
Abstract
Objective
The aim of this study was to evaluate whether the addition of concomitant tricuspid valve surgery (TVS) negatively impacted operative outcomes of minimally invasive mitral valve surgery (MIMVS).
Methods
Patients undergoing MIMVS via a port-access right minithoracotomy between 2002 and 2014 at a single institution were reviewed. Patients were primarily stratified by those undergoing isolated MIMVS versus MIMVS+TVS. Propensity-matched cohorts were generated. Operative outcomes were compared between the propensity-matched cohorts and included operative mortality, complications, and length of hospital stay.
Results
A total of 1,158 patients underwent MIMVS via port-access right minithoracotomy. The majority of cases were elective (93%; n = 1,071) and 148 (13%) underwent concomitant MIMVS + TVS. Patients undergoing MIMVS + TVS were at higher risk at baseline. After propensity-matching, there were 119 isolated MIMVS and 119 MIMVS + TVS patients that were well matched with respect to all baseline variables. Cardiopulmonary bypass (148 ± 54 minutes versus 175 ± 54 minutes, P < 0.001) and aortic occlusion times (105 ± 36 minutes versus 128 ± 40 minutes, P < 0.001) were longer in the MIMVS + TVS group. Operative mortality was comparable (3% isolated MIMVS versus 4% for MIMVS + TVS; P = 0.73). Permanent pacemakers were required less frequently in the isolated MIMVS group (1% versus 6%; P = 0.03). All other complication rates were similar. Median length of hospital stay (7 versus 8 days; P = 0.13) and discharge-to-home rates (89% versus 94%; P = 0.15) were comparable.
Conclusions
Despite longer operative times, minimally invasive TVS performed concomitantly with MIMVS has similar operative outcomes with the exception of a higher pacemaker rate when compared with isolated MIMVS.
Introduction
Indications to surgically address tricuspid valve disease at the time of left-sided valve surgery remain debated. According to the 2014 American Heart Association and American College of Cardiology guidelines, the only class I recommendation for tricuspid valve surgery (TVS) at the time of left-sided valve surgery is in the setting of severe tricuspid regurgitation (TR). 1 Class II recommendations include TVS for mild or greater TR at the time of left-sided valve surgery when there is tricuspid annular dilatation or evidence of right heart failure, as well as in the setting of moderate functional TR with pulmonary artery hypertension. 1 An ongoing randomized clinical trial sponsored by the Cardiothoracic Surgical Trials Network will evaluate the utility of tricuspid valve repair in patients with mild-to-moderate TR at the time of mitral valve surgery.
Two important factors to consider when determining whether TVS should be added to isolated mitral valve surgery or not is the potential impact on early operative outcomes and the natural history and longer-term clinical sequelae of untreated TR. With regard to the former, data have been conflicting. 2,3 It is also unclear whether additional operative complexity such as performing these operations with minimal-access approaches changes the relative effect of concomitant TVS on operative outcomes. The aim of this study was to evaluate the impact of concomitant minimally invasive TVS on operative outcomes of minimally invasive mitral valve surgery (MIMVS).
Methods
Study Cohort
The study cohort consisted of adult patients aged 18 years or older undergoing MIMVS via port-access right minithoracotomy between January 1, 2002 and December 31, 2014 at a single academic institution. Data were prospectively recorded in an institutional registry and retrospectively analyzed. Reoperative surgery as well as urgent or emergent cases were included. This study was given exempt status from the institutional review board.
Baseline Characteristics
The study cohort was primarily stratified into isolated MIMVS versus MIMVS + TVS. Baseline characteristics were compared between these cohorts. Preoperative variables included age, sex, body mass index, diabetes mellitus, hyperlipidemia, hypertension, chronic kidney disease, hypertension, chronic lung disease, peripheral arterial disease, cerebrovascular disease, coronary artery disease, left ventricular ejection fraction <45%, smoking history, immunosuppression, and etiology of mitral and tricuspid valve disease. Intraoperative variables included operative urgency (elective, urgent, or emergent), arterial and venous cannulation site, aortic occlusion strategy (endoballoon or aortic cross-clamp), cardiopulmonary bypass time, and aortic occlusion time.
