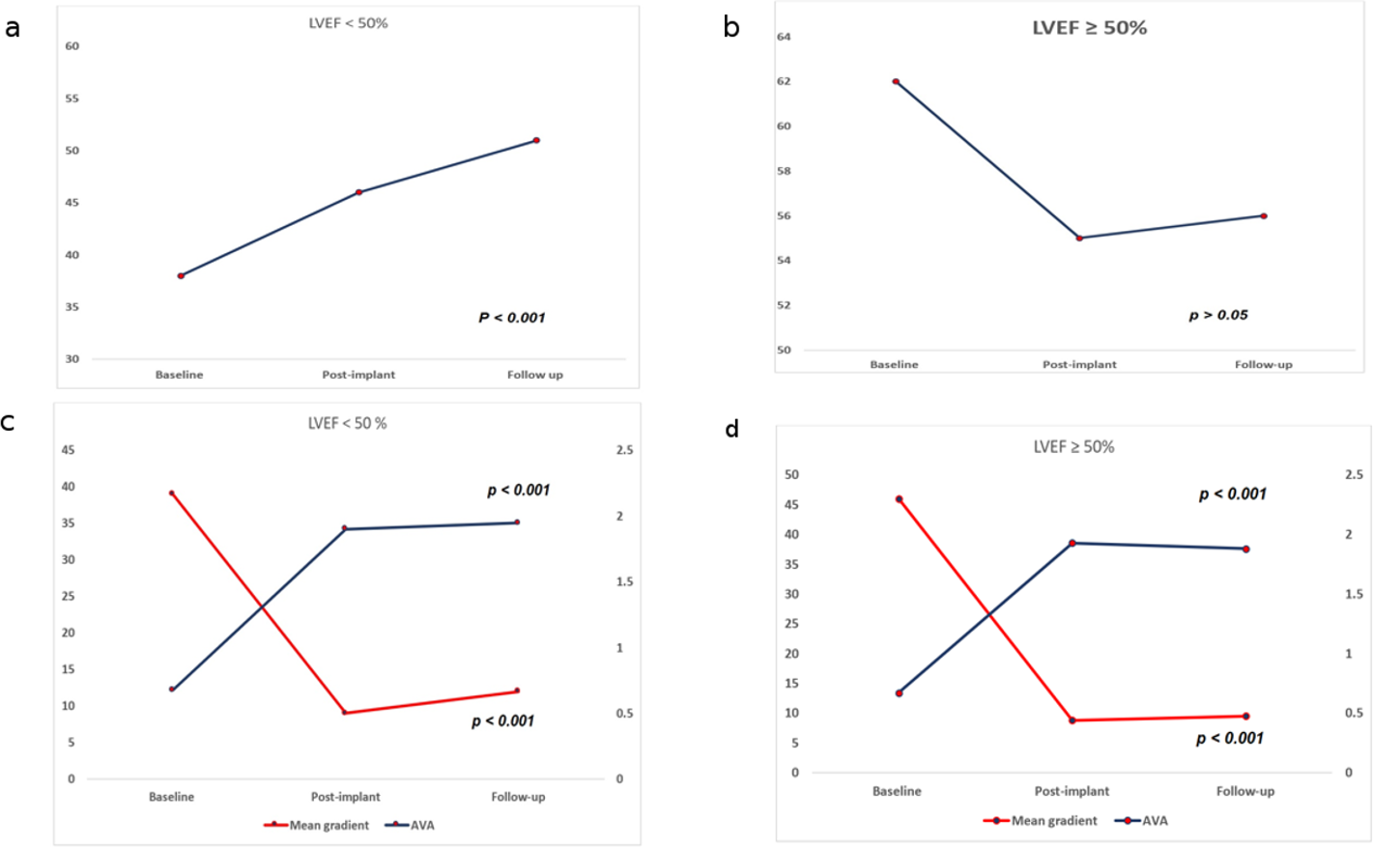
Graphical representation of changes in LVEF (a, b) and valvular function (c, d) at baseline, postimplant, and follow-up in CABG patients stratified by baseline LVEF (LVEF < 50% vs. LVEF ≥ 50%). AVA, aortic valve area; CABG, coronary artery bypass graft; LVEF, left ventricular ejection fraction.
Operative outcome comparison between TAVR-CABG patients stratified by LVEF is shown in Table 4. All outcomes were comparable and survival between both groups after stratifying them by LVEF was similar (Fig. 3).
Operative Outcomes in Coronary Artery Bypass Graft Patients Stratified by LVEF <50%.