Operative Technique
Our operative technique is similar to prior reports of right minithoracotomy approaches to mitral valve surgery. A few brief points regarding our preferences are described below. We make our minithoracotomy incision roughly 4 cm and place it just inferior to the nipple in males and just superior to the inframammary crease in females to avoid irritation from bras. We routinely use a wound protector with no rib spreading in the working incision. We also typically utilize a retraction suture in the diaphragm for improved exposure. The anesthesia team places a venous cannula in the superior vena cava via the neck in all patients. We have largely shifted from aortic cross-clamping to the use of the endoballoon for aortic occlusion. A coordinated team approach with anesthesia and perfusion is essential to safely and effectively use the endoballoon. The endoballoon is advanced and when ready, inflated and standard 4:1 blood cardioplegia administered under direct echocardiographic guidance. Unlike the sternotomy approach where the A1/P1 area is the most difficult area of the annulus to expose, the P3 area is most difficult with MIMVS and we, therefore, start our annular stitches at the right fibrous trigone where visualization is the easiest. We typically perform concomitant TVS in cases of tricuspid endocarditis at the time of mitral endocarditis surgery, moderate or worse tricuspid stenosis, and severe TR or mild or moderate TR with a dilated tricuspid annulus >40 mm. The TVS was performed either with aortic occlusion following the MIMVS or beating heart without aortic occlusion. In either case, inflow occlusion with caval snares was obtained during the TVS.
Data Analysis
Data analyses were performed with version 14 STATA statistical software (StataCorp LP, College Station, TX, USA). Continuous variables were tested for normality using the skewness and kurtosis test. Continuous variables that were normally distributed were described as mean with standard deviation and compared using Student’s t-test. Continuous variables that were not normally distributed were presented as medians with interquartile ranges and were compared using the Wilcoxon–Mann–Whitney test. Categorical variables were compared using the χ 2 test.
Due to differences in baseline characteristics, a propensity-matched analysis was performed. A 1:1 nearest neighbor propensity-score matching without replacement was utilized. The variables that were matched were based on clinical relevance including age, sex, etiology of mitral valve disease, degree of tricuspid insufficiency, chronic lung disease, chronic kidney disease, peripheral arterial disease, cerebrovascular disease, myocardial infarction, ejection fraction <45%, and prior open-heart surgery. The PSMATCH2 statistical module for STATA was used for this purpose.
Outcomes were then compared between the propensity-matched cohorts. The primary outcome was operative mortality, defined as 30-day or in-hospital mortality. Secondary outcomes included postoperative complications such as pacemaker insertion, acute renal failure requiring dialysis, stroke, prolonged mechanical ventilation >24 hours, pneumonia, reoperation for bleeding, gastrointestinal complication, acute limb ischemia, and sepsis. Other secondary outcomes included blood product transfusion, discharge to home rates in hospital survivors, and length of hospital stay.
Results
Baseline Characteristics of the Unmatched Cohorts
During the study period, 1,158 patients underwent MIMVS via port-access right minithoracotomy (Online Supplementary Table S1). Most of the operations (82%; n = 949) were performed by the senior author (W.C.H.). There were 148 (13%) patients who underwent MIMVS with concomitant TVS. All but 1 TVS was a repair. The most common sizes of partial tricuspid annuloplasty rings were 30 (37%), 32 (35%), or 28 (24%). A total of 54 (4.7%) patients had a concomitant procedure for atrial fibrillation.
The majority of cases were elective (93%). A total of 72 (6%) patients had prior open-heart surgery. Patients in the MIMVS + TVS cohort were at higher risk at baseline, including older age, more chronic lung disease, and more cerebrovascular disease (Online Supplementary Table 1). There were also a higher percentage of females in the MIMVS + TVS group.
Operative characteristics were similar between groups with the exception of cardiopulmonary bypass and aortic occlusion times, which were longer in the MIMVS + TVS cohort (Online Supplementary Table 2). Aortic occlusion was most commonly achieved via endoballoon (74%) at a similar frequency between groups. There were 3 (0.4%) aortic dissections in the endoballoon occlusion group. Most cases entailed a mitral valve repair (83%) and were again similar between MIMVS and MIMVS + TVS.
Operative Outcomes in the Unmatched Cohorts
There were 29 (2.5%) operative mortalities in the overall study population. There was comparable mortality in the MIMVS +TVS group in the unmatched comparison (4.7%, 2.2%; P = 0.06) (Online Supplementary Table 3). Permanent pacemaker implantation was required more frequently in the MIMVS + TVS cohort. Discharge-to-home rates were also lower in the MIMVS + TVS cohort in the unmatched comparison (Online Supplementary Table 3). The remainder of complications were similar between the unmatched cohorts.
Baseline Characteristics After Propensity Matching
Propensity matching yielded 119 MIMVS and 119 MIMVS + TVS patients (Table 1). These cohorts were well matched with respect to all preoperative baseline variables with no significant differences noted (Table 1). The proportions of patients undergoing elective surgery remained similar, as did the proportions utilizing endoballoon aortic occlusion and undergoing mitral valve repair (Table 2). In those undergoing mitral valve replacement, 23 (51%) were bioprosthetic valves and 22 (49%) were mechanical valves. Most repairs were considered complex (64%; n = 124). Leaflet resection was limited to the posterior leaflet and leaflet preservation was employed with anterior leaflet pathology. In total, 40 (21%) of mitral repairs had neochords in the propensity-matched groups. Cardiopulmonary bypass and aortic occlusion times, which were not involved in the propensity matching due to the expected longer times with concomitant procedures, remained longer in the MIMVS +TVS cohort (Table 2).
Comparison of Baseline Preoperative Characteristics Between the Propensity-Matched Cohorts.
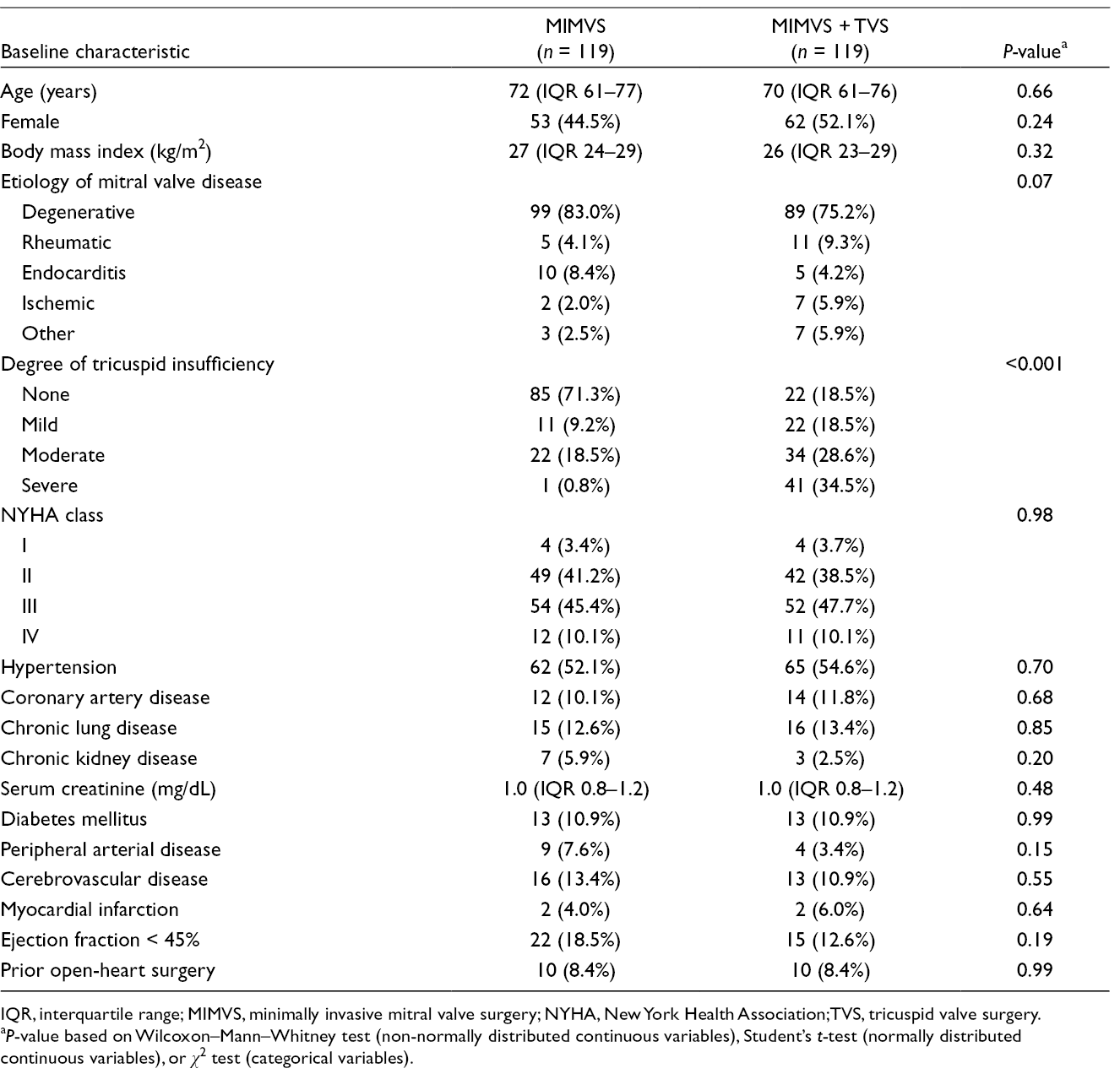
IQR, interquartile range; MIMVS, minimally invasive mitral valve surgery; NYHA, New York Health Association;TVS, tricuspid valve surgery.