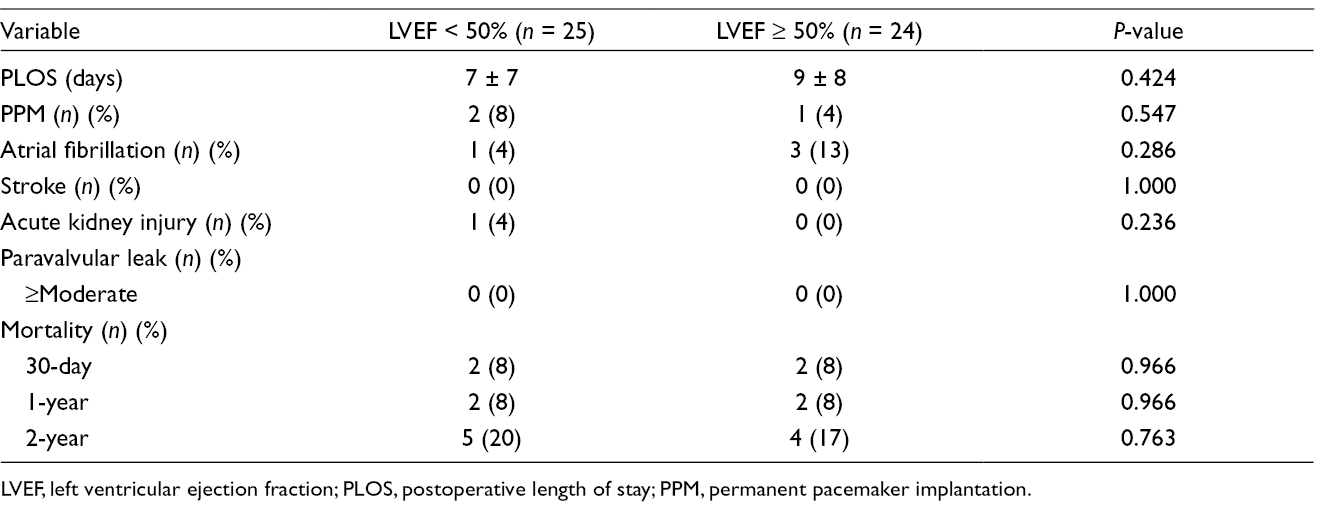
LVEF, left ventricular ejection fraction; PLOS, postoperative length of stay; PPM, permanent pacemaker implantation.
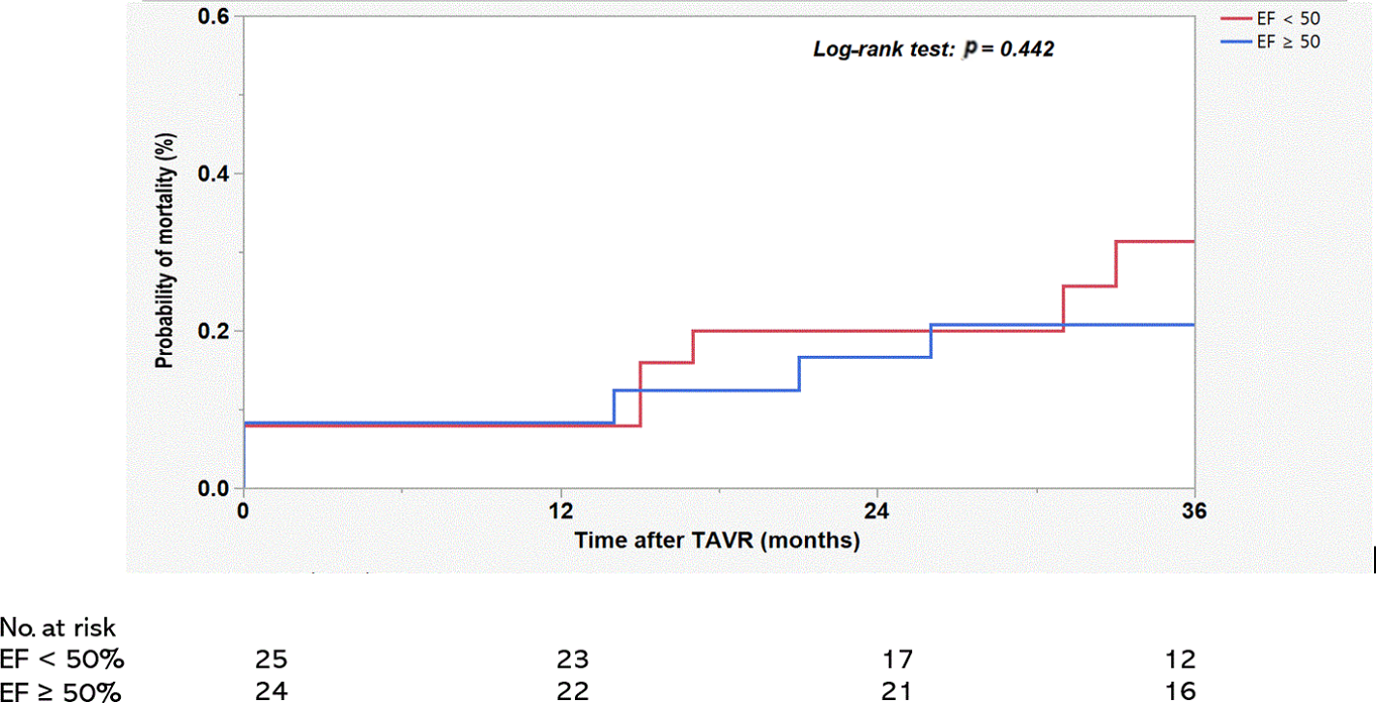
Kaplan-Meier survival curves comparing survival in patients with a history of CABG stratified by prior CABG surgery. CABG, coronary artery bypass graft; EF, ejection fraction; TAVR, transcatheter aortic valve replacement.