a P-value based on Wilcoxon–Mann–Whitney test (non-normally distributed continuous variables), Student’s t-test (normally distributed continuous variables), or χ 2 test (categorical variables).
Comparison of Baseline Intraoperative Characteristics Between the Propensity-Matched Cohorts.
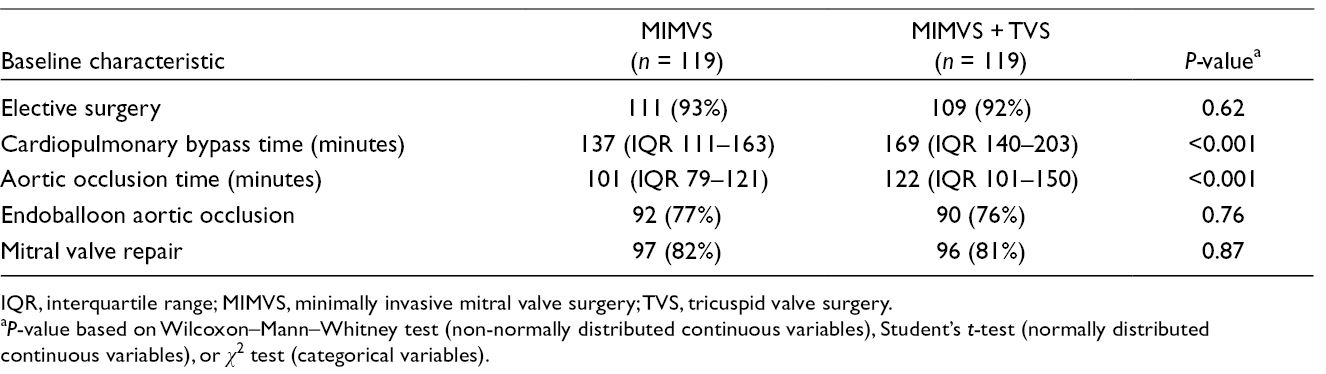
IQR, interquartile range; MIMVS, minimally invasive mitral valve surgery; TVS, tricuspid valve surgery.
a P-value based on Wilcoxon–Mann–Whitney test (non-normally distributed continuous variables), Student’s t-test (normally distributed continuous variables), or χ 2 test (categorical variables).
Operative Outcomes After Propensity Matching
All operative outcomes were similar between MIMVS and MIMVS +TVS after propensity matching with the exception of pacemaker implantation which was higher in MIMVS +TVS (1%, 6%; P = 0.03) (Table 3). Operative mortality was 3.4% for MIMVS and 4.2% for MIMVS +TVS (P = 0.73). Most patients were discharged home (91%) with no differences between groups. Blood products were transfused in 29%, again with no difference between cohorts. The early reoperation rate was 7.1% and similar between groups. Median length of hospitalization was also comparable at 7 and 8 days for MIMVS and MIMVS +TVS, respectively (P = 0.13). Similar findings were demonstrated when limiting the analysis to only patients with degenerative mitral valve disease and secondary functional TR.
Comparison of Outcomes After Propensity Matching.
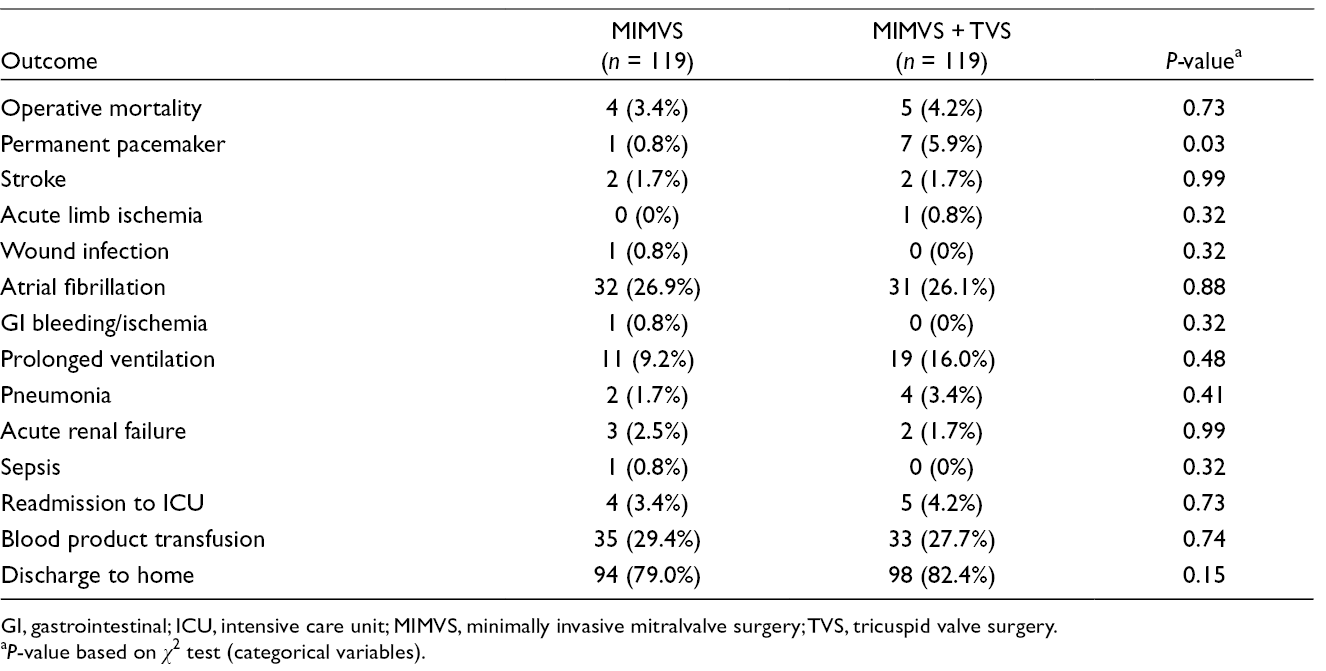
GI, gastrointestinal; ICU, intensive care unit; MIMVS, minimally invasive mitralvalve surgery; TVS, tricuspid valve surgery.
a P-value based on χ 2 test (categorical variables).
Discussion
Study Rationale
MIMVS was introduced in the 1990s and subsequently included a variety of surgical approaches such as parasternal, minithoracotomy, robotic, and hemisternotomy. 4,5 Our preference has been to use the Heartport platform utilizing a right minithoracotomy approach. Certain contraindications are generally applied regardless of the individual surgeon’s experience with MIMVS. These include significant peripheral arterial disease, low ejection fraction, more than mild aortic insufficiency, severe right ventricular dysfunction, significant mitral annular calcification, and severe pulmonary hypertension. Other factors can make a minimally invasive approach to mitral surgery more challenging, such as morbid obesity, chest wall deformities, pulmonary disease with inability to tolerate prolonged periods of single-lung ventilation in the case of right minithoracotomy approaches, and abdominal pannus, inguinal hernias, or prior groin incisions. It is generally recommended that surgeons with less minimal-access experience typically confine their practice early on to isolated MIMVS with simple mitral valve repairs. Complex mitral repairs as well as those requiring concomitant tricuspid valve or atrial fibrillation procedures are generally attempted once more experience accumulates with MIMVS. In this report, we evaluate the impact of concomitant TVS on outcomes of MIMVS at a single academic institution. The principal finding was that despite longer cardiopulmonary bypass and aortic occlusion times, the addition of concomitant TVS did not have an adverse impact on operative outcomes of MIMVS.