Discussion
Findings from the present study showed that TA-TAVR could be safely performed in patients with a history of CABG with acceptable outcomes. Among individuals with prior CABG surgery and reduced LVEF, significant improvement in both LV and valve function is seen in mid-term follow-up.
Compared to TA-TAVR patients with no history of CABG surgery, a history of CABG surgery does not affect both postoperative morbidity and mortality. These findings are consistent with what has been reported by multiple studies in the literature. 5,6 An Italian registry of TA-TAVR reported similar all-cause and cardiovascular mortality at 30 days, 1 and 2 years between patients with and without prior CABG. 5 Moreover, the authors did not find any significant differences between the 2 groups regarding postprocedure complications. In another study of propensity-matched subgroups of 45 TAVR patients, Papadopoulos et al 2 showed no difference between short- and long-term mortality. Similarly, Voudris et al found no difference in mortality rates in their single-center evaluation of 126 TA-TAVR patients. 7 All these reports are comparable with that described by Drews et al 8 and Walther et al 9 and reaffirm the notion that a history of CABG surgery does not have a significant impact on both morbidity and mortality after TA-TAVR. The present study confirms findings previously reported in the literature regarding TA-TAVR in patients with a history of CABG surgery. Moreover, the results of our study suggest that a history of CABG surgery does not impair improvement in LV function as assessed by ejection fraction at 1 year.
In our cohort of TA-TAVR patients with a history of CABG, half of them had a baseline LVEF <50%. Mean LVEF of this cohort was 35% representing a high incidence of depressed LV function. A significant improvement in LVEF was seen at both postimplant, and mid-term follow-up. Our study is the first to look at LV function recovery in this subset of patients. In a similar study of TA-TAVR patients from 33 centers in an Italian registry, D’nofrio et al investigated outcomes after TA-TAVR in a subset of patients with severely reduced EF (LVEF ≤ 35%). The authors found a significant increase of ≥10% in LVEF at discharge, which was persistent at 1-year follow-up. 10 Theoretically, it can be assumed that manipulation of the LV apex will worsen the functioning of an already suffering LV myocardium. Findings from this study, however, does not support this notion. Furthermore, the likelihood of LVEF improvement was significantly higher in the cohort with reduced LVEF than those with normal or preserved LVEF. This observation is similar to that reported in another study by D’Onofrio et al. who demonstrated a higher improvement in TA-TAVR patients with LVEF <35%. 11 Purse-string sutures and perforation of the ventricular wall by the needle and by the device delivery system can lead to myocardial damage, but this degree of myocardial dysfunction is far outweighed by the afterload reduction.
This study is a single-center retrospective study with small sample size and as such suffers all limitations inherent to retrospective studies such as a smaller sample size, and institutional and selection biases. Although all echocardiograms were completed by a single observer, assessing LV function with echocardiogram alone might not be appropriate. A better method of assessing LV function via speckle-tracking echocardiography with strain assessment would have yielded a more objective way of defining LV function. Also, we did not objectively assess coronary ischemic disease status of all patients prior to TAVR. Data on cardiac catheterization were not available for all patients and this limits the interpretation of the results above from a revascularization standpoint. Knowledge of other areas of ischemia would have been pertinent to a better understanding of how to manage this patient population. Larger randomized studies with a longer follow-up time are needed to evaluate the long-term recovery of LVEF.
Conclusions
TA-TAVR can be safely performed with acceptable postoperative outcomes in patients with a history of CABG surgery. Among those with decreased baseline LVEF, significant improvements in LV and valve functions are seen in mid-term follow-up. Given that this is a small sample size resulting from a single-center retrospective study, further evaluation of postoperative outcomes in this patient population is required.
Footnotes
*
Presented at the 56th Annual Scientific Meeting of the Eastern Cardiothoracic Surgical Society, October 17-20, 2018, Clearwater Beach, FL, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.