Study Implications
The indications for concomitant TVS in the setting of left-sided valve surgery remain debated. An ongoing randomized clinical trial sponsored by the Cardiothoracic Surgical Trials Network will randomize patients undergoing mitral valve surgery for degenerative mitral regurgitation with moderate TR or trace or mild TR with a dilated tricuspid annulus of 40 mm or more to isolated mitral valve surgery versus mitral valve surgery with tricuspid repair. Although the debate on whether to perform concomitant tricuspid repair often revolves around longer-term outcomes such as survival, development or progression of heart failure, and natural history of untreated TR, operative outcomes are an essential component of the discussion as well. A multicenter study involving 17 institutions and 5,495 operations demonstrated that concomitant TVS during mitral valve surgery had an increased unadjusted and risk-adjusted impact on operative mortality risk. 3 A conflicting analysis of the Society of Thoracic Surgeons national database evaluated 88,473 patients undergoing mitral valve surgery, and found that at all grades of TR, the addition of concomitant TVS had no impact on risk-adjusted operative mortality risk. 2 A single-center study demonstrated no difference in operative outcomes between isolated mitral valve surgery and mitral valve surgery with concomitant TVS in patients with degenerative mitral regurgitation. 6
There is less data regarding the impact of concomitant TVS on outcomes of MIMVS as compared to the literature in the setting of conventional sternotomy. A single institution analysis of 132 patients undergoing MIMVS with concomitant TVS over 5 years demonstrated an in-hospital mortality rate of 4% and 5-year survival of 88%. 7 Another study similarly concluded that MIMVS with concomitant TVS was a safe procedure, with a 4.3% 30-day mortality rate, 5-year survival of 77%, and 5-year freedom from tricuspid valve-related reoperation of 91%. 8
The safety of MIMVS overall has been established in multiple prior studies. A high-volume experience of 1,604 consecutive patients undergoing MIMVS, including 15% with concomitant TVS, demonstrated an in-hospital mortality of 1.1%. 9 Studies comparing MIMVS with conventional mitral valve surgery through a sternotomy have produced mixed results. A systematic review and meta-analysis including over 20,000 patients from 45 studies found that 30-day stroke and all-cause mortality were similar between approaches, although time in the intensive care unit, hospital stay, and mechanical ventilation time were all shorter with MIMVS. 10 This came at the expense of a higher rate of aortic dissections and longer operative times in the MIMVS cohort. There is undoubtedly a learning curve associated with MIMVS and this has been analyzed and demonstrated in various studies. 11,12
The rate of pacemaker implantation was higher with concomitant TVS in our analysis. The impact of this on longer-term outcomes of MIMVS should be evaluated in future studies. An analysis of surgical aortic valve replacement demonstrated an increased risk of long-term death in those who required early pacemaker implantation. 13 In transcatheter aortic valve replacement, the need for a pacemaker postprocedurally was associated with an increased risk of heart failure readmission but not mortality at 4 years. 14 Interestingly, a study of tricuspid valve operations found that postoperative pacemaker implantation was associated with improved life expectancy albeit with greater morbidity. 15
The major implication of our study is that despite longer operative times and higher pacemaker rate, the addition of concomitant TVS to MIMVS does not have a substantial adverse impact on operative outcomes. Accordingly, our data support the notion that future trials aiming to evaluate the potential benefits of concomitant TVS should not exclude patients undergoing MIMVS. Despite a steeper learning curve and added complexity when performed minimally invasively, concomitant TVS can be performed safely by surgeons experienced in MIMVS.
Study Limitations
One limitation of this study is its retrospective nature. There are potential confounders that may not have been accounted for in the analyses. In addition, most of the operations (82%) were done by an experienced MIMVS surgeon and these results may not be accurately extrapolated to other surgeons or other institutions, particularly with those with less experience. There was also no longitudinal echocardiographic data evaluated in this analysis although that is certainly of interest in determining the impact of concomitant TVS on outcomes of mitral valve surgery. Finally, there is the potential for type II error where no differences in outcomes were detected although there may be a difference that becomes apparent with larger sample sizes of patients.
Conclusions
In this study, we evaluated our pool of 1,158 MIMVS patients to compare the operative outcomes of MIMVS plus concomitant TVS versus isolated MIMVS. Due to significant baseline differences, the groups were propensity matched. After matching, longer operative times were noted in the MIMVS plus concomitant TVS group. Despite this, there were no differences in operative outcomes with the exception of pacemaker implantation, which was higher in MIMVS plus TVS. Collectively, these results suggest that concomitant TVS can be performed safely in the setting of MIMVS.
Supplemental Material
Online supplementary - Supplemental material for Operative Outcomes of Concomitant Minimally Invasive Mitral and Tricuspid Valve Surgery
Supplemental material, Online supplementary, for Operative Outcomes of Concomitant Minimally Invasive Mitral and Tricuspid Valve Surgery by Arman Kilic, Wilson Y. Szeto, Pavan Atluri, Michael A. Acker and W. Clark Hargrove in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kilic is on the Advisory Board for Medtronic.
Funding
The author(s) recieved no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